
Abstract
Surgical resection remains the primary treatment modality for well-differentiated thyroid carcinoma. However, hypoglossal nerve injury following thyroidectomy represents a rare complication. We report a case of bilateral hypoglossal nerve palsy in a 57-year-old female patient who underwent bilateral total thyroidectomy with neck dissection and thyroglossal duct cyst excision under general anesthesia. Comprehensive imaging and electrophysiological studies confirmed bilateral hypoglossal nerve dysfunction, although surgical re-exploration revealed anatomically intact nerves. Despite empirical steroid treatment, neurological improvement was limited. The patient subsequently underwent intensive, multidisciplinary neurorehabilitation. Over the following months, swallowing function gradually improved, allowing a return to oral intake, although mild dysarthria persisted. This case presents a complex and rare neurological complication following thyroid surgery. Although thyroidectomy techniques are well-established, preoperative assessment should carefully consider the potential risk factors for hypoglossal nerve injury to optimize surgical outcomes.
Introduction
Thyroid carcinoma is a prevalent malignancy with increasing incidence in recent years. 1 Surgical resection remains the primary curative treatment for most well-differentiated thyroid carcinomas, with an excellent prognosis reflected by a 5-year relative survival rate of approximately 98.5%. 2 While postoperative complications such as superior and recurrent laryngeal nerve injuries are well-documented, hypoglossal nerve (cranial nerve XII) injury is exceedingly rare. The hypoglossal nerve (cranial nerve XII) provides motor innervation to all intrinsic tongue muscles, three extrinsic tongue muscles (genioglossus, hyoglossus, and styloglossus), and the geniohyoid muscle. 3 Injury to this nerve typically manifests as ipsilateral tongue deviation, dysarthria, dysphagia, tongue atrophy, and unintentional tongue biting. 4 Here, we present a rare case of bilateral hypoglossal nerve palsy following bilateral total thyroidectomy with neck dissection and excision of a thyroglossal duct cyst under general anesthesia. This case report was prepared in accordance with the CARE guidelines. 5
Case Description
A 57-year-old woman with no significant prior medical history was diagnosed with bilateral thyroid nodules during a routine health examination. Fine-needle aspiration biopsy confirmed papillary thyroid carcinoma with bilateral cervical lymph node metastases. On November 6, 2023, she underwent bilateral total thyroidectomy, central and lateral neck dissection, and excision of a concomitant thyroglossal duct cyst under general anesthesia. Intraoperatively, a 0.6 × 0.5 cm mass was palpated at the lower pole of the left thyroid gland, and a 0.8 × 0.5 cm mass at the lower pole of the right thyroid gland. Both masses were hard in consistency, with ill-defined margins, grayish-white on cut surface, no obvious capsule, no extrathyroidal extension, and no adhesion to the recurrent laryngeal nerve. Small lymph nodes were palpable in the bilateral central compartments and bilateral cervical levels III and IV. A nodule was palpated in the right paramedian anterior cervical region, below the hyoid bone; it was hard and solid, slightly adherent to surrounding tissues, and extended upward posterior to the hyoid bone. During the procedure, the recurrent laryngeal nerve, vagus nerve, and phrenic nerve were exposed and protected. Immediately after extubation, the patient developed acute dyspnea and pronounced stridor. Neurological examination showed grade 4 muscle strength in all limbs. Despite intravenous dexamethasone, her respiratory distress worsened, necessitating an emergent bedside tracheostomy. The patient had no history of allergies, substance use, smoking, or alcohol consumption, and was well-nourished.
On postoperative day 1, she exhibited symptoms suggestive of bilateral hypoglossal nerve palsy: profound dysphagia, unintelligible speech, and severely restricted tongue movement. Cranial CT and MRI revealed no structural lesions. A course of dexamethasone provided no significant improvement.
On postoperative day 14, surgical exploration of the bilateral hypoglossal nerves was performed; both nerves were found to be anatomically intact, with no evidence of transection or hematoma. Further tests, including for myasthenia gravis and paraneoplastic antibodies, were negative.
A neurology consultation on postoperative day 18 established a diagnosis of bulbar palsy. A two-week trial of intravenous methylprednisolone (80 mg/day) was initiated but discontinued due to lack of efficacy. Recommendations from head and neck surgery included excluding central lesions and starting early rehabilitation and neurotrophic therapy. The tracheostomy tube was removed 6 weeks after the surgery.
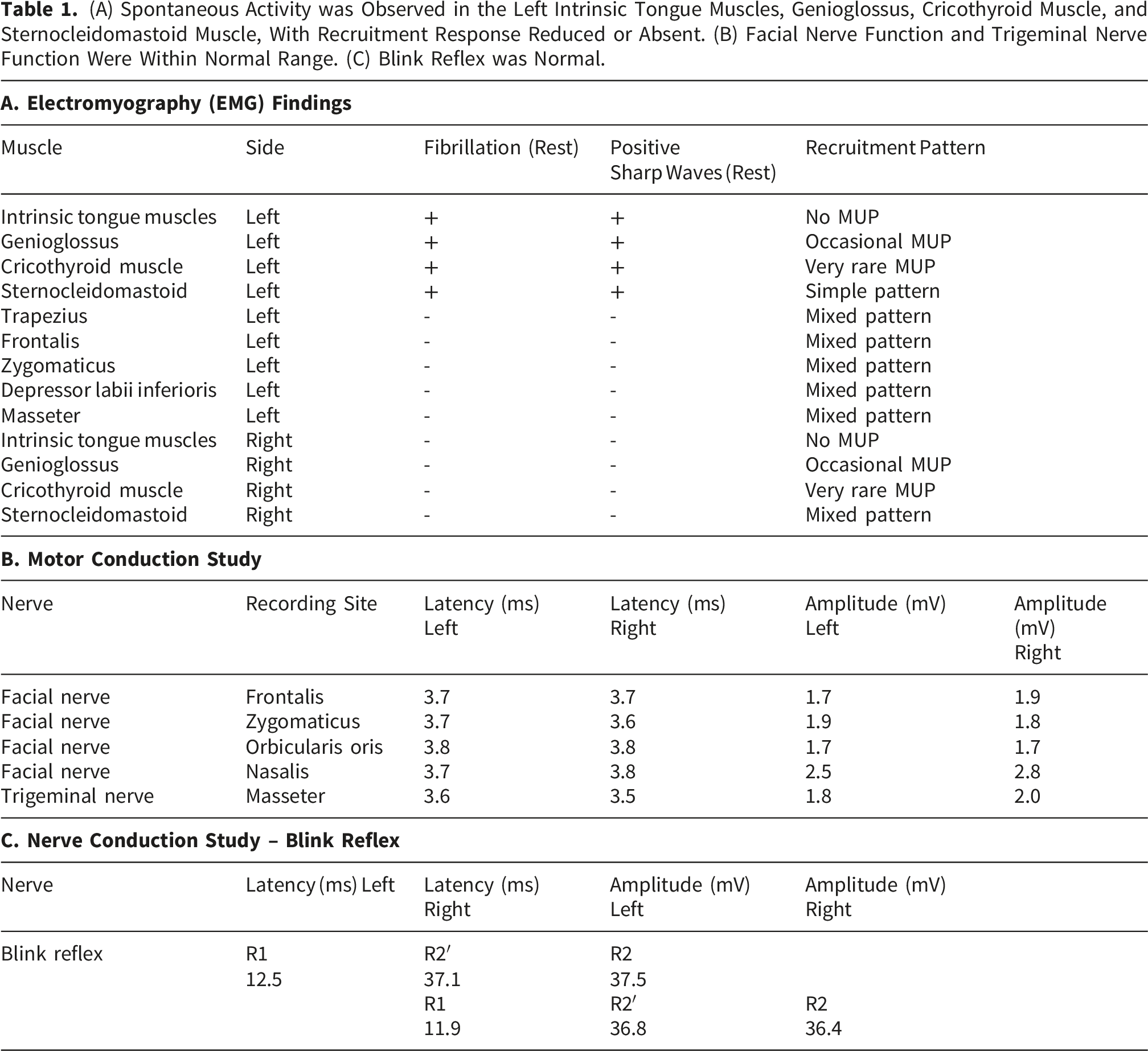
Electromyography examination indicated axonal neurogenic damage (Table 1): • Bilateral hypoglossal nerves (intrinsic tongue and genioglossus branches) • Bilateral superior laryngeal nerve (cricothyroid branch) • Left accessory nerve (sternocleidomastoid branch) (A) Spontaneous Activity was Observed in the Left Intrinsic Tongue Muscles, Genioglossus, Cricothyroid Muscle, and Sternocleidomastoid Muscle, With Recruitment Response Reduced or Absent. (B) Facial Nerve Function and Trigeminal Nerve Function Were Within Normal Range. (C) Blink Reflex was Normal.
Flexible endoscopic evaluation of swallowing (FEES) revealed: • Asymmetric laryngeal edema (severe left/moderate right arytenoid swelling) • Epiglottic retroflexion with pharyngeal wall adhesion • Impaired left vocal cord adduction and arytenoid mobility • Trace aspiration across all food consistencies (Murry secretion score: 2)
Starting December 22, which was the 7th week after the surgery, the patient received intensive oromotor and swallowing rehabilitation, including: • Tongue pressure biofeedback • Lingual resistance exercises in multiple directions • Articulation and mandibular strengthening • Progressive diet training
She also received oral mecobalamin, vitamin B1, and vitamin B6.
Marked atrophy of the lingual musculature and limited tongue extension could be observed in the patient when she was admitted to Rehabilitation Department on December 22nd (Figure 1A). During the patient’s rehabilitation process, we used tongue pressure measurement to objectively assess the recovery of the patient’s lingual muscle strength (See the supplementary materials for details). Serial documentation showed gradual improvement in tongue mobility and function (Figure 1B–D). (A) The patient has limited tongue extension when she was admitted to Rehabilitation Department on December 22nd. (B) Changes in tongue pressure while the tongue extended toward the middle during rehabilitation. (C) Changes in tongue pressure while the tongue extended to the left during rehabilitation. (D) Changes in tongue pressure while the tongue extended to the right during rehabilitation.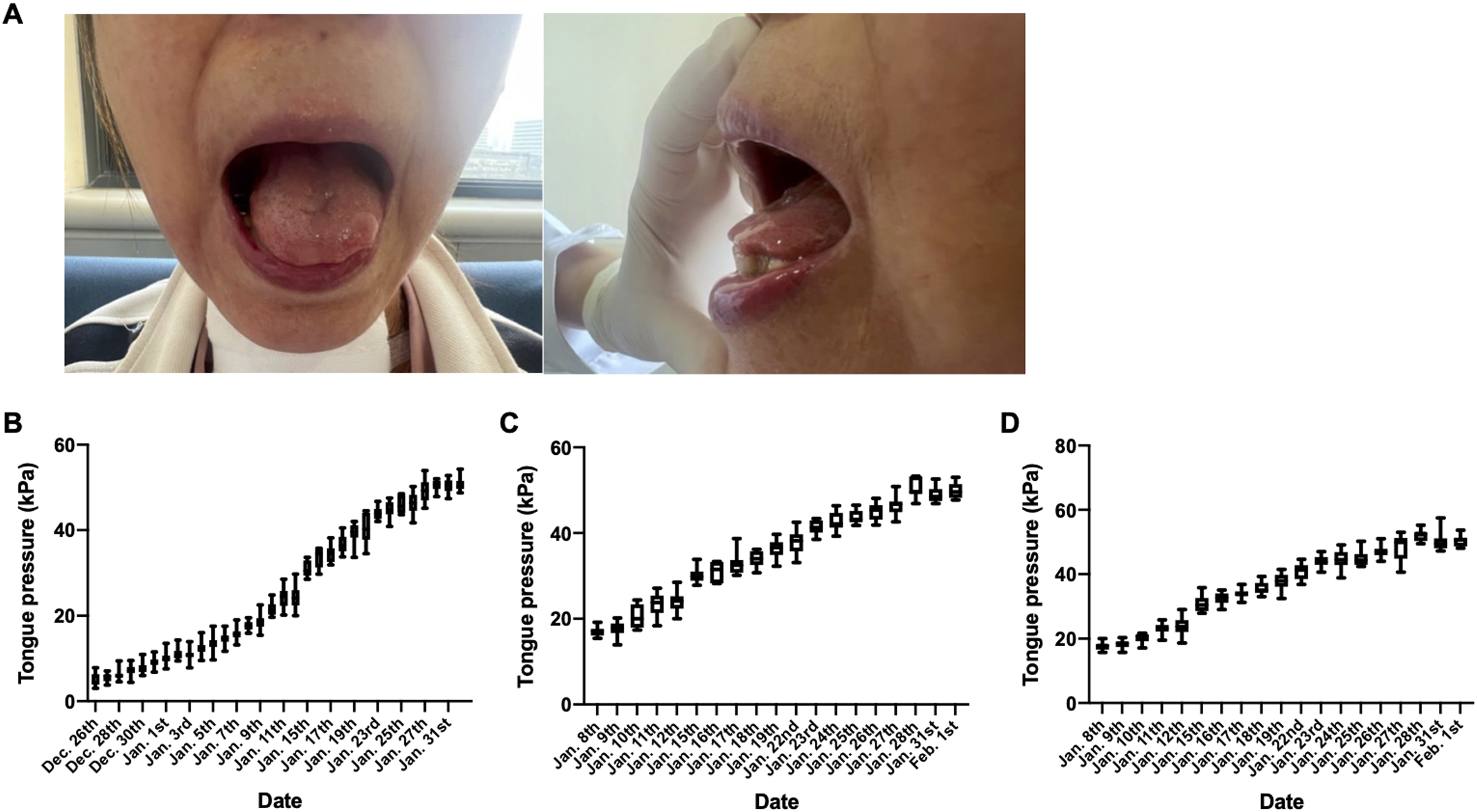
At the six-month follow-up, the patient had achieved full oral intake despite mild residual dysarthria. One year postoperatively, speech and swallowing showed further improvement but had not returned to preoperative baselines. The patient was satisfied with her functional progress; however, she declined repeat EMG and FEES examinations.
Discussion
This report presents the first documented case of bilateral hypoglossal nerve palsy following bilateral total thyroidectomy with neck dissection and thyroglossal duct cyst excision. While hypoglossal nerve injury after thyroid surgery remains uncommon, with only three cases of unilateral palsy previously reported, this bilateral presentation represents a novel clinical entity that warrants careful analysis.
The hypoglossal nerve (cranial nerve XII), which provides motor innervation to both intrinsic and extrinsic tongue muscles, is susceptible to injury from diverse etiologies. These include anatomical variations along its course, vascular compromise, inflammatory processes, infectious agents, traumatic insults, and neoplastic involvement. 3 This patient’s bilateral hypoglossal nerve palsy likely resulted from multiple contributing factors. Anesthesia-related mechanisms included potential nerve compression between the endotracheal tube and adjacent rigid structures (cervical vertebrae, thyroid cartilage, and hyoid bone), particularly given the nerve’s vulnerable anatomical course. Several intraoperative anesthetic factors may have compounded this risk: prolonged hemodynamic instability, extended surgical duration, endotracheal tube cuff overinflation or malpositioning, and repeated laryngoscopy with lateral tongue base pressure. The nerve’s superficial position beneath the mandibular angle and proximity to the hyoid bone’s greater cornu further increased susceptibility to injury during airway management, particularly as the patient underwent two general anesthetics within a short timeframe.4,6,7
Tapia’s syndrome occurs in a small number of patients following invasive airway manipulation. Tapia’s syndrome was first described in 1904 by the Spanish otolaryngologist Antonio Garcia Tapia and is characterized by hoarseness and dysphagia, believed to result from mechanical trauma to the cranial nerves X and XII. Cases are most commonly reported after various types of surgery requiring orotracheal intubation under general anesthesia, including cardiac, neurosurgical, orthopedic, and otolaryngologic procedures. 8 Here, we reference Tapia syndrome not as a confirmed diagnosis, but as a conceptual framework to systematically consider differential causes of concurrent dysphagia and dysarthria. Based on the EMG results, the diagnosis is currently less likely given the absence of recurrent laryngeal nerve involvement in the patient.
Surgical factors equally contributed to this complication. The extensive dissection required for bilateral cervical lymph node clearance and thyroglossal cyst resection created multiple potential injury mechanisms: direct mechanical traction, thermal damage from energy devices, and compressive hematoma formation. The hypoglossal nerve’s anatomical relationship to these surgical fields, coursing medial to the internal jugular vein and descending between the internal carotid artery and jugular vein before passing beneath the posterior belly of the digastric muscle, renders it particularly vulnerable during such procedures. According to the patient’s surgical records, intraoperative exposure and protection of the hypoglossal nerve were not explicitly documented. Consequently, a potential contribution of surgical factors to the observed neurological findings cannot be entirely excluded.
The patient’s anatomy, such as a potentially prominent hyoid bone or robust neck musculature, may have increased susceptibility. Furthermore, the possibility of a hereditary neuropathy with liability to pressure palsies (HNPP) was considered, an autosomal dominant generalized demyelinating neuropathy, may increase the susceptibility of all nerves to compression, including cranial nerves. 9 The diagnosis of HNPP can be genetically confirmed through PMP22 mutation analysis. Additionally, electrophysiological findings of reduced common peroneal nerve conduction velocity may provide supportive evidence for this diagnosis, as they reflect the characteristic diffuse neural vulnerability observed in HNPP. The bilateral nature of the patient’s nerve damage, along with electrophysiological evidence of additional cranial nerve involvement, suggests a more generalized neuropathic vulnerability or a common mechanism of injury, such as prolonged compression or stretch during positioning. Regrettably, neither of these diagnostic tests was performed in this patient, leaving the potential HNPP diagnosis unverified. Had the patient been diagnosed with HNPP preoperatively, special perioperative considerations would have been warranted, including meticulous attention to patient positioning to minimize nerve compression and optimization of surgical duration to reduce prolonged pressure exposure. Such preventive measures would be particularly crucial for procedures involving vulnerable neural structures such as the hypoglossal nerve.
Although thyroidectomy is a well-established surgical procedure, preoperative assessment must rigorously evaluate risk factors associated with potential hypoglossal nerve injury. Intraoperatively, strategies to mitigate iatrogenic harm should be systematically implemented, including minimizing tracheal intubation related trauma, optimizing operative efficiency to reduce overall surgical duration, meticulous identification and protection of the hypoglossal nerve throughout dissection, and careful patient positioning to prevent nerve compression. These evidence-informed measures may enhance surgical safety and reduce the incidence of postoperative hypoglossal nerve dysfunction.
Regarding prognostic outcomes, current evidence suggests that most patients with hypoglossal nerve injury achieve complete functional recovery within approximately three months6,7,10,11 when treated with corticosteroids and neurotrophic medications. The present case demonstrates a similar favorable trajectory, with the patient showing marked improvement in tongue mobility, speech articulation, and swallowing function following a comprehensive therapeutic regimen combining pharmacologic intervention and targeted rehabilitation therapy. These clinical improvements were particularly notable given the bilateral nature of the nerve injury in this case. The patient has achieved near-complete recovery to the preoperative functional status, with only minimal residual deficits persisting. This gradual yet incomplete recovery pattern suggests persistent hypoglossal nerve dysfunction, consistent with the bilateral nature of the injury and emphasizing the need for extended rehabilitation in such cases.
Conclusions
Bilateral hypoglossal nerve palsy following thyroid surgery is a rare and severe complication that may arise from a combination of anesthetic, surgical, and patient-specific factors. A high index of suspicion, timely diagnostic investigations, and early multidisciplinary management are crucial. Rehabilitation plays a central role in functional recovery. This case underscores the need for careful preoperative assessment, including evaluation of anatomical and genetic risk factors for nerve injury, and highlights the importance of tailored surgical and perioperative strategies to minimize neurological complications.
Supplemental Material
Supplemental Material - Bilateral Hypoglossal Nerve Palsy After Thyroidectomy: A Case Report
Supplemental material for Bilateral Hypoglossal Nerve Palsy After Thyroidectomy: A Case Report by Yuwei Gu, Rongrong Lu, Tingwei Wang and Junfa Wu in Ear, Nose & Throat Journal.
Supplemental Material
Supplemental Material - Bilateral Hypoglossal Nerve Palsy After Thyroidectomy: A Case Report
Supplemental material for Bilateral Hypoglossal Nerve Palsy After Thyroidectomy: A Case Report by Yuwei Gu, Rongrong Lu, Tingwei Wang and Junfa Wu in Ear, Nose & Throat Journal.
Footnotes
We are grateful to the patient P.C. for agreeing to be the subject of this manuscript.
Ethical Considerations
Our institution does not require ethical approval for reporting individual case.
Consent to Participate
Written informed consent was obtained from the patient.
Consent for Publication
Informed consent for publication was provided by the participant.
Author Contributions
(I) Conception and design: Junfa Wu. (II) Administrative support: Junfa Wu. (III) Provision of study materials or patients: Yuwei Gu, Rongrong Lu. (IV) Collection and assembly of data: Yuwei Gu, Tingwei Wang. (V) Data analysis and interpretation: Yuwei Gu. (VI) Manuscript writing: All authors. (VII) Final approval of manuscript: All authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the project of Shanghai Commission of Science and Technology of China (No. 19411968700) and the project of Yangpu District Health System of Shanghai (YPQ202505).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.