
Abstract
Balloon sinus dilation is widely utilized for the management of chronic rhinosinusitis and is generally considered safe when employed in appropriately selected patients. However, successful frontal sinus balloon dilation may be technically challenging due to the complexity of the frontal recess anatomy and is associated with potentially serious complications including skull base injury. We report a case of a 78-year-old man who developed acute tension pneumocephalus following office-based frontal balloon sinuplasty due to inadvertent skull base entry in the setting of complex frontal recess anatomy. The patient required emergent open craniotomy followed by definitive endoscopic skull base repair at a tertiary care center. This case highlights the importance of careful review of preprocedural computed tomography scans of the sinuses and appropriate patient selection when considering frontal sinus balloon dilation.
Introduction
Since its FDA approval in 2005, balloon sinuplasty (BSP) has grown in popularity among otolaryngologists as a minimally invasive treatment option for patients with chronic rhinosinusitis. 1 The technique involves using an inflatable balloon to dilate the maxillary, sphenoid, or frontal sinus ostia and outflow tracts via local microfracture. It is a tissue-preserving procedure that can lead to improved mucociliary clearance by minimizing obstruction of the outflow tracts without excising sinonasal mucosa. 2 Recent meta-analyses have shown excellent patient outcomes that are comparable to functional endoscopic sinus surgery for appropriately selected patients undergoing BSP. 3
Although a minimally invasive procedure, BSP is performed in the delicate region of the paranasal sinuses and can result in serious complications including injury to the orbit or skull base. Prior studies have demonstrated that nearly half of serious complications from BSP occur during frontal sinus dilation; this is in part due to the proximity of the frontal sinus to the skull base, but also due to the variable anatomy of the frontal recess, with some pneumatization patterns making successful dilation of the frontal sinus ostium especially difficult. 4 In this report, we present a case of skull base injury leading to cerebrospinal fluid leak and tension pneumocephalus after in-office frontal sinus balloon dilation, focusing on the anatomic risk factors which contributed to this complication and preventive strategies for surgeons who perform BSP.
Case Report
A 78-year-old man with chronic rhinosinusitis without polyps underwent in-office BSP of the bilateral maxillary, sphenoid and frontal sinuses under moderate sedation at a community otolaryngology practice. Postoperatively, the patient exhibited delayed emergence from sedation and difficulty ambulating. He was discharged home despite these findings.
Within minutes of leaving the clinic where BSP was performed, the patient developed progressively worsening altered mental status in the parking lot and eventually became unresponsive. He was transported via ambulance to a local emergency department, where computed tomography (CT) scan of the head revealed tension pneumocephalus (Figure 1A-B). The patient underwent emergent bifrontal craniotomy with placement of a subdural drain. The patient’s postoperative course was complicated by a temporal lobe intraparenchymal hemorrhage, left-sided clear rhinorrhea, as well as persistent altered mental status, including confusion, dysarthria, and impaired memory. On the 7th postoperative day after his craniotomy, the patient was transferred to our tertiary care referral center for definitive repair of his skull base injury and cerebrospinal fluid (CSF) leak. On examination at our institution, he had intermittent clear rhinorrhea from the left nasal cavity, which was positive for presence of beta-2 transferin, confirming it to be CSF. A preoperative maxillofacial CT scan was performed and revealed a defect in the left cribriform plate in addition to a narrow left frontal sinus outflow tract with a prominent agger nasi and suprabullar frontal cell (Figure 1C-D). (A) Axial and (B) coronal computed tomography scan of the head demonstrating extensive intracranial air (asterisk) consistent with tension pneumocephalus after attempted balloon dilation of the frontal sinuses. (C) Coronal computed tomography scan of the maxillofacial skeleton demonstrating a skull base defect involving the left cribriform plate (arrow). (D) Sagittal scan of the left nasal cavity demonstrating a thick nasofrontal beak, small frontal sinus, prominent agger nasi (open circle) and suprabullar frontal cell (closed circle) resulting in a narrow frontal sinus ostium and outflow tract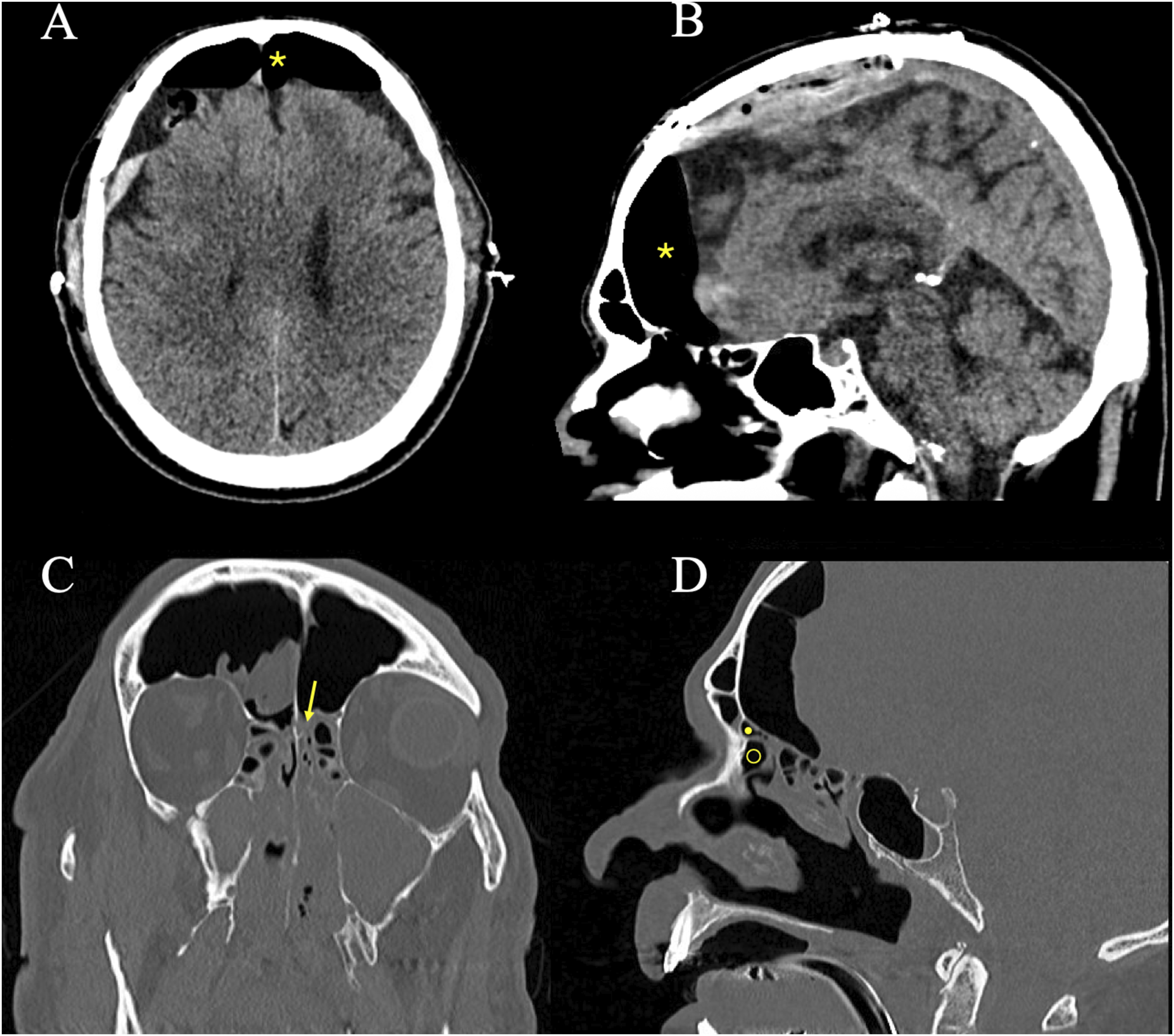
The patient was taken to the operating room with a rhinologist and neurosurgeon for definitive repair through an endoscopic endonasal approach. A lumbar drain was placed and intrathecal fluorescein was administered to help identify the location of the skull base defect. Complete left-sided image-guided endoscopic sinus surgery, including maxillary antrostomy, total ethmoidectomy, sphenoidotomy, and a Draf IIb frontal sinusotomy, was then performed on the left to adequately expose the frontal sinus drainage pathway and skull base defect. An approximately 1 cm diameter cribriform plate defect was identified posteromedial to the frontal recess with visible egress of fluorescein-dyed CSF. The defect was smooth in contour and appeared to have been balloon-dilated, with visible brain parenchyma in the anterior cranial fossa (Figure 2A). After stripping the mucosa surrounding the defect, it was repaired in a multilayer fashion with DuraGen collagen matrix placed subdurally and a nasoseptal flap placed in an onlay fashion (Figure 2B). Following surgery, the patient remained hospitalized for ten days. The lumbar drain was removed on postoperative day 3. On the 10th postoperative day, the patient was doing well without further CSF rhinorrhea as well as improved mental status and was discharged to a nearby rehabilitation facility. At his six-month follow-up, the patient demonstrated complete resolution of neurological symptoms and had no evidence of recurrent CSF rhinorrhea. Intraoperative endoscopic views demonstrating (A) exposure of left cribriform defect with visible brain parenchyma (asterisk) and (B) reconstruction of the skull base defect using a vascularized nasoseptal flap (open circle)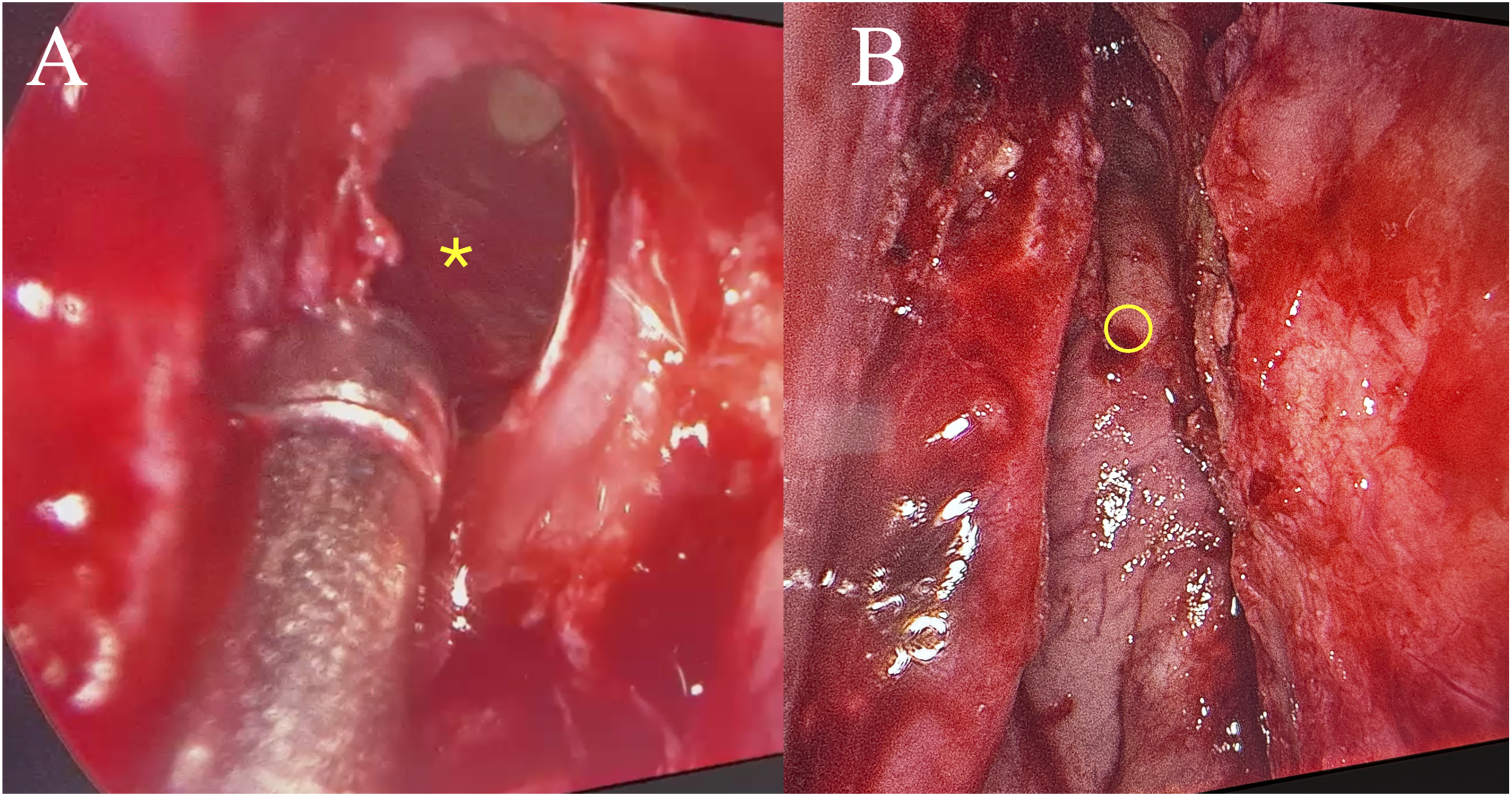
Discussion
This case demonstrates a serious complication of skull base injury and tension pneumocephalus after frontal BSP in the setting of unfavorable frontal sinus anatomy. Review of the patient’s CT imaging revealed a thick nasofrontal beak, small frontal sinus, prominent agger nasi, and a suprabullar frontal cell, resulting in a narrow frontal ostium and restricted outflow tract. These features significantly increased the risk of posterior misdirection of the balloon catheter toward the anterior skull base rather than the natural drainage pathway, resulting in the creation of a false passage intracranially through the thin cribriform plate.
The frontal sinus is the most anatomically complex of the paranasal sinuses due to the narrow and highly variable configuration of its outflow tract, its superiorly oriented trajectory, as well as its close proximity to both the orbit and anterior skull base. 5 The narrowest point of the frontal sinus drainage pathway is the frontal recess, which is bounded anteriorly by the agger nasi and frontal beak and posteriorly by the ethmoid bulla and skull base. 5 This region can have significant variability between patients in terms of diameter, angulation, and pneumatization pattern, making surgical access uniquely challenging and dependent on careful preoperative planning. The agger nasi cell is present in approximately 95% of individuals and can significantly alter the frontal sinus outflow tract on its own, while additional cells, including supra-agger, suprabullar, and supraorbital ethmoid cells, may further constrict the drainage pathway.6-8 These frontal recess cells can also shift the drainage pathway medially, posteriorly, or anteriorly, producing a tortuous access route rather than a linear tract to the frontal sinus, thereby limiting instrumentation and increasing procedural difficulty. 6
Unlike traditional endoscopic frontal sinusotomy, balloon dilation does not remove bony partitions but instead relies on successful passage of a catheter through the native drainage pathway. When that pathway is narrow or angulated, the device may follow the path of least resistance rather than the true ostium, predisposing to false passage and skull base violation. In support of this mechanism of injury, a recent cadaveric radiologic analysis from Lopez et al. (2020) demonstrated that even in the hands of fellowship-trained rhinologists, balloon dilation does not consistently enlarge the frontal sinus outflow tract and may instead enter and dilate adjacent structures such as the agger nasi or other cells, producing unintended anatomic changes.
9
In our present case, the patient’s combination of a prominent agger nasi, suprabullar frontal cell, thick nasofrontal beak, and small frontal sinus resulted in marked narrowing of both the frontal sinus ostium and recess. These anatomic characteristics likely altered the natural trajectory of the balloon catheter and created resistance to catheter advancement, resulting in posterior misdirection and skull base violation rather than entry into the frontal sinus (Figure 3). Proposed mechanism of injury. Schematic illustration demonstrating posterior misdirection of the balloon catheter (arrow) toward the anterior skull base due to a large agger nasi, suprabullar frontal cell, and thick nasofrontal beak, resulting in skull base violation rather than entry into the frontal sinus.
Although BSP is generally considered safe, skull base injuries and other complications of BSP have been reported previously. Separate analyses of the MAUDE and openFDA databases demonstrated that frontal sinus balloon dilation was associated with the highest number of complications among the paranasal sinuses.4,10 Of these complications, skull base injury with CSF leak was the most common. Similarly to our case, a recent case report also described tension pneumocephalus following frontal sinus balloon dilation in a patient with a large agger nasi cell and narrowed drainage pathway. 11 Taken together, our case and others in the literature indicate that a careful review of preoperative imaging is critical to preventing complications from BSP. For patients with complex anatomy and those undergoing revision procedures, the use of image-guidance during BSP may be beneficial. 12
Another key takeaway from this case is the necessity of promptly recognizing an iatrogenic skull base injury and repairing the defect or transferring the patient to a tertiary care center before complications such as tension pneumocephalus, meningitis, and brain herniation can occur. The success rate of primary repair of such iatrogenic defects is high and ranges from 80-100%, such that the most important factor is often repairing the defect before devastating sequelae can arise.13,14 In our case, a multilayered repair with collagen matrix and a nasoseptal flap, in addition to a lumbar drain, was employed due to the large cribriform defect and initial tension pneumocephalus that occurred after injury. For repair of smaller iatrogenic skull base injuries with low-flow CSF leak and no evidence of tension pneumocephalus, it is often sufficient to utilize an onlay free mucosal graft with or without an inlay repair. 15 In the setting of large defects, high-flow leaks and tension pneumocephalus, it is preferable to utilize a nasoseptal flap if available. 15
Conclusion
This case illustrates how unfavorable frontal recess anatomy can convert an otherwise low-morbidity intervention into a potentially life-threatening complication. Balloon dilation of the frontal sinus should be reserved for patients with demonstrably accessible drainage pathways, and surgeons must maintain a low threshold to employ traditional endoscopic approaches, or utilize image-guided dilation devices, when preoperative imaging reveals high-risk anatomic variants that result in a tortuous and narrowed frontal recess and ostium.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases.
Consent to Participate
Written informed consent was obtained from the patient for their inclusion in this case report.
Author contributions
SW drafted the article with IB and worked on figure creation. IB drafted the article with SW, worked on figure creation, and extracted data from the medical record. BW performed the interventions described in this case report and assisted with article drafting and figure creation. All authors approved of the final article for publication and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.