
Abstract

Jean Cruveilhier (1791-1874) the newly appointed Chairman of Surgery and Pathologic Anatomy at the Paris’ “La Salpêtrière” hospital was committed to the clinical – pathological correlation of disease. He spent his mornings practicing medicine and his afternoons occupied with dissection – often of his own deceased patients. His dedication to finding the anatomic basis of maladies eventually led to his descriptions of the lesions of amyotrophic lateral sclerosis, gastric ulcers and the effects of increased intracranial pressure on the optic nerves.
In his great pathologic canon, Anatomie pathologique du corps humain – Descriptions, avec figures lithographiées et coloriées, des altérations morbides dont le corps humain est susceptible,
1
begun in 1829, he described the case of an 18-year-old woman who was carried short-of-breath and numb to the Charité Hospital. She died 2 hours after her admission. By her physician’s account, she had displayed new psychiatric symptoms for 2 months, but no focal neurological signs. At autopsy he found a large suprasellar pearly mass with multiple small shiny buds (Figure 1). The tumor was surrounded by arachnoid and had a waxy interior. It engulfed the cranial nerves without invasion. Cruveilhier correctly assumed that the slow growth of this ‘tumeur perlée’ led to few symptoms until it compressed the third ventricle and cerebral peduncles, causing sudden death. Base (left) and sagittal (right) drawings with Cruveilhier’s description: “The pons and the anterior and posterior peduncles are obscured by a large, prominent tumor, resembling the brightest pearl surmounted by a multitude of bumps like small, clustered pearls of unequal size. The distended optic commissure established its anterior boundaries. The nerves of the third cranial nerve, those of the fifth cranial nerve, and those of the seventh cranial nerve appear to emerge intact from the middle of this tumor.”
1
Courtesy of the University of Iowa, Hardin Health Sciences Library, John Martin Rare Book Room [FOLIO RB25 .C9]. Text translation by Google Translate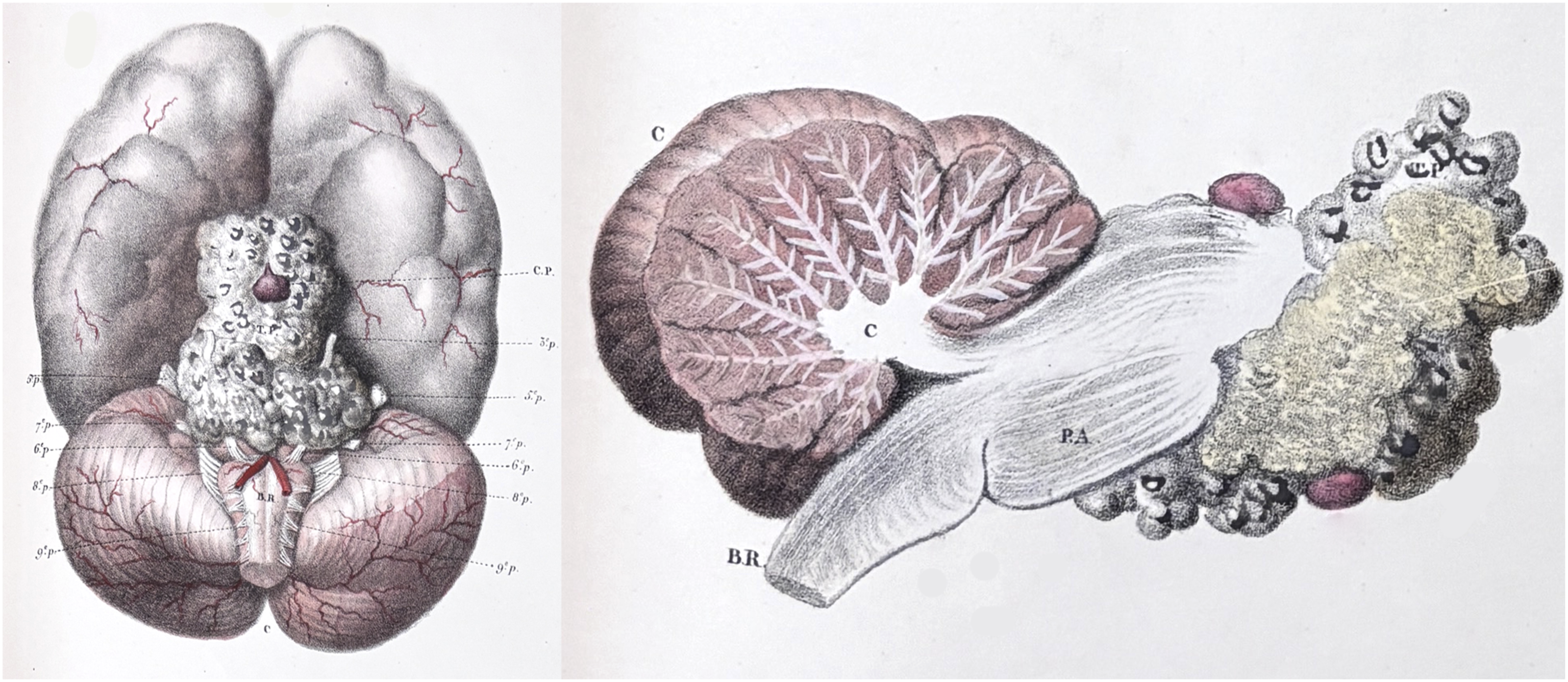
These intracranial pearly tumors were later called cholesteatomas or epidermoid cysts. Depending on their location, they presented with seizures, headache, diplopia, vision loss, gait disturbances or vomiting. They remained autopsy findings through the 1800s given the lack of focal neurologic signs and their invisibility on plain radiographs. 2 In a series of 14,005 autopsies by Seydel and Beck, cholesteatomas made up just 0.1% of 135 brain tumors. They were typically found at the cerebellopontine angle and beneath the pons and midbrain.
By 1920, the pioneering neurosurgeon Harvey Cushing had encountered two epidermoid tumors during surgery.3,4 Cushing explored the posterior fossa, based on symptoms alone as no advanced imaging existed. An attempted tumor resection was described by his assistant Percival Bailey in a follow-up paper
5
(Figure 2): Case 3 – Examination: The patient had bilateral choked disks with elevation of 4 diopters, development of coarse nystagmus on looking to the right and left, unsteadiness of station and gait, and slight incoordination of all the extremities of cerebellar type. Operation (December 20, by Dr. Cushing). …When the dura was opened, the hemispheres appeared normal, and exploration of the recesses disclosed no tumor; but when the two hemispheres, which had herniated down into the foramen, were separated, the glistening surface of a pearly tumor was seen. The vermis was split and held apart, and a good view of the tumor was obtained. It was found impossible to remove the capsule because some large vessels were firmly attached to it. However, as the tumor was soft, the contents were scooped out with a pituitary spoon…There was a transitory hyperthermia, reaching 104 F., after which recovery was uninterrupted except for annoying and persistent hiccups… Jan. 19, 1922, the patient was discharged.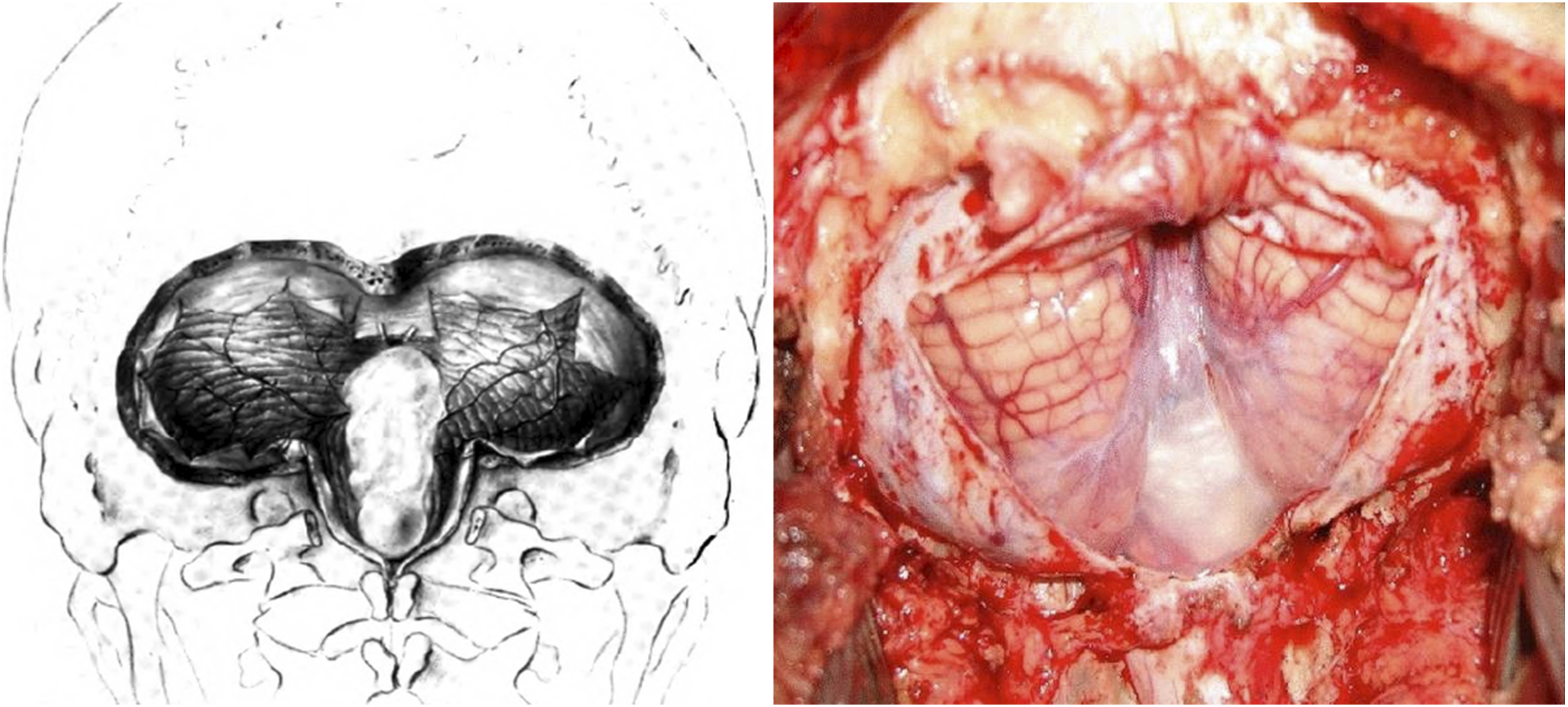
Although Cushing described complete resection of a cholesteatoma arising from the calvarium, decompression or partial resection was the rule for brain lesions prior to the introduction of the operative microscope in the 1950s. Even with modern imaging and microsurgical technique, almost half of brainstem and cerebellopontine cholesteatomas are incompletely resected as the matrix is often firmly adherent to vital nervous and vascular structures. 7
Footnotes
Ethical Considerations
This article does not contain any studies with human or animal participants.
Consent to Participate
There are no human participants in this article and informed consent is not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
This paper contains no new data. All data included are available through conventional library sources. The authors would be pleased to assist interested researchers via the corresponding author’s email.