
Abstract
Background
Vocal fold leukoplakia (VFL) comprises a heterogeneous spectrum of epithelial lesions with variable risks of recurrence and malignant transformation. Laryngopharyngeal reflux (LPR) has increasingly been considered a chronic mucosal stressor in VFL, and pepsin has emerged as one of the most biologically relevant reflux-associated molecules.
Objective
To summarize current evidence on the pathobiological role of pepsin in VFL and to discuss its diagnostic and therapeutic relevance.
Methods
A PRISMA-informed review was conducted using a prespecified PICO framework. PubMed, Web of Science, Embase, Google Scholar, and relevant gray-literature sources were searched from database inception to March 2026. Two reviewers independently screened records, extracted data, and assessed methodological quality using design-appropriate tools. The certainty of evidence was summarized using the GRADE framework. Owing to clinical, methodological, and outcome heterogeneity, formal meta-analysis was not performed.
Results
Available evidence suggests that pepsin may function not only as a marker of reflux exposure but also as an active mediator of epithelial injury. Tissue and translational studies indicate associations between pepsin-related reflux and epithelial barrier disruption, inflammatory infiltration, oxidative stress, autophagy, and metabolic reprogramming in vocal fold tissues. In VFL, tissue pepsin expression appears to increase with dysplasia severity, whereas salivary pepsin testing remains method-dependent and diagnostically inconsistent. Endoscopic morphology, vascular pattern assessment, and histopathology remain the core of risk stratification. Laser-based interventions continue to expand treatment options, but pepsin-directed management remains investigational.
Conclusions
Pepsin is a promising link between reflux biology and VFL progression, but the overall certainty of current evidence remains low to very low. At present, its main value lies in complementing established clinical and pathological assessment while refining mechanistic understanding of lesion behavior. Prospective studies integrating objective reflux testing, standardized pepsin measurement, advanced imaging, pathology, and longitudinal outcomes are needed before pepsin can be incorporated into routine clinical decision-making.
Introduction
Vocal fold leukoplakia (VFL) is a descriptive clinical term rather than a single histopathologic diagnosis. It encompasses epithelial alterations ranging from hyperkeratosis without dysplasia to high-grade dysplasia and carcinoma in situ. This heterogeneity explains why VFL remains one of the most challenging lesions in laryngology: endoscopically similar plaques may behave very differently over time. Management therefore depends on accurate pathological diagnosis, rational risk stratification, and longitudinal surveillance rather than on morphology alone.1-3
The significance of this challenge has become clearer with modern classification systems for laryngeal precursor lesions. In particular, the World Health Organization two-tier framework emphasizes the clinical importance of high-grade dysplasia and narrows the distinction between moderate dysplasia and biologically more aggressive lesions.1,3 Clinically, the key question is whether a lesion is biologically stable, prone to recurrence, or already on a pathway toward malignant transformation.
Traditional risk factors such as smoking and alcohol remain important, but chronic inflammatory and chemical stressors are increasingly recognized. Laryngopharyngeal reflux (LPR) has been implicated in this context. The 2024 International Federation of Otorhinolaryngological Societies (IFOS) consensus defined LPR as a disease of the upper aerodigestive tract resulting from the direct and/or indirect effects of gastroduodenal refluxate, producing morphological and/or neurological changes in the upper aerodigestive tract. 4 This definition is particularly relevant to VFL because it frames reflux as a tissue-level aggressor.
Among refluxate components, pepsin has attracted particular interest because it is biologically plausible and measurable in tissue and saliva. Available studies suggest that pepsin may act not only as a marker of reflux exposure but also as a potential mediator of epithelial injury, metabolic reprogramming, and dysregulated repair.5-8 However, the evidence remains fragmented across clinical, translational, and review literature. Accordingly, this review synthesizes the available evidence on the pathobiological role of pepsin in VFL and evaluates its diagnostic and therapeutic relevance in current practice.
Methods
Search Strategy and Information Sources
This review was conducted using a PRISMA-informed approach and was revised to improve transparency in accordance with PRISMA 2020 principles. 9 PubMed, Web of Science, and Embase were searched from database inception to March 2026 using the following terms: “vocal fold leukoplakia” or “vocal cord leukoplakia” and “laryngopharyngeal reflux” or “LPR” or “gastroesophageal reflux” or “GERD” or “pepsin”. Reference lists of relevant studies were also screened.
Review Question and PICO Framework
The review question was: in patients with vocal fold leukoplakia, what is the biological, diagnostic, and therapeutic relevance of pepsin or pepsin-related laryngopharyngeal reflux exposure? The PICO framework was defined as follows: Population, patients with vocal fold leukoplakia or experimental models of vocal fold leukoplakia; Intervention/exposure, pepsin detection, pepsin exposure, or reflux-related biological stress; Comparator, patients or models without pepsin/reflux exposure, lower-grade lesions, non-dysplastic lesions, or alternative clinical assessment strategies when available; Outcomes, epithelial injury, inflammatory and oxidative stress responses, autophagy, metabolic reprogramming, dysplasia grade, recurrence, malignant transformation, diagnostic performance, and management implications.
Gray Literature and Supplementary Searches
To reduce publication bias, supplementary searches were conducted in Google Scholar, ClinicalTrials.gov, major conference/proceedings sources when accessible, and reference lists of eligible articles. Gray-literature records were considered eligible if they provided sufficient methodological and outcome information relevant to the PICO question. No additional gray-literature record met all eligibility criteria for inclusion in the final qualitative synthesis.
Eligibility Criteria and Study Selection
Eligible studies included English-language clinical, translational, and experimental studies directly addressing pepsin, reflux-related biological mechanisms, diagnostic assessment, or management implications in vocal fold leukoplakia. Primary studies were prioritized for evidence synthesis. Consensus statements, systematic reviews, and narrative reviews were not pooled with primary evidence; they were used only to frame definitions, clinical context, or methodological limitations. Conference abstracts, duplicate reports, non-English articles, studies without sufficient methodological information, and studies not specifically related to vocal fold leukoplakia, pepsin, or reflux-related laryngeal biology were excluded.
Study Selection Process
Two reviewers independently screened titles and abstracts, assessed full-text eligibility, and extracted data using a standardized extraction form. Disagreements were resolved by discussion and, when necessary, by consultation with a senior author. Extracted variables included study design, study population or experimental model, pepsin or reflux-assessment method, comparator group, primary outcomes, main findings, and limitations relevant to bias or applicability.
Data Extraction and Synthesis
Because of heterogeneity in study design, populations, pepsin-assessment methods, comparators, and outcome reporting, formal meta-analysis was not performed. Instead, the available evidence was synthesized narratively and comparatively across biological, diagnostic, and clinical domains. When diagnostic or management studies reported quantitative estimates, the values were summarized descriptively rather than pooled.
Risk-Of-Bias and Certainty-Of-Evidence Assessment
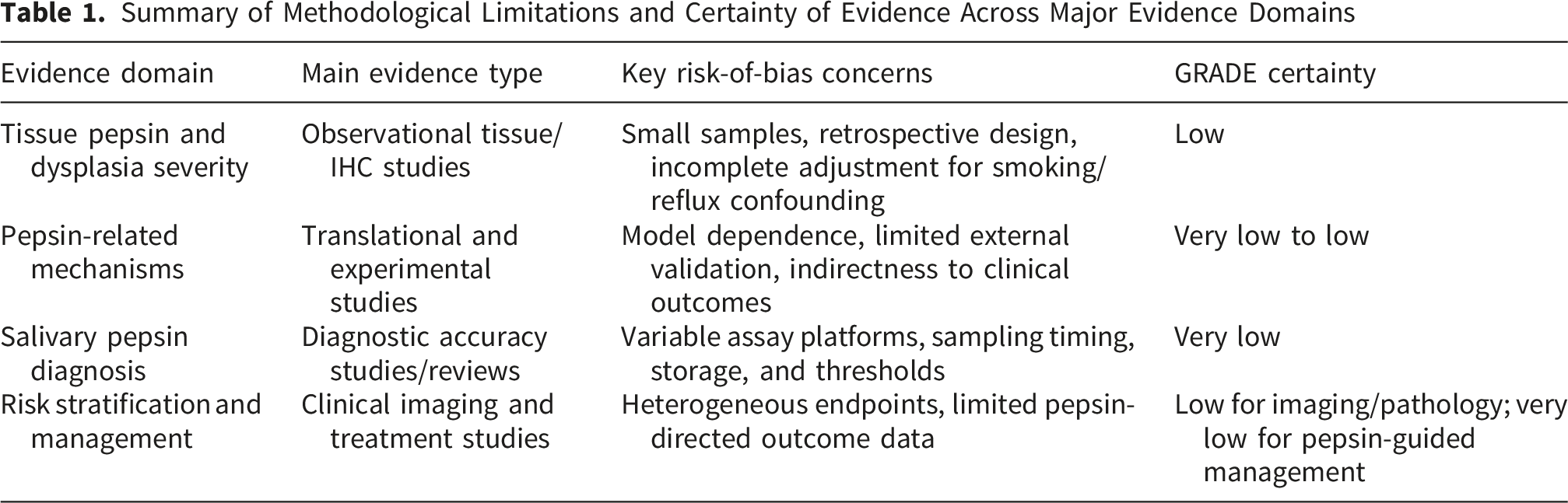
Methodological quality and risk of bias were assessed using design-appropriate tools. Observational cohort and case-control studies were appraised with the Newcastle-Ottawa Scale, 10 diagnostic studies were evaluated with domains conceptually aligned with QUADAS-2, 11 and experimental or translational studies were assessed using relevant Joanna Briggs Institute critical-appraisal domains. 12 Evidence certainty was summarized using the GRADE framework. 13 Certainty ratings considered risk of bias, inconsistency, indirectness, imprecision, and publication bias. Because most included studies were observational or translational and because outcome measures were heterogeneous, the certainty of evidence was expected to range from low to very low for most clinical conclusions.
Statistical Analysis
No new patient-level statistical analysis was performed. The search yield and selection process were summarized using counts and a PRISMA flow diagram. Reported statistics from included studies, including P values, diagnostic estimates, recurrence rates, or associations with dysplasia grade, were extracted when available and interpreted according to the criteria used in the original studies. Meta-analysis, subgroup analysis, and publication-bias funnel plots were not undertaken because the included studies differed substantially in design, exposure definition, comparator selection, assay platform, and outcome measurement.
Results
Study Selection and Overview
The database search identified 226 records. After removal of duplicates, 44 unique records remained for title and abstract screening. Of these, 20 records were excluded because they were not directly related to vocal fold leukoplakia, pepsin, or laryngopharyngeal reflux. The remaining 24 full-text articles were assessed for eligibility and included in the qualitative synthesis. Primary studies were used for evidence synthesis, whereas review articles and consensus documents were used only for contextual interpretation. The study selection process is summarized in Figure 1. PRISMA flow diagram of study selection.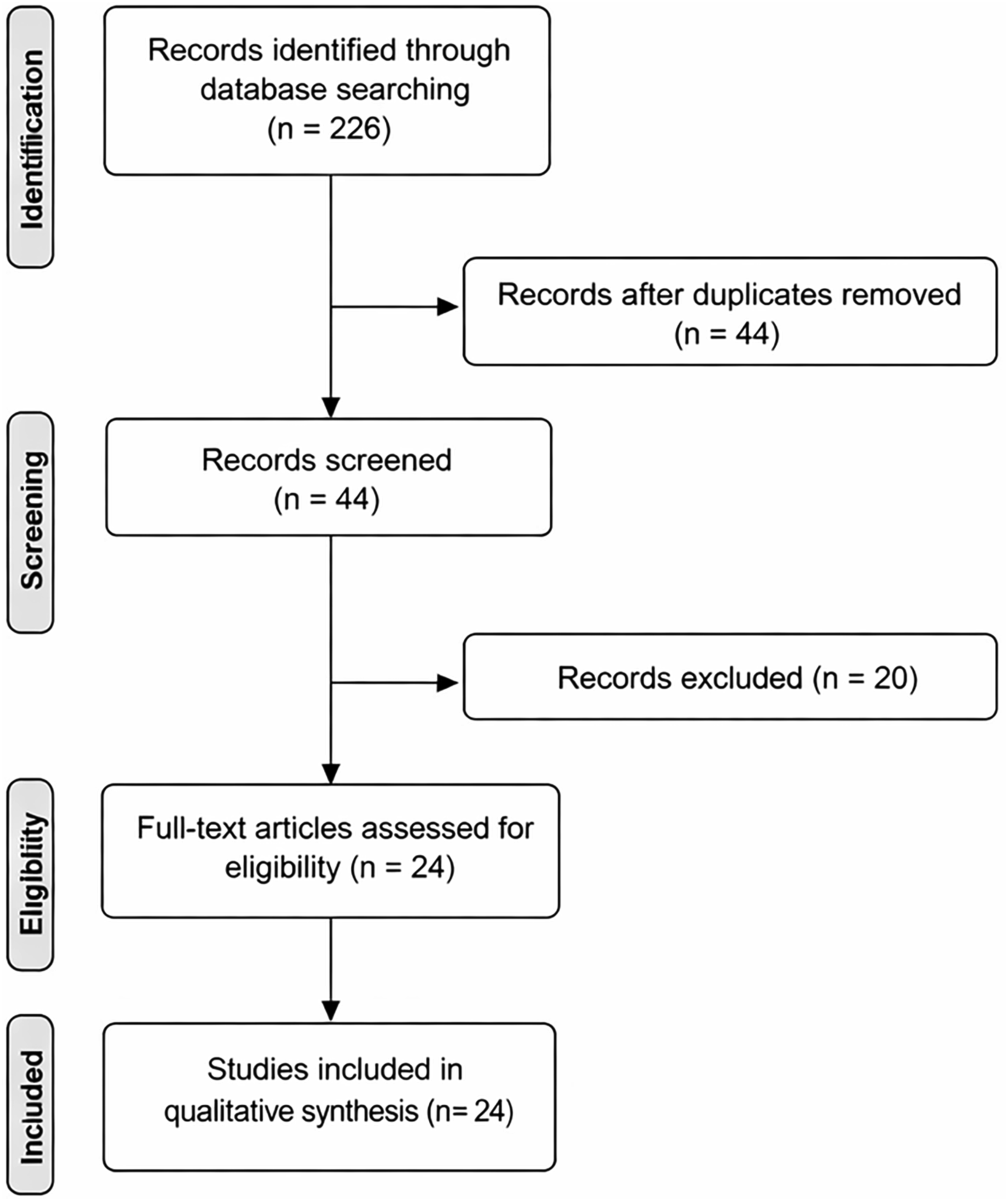
Risk-Of-Bias and Certainty Summary
Summary of Methodological Limitations and Certainty of Evidence Across Major Evidence Domains
Biological Evidence for Pepsin in Vocal Fold Leukoplakia
The biological relevance of pepsin in vocal fold leukoplakia (VFL) is supported by two related observations: pepsin can be detected in reflux-related laryngeal disease, and pepsin exposure is associated with structural and molecular alterations in laryngeal tissues.14,15 Reflux- and pepsin-related laryngeal injury has been linked to inflammatory infiltration, epithelial junctional disruption, widening of intercellular spaces, oxidative stress, and altered mucosal defense factors5. These findings suggest that chronic reflux-related exposure may create a vulnerable epithelial microenvironment rather than a transient mucosal insult.
In VFL, this is clinically relevant because chronic epithelial injury and dysregulated repair may contribute to lesion persistence and progression. Tissue-based studies suggest that pepsin-positive lesions may represent a biologically distinct subset and that both overall pepsin expression and strong pepsin positivity increase with dysplasia severity.14,15 Although these findings do not establish causation, they support the interpretation of pepsin as more than an incidental reflux marker.
Translational studies further suggest that pepsin may participate in several interconnected pathogenic processes. One proposed mechanism involves the Glut-1/H+/K+-ATPase axis. Elevated Glut-1 expression may promote vocal cord leukoplakia by upregulating laryngeal H+/K+-ATPase, thereby facilitating reactivation of absorbed pepsin and aggravating mucosal injury6-8. This finding links reflux biology to metabolic adaptation and indicates that retained pepsin may remain biologically relevant when local conditions permit reactivation.
Metabolic reprogramming represents another important mechanism. Acidified pepsin has been shown to enhance glycolysis in dysplastic VFL epithelial cells, promote proliferation and migration, reduce oxidative phosphorylation, and drive a shift toward aerobic glycolysis. 7 Autophagy may also contribute to pepsin-related epithelial adaptation, as pepsin has been reported to increase proliferation of vocal cord leukoplakia epithelial cells by inducing autophagy. 8 These findings suggest that pepsin-related stress may activate pro-survival pathways rather than merely causing destructive injury.
The reflux-related biological framework is not limited to pepsin. Deoxycholic acid has been shown to drive ATP4A-dependent growth and migration of VFL epithelial cells through the TGR5/JAK2/STAT3 signaling pathway, suggesting that bile acid reflux may cooperate with pepsin-related mechanisms11. Other reflux-associated pathways, including NF-κB and SphK1/S1PR1 signaling, have also been implicated in progression-associated changes.16,17 Taken together, the available evidence supports a model in which pepsin contributes to epithelial barrier dysfunction, chronic inflammation, oxidative stress, metabolic reprogramming, autophagy, and dysregulated repair in a susceptible epithelial microenvironment. Pepsin may therefore be conceptualized as a marker-effector molecule that reflects reflux exposure and may amplify reflux-induced epithelial injury and lesion persistence (Figure 2). However, current mechanistic evidence remains limited and requires external validation before these pathways can be incorporated into predictive or therapeutic models of VFL progression. Proposed role of pepsin in the development and progression of vocal fold leukoplakia. Pepsin derived from laryngopharyngeal reflux may accumulate in the laryngeal mucosa and contribute to epithelial injury, chronic inflammation, oxidative stress, metabolic reprogramming, autophagy, and dysregulated repair. These biological effects may promote lesion persistence, dysplasia progression, recurrence, and malignant potential in vocal fold leukoplakia. Non-acid reflux components, such as bile acids, may further cooperate with pepsin-related pathways. Solid arrows represent evidence-supported associations, and dashed arrows represent proposed mechanisms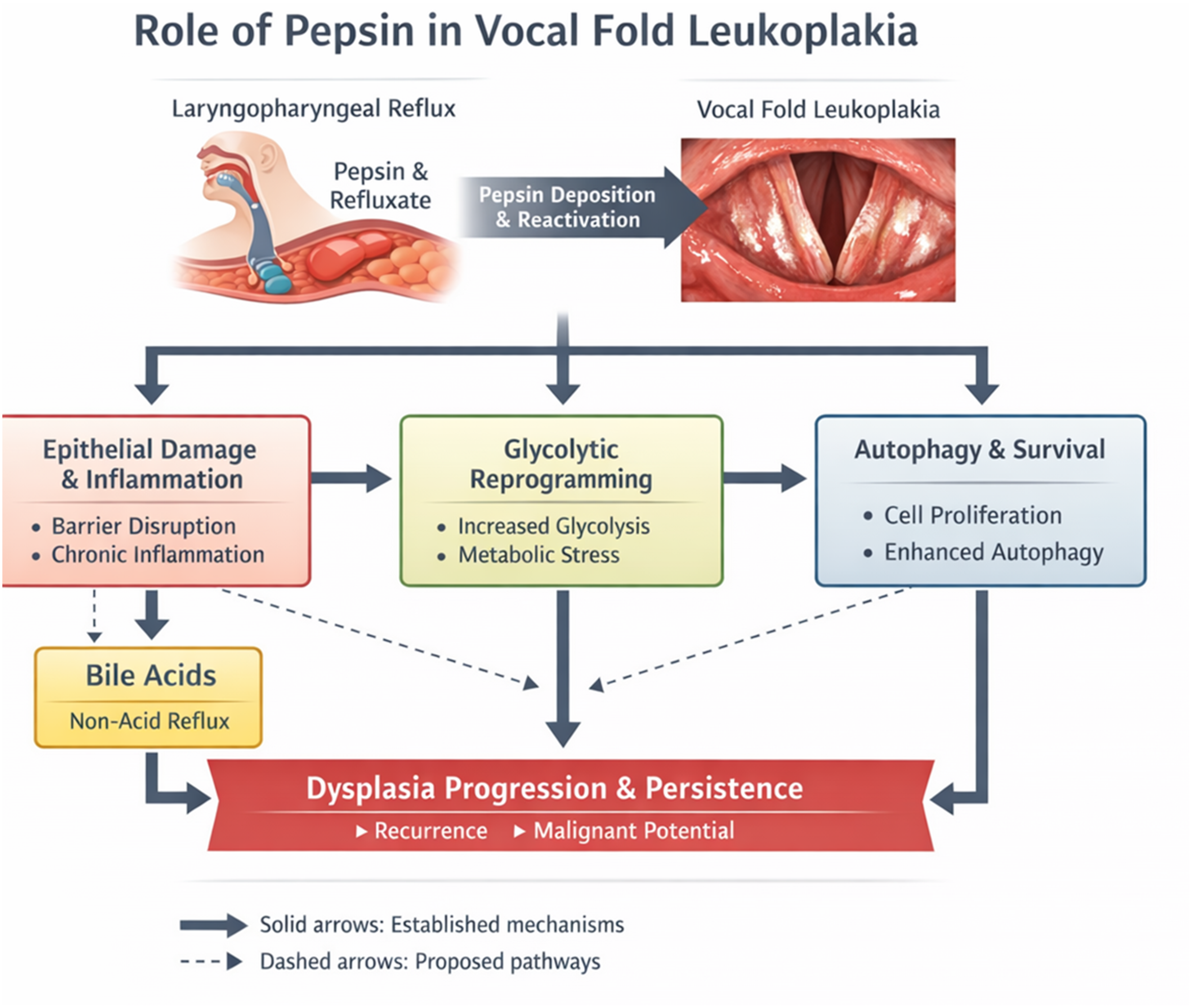
Diagnostic Evidence
Pepsin is clinically attractive because it provides a measurable link between reflux biology and laryngeal disease. In VFL, this is relevant because clinicians must determine whether biomarkers can add information beyond morphology and histopathology. Pepsin can be assessed in tissue specimens and saliva, offering either tissue-based confirmation of reflux exposure or noninvasive outpatient testing.
Tissue-based assessment has conceptual advantages. Biopsy is already part of the diagnostic pathway for many suspicious or persistent vocal fold lesions, and pepsin immunohistochemistry can therefore be performed without an additional invasive procedure. Previous biopsy-based studies suggest that pepsin immunohistochemistry may help identify reflux-related biological exposure in laryngeal lesions, including VFL.14,15,18 Its value lies not in independently diagnosing laryngopharyngeal reflux, but in providing evidence that reflux-associated components have interacted with lesion-bearing mucosa.
However, the clinical meaning of tissue pepsin staining should not be overstated. A positive result does not by itself define lesion aggressiveness, predict recurrence, or determine malignant potential.1,3,16,19 Nor does it replace established reflux testing when formal LPR assessment is clinically indicated.4,18,20 Tissue pepsin should currently be interpreted as supportive biological evidence and integrated with reflux symptoms, endoscopic findings, smoking status, lesion morphology, and pathological grade.1,3,20 Used in isolation, it remains too nonspecific to function as a decisive clinical tool.
Association studies also support a relationship between reflux and VFL. Earlier observational studies linked gastropharyngeal or laryngopharyngeal reflux with vocal fold leukoplakia and related epithelial lesions, and later studies confirmed associations between LPR and VFL in contemporary cohorts.19-24 These data suggest clinical relevance, although causality cannot be established.
Salivary pepsin testing is appealing because it is noninvasive, repeatable, and potentially suitable for serial monitoring. However, its diagnostic performance remains variable because of differences in assay methods, collection protocols, sampling timing, storage conditions, and thresholds. 25 For VFL, this limitation is especially important because the central clinical problem is not merely reflux detection but assessment of dysplasia severity and oncologic risk. Even when pepsin confirms reflux exposure, clinicians must still determine whether the lesion is hyperplastic, dysplastic, or malignant. Pepsin may therefore help explain the biological background, but it does not resolve the core pathological question.
This cautious interpretation is consistent with modern LPR literature, which emphasizes multimodal diagnosis rather than reliance on symptom scores, laryngoscopic appearance, or a single biomarker.4,25 Similarly, in VFL, pepsin cannot replace laryngoscopic morphology, vascular pattern assessment, histopathology, and longitudinal surveillance. Its most realistic current role is as an adjunctive biomarker that may add incremental value in selected patients, such as those with recurrent leukoplakia, disproportionate lesion persistence, strong reflux background, or discordance between symptoms and endoscopic findings.1,4,16,19,20 In research settings, standardized pepsin assessment may also contribute to composite models combining pathology, imaging, and host factors.1,2,26-31
Clinical Implications for Risk Stratification and Management
Despite growing interest in biomarkers, VFL risk stratification remains based primarily on endoscopic morphology, vascular pattern analysis, and histopathology. Accurate pathological diagnosis is essential because a white vocal fold lesion has a broad differential diagnosis and different implications depending on the presence and grade of dysplasia1. Contemporary evidence on moderate laryngeal dysplasia further supports careful risk stratification, as malignant transformation rates may resemble those of severe dysplasia and carcinoma in situ more closely than those of low-grade lesions. 3
Endoscopic imaging is improving this process. Narrow-band imaging has shown diagnostic value for identifying malignant transformation in vocal cord leukoplakia. 26 A combined classification based on intrapapillary capillary loops and morphology demonstrated high predictive accuracy for VFL pathology, with mean area-under-the-curve values exceeding 0.95 and excellent sensitivity. 27 Artificial intelligence and optical imaging are also emerging. A multicentre diagnostic study reported that a multi-instance learning model improved pathological classification of VFL using white-light and narrow-band imaging datasets24, and machine learning-assisted handheld optical coherence tomography has enabled rapid intraoperative classification of low-risk, high-risk, and malignant lesions. 29 These approaches may eventually support real-time, voice-preserving decision-making.
Nevertheless, pathology remains the reference standard. Imaging and computational tools improve preoperative and intraoperative prediction, but they do not replace histological diagnosis.1,3,26-29 In this framework, pepsin should be regarded as complementary rather than competing. Imaging and pathology define structural severity, whereas pepsin may help explain a reflux-related biological background that influences lesion behavior over time.4,18,20
Therapeutically, pepsin currently refines clinical reasoning rather than defines a new treatment pathway. If reflux-associated injury contributes to epithelial instability in some patients, reflux control may deserve greater attention in individualized management.4-8,14,15,18,20,32 However, current evidence does not support using pepsin assessment to replace biopsy or independently determine conservative versus surgical treatment. Management should still be based on lesion morphology, pathological severity, recurrence pattern, comorbidity, and voice needs.1,16,17,19,33
Recent clinical studies indicate that smoking, lesion size, pathological grade, and endoscopic factors influence recurrence and treatment outcome.30,31,33-37 A retrospective study of 351 patients found that smoking and lesion size influenced conservative treatment outcomes, while lesion size affected recurrence after surgery. 38 A recurrence risk model similarly identified smoking, age, and endoscopic factors as important determinants. 31 These findings support composite risk-based management rather than pepsin-guided treatment alone.
Laser-based approaches remain important in surgical care. Office-based laser surgery has been reported as safe and effective for vocal fold dysplasia and leukoplakia, with complete or partial regression in most cases. 39 A recent case series suggested that a single office-based blue laser session may achieve meaningful regression in selected dysplastic lesions, with outcomes related to dysplasia grade33. These approaches are relevant because they balance disease control with voice preservation.
Overall, pepsin-related information is best regarded as supportive biological context. In patients with recurrent lesions, clear reflux symptoms, objective reflux findings, or histologically confirmed pepsin positivity, clinicians may consider intensified reflux management, lifestyle modification, and closer follow-up. However, pepsin-guided therapy has not yet been proven to improve recurrence, malignant transformation, or voice outcomes. Thus, pepsin remains mechanistically informative and clinically suggestive, but not practice-defining.
Discussion
Principal Findings
The available evidence suggests that pepsin is biologically relevant in vocal fold leukoplakia and may function as both a marker of reflux exposure and a potential mediator of epithelial injury. The strongest current evidence supports associations with dysplasia severity, metabolic reprogramming, autophagy-related epithelial proliferation, and reflux-related mucosal stress, whereas diagnostic and therapeutic applications remain less established.5-8,14,15,25 After risk-of-bias and GRADE assessment, these conclusions should be interpreted with caution: current evidence is sufficient to support biological plausibility, but insufficient to support pepsin as an independent clinical decision-making tool.
Implications for Practice
From a clinical perspective, pepsin should currently be regarded as an adjunctive biomarker rather than a stand-alone diagnostic or treatment-selection tool. Endoscopic morphology, vascular pattern assessment, and histopathology remain the core of risk stratification. In selected patients with recurrent lesions, strong reflux background, or disproportionate lesion persistence, pepsin-related findings may still provide useful biological context and support closer follow-up or intensified reflux contro.3,4,16,18-20,26-29,32
Limitations of Current Evidence
The current evidence base remains limited by small sample sizes, methodological heterogeneity, inconsistent pepsin detection protocols, incomplete control of confounding factors, and a limited number of mechanistic studies. Much of the available evidence is observational or translational, and independent external validation remains insufficient. The inclusion of contextual review articles was restricted to background interpretation to avoid duplication of primary data. The heterogeneity of study design and outcome reporting also prevented quantitative meta-analysis and limited direct comparison across studies.5-8,14-17,19,20,31
Future Directions
Future studies should integrate standardized pepsin measurement with objective reflux testing, advanced imaging, histopathology, and longitudinal clinical outcomes. The most promising direction is likely a multimodal risk model in which pepsin contributes incremental value rather than functioning as a stand-alone biomarker.2,4,25-31,38,39
Conclusion
Pepsin is a biologically relevant link between laryngopharyngeal reflux and vocal fold leukoplakia. Current evidence supports its role as a marker of reflux exposure and a potential mediator of epithelial injury, but the certainty of evidence remains low to very low for most clinical applications. Pepsin should not be used as a stand-alone diagnostic, prognostic, or treatment-selection tool. Its present value lies in complementing established endoscopic and pathological assessment and in refining mechanistic understanding of lesion behavior. Prospective studies integrating objective reflux testing, standardized pepsin measurement, advanced imaging, pathology, and longitudinal outcomes are required before pepsin can be incorporated into routine clinical decision-making.
Footnotes
Ethical Considerations
This article is a review of previously published literature and does not involve human participants, human tissue, animal experiments, or identifiable patient information. Ethical approval was therefore not required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (No. 82471148).
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No new data were generated or analyzed in support of this review.
Artificial Intelligence Disclosure
During manuscript revision, an AI-based language assistance tool was used only for grammar, clarity, and editorial organization. No AI tool was used to screen studies, extract data, assess risk of bias, perform statistical analysis, or generate scientific conclusions. All authors reviewed the final manuscript and take full responsibility for the accuracy and integrity of the work.