
Abstract
The common causes of epistaxis in children are mostly local mucosal dryness, trauma, or inflammation, while epistaxis caused by leech infestation is clinically rare and easily overlooked. This article reports a case of epistaxis in a child due to leeches and, combined with a literature review, analyzes its clinical characteristics and key points of diagnosis and treatment. Children often present with recurrent unilateral epistaxis, nasal obstruction, and a feeling of insect crawling, and most have a history of exposure to natural water. The diagnosis of epistaxis due to nasal hirudiniasis mainly relies on the detection of leeches through anterior rhinoscopy or endoscopic examination, and it is necessary to differentiate it from the common causes of epistaxis. The primary treatment is the thorough removal of leeches, supplemented by nasal irrigation or anti-infective measures. This study emphasizes that in endemic areas or in the context of relevant exposure history, leech infestation should be included in the differential diagnosis of intractable epistaxis in children to improve clinical vigilance and avoid misdiagnosis or missed diagnosis.
Significance Statement
Nasal leech infestation is a rare but easily misdiagnosed cause of pediatric recurrent epistaxis, especially in children exposed to freshwater. This successful case demonstrates that intranasal 2% lidocaine combined with negative pressure suction is a safe and effective strategy to remove adherent and retractable nasal leeches. It also emphasizes detailed investigation of exposure and systematic examinations to avoid missed diagnosis and severe bleeding complications in suspicious cases.
A 6-year-old child presented to the Department of Otorhinolaryngology with a 3-day history of recurrent epistaxis of the left side. Ten days before presentation, the patient had outdoor activity in a ditch. She developed intermittent nasal bleeding one week later and initially sought medical attention at a local township health center, where she was diagnosed with rhinitis-related epistaxis. Despite intravenous treatment with antibiotics and hemostatic agents, her nasal bleeding symptoms did not show significant improvement. Anterior rhinoscopy identified a live leech that resides in the left nasal cavity. Cranial CT (CT) further demonstrated a 2.7 cm strip-like isodense lesion within the left nasal fossa (Figure 1a). Routine blood examinations revealed elevated levels of lymphocytes and eosinophils: white blood cell count 7.93×109/L (reference range: 4–10×109/L), lymphocyte percentage 50.10% (reference range: 20%–40%), absolute lymphocyte count 3.97×109/L (reference range: 1.39–3.19×109/L), eosinophil percentage 9.50% (reference range: 0.8%-5.3%) and absolute eosinophil count 0.75×109/L (reference range: 0.05–0.35×109/L). Integrating the patient’s medical history, clinical manifestations and imaging findings, a definitive diagnosis of nasal leech infestation was made. The patient was removed from the leech under general anesthesia. Given the soft body texture of the leech and strong mucosal adhesion, conventional forceps extraction was infeasible and operative manipulation caused the leech to retract upward into the nasopharynx. Subsequently, 5 ml of 2% lidocaine solution was sprayed intranasally to paralyze the parasite, followed by a complete successful removal of the leech using a negative pressure suction device (Figure 1b and c). Intraoperative nasal endoscopy revealed mild mucosal erosion and focal bleeding at the posterior margin of the left middle turbinate (Figure 1d).The patient’s epistaxis resolved immediately after leech extraction. Postoperatively, nasal irrigation with normal saline was administered daily for five consecutive days to promote mucosal repair. The child achieved an uneventful recovery, with no recurrent bleeding or complications observed during the 4-month follow-up period. (a) Results of the computed tomography of the paranasal sinuses, transverse view. (b) Nasal endoscopy showing leech aspiration with a negative pressure suction tube. (c) The intact leech that was removed. (d) Nasal endoscopy showing a small amount of ulceration and blood oozing on the surface of the posterior end of the middle turbinate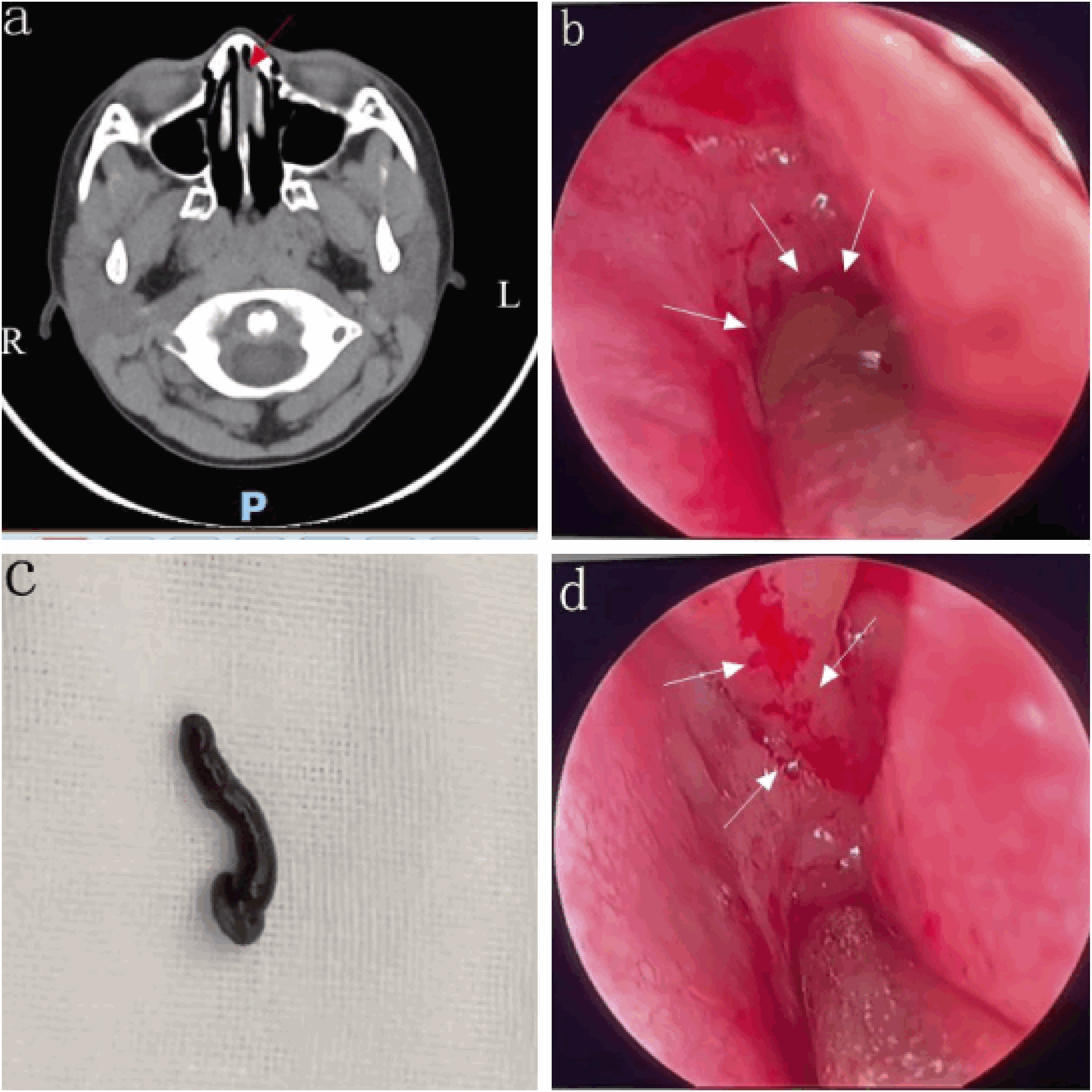
Leech infestation is mainly caused by contact with contaminated water and is a rare etiology of epistaxis. Although reports of leeches carrying pathogens are extremely rare and the risk of infection from their bites is usually low, they can still cause massive bleeding, which can lead to hemorrhagic shock or even death. 1 Therefore, for patients with unexplained epistaxis and a history of freshwater exposure, the possibility of leech infestation should be considered.
For patients with suspected leech infestation, examinations such as complete blood count, anterior rhinoscopy or nasal endoscopy, and CT should be performed. Eosinophilia is associated with many causes; however, the most common cause worldwide is related to parasitic infections. 2 Anterior rhinoscopy is a simple procedure that uses a nasal speculum or otoscope to examine at least one-third of the anterior nasal cavity. 3 However, nasal endoscopy can magnify the anterior nasal structures and directly visualize the posterior nasal structures and nasopharynx. This procedure helps identify the bleeding site (anterior or posterior) and directly treat active or recurrent bleeding. In young children, it is also common practice to use an otoscope to examine the anterior nasal cavity. 4 If a leech is found in the body, a CT scan may be useful to exclude multiple attached leeches.5,6
The present case indicates that, for epistaxis, to avoid misdiagnosis and improper treatment, a detailed investigation of the history of exposure to freshwater is essential. Further examinations are required, including complete blood count analysis, rhinoscopy, or CT, to rule out the possibility of leech infestation. A 2% lidocaine spray holds potential application value in nasal leech extraction: It can prevent leech escape during the clamping procedure and induce leech paralysis before removal using a leech negative pressure suction catheter. 7 Written informed consent for treatment, as well as for the publication of this report and any potential future publications, was obtained from the patient’s legally authorized representative and every effort was made to ensure the patient’s anonymity.
Footnotes
Acknowledgments
The authors thank the patient for granting permission to publish this information.
Ethical Considerations
Ethical approval is not required for this study in accordance with local guidelines. The authors declare that appropriate written informed consent was obtained from the legally authorized representative of the patient for the publication of details of his medical cases and any accompanying images.
Authors Contributions
Concept or design: CW,PL,FD,CZ.
Acquisition of data: CW,PL.
Analysis or interpretation of data: CW,PL,CZ.
Drafting of the article: CW,PL.
Critical review of important intellectual content: CW,PL,FD,CZ.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Original contributions presented in the study are included in the article.