
Abstract
Masculinization of the thyroid cartilage (“Adam’s apple”) is an important yet underreported component of gender-affirming surgery. Traditional augmentation techniques using autologous rib cartilage provide durable projection but introduce additional donor site morbidity. We describe a novel single-incision technique utilizing autologous thyroid alar cartilage grafts for thyroid cartilage augmentation. A 29-year-old transmale underwent augmentation via a high cervical incision. Bilateral thyroid alar cartilage grafts were harvested, fashioned into a neothryoid notch construct, and secured to the native cartilage to enhance anterior projection. The patient was discharged without complication and reported high satisfaction with both aesthetic and tactile outcomes at 15 days and 9.5 months postoperatively. This approach leverages the favorable properties of thyroid alar cartilage while avoiding the morbidity associated with distant donor sites. The technique allows for effective augmentation through a single, less-invasive operative field. Thyroid alar cartilage grafting represents a promising, less invasive alternative for masculinization of the thyroid cartilage in appropriately selected patients.
Introduction
The male thyroid cartilage (“Adam’s apple”) is a defining feature of the masculine neck. In men the thyroid cartilage is more pronounced with a narrow notch. While gender-affirming facial surgery describes approaches to either feminize or masculinize the face, modifying the profile of the thyroid cartilage is often an equally sought out feature. Techniques to augment or masculinize the thyroid cartilage have been described using autologous rib cartilage grafts.1,2 While these techniques provide durable augmentation, they require the morbidity of an additional donor site and, if performed with other procedures such as facial masculinization, the cartilage may be needed for these additional procedures (e.g. rhinoplasty). Thyroid alar cartilage grafts have been well described in laryngotracheal reconstruction.3,4 Here we describe for the first time, a novel single-incision technique for thyroid cartilage augmentation using thyroid alar grafts.
Case Report
A 29-year-old transmale presented for consideration of thyroid cartilage (“Adam’s apple”) augmentation. He began his transition 6 years prior and has been on intramuscular testosterone injections receiving 100 milligrams every 2 weeks during this time. While he has developed many male secondary sexual characteristics including a deeper voice, the prominence of his thyroid cartilage did not change. We counseled him on the various techniques for thyroid cartilage augmentation including autologous and cadaveric rib cartilage while providing them the option to try a novel approach through a single incision using thyroid alar cartilage grafts. After a thorough discussion of the risks, benefits, rationale, and possible expectations, they elected to proceed with this novel approach and written informed consent was obtained both for surgery and this publication.
General anesthesia was administered using a Laryngeal Mask Airway (LMA). This was chosen to permit ease of flexible fiberoptic laryngoscopy through a bronchoscope adapter should external localization of the endolaryngeal anatomy be required, as is done during chondrolaryngoplasty (“Tracheal shave”). A small shoulder roll was placed to slightly extend the neck. A 4-centimeter incision was placed in a high cervical skin crease at or near the cervicomental angle (Figure 1). Dissection was carried down to the midline raphe. The strap muscles retracted laterally to reveal the thyroid cartilage. A freer elevator can be used to elevate bluntly below the strap muscles to reveal most of the anterior face of the thyroid cartilage. A 15 blade is used to score the superior edge of the thyroid cartilage, and the perichondrium was elevated inferolaterally. The larynx was then rotated to the right. Inner perichondrium was elevated with cottle in the region of planned left alar graft. To demarcate a safe inferior extent of the graft before harvest, we placed a 22-gauge needle through the anticipated inferior extent of the thyroid alar cut while performing flexible bronchoscopy to confirm this location was above the laryngeal ventricle. Once confirmed the needle was removed and an oscillating saw was used to harvest the graft. We the repeated this on the right side to harvest a symmetric alar graft. We rinsed the grafts in saline and sutured them together to form a new thyroid notch with 4-0 prolene suture as shown in Figure 1. We then affixed this construct onto the thyroid cartilage with 4-0 prolene suture in 4 quadrants overlying and augmenting the native thyroid notch (Figure 2). The strap muscles were then closed over the midline with 3-0 vicryl suture followed by 5-0 monocryl subcuticular closure and skin glue. The patient was discharged home from the post-anesthesia care unit without complication. The patient was seen 15 days later very satisfied with the visible and tactile aspect of their result. This satisfaction and appearance were durable at their 9.5 months follow-up as well (Figure 2) without any chance in voice or flexible laryngoscopic findings. The Glasgow Benefit Inventory, a validated post-interventional questionnaire, was used to quantify the procedural impact on his quality of life.
5
Scores range from -100 to +100 with zero indicating no benefit and +100 maximum benefit. This patient scored a 33.3. Thyroid alar cartilage harvest and construct. (A) Incision in a crease nearest the cervicomental angle; (B) Exposure of thyroid cartilage; (C) Right alar graft harvest; (D) Left alar graft harvest; (E) Bilateral alar grafts; (F) Side profile showing thickness of graft; (G) Anterior face of grafts sutured together with 4-0 prolene suture; (H) Posterior face of construct; (I) Lateral or oblique view of construct. C – cricoid, L – Left alar harvest side, R – Right alar harvest site, V – thyroid notch Placement of thyroid augmentation construct and outcomes. (A) Construct sutured in place overlying native thyroid notch; (B) Closed incision; (C) Pre-operative neck profile. Red line highlights contour at level of thyroid notch; (D) 15 days post-operative neck profile. Green line highlights new contour of thyroid notch; (E and F) Neck profile 2.5 and 9.5 months post-operatively with green line highlighting contour from augmented thyroid notch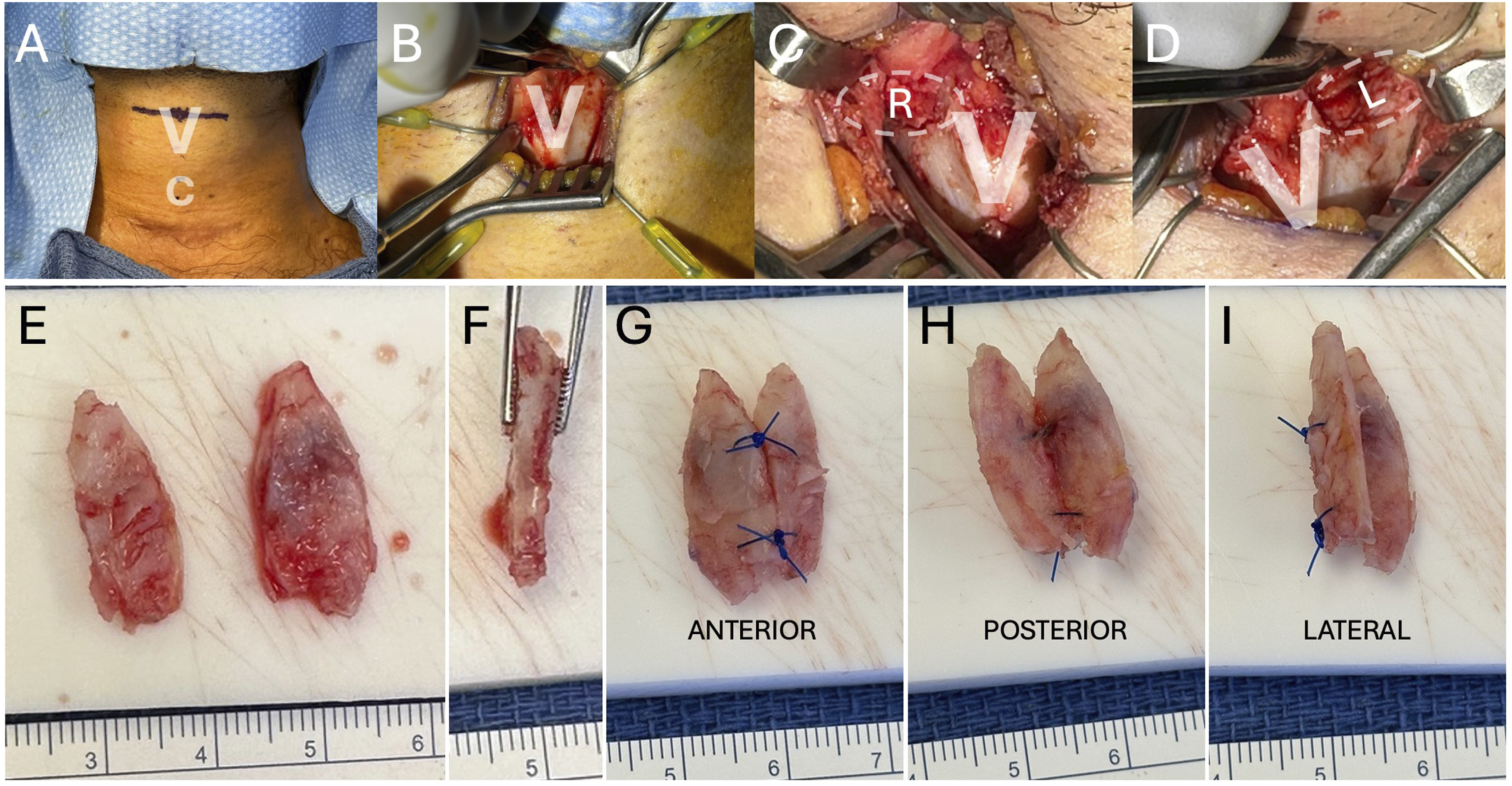

Discussion
Use of thyroid alar cartilage for laryngotracheal reconstruction is well described. In comparison to other cartilage grafts for this purpose, autologous thyroid alar cartilage compares favorably. 6 Additionally the donor site discomfort and morbidity of ear and rib cartilage are also well documented problems. Ideally, graft harvest should have minimal donor site morbidity and be obtained through the same operative incision through which the graft is to be placed. The same advantages that thyroid alar cartilage provides for laryngotracheal reconstruction apply to thyroid cartilage augmentation. Specifically, the incision and exposure are all the same. There is no added donor site morbidity. The goal of thyroid cartilage augmentation is to increase the prominence of the thyroid cartilage and notch. The lateral thyroid ala does not contribute to the prominence, so can be harvested without aesthetic consequence so long as the anterior midline thyroid cartilage (notch) is left intact. During harvest, one should take care to elevate as much inner perichondrium as possible so the cartilage graft can be removed easily after the cuts are made. A drawback to this technique may be the unfamiliarity with the external laryngeal landmark correlates to the endolaryngeal structures in the region of the mid to posterior thyroid lamina. If there is concern that the inferior extent of the graft harvest may be too inferior and close to the apex of the laryngeal ventricle, we recommend placing a needle through the cartilage while visualizing it endoluminal with a flexible fiberscope to be sure you are in a safe region above the laryngeal ventricle. Cutting too low at the level of the laryngeal ventricle may pose of risk of laryngotomy into the airway. Such a defect would need primary repair and considerations for post-operative overnight stay with precautions and antibiotics. The ossification of the thyroid cartilage can be unpredictable. If the cartilage is soft, one can attempt to harvest the grafts with a scalpel (number 15 blade). However, if the cartilage is ossified, we recommend using an oscillating saw or pieozoelectric (ultrasonic) cutter. Anchoring the neothyroid notch construct to the thyroid cartilage is important to prevent migration in the short-term. When sewing the construct in place, it is important to avoid throwing sutures through the thyroid cartilage that may be in close range to the anterior commissure and vocal folds. The vocal folds anchor to the thyroid cartilage anteriorly midway between the bottom of the thyroid notch and the inferior border of the thyroid cartilage. It is optimal to sew the construct to the superior and inferior ledges of the thyroid cartilage to avoid the critical region of the anterior commissure. Suture in close proximity to this region could result in unwanted voice change for a surgery focused on aesthetic change.
Traditional rib cartilage grafts used for thyroid cartilage augmentation reportedly can achieve around 5-7 millimeters of added projection. 2 Here we can achieve similar results with thyroid alar cartilage grafts as shown in Figure 1. Most important is to achieve the desired outcome that your patient seeks. Here our patient wanted a larger “Adam’s apple” that looked and felt more prominent in a natural way. We were able to achieve this without complication and less morbidity with this novel technique.
Technical Pearls: 1. Use of a shoulder roll can be helpful but one should avoid using a large shoulder roll. If you are trying to hide the incision high in or near the cervicomental crease, less neck extension helps keep the larynx higher and closer to this more desirable incision site. This helps reduce dissection and the need for excessive skin retraction. 2. Use of an LMA with bronchoscopy adapter affords the ability to check the endoluminal airway before and after thyroid alar cartilage graft harvest ensuring a safe approach and execution. 3. Ensure adequate inferior elevation of the perichondrium along the thyroid alar inner and outer surfaces to accommodate the planned grafts. 4. Use of a 22 gauge needle, or smaller, inserted through the thyroid cartilage in the region of the inferior margin of the planned graft helps to confirm the location is above the laryngeal ventricle and therefore safe from inadvertent damage, 5. Anchor the neothyroid notch construct to the superior and inferior borders of the thyroid cartilage. Avoid sutures along the mid body of the thyroid cartilage to avoid inadvertent damage to the vocal folds.
Conclusion
A more prominent thyroid cartilage is a key feature to gender congruence for transmale patients. This can be achieved traditionally with autologous rib cartilage. Here we achieve a satisfactory outcome using a single-incision and thyroid alar cartilage grafts in a 29-year-old transmale patient.
Footnotes
Ethical Considerations
All authors comply with all ethical procedures set out by UC San Diego Health and Sage publishing. There is no plagiarism or breaches in ethical principals.
Consent to Participate
Written Informed Consent Obtained.
Author Contribution
Elisa Bass, BA – literature review, writing.
Jeffrey D. Bernstein, MD – literature review, writing.
Andrew M. Vahabzadeh-Hagh, MD – performed the surgery and provided clinical care.
Wrote and edited the manuscript. Made figures.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Available on request.
IRB Protocol
IRB #813401 was determined exempt. Letter from UCSD IRB provided as supplement.