
Abstract
Solitary fibrous tumor (SFT) is a rare mesenchymal neoplasm, and its involvement at the orbitonasal junction is exceptionally uncommon. We report an extremely rare case of atypical SFT arising at the orbitonasal junction in a patient with an 18-year history of recurrent left orbital mass who had undergone multiple excisions and eventual enucleation, and finally presented with extensive osteolytic destruction extending into the nasal cavity and paranasal sinuses. After preoperative evaluation, a combined surgical approach using Lynch incision (transfacial medial orbitotomy) and endoscopic endonasal resection successfully achieved complete tumor removal and orbital reconstruction. Histopathology and immunohistochemistry (STAT6+, CD34+, Ki-67 20%) confirmed the diagnosis of atypical SFT.This case enriches the clinical literature on this rare entity and offers a surgical reference for orbitonasal SFT.
Keywords
Case Presentation
A 71-year-old woman presented with an 18-year history of recurrent swelling at the left orbitonasal junction, initially with proptosis and restricted ocular motility. Over the past month, the swelling had progressively worsened, along with left nasal foreign body sensation, epistaxis, epiphora, and headache.
She underwent surgical resections of the left orbital mass at outside hospitals in 2007, 2015, and 2018, without histopathological examination at those times. In 2020, due to further recurrence, she underwent left orbital mass resection and enucleation of the left eye at our department, with histopathology revealing an atypical solitary fibrous tumor. The patient did not receive any radiotherapy or chemotherapy.
The patient had a history of hypertension, hyperlipidemia, and hyperthyroidism, and was on long-term medications including valsartan, metoprolol, triamterene, methimazole, and atorvastatin.
Physical examination showed an absent left globe, swelling of the skin at the left orbitonasal junction, and a palpable subcutaneous mass that was firm, poorly mobile, and ill-defined (Figure 1A). Nasal endoscopy revealed a dark-red, eroded mass at the posterior portion of the left middle nasal meatus. Patient’s preoperative condition: swelling at the nasal-orbital junction (1A), preoperative imaging: cranial CT (1B), coronal head MRI (1C)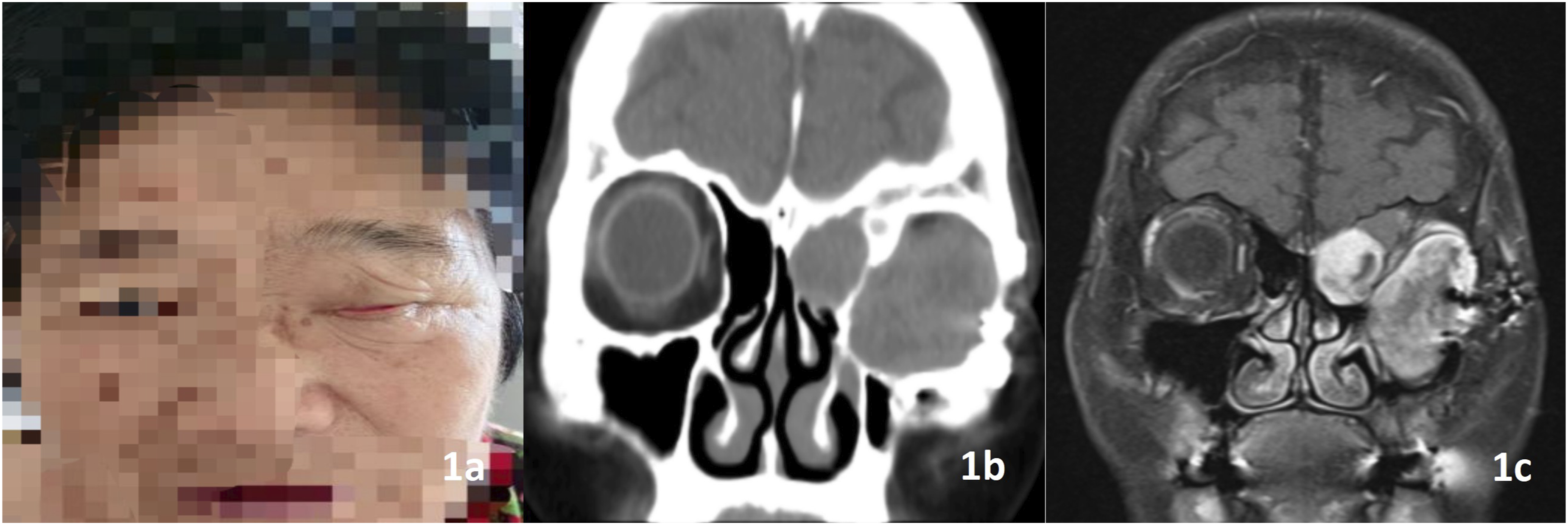
Imaging findings: CT of the paranasal sinuses demonstrated a soft-tissue mass in the left orbit with involvement of the left maxillary, frontal, and ethmoid sinuses accompanied by bony destruction (Figure 1B). Orbital MRI revealed fluid accumulation in the left maxillary, ethmoid, and frontal sinuses with heterogeneous peripheral enhancement, as well as swelling of the facial subcutaneous soft tissues (Figure 1C).
Therapeutic Intervention
1. Surgical Method
A combined endoscopic endonasal and transfacial approach was performed. The procedure consisted of three components: (1)endoscopic anterior ethmoidectomy to expose the tumor extending from the orbit into the ethmoid sinus; (2)left facial Lynch incision combined with a supraorbital incision to access the orbit and maxillary sinus; (3)en bloc resection of the orbitonasal tumor, including the involved nasolacrimal duct and bone margins, followed by orbital reconstruction.
2. Surgical Procedure
Nasal mucosa was decongested with adrenaline-soaked cottonoids.Under 0° endoscopy, the left anterior ethmoid cells were opened, revealing tumor herniation from the inferomedial orbital wall into the ethmoid sinus with compression of the nasofrontal duct. The sinus ostium was widened, secretions were suctioned, and the cavity was temporarily packed.
A left Lynch incision combined with a supraorbital incision was then made. The skin incision extended from 5 mm below the orbital floor along the left nasal sidewall, around the ala to the nasolabial fold and columella, then through the upper lip and gingivolabial mucosa to the first molar. The superior limb was extended along the brow to the lateral canthus. The facial flap was elevated to expose the orbital rim and anterior maxillary wall (Figure 2A). Surgical procedure:Incision design and exposure of the orbital rim and maxillary wall(A);Tumor invasion of the orbit and sinonasal tract(B);Margin drilling and orbital preparation(C)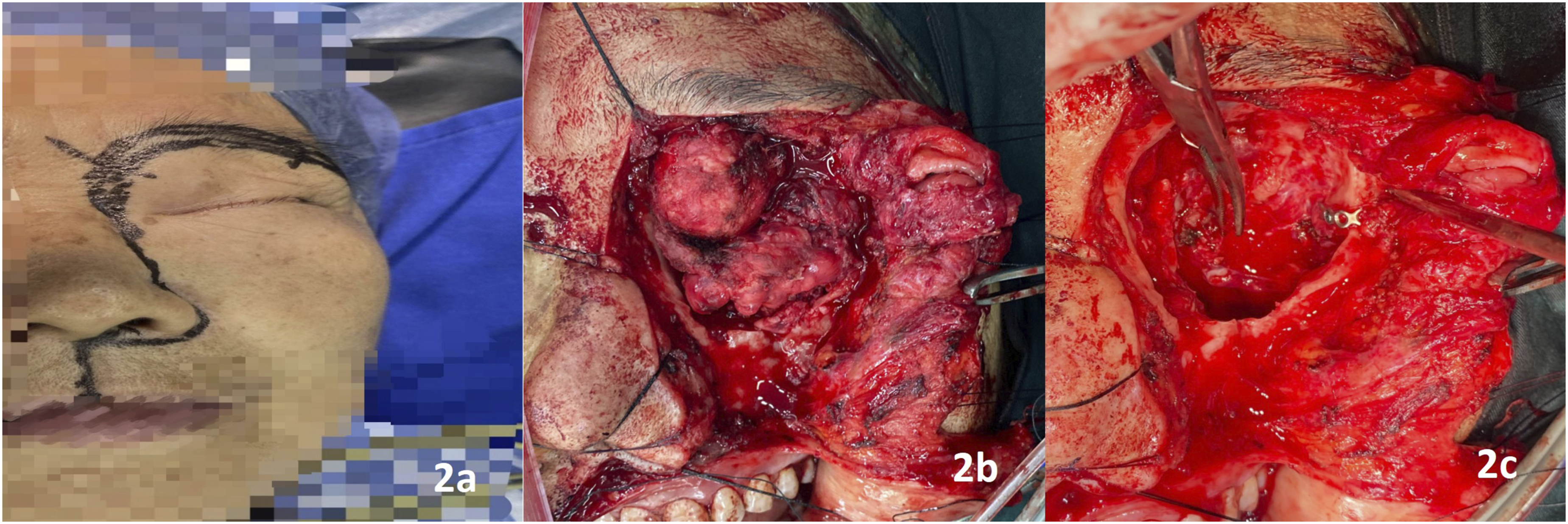
The orbit was occupied by a lobulated, ill-defined mass; the left globe had been previously enucleated. The anterior medial orbital wall was destroyed, creating a direct communication with the nasal cavity, and the nasolacrimal duct was dilated (Figure 2B). The tumor was dissected bluntly along the orbital walls. The superior wall was intact. On the lateral wall, titanium plates and screws from prior surgery were removed due to fibrous adhesion. The medial wall showed bone destruction involving the anterior ethmoid cells and the nasolacrimal duct, with tumor extension into the maxillary sinus. The infraorbital wall was partially eroded. The involved nasolacrimal duct and intranasal tumor components were completely excised. Irregular bone along the orbital walls was drilled to healthy margins (Figure 2C). The orbit was reconstructed and closed in layers. Estimated blood loss was 150 mL.
3. Postoperative Outcome
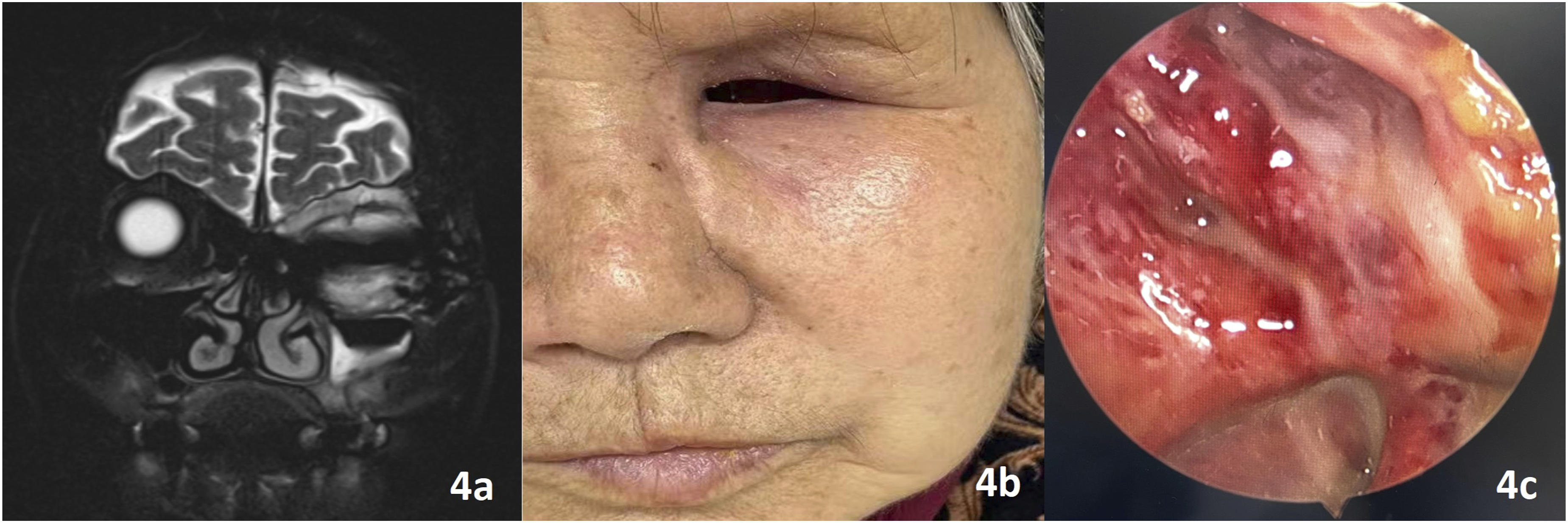
Histopathological examination of the resected specimen (5.0 × 6.5 cm) confirmed an atypical solitary fibrous tumor with focal malignant transformation (Figure 3A), showing high cellularity, nuclear atypia, mitotic count >4/HPF (up to 10/HPF in hotspots), and foci of necrosis and hemorrhage. Immunohistochemistry was positive for STAT6, CD34, CD99, Bcl-2, and vimentin, with a Ki-67 index of 20%, and negative for CK, SMA, desmin, and S-100. The wound healed primarily (Figure 3B and C). Facial nerve function was House-Brackmann grade I. The patient remains under close surveillance. During the short-term follow-up period of 8 months post-surgery, MRI and nasal endoscopy showed no overt signs of recurrence or metastasis(Figure 4). Postoperative condition: The completely removed tumor tissue(3A); Sutured surgical margin(3B); Well-healed incision at postoperative day 7(3C) Follow-up assessment: Head MRI performed at 2 months after discharge(4A); Skin incision healing at 5 months after discharge(4B);Nasal endoscopic view(4C).
Discussion
Solitary fibrous tumor (SFT) is a rare mesenchymal neoplasm of fibroblastic origin, first described in the pleura in 1931,with an overall incidence of 1–2 per million.Extrapleural sites are increasingly recognized, accounting for approximately 6–18% of all SFTs, with the oral cavity, salivary glands, and sinonasal tract being most frequently involved. 1 SFTs involving the orbitonasal junction are exceptionally rare, with fewer than 10 cases reported in the literature. They predominantly affect adults aged 20–70 years with a slight male predominance. 2 Histologically, SFT is characterized by spindle cell proliferation in a collagenous stroma with a “patternless pattern” and branching “staghorn” vessels. The defining molecular event is the NAB2-STAT6 gene fusion, reliably detected by diffuse nuclear STAT6 immunoreactivity, a surrogate marker with diagnostic sensitivity exceeding 95%. 3 In this discussion, we focus on three aspects highlighted by this case: the biological behavior of long-standing SFT, the anatomical complexity of the orbitonasal junction, and the rationale for the combined surgical approach.
1. Long-Standing SFT With Four Recurrences: The Critical Role of Early Pathological Diagnosis
SFTs exhibit unpredictable behavior: most follow an indolent course, but a subset shows aggressive features (local infiltration, recurrence, and even malignant transformation with metastatic potential). 4 Compounding this challenge, recurrences can occur after prolonged latency—sometimes decades post-resection—with reported intervals of 6–15 years. 5 The present case is particularly instructive in this regard. Our patient underwent four recurrences over an 18-year course, with the first three surgeries performed at outside hospitals without histopathological examination. This delay in diagnosis meant that the tumor’s true nature—and its progressive evolution toward malignancy—remained unrecognized for nearly two decades. When the tumor was finally diagnosed as atypical SFT in 2020 after enucleation, it had already exhibited histological features of malignant transformation, including high cellularity, significant nuclear atypia, mitotic activity up to 10/HPF, foci of necrosis, and a Ki-67 index of 20%. What makes this case particularly instructive is the sheer length of the diagnostic odyssey—18 years from first presentation to definitive histology. The lesson is not merely academic: a recurrent mass in this region, even if it appears indolent or has been previously resected without complication, should prompt immediate histopathological evaluation with immunohistochemistry. Waiting for recurrence, as happened here, risks missing the window for less morbid surgery and allows potential malignant transformation to proceed unchecked.
2. Anatomic Challenges at the Orbitonasal Junction
The orbitonasal junction is anatomically complex, with the orbit communicating with the nasal cavity and paranasal sinuses via the nasolacrimal canal, ethmoidal air cells through the lamina papyracea, and the inferior orbital fissure. The lamina papyracea is exceptionally thin and fenestrated, offering minimal resistance to tumor spread. 6 This vulnerability explains why orbitonasal communicating tumors, though comprising only 2.0% of primary orbital neoplasms, have a strikingly high malignancy rate of 82.4%. 7 Critical neurovascular structures in this region include the anterior and posterior ethmoidal arteries (branches of the ophthalmic artery), the nasociliary nerve (providing sensory innervation to the medial canthus and nasal dorsum), and the optic nerve. 8 In our patient, epiphora resulted from nasolacrimal duct obstruction, and headache likely reflected sinus involvement. During surgery, we carefully preserved uninvolved neurovascular structures, completely excised the obstructed nasolacrimal duct, and drilled bony margins until healthy tissue was confirmed to minimize residual disease.
3. Lynch Incision Plus Endonasal Endoscopy: A Strategic Combination for Complete Tumor Clearance and Orbital Reconstruction
Surgery remains the cornerstone of treatment for localized SFTs, and achieving negative (R0) margins is the most critical determinant of favorable long-term outcome. 9 In the present case, the tumor’s involvement of both the orbit and the sinonasal tract posed a formidable surgical challenge: no single conventional approach could adequately expose both compartments simultaneously. 10 Traditional transcutaneous medial orbitotomy (Lynch incision) provides excellent access to the medial orbital wall, the orbital apex, and the anterior ethmoid region, but it offers limited visualization of the posterior ethmoid sinuses, maxillary sinus, and nasal cavity. 11 Conversely, the endoscopic endonasal approach is well-suited for tumors located predominantly in the medial and inferior orbit as well as the paranasal sinuses, but it struggles to access the anterior orbit, the supraorbital region, and the orbital apex when the optic nerve is shifted medially. 12 This complementary limitation of the two approaches informed our decision to adopt a combined strategy: endoscopic endonasal access was used to address tumor extension into the ethmoid and maxillary sinuses and to relieve compression of the nasofrontal duct, while the Lynch incision provided a wide, direct field for resecting the orbital component, reconstructing the orbital walls, and achieving complete tumor clearance under direct visualization. 13 This combined approach allowed for en bloc tumor resection with negative margins (R0), as confirmed by histopathological examination. Importantly, it also facilitated simultaneous orbital reconstruction using bone drilling to achieve healthy margins. The postoperative recovery was uneventful, with no wound complications or functional deficits. This case demonstrates that for tumors straddling the orbitonasal junction with extensive bone destruction, a carefully planned combined approach—transfacial medial orbitotomy via Lynch incision plus endoscopic endonasal surgery—offers distinct advantages over any single approach: it provides comprehensive exposure, enables R0 resection, allows for one-stage reconstruction, and minimizes morbidity by avoiding more extensive craniofacial resections.
4. Limitations and Outlook
Several limitations should be acknowledged.First, the Lynch incision, while providing excellent exposure, carries the risk of medial canthal web formation and visible scarring. Second, this combined approach demands surgical expertise in both orbital and endoscopic sinonasal techniques, along with careful consideration of patient-specific factors such as overall health status, tumor extent, and prior surgical history. Third, given that atypical SFT carries a significant risk of recurrence and poor prognosis, long-term follow-up of this patient is essential. We will continue to monitor her closely with serial clinical and imaging examinations.
Footnotes
Acknowledgments
The case report was written by Xiaoxiao Luo, Hangzhou, China. The contributions of each author are as indicated in the “Author Contributions” section.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or series of cases.
Consent to Participate
The patient in this case report has provided written informed consent. The patient confirms and agrees that we can conduct research, publish research, and use his photos and other case data.The signed written informed consent form was documented in the patient’s medical record.
Consent for Publication
The patient is aware and agrees that the article may be published in an open access manner. The signed written informed consent form was documented in the patient’s medical record.
Author Contributions
Concept and design: Xiaoxiao Luo. Acquisition, analysis, and interpretation of data:Xiaoxiao Luo,Xiangnan Du,Yufei Zhao. Drafting of the manuscript: Xiaoxiao Luo. Critical revision of the manuscript for important intellectual content: Xiaolin Cao
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Hangzhou Key Medical Discipline Construction Project (Clinical Research and Evaluation) (Grant No. 2025HZGF04).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data in this article: images, imaging data, etc., can be obtained by sending an email to: