
Abstract
Residual cholesteatoma is a known potential pitfall of surgical resection. While most patients with suspected residual disease undergo second-look surgery or magnetic resonance imaging (MRI) for surveillance, the very long-term consequences of subclinical residual cholesteatoma are rarely described. We present the case of a 64-year-old male who presented with severe otalgia and dizziness 45 years after his last otologic surgery. Subsequent examination and imaging revealed a giant cholesteatoma with significant intracranial extension, developed over nearly half a century.
Introduction
Cholesteatomas are keratinized squamous epithelium that can affect the middle ear, mastoid, or other parts of the temporal bone, and can be acquired or congenital.1,2 Left untreated, these lesions cause progressive bone resorption through both mechanical pressure and the activation of complex inflammatory cascades. 3 Erosion typically begins in the middle ear, affecting the ossicles, most commonly the incus, and can extend to the semicircular canals or the petrous apex. 4 Alternatively, cholesteatomas may be destructive in the mastoid and temporal bone, with erosion through the tegmen mastoideum into the middle cranial fossa, or into the posterior cranial fossa and lead to intracranial infections or abscess formation. 2
Surgical eradication is the primary treatment, typically utilizing canal wall up (CWU) or canal wall down (CWD) mastoidectomy. While CWU surgery is more physiological and preserves ear anatomy, it is associated with a higher residual disease rate than CWD surgery, 5 often necessitating second-look procedures. To lower recidivism rates, supplementary tools like otoendoscopy, 6 lasers, 7 and more recently, optical coherence tomography 8 have been adopted.
Additionally, MRI has been found to be highly sensitive for detecting residual cholesteatoma in the vast majority of patients with a low false-positive rate. 9 Long-term, cholesteatomas can lead to horizontal canal destruction, facial nerve involvement, and tegmen destruction, among others.2,10,11 We present a case of a residual cholesteatoma that grew over a 45-year period to extend into the middle cranial fossa with displacement of the brain.
Case Presentation
A 64-year-old man presents with a 5-month history of progressive left ear pain without discharge. The pain had become so severe that his primary care physician had prescribed hydrocodone. For the past few weeks prior to presentation, he had developed progressive dizziness. His otologic history was notable for three prior otologic surgeries on his left ear. The patient reported that the first two surgeries were performed in 1973, at the age of 12, and the third in 1980, at the age of 19. In the 45 years since his last surgery, he had not experienced any otologic complaints.
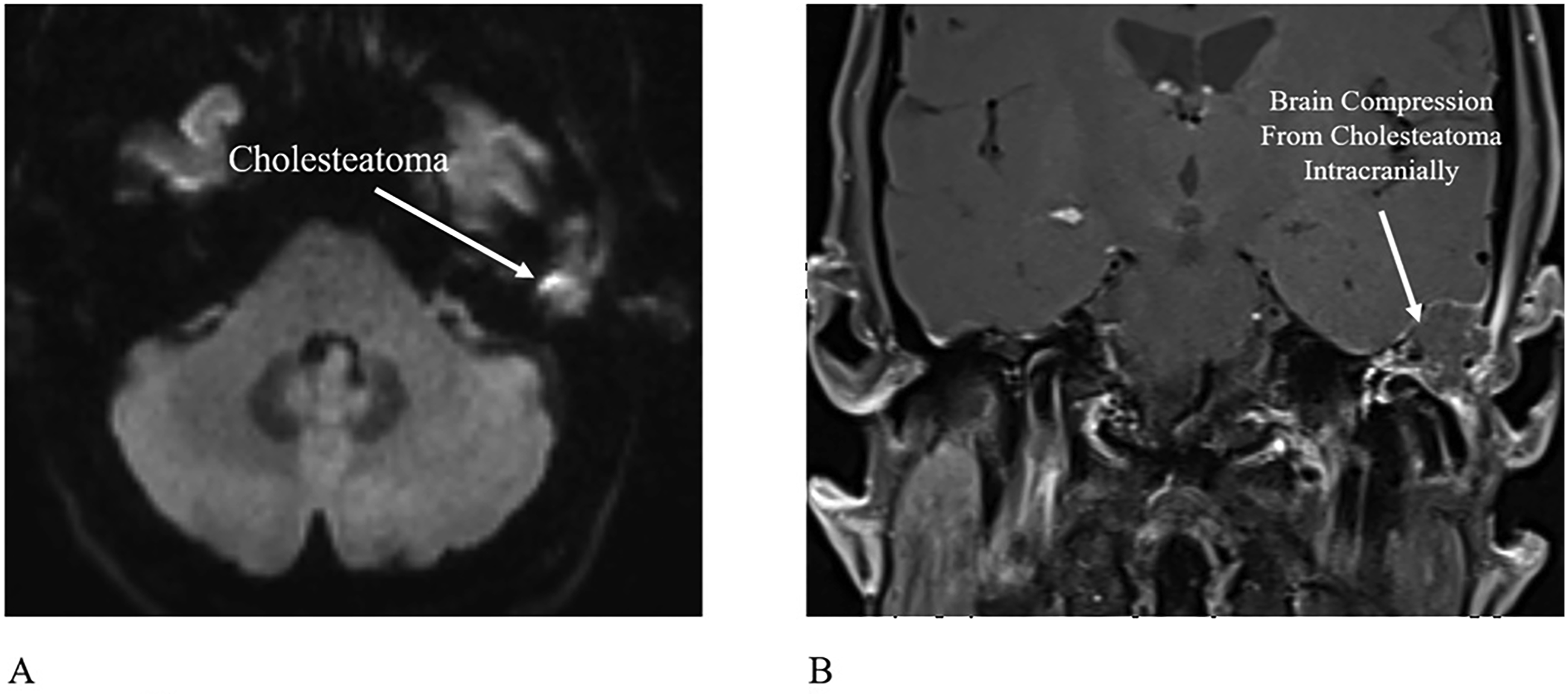
On physical examination, the left ear canal showed exposed bone along its posterior bony wall, with a soft bulge positioned superiorly within the canal. The tympanic membrane (TM) showed post-operative changes but was intact. Subsequent imaging included a computed tomography (CT) scan of the temporal bone and an MRI of the internal auditory canal. The CT scan revealed evidence of a previous mastoidectomy with a destructive mass containing calcification, eroding through the tegmen mastoideum with extension into the middle cranial fossa (Figures 1A and B). The MRI showed an isointense mass on the T1 post-gadolinium and T2 sequences. It showed diffusion restriction on the axial diffusion-weighted imaging (DWI) sequence and was isointense on the Apparent Diffusion Coefficient (ADC) map (Figures 2A and B). (A). Axial CT image of the left temporal bone at the level of the internal auditory canal (IAC) demonstrating a defect in the tegmen with calcification within the cholesteatoma in the zygomatic root. (B). Coronal CT image at the zygomatic root level showing calcification (white dots) within the cholesteatoma extending intracranially. GG: geniculate ganglion; PSC: posterior semicircular canal (A). Axial DWI MR image showing hyperintensity (brighter than brain (white)) in left temporal bone. (B). Coronal T1 post-gadolinium MR image showing compression of the temporal lobe with rim enhancement of the cholesteatoma from surrounding granulation tissue and dural enhancement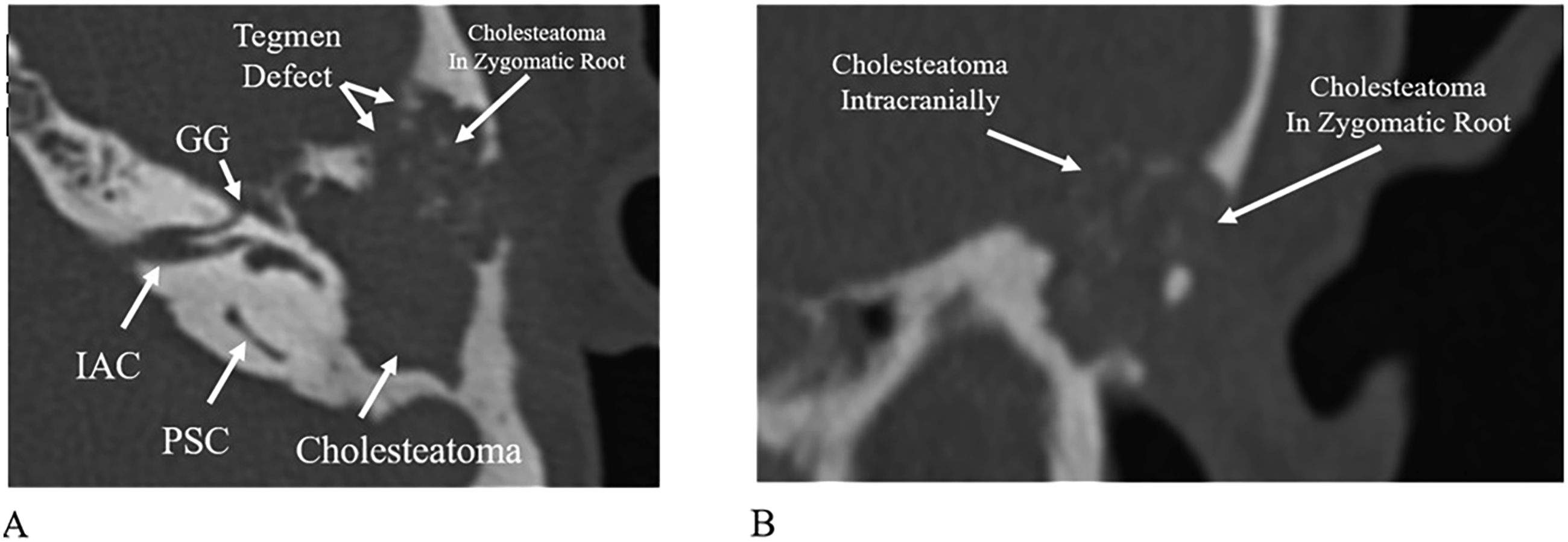
We utilized a partial canal wall down approach and encountered cholesteatoma with a fibrous granulation capsule. The cholesteatoma had displaced the middle fossa dura superiorly and extended into the zygomatic root. Blunt dissection using a duckbill elevator was used between the fibrous granulation capsule and the dura to separate the cholesteatoma from the dura (Figure 3A). No dural violations occurred. Drilling was necessary in the zygomatic root to fully expose the anterior extent of the cholesteatoma. After the cholesteatoma was fully extirpated, the external auditory canal was reconstructed using fascia in contact with the canal skin, cartilage under the fascia, and bone pâté covering the cartilage. Bone pâté was also used to cover the dura (Figure 3B). Due to the large size of the defect, Stryker Direct Inject hydroxyapatite bone cement was used to fill in the rest of the defect (Figure 3C). (A). Intraoperative image showing cholesteatoma surrounded by fibrous granulation separated from the dura. (B). Intraoperative image of left sided surgery showing bone pâté on the tegmen and canal defects. (C). Intraoperative image showing hydroxyapatite bone cement filling the defect between the bone pâté covering the dura and reconstructing the canal.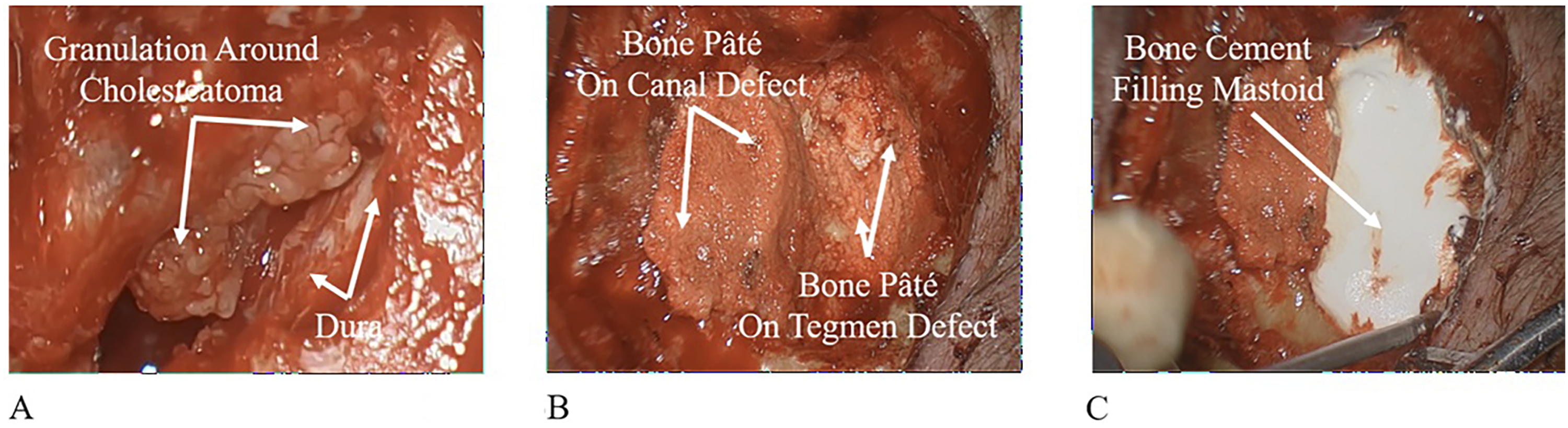
Discussion
This case underscores the importance of lifelong surveillance in patients with cholesteatoma. This case is remarkable for its long-time latency period and its unique clinical presentation, suggesting that microscopic residual tissues can undergo an extraordinarily slow, subclinical regrowth before manifesting as an intracranial condition. One key implication is that the risk of postoperative cholesteatoma might not be fully identified through short-term follow-up windows. Recent pooled analyses show that recurrence estimates increase as follow-up duration extends, highlighting a “long tail” of disease risk that can cause delayed presentations.5,12 Terminology is important when interpreting postoperative disease. The European Academy of Otology and Neurotology and the Japanese ontological Society (EAONO/JOS) consensus statements distinguish residual cholesteatoma, regrowth from incompletely removed epithelium, from recurrent cholesteatoma, new disease formation often arising from a retraction pocket.13,14 Many studies use recidivism to encompass both phenomena.13,14 In this patient, the exceptionally long interval between surgery and detection is compatible with slow-growing residual disease that remained clinically silent until it reached a size producing pain, dizziness, and skull-base involvement. Consistent with this concept, Geven et al described patients presenting with giant recurrent or residual cholesteatoma after intervals ranging from 2 to 50 years and emphasized the need for long-term follow-up strategies. 15
To our knowledge, this is the first reported case of residual cholesteatoma presenting with the combination of severe, progressive otalgia and dizziness with intracranial extension and brain compression nearly half a century after the primary resection. While a few giant recurrences have been documented after 40 to 50 years, the symptomatic profiles differ significantly from our findings. A study described cholesteatoma extending into the middle cranial fossa 45 years after a radical mastoidectomy; however, that patient presented only with a vague sensation of heat in the head and lacked distinct neurological signs. 16 In contrast, our patient presented with acute, debilitating pain likely from dural irritation that served as a clinical red flag. The temporal lobe compression from a slow growing mass may not cause symptoms unless significant dural irritation occurs as in this case.
The skull base and intracranial extension of this case require special attention. Tegmen defects due to cholesteatoma can create pathways for intracranial involvement and complications, and preoperative prediction of dural exposure can meaningfully affect operative planning and counseling. Motegi et al evaluated CT bone density discontinuities in the middle cranial fossa and found that approximately half were associated with intraoperative dural exposure, suggesting that CT measurements can help anticipate this risk. 17 For patients with cholesteatoma coexisting with major tegmen defects, temporal bone meningoencephalocele, or intracranial involvement, the literature supports tailoring the surgical approach to the size and location of the defect and the extent of disease.18,19 A combined transmastoid-middle fossa approach has been reported as a strategy to achieve complete removal with skull-base reconstruction in cases with middle cranial fossa involvement. 19 The transmastoid portion of the surgery is performed utilizing a canal wall down mastoidectomy providing for excellent visualization for complete removal of the cholesteatoma from the middle ear and mastoid. The middle fossa approach provides good visualization of the skull base and dura, allowing complete removal of cholesteatoma from the dura and the intracranial space. In addition, the temporal craniotomy allows for a bone flap and galeal flap to enable a solid repair of the middle fossa defect. 19 In cases where a dural defect is present, a pedicled temporalis muscle flap can be rotated between the dural defect and the bone flap. 20 In this case, we elected to forego a middle cranial fossa approach due to the age of the patient and discussed with the patient the possibility of the need for a future middle cranial fossa approach if we could not successfully separate the mass from dura. Resection of dura is rarely necessary in separating cholesteatoma from dura and it would not be advisable in a transmastoid approach where a dural repair or patching cannot be effectively performed. In this case we repaired the skull base defect with autologous bone pâté supported with hydroxyapatite bone cement. Direct contact between hydroxyapatite bone cement and dura can sometimes lead to cement breakdown 21
Imaging is essential for the diagnosis and postoperative surveillance of cholesteatoma. High-resolution CT is valuable for evaluating bony anatomy, erosion, and surgical planning, but repeated imaging is not advised due to radiation exposure and CT cannot reliably distinguish cholesteatoma from other postoperative soft-tissue changes and should be interpreted alongside MRI.22-24 Non–echoplanar diffusion weighted imaging (DWI) MRI offers high diagnostic accuracy for detecting residual or recurrent disease and is superior to older echoplanar imaging (EPI) techniques. 25 However, early postoperative DWI may miss small lesions and has limited negative predictive value in some settings, 26 while false positives can occur due to cartilage used for obliteration or inflammatory changes. 9 Therefore, imaging findings should be interpreted in a clinical context and, when necessary, confirmed with serial imaging before revision surgery. 9 We recommend yearly postoperative MRI using non-echoplanar diffusion-weighted imaging on a 1.5T scanner, as this minimizes skull base distortion. Surveillance is continued annually for three years, with a final scan at five years to rule out recurrent disease.
Conclusion
This case highlights the potential for extraordinarily delayed presentation of residual or recidivistic cholesteatoma, with clinically silent regrowth occurring over decades before manifesting as symptomatic intracranial disease. It reinforces the importance of long-term, and potentially lifelong, surveillance following cholesteatoma surgery. Persistent or unexplained otologic symptoms should lead to thorough evaluation with both CT and diffusion-weighted MRI. Early recognition and appropriate surgical management are essential to prevent advanced skull-base erosion and intracranial complications.
Footnotes
Acknowledgements
The authors have no acknowledgements to declare.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Hamid R. Djalilian holds equity in Elinava Technologies, and Cactus Medical LLC. He holds equity and is a consultant to NeuroMed Tinnitus Clinic and Finally Quiet!. Dr. Djalilian has equity in NeuroMedCare LLC, Elinava Technologies, and Cactus Medical LLC. The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.