
Abstract
We report the case of a 36-year-old male patient with an 18-year history of Behçet's disease who was referred to our department in October 2025 for dyspnea and dysphagia. Flexible laryngoscopy revealed a partial epiglottic defect with supraglottic mucosal hyperplasia and edema. Microlaryngoscopic carbon dioxide (CO₂) laser surgery of the larynx was performed, with dyspnea disappearing after the operation. No recurrence of dyspnea was observed during the 3-month follow-up.
Significance Statement
This case illustrates a distinct acute-on-chronic process: long-standing, recurrent epiglottic ulceration led to architectural distortion that silently depleted airway reserve, rendering the airway susceptible to critical compromise from acute inflammatory edema. We highlight that even mild-to-moderate supraglottic swelling can precipitate critical airway obstruction in patients with such structural remodeling, underscoring the need for proactive surveillance in patients with long-standing Behçet’s disease
Case Presentation
A 36-year-old male was admitted to our hospital with a 2-day history of dyspnea and dysphagia. The patient presented with dyspnea and a loud laryngeal stridor upon respiration. Additionally, the patient did not present with hoarseness. The patient had an 18-year history of Behçet’s disease. Eighteen years earlier, he had presented with oral pain, ocular pain, and dysphagia, and was diagnosed with oral ulcers, uveitis, and esophageal ulcers. According to the 2006 International Criteria for Behçet’s Disease (ICBD), the presence of oral ulceration and ocular involvement yielded a total score of 4 points, fulfilling the criteria for a definitive diagnosis of Behçet’s disease.
The diagnostic evaluation also included hematological examinations, electronic laryngoscopy, esophagogastroduodenoscopy (EGD), and pathological examination to further confirm the diagnosis of Behçet’s disease. Crucially, despite recurrent oral aphthous ulcers, the patient received no pharmacological intervention during the 18 years following diagnosis. Over the four months preceding admission, the patient experienced recurrent episodes of odynophagia and globus pharyngeus and developed progressively worsening stridor. These symptoms were managed conservatively without formal diagnostic evaluation or targeted therapy. Two days prior to admission, the patient developed progressively worsening dyspnea.
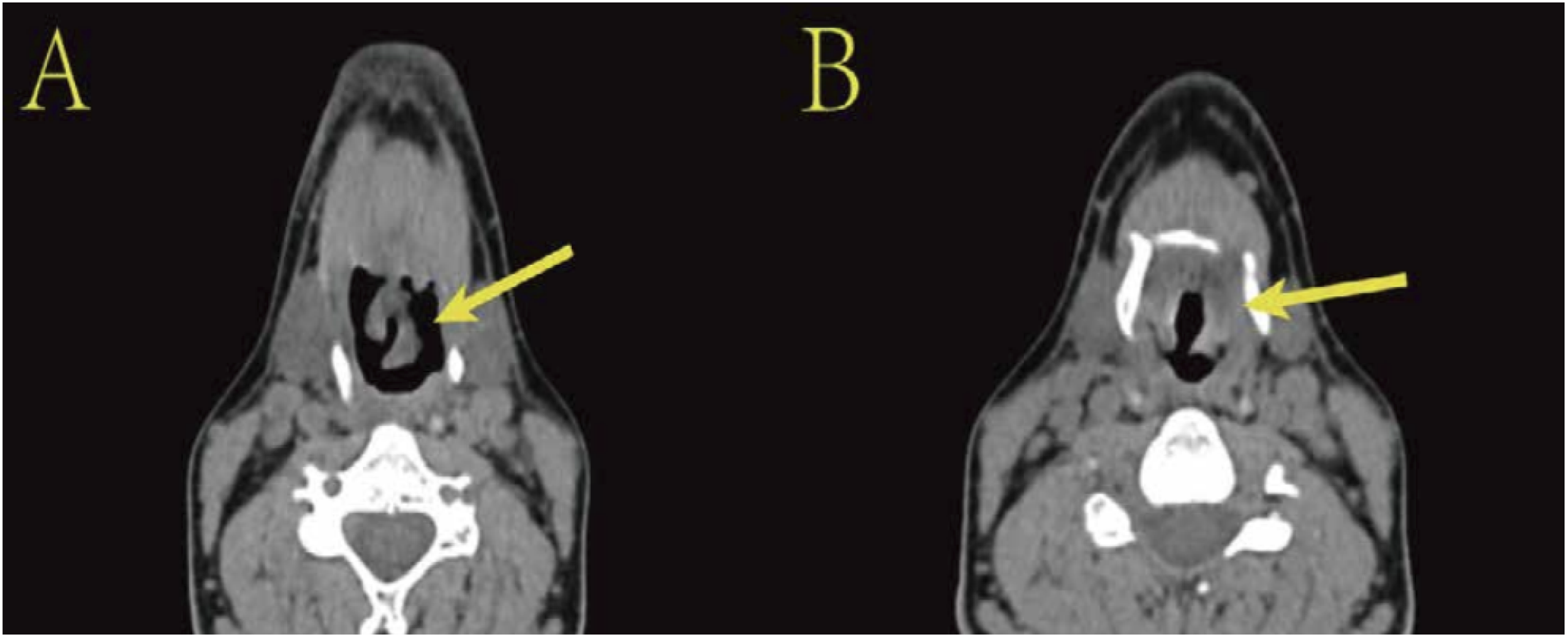
After admission, an electronic laryngoscopy and an Axial CT were performed (Figures 1 and 2), which revealed congestion and morphological changes of the epiglottis, with a partial defect observed at the right epiglottic margin. Supraglottic mucosa showed hyperplasia and edema, obscuring the glottis. Bilateral vocal cords demonstrated good mobility. Post-admission fiberoptic laryngoscopy revealed epiglottic deformity and defects. Crucially, the epiglottis exhibited irreversible structural alterations inconsistent with a de novo acute process. Coupled with the clinical trajectory over the preceding 4 months, these findings collectively point to a chronic evolution of the epiglottic pathology. The 4-month symptom progression reflects a gradual depletion of the laryngeal inlet reserve due to chronic scarring, culminating in critical airway obstruction precipitated by superimposed acute supraglottic edema. Laryngeal endoscopic findings. The laryngeal images (A, B) show epiglottic malformation and defect with partial absence of the right epiglottic margin (arrow). Hypertrophic edema of the supraglottic mucosa causing glottic obstruction (C) (arrow). (A) laryngeal image obtained at the one-month postoperative follow-up shows normal findings (D) Axial CT at the initial presentation. Axial CT demonstrates epiglottic malformation and defect (A) (arrow). Thickening of the epiglottis and bilateral aryepiglottic folds with pharyngeal stenosis (B) (arrow)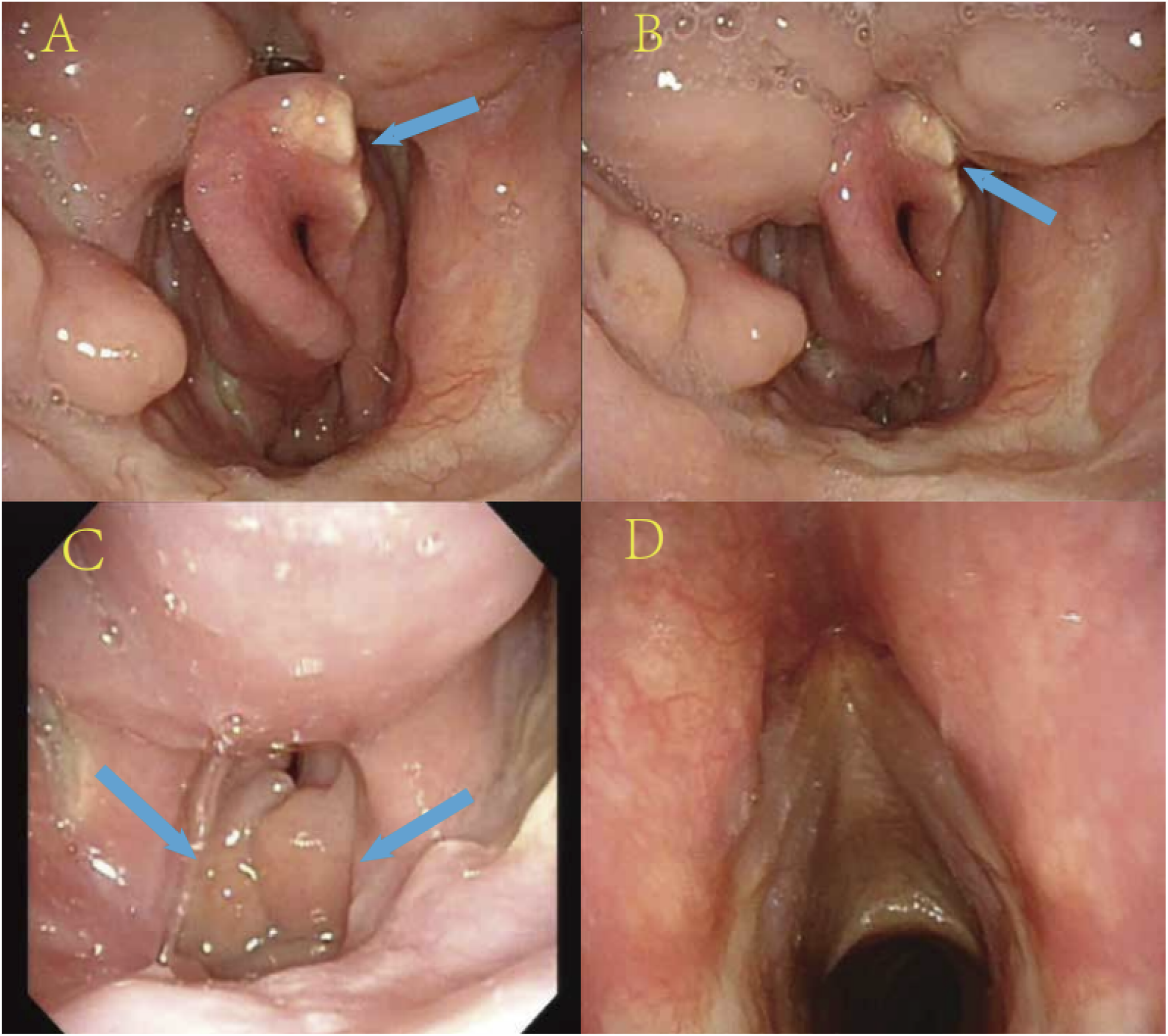
The surgical procedure was performed using a Lumenis 40C CO2 laser surgery system coupled with an operating microscope (Sensera/S7, Carl Zeiss). A dilating laryngoscope was utilized to expose the larynx, alongside a standard set of laryngeal microsurgical instruments. The laser was operated in superpulse mode with a power output of 8–10 W. Microlaryngoscopic carbon dioxide (CO2) laser surgery of the larynx was performed in November 2025, and tracheostomy was not performed intraoperatively. During the procedure, an incision was made along the margin of the supraglottic edema, achieving complete excision of the edematous tissue bilaterally, and a biopsy of the epiglottic ulcer was sent for pathological examination. Intraoperative blood loss was minimal, and the patient reported no significant postoperative pain. Histopathological findings of the supraglottic tissue revealed epithelial edema, hemorrhage, partial areas of hyperplasia, local ulceration, interface inflammation in a few regions, no prominent small vessel vasculitis, and scant lymphocytic infiltration around some small vessels. Histopathological examination of the resected epiglottic tissue revealed edematous squamous hyperplasia with focal ulceration, and inflammatory cell infiltration consisting mainly neutrophils, lymphocytes, and plasma cells, with evidence of interface inflammation, vasculitis, and perivascular inflammation (Figure 3). The pathological examinations revealed changes in the larynx consistent with Behçet’s disease. Photomicroscopic views of the resected epiglottis tissue (A) and supraglottic tissue (B) (×40 magnification). The pathological examinations revealed changes in the larynx consistent with Behçet’s disease (H & E staining)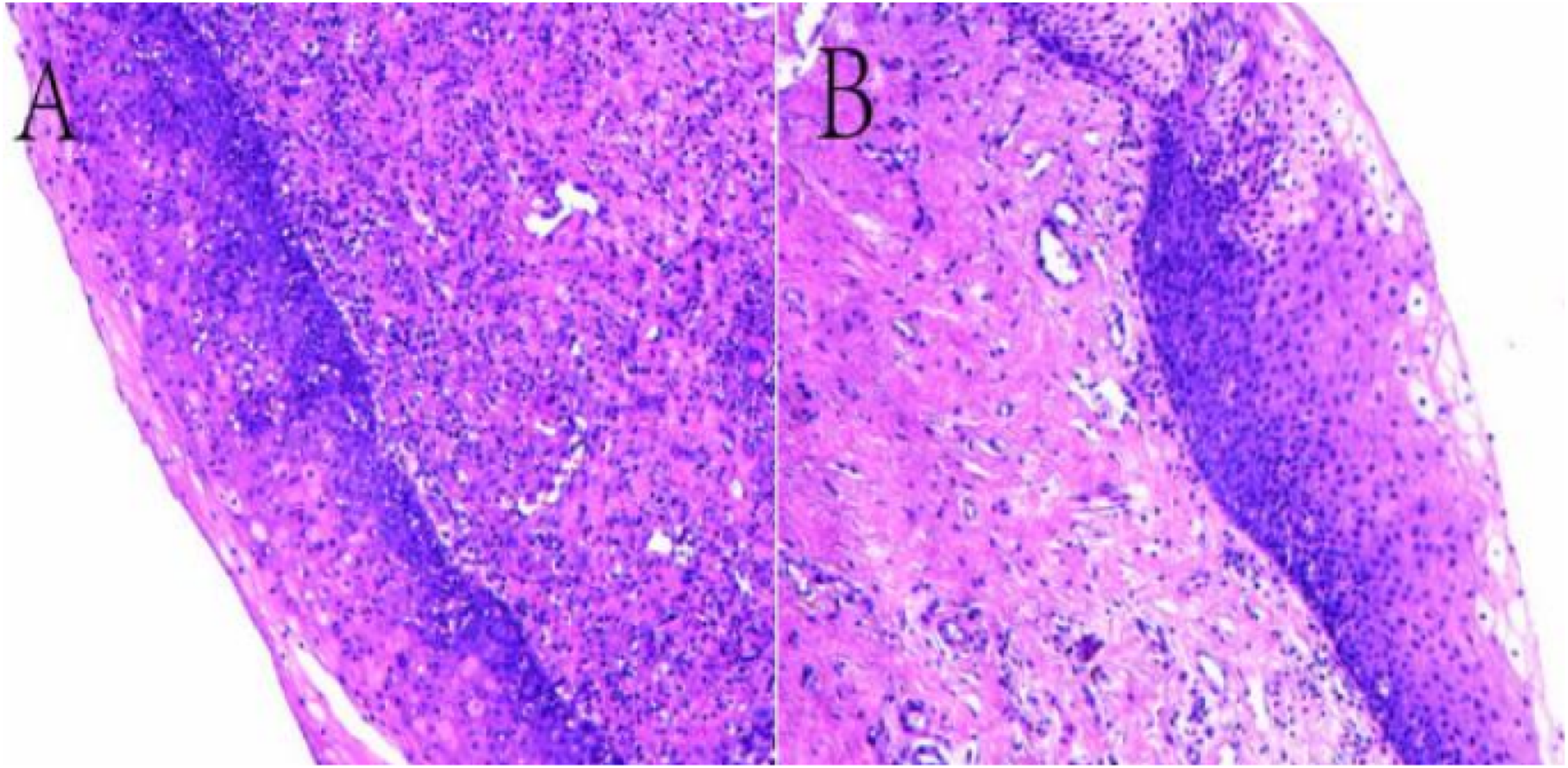
Postoperative day 1: Significant alleviation of dyspnea and stridor was observed. Following resection of the edematous supraglottic tissue, the patient received intravenous methylprednisolone (40 mg daily for 4 days) and was concurrently administered nebulized budesonide (0.5 mg twice daily) to reduce local inflammation. The regimen was well tolerated, and no adverse events were observed during hospitalization. On discharge, he was treated with prednisone acetate tablets at 30 mg/day, thalidomide tablets at 50 mg/day, and mycophenolate mofetil capsules at 1.5 g/day. The aforementioned medications were taken continuously for a total of 30 days. Follow-up at one month: Stridor resolved completely, and respiratory distress disappeared. Dyspnea has not recurred for 3 months after the operation. No adverse events were observed during the subsequent three-month course of oral therapy.
Discussion
Behçet’s disease (BD) is a systemic vasculitis, frequently presenting with a recurrent–relapsing pattern, involving both arterial and venous vessels of different calibers. Typically, BD presents with recurrent oral aphthae, followed by eye and joint involvement and genital ulcers. 1 The disease typically affects individuals in their third to fourth decade of life and does not display a gender preference. However, severe morbidities are more prevalent in men. The disease may also affect the larynx, the nervous system, and the gastrointestinal tract.2,3
The skin and mucosa of patients with Behçet’s disease show the hyperreactivity response and recurrent vasculitis. Furthermore, recurrent episodes of vasculitis lead to epiglottic mucosal hyperemia and edema, which may progress to ischemic necrosis in severe cases, ultimately resulting in epiglottic ulcers and defects.4,5
Current management of Behçet’s syndrome follows the 2025 update of the EULAR recommendations, which prioritizes early anti-TNF-α therapy combined with glucocorticoids for life-threatening organ involvement, aiming to avoid prolonged steroid monotherapy. In the present case, severe supraglottic edema with acute dyspnea necessitated immediate airway intervention. We performed emergency CO2 laser resection to relieve the obstruction, followed by systemic corticosteroids to control the underlying vasculitis. This approach aligns with contemporary practice, which views surgery as a critical adjunct to definitive immunosuppression rather than as a standalone treatment. 6
This case highlights the need for proactive airway surveillance in Behçet’s patients with established supraglottic involvement, aiming to anticipate the depletion of anatomical reserve and preempt catastrophic respiratory events.
Consent for Publication
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. The patient understands that their name and identity will not be revealed in the published article.
Footnotes
Acknowledgements
We extend our gratitude to Professor for his expert mentorship and insightful feedback on this case report. We also appreciate the assistance provided by AI-powered writing tools for language editing. Special thanks to the patient for participating in this study.
Ethical Considerations
In accordance with the ethical standards of the Declaration of Helsinki and national regulations, this type of retrospective case report is exempt from formal ethical review. Patient anonymity has been strictly preserved. Informed consent was obtained from all involved patients.
Consent to Participate
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. The patient was provided with a copy of the consent form.
Author Contributions
C Zhao: literature screening, literature search and drafting and revision of the case report; S Duan: revision of critical content. All authors approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by the Cuiying Scientific and Technological Innovation Program of The Second Hospital & Clinical Medical School, Lanzhou University (No.CY2024MSB16).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Data Availability Statement
Data are not publicly available due to patient privacy regulations but are available from the corresponding author on reasonable request, subject to ethical approval and a signed data access agreement.