
Abstract
A high-riding jugular bulb is defined by the superior aspect of the jugular bulb being present above the level of the inferior aspect of the internal auditory canal. Though typically asymptomatic, patients with high-riding jugular bulb may report several otologic and vestibular symptoms, most often conductive hearing loss, pulsatile tinnitus, and vertigo. The presentation of each symptom is highly variable and related to the anatomy abutted. The abnormal positioning of the jugular bulb, depending on its location, may have implications related to the viability of certain clinical procedures (like myringotomy) and in the treatment of presenting symptoms. It may also affect surgical planning, especially if mastoidectomy or a translabyrinth approach is being considered. We present the case of a 12 year old male seen in clinic for worsening conductive hearing loss and having no family history of hearing loss or anatomical abnormality. Upon otoscopy, a dark mass was visible posterior to the tympanic membrane, prompting further examination of temporal structures via computed tomography. CT revealed a dehiscent sigmoid plate with the jugular bulb protruding into the middle ear past the round window and contacting the stapes, an uncommon extreme case of high-riding jugular bulb. This case exemplifies a situation in which high-riding jugular bulb must be considered while treating conductive hearing loss and underscores the importance of recognizing any abnormal venous structure in the middle ear before proceeding with myringotomy or surgical intervention.
Introduction
The jugular bulb refers to the venous structure seen at the superior aspect of the internal jugular vein through which the sigmoid and inferior petrosal sinuses drain 1 . This structure is known to occasionally extend more superiorly at the petrous temporal bone, surpassing the inferior aspect of the internal auditory canal, defining what is referred to as a “high-riding jugular bulb”. This abnormality may involve a venous diverticulum, often seen at the superior aspect of the bulb if present at all. Patients with high-riding jugular bulb may or may present with deficient sigmoid plate, causing dehiscence of the venous structure. 2 While non-dehiscent cases often do not involve structures superior to the mastoid, migration of the jugular bulb is highly variable and can extend as far as the external auditory canal, a fate often associated with dehiscent cases. 3
The presence of a high-riding jugular bulb with or without dehiscence may be visualized with cranial computed tomography (CT) imaging, 4 in which the degree of venous protrusion into the middle ear and ossicular chain can be appreciated in the axial coronal planes. In advanced cases, the bulb may be otoscopically visible as a purple discoloration or apparent mass posterior to the posteroinferior quadrant of the tympanic membrane. Accompanying symptoms most often include conductive hearing loss and pulsatile tinnitus, though in the majority of cases this abnormality is asymptomatic.5,6 The prevalence of otologic symptoms is significantly greater among those with dehiscent high-riding jugular bulb. 2 Radiographic studies have indicated that incidence of high-riding jugular bulb is especially high in children, with cranial CT imaging showing this anomaly 42% of asymptomatic children overall 7
Grading of high-riding jugular bulb has been described by Prasad et al 8 as having five distinct levels, with the lowest only involving the tympanic annulus and subsequent grades extending to encompass the inferior margin of the round window, entire round window niche, margin between round window and stapes, and Stapes arch. We present a pediatric case in which the jugular bulb has migrated to the inner ear, abuting the stapes arch.
Case Presentation
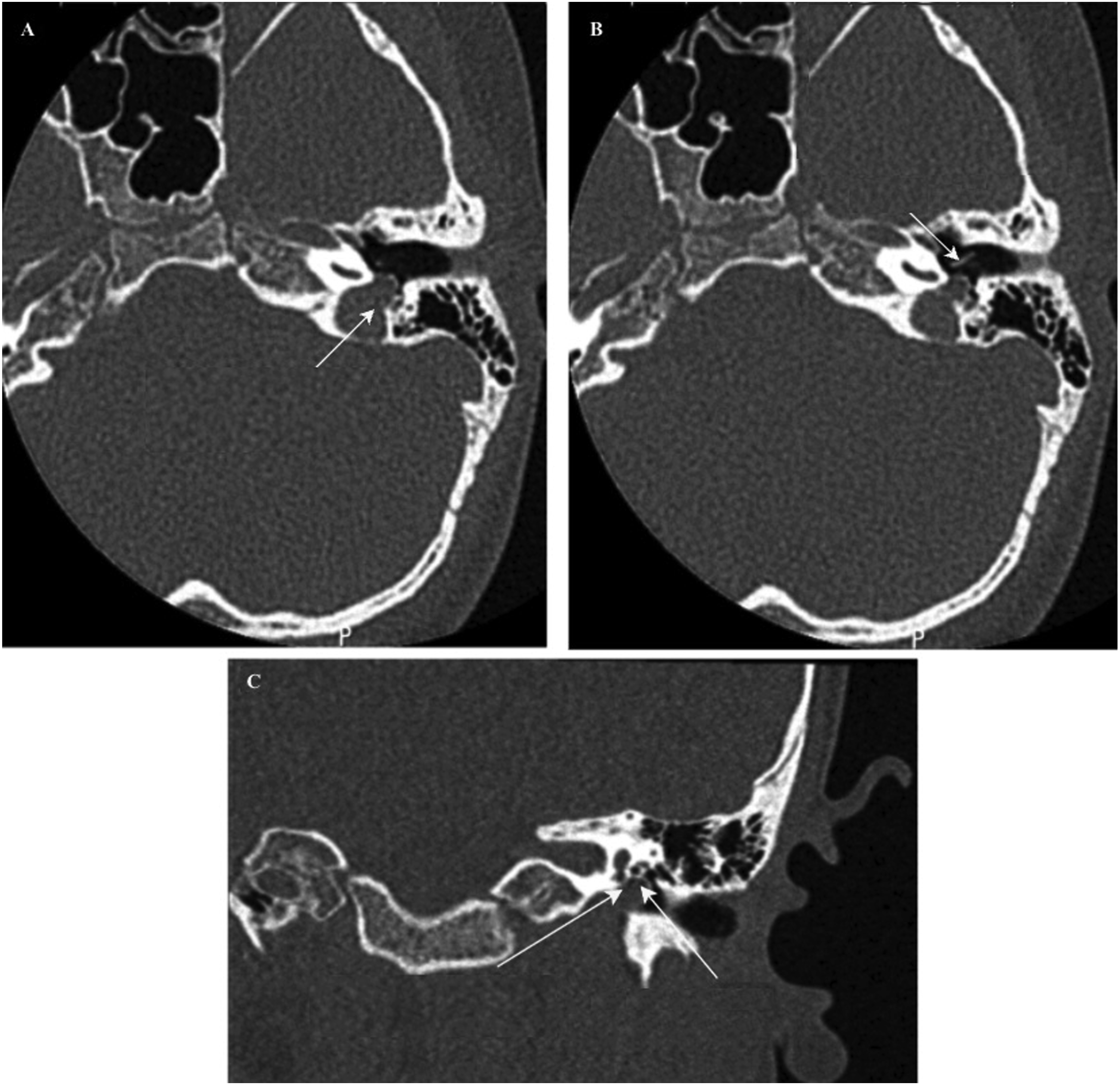
A 12-year-old male recently diagnosed with conductive hearing loss was referred to a tertiary medical center. He presented without tinnitus and had no known family history of conductive hearing loss or other relevant otologic conditions. Although there was a history of myringotomy and tubes, this patient had no significant infectious history upon parental interview and chart review. Pure tone audiometry (Figure 1) confirmed left-sided conductive hearing loss. Otoscopy revealed an in-tact tympanic membrane with a bluish mass posterior to the TM (Figure 2). CT imaging revealed an apparent dehiscent sigmoid plate with the jugular bulb protruding well into the middle ear, making contact with the stapes and round window (Figure 3). Upon this discovery, the parents were counseled on the implications of this finding, including its potential involvement in CHL and additional associated symptoms that may be noticed in the future. They were also made aware of the increased surgical risk introduced by the venous structure in the middle ear and instructed to note any changes or bleeding in the region. A referral was made for hearing aid prescription, and continued audiologic follow-up was recommended. Written informed consent was obtained from the patient’s legally authorized representative (parent) and institutional board approval was waived due to the non-experimental nature of this report. Audiological testing reviewed a conductive hearing loss on the left ear. Graphic generated using Audgen
9
Endoscopic examination of the left ear revealed a bluish mass posterior to the tympanic membrane below the posteroinferior quadrant 3A: CT scan, axial cut, demonstrating dehiscence of jugular bulb and deficient sigmoid plate (arrow). 3B: The jugular bulb is shown to invade the middle ear, protruding past the region of the round window toward the stapes. 3C: Coronal plane CT shows jugular bulb protrusion into the mesotympanum and contact with the round window (left arrow) and anterior crus of the stapes (right arrow)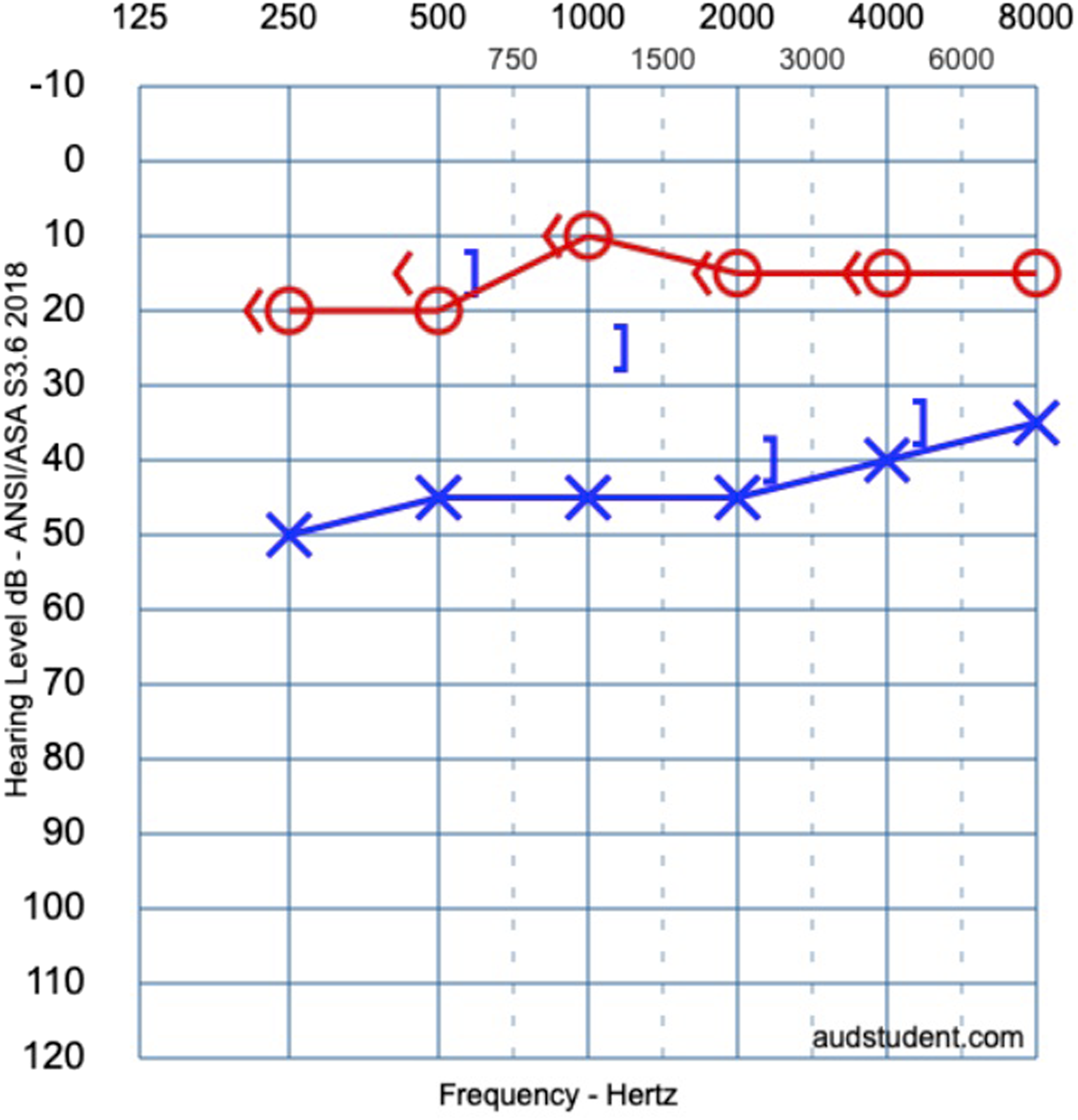

Discussion
This case represents a rare and extreme pediatric manifestation of high-riding jugular bulb, classified as grade V according to the criteria described by Prasad et al. Around 2% high-riding jugular bulb cases fall under this category. Notably, this case was dehiscent, with imaging showing a clear deficiency of the sigmoid plate despite having no pulsatile tinnitus, known to be associated with sigmoid sinus dehiscence.10,11 The presence of conductive hearing loss is consistent with the experience of most symptomatic patients, 12 though the exact etiology of CHL in these cases is unknown. It has been proposed that obstruction of the round window may be involved given its frequent presence alongside CHL in cases of high-riding jugular bulb.13,14 To date, however, limited evidence is available to substantiate whether round window involvement is more, less, or equally relevant to CHL than ossicular chain interference or direct tympanic membrane proximity in cases like this. 14
As this abnormality is uncommon, the bluish purple mass visualized otoscopically behind the tympanic membrane may be easily mistaken for other structures, especially those known to present with similar otologic symptoms like cholesterol granulomas or glomus tympanicum tumors.15,16 Importantly, masses of this type should be closely scrutinized to confirm the presence or absence of a high-riding jugular bulb before continuing with procedures to treat other conditions of the ear. Given the close proximity of the jugular bulb to the tympanic membrane, a much higher risk of inadvertent puncture of the jugular bulb is present, which can cause severe hemorrhage. 4 Thus, myringotomy and tympanoplasty may be unfavorable. Surgical treatment of high-riding jugular bulb is most often done to reduce chronic vestibular symptoms and tinnitus, which is known to occasionally manifest similarly to or concurrently with Ménière’s disease. 17
Conclusion
This pediatric case of symptomatic extremely high-riding jugular bulb demonstrates a clear example of middle ear invasion, emphasizing the importance of its consideration in differential diagnosis of an apparent mass posterior to the tympanic membrane. Computed tomography is useful in elucidating the presence and severity of high-riding jugular bulb, with non-contrast CT usually sufficient. Surgeons should be vigilant of jugular bulb invasion and take into consideration how it may be encountered when choosing a surgical approach. Clinicians should be cautious of any bluish mass posterior to the tympanic membrane and should avoid myringotomy until its nature is better understood.
Footnotes
Acknowledgements
The authors would like to thank the subject and their parents, as well as the House Institute Foundation and staff at the House Clinic of PIH Good Samaritan Hospital.
Ethical Considerations
Ethical approval to report this case was deemed not necessary by the institutional review board of PIH Good Samaritan Hospital.
Consent to Participate
The authors of this report declare that written and verbal informed consent to participate was obtained by the parents of the sole pediatric patient involved with requirement for further review waived by the IRB of PIH Good Samaritan Hospital; All necessary precautions related to the use of protected health information in research were taken.
Author Contributions
Benjamin Heifetz - design, acquisition, analysis, drafting manuscript, figure production. Kevin A. Peng - design, acquisition, interpretation of data, editing and critical review of manuscript, figure production.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This report is funded by the House Institute Foundation and does not have an associated grant number. The authors declare that support for the publication of this article is provided by The House Institute Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
This manuscript, being a case report, does not involve data outside that which is protected by The Health Insurance Portability and Accountability Act (HIPAA).