
Abstract
Keloids of the auricular lobule remain difficult to manage because recurrence is common after excision alone. Traditional surgical teaching has supported intralesional or “core” excision with preservation of a peripheral cuff of keloid tissue, based on the premise that avoiding injury to adjacent keloid-prone skin may reduce recurrence and allow lower-tension closure. More recent histopathologic and clinical studies challenge this approach, suggesting that residual keloid tissue, particularly the peripheral rim, may contain proliferative fibroblasts and profibrotic signaling associated with recurrence. However, concurrently, other recent systematic reviews suggest that core excision can achieve acceptable outcomes when combined with adjuvant therapy. Current evidence does not support a universal approach. For small to medium auricular lobule keloids, complete excision of clinically abnormal tissue with tension-minimized closure is reasonable. For large auricular lobule keloids, limited cuff-preserving core excision, staged serial excision, or stellate excision may be considered to minimize the risk of high-tension closure. Regardless of technique, postoperative adjuvant therapy, particularly serial corticosteroid injection, should be strongly considered.
Keywords
Auricular keloids of the lobule remain a frustrating problem for otolaryngologists and facial plastic surgeons because recurrence is common, lesions are visible, and treatment must preserve ear contour. A persistent technical question is whether the surgeon should intentionally preserve a peripheral cuff of keloid tissue during excision, or instead remove all clinically abnormal tissue to decrease risk of recurrence.
The traditional rationale for “intralesional”, “intramarginal” or “core,” excision is practical. Leaving a thin peripheral rim may avoid violating adjacent keloid-prone skin, reduce wound tension, and minimize distortion of the lobular contour. Conventional treatment paradigms therefore have supported conservative excision combined with adjuvant therapy, particularly corticosteroid injection1,2 This approach remains attractive when complete excision would create a large defect, require excessive skin recruitment, or compromise cosmesis.
However, the biologic argument for leaving keloid tissue behind can be concerning to some surgeons. Histologic and clinical studies suggest that residual proliferative keloid tissue may act as a nidus for regrowth. Chong et al reported reduced recurrence after complete excision of the proliferating core in auricular keloids, and Lemperle et al and Tan et al emphasized that residual active keloid tissue may contribute to recurrence.3-5 These findings support complete excision of clinically abnormal tissue when closure can be achieved without undue tension or anatomic distortion.
The counterpoint is that recurrence is not determined by margin status alone. Surgical tension, lesion size, location, patient biology, postoperative surveillance, and adjuvant therapy all influence outcome. Recent evidence supports the continued role of intralesional excision in selected cases. Lawera et al found a pooled recurrence rate of 13% after keloid intralesional excision in a meta-analysis of 608 keloids, and Ran et al concluded that core excision can achieve low recurrence when combined with adjuvant therapy.6,7 Thus, preserving a cuff should not be considered inherently wrong; rather, it should be reserved for circumstances in which complete excision would create a worse reconstructive problem.
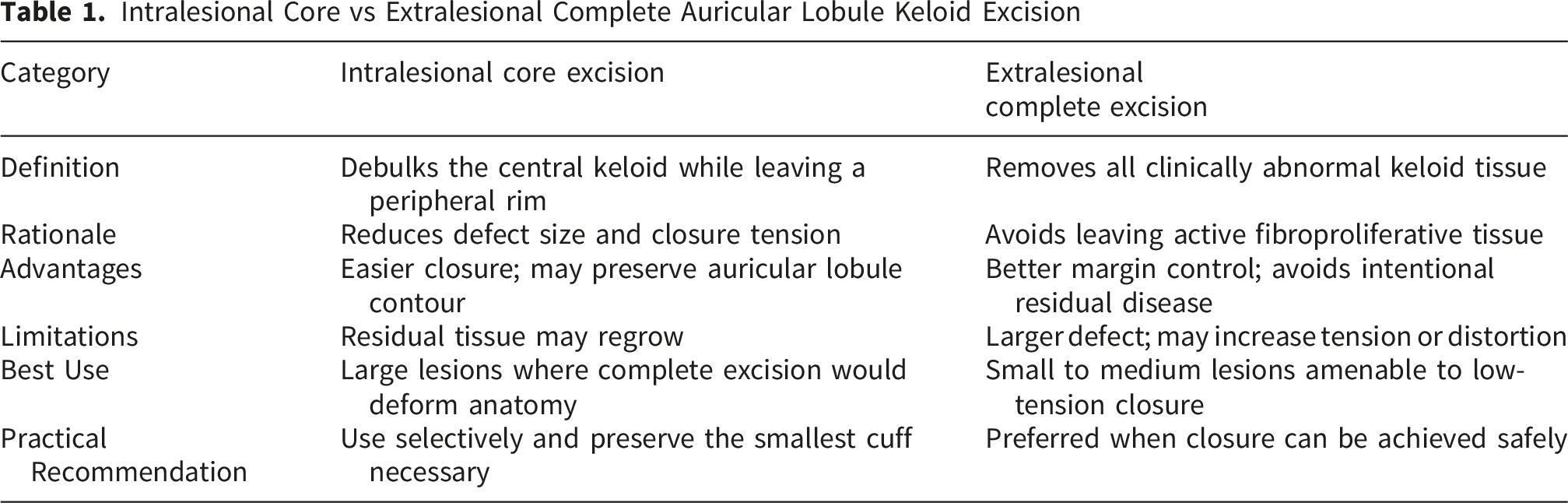
Intralesional Core vs Extralesional Complete Auricular Lobule Keloid Excision
Regardless of the excisional plan, excision alone is insufficient. Serial intralesional corticosteroid injection should be strongly considered after surgery. Pressure therapy, silicone therapy, 5-fluorouracil, and radiotherapy may be appropriate for selected recurrent or high-risk lesions.8-10 The most defensible approach is therefore, not “always preserve” or “never preserve,” but rather be tension and contour conscious when planning auricular lobule keloid removal and closure.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.