
Abstract
Laryngeal schwannomas are extremely rare, accounting for approximately 0.1% of benign laryngeal neoplasms. Those arising from the aryepiglottic fold are even rarer, and classic symptoms include dysphagia or globus sensation. Isolated chronic cough as the sole presentation is rare in schwannoma. We report a 72-year-old female with persistent cough for 10 years, found to have a large round mass on the posterior edge of the right aryepiglottic fold. Intraoperative frozen section and postoperative immunohistochemistry confirmed the diagnosis of schwannoma. She underwent successful endoscopic transoral resection using a low-temperature plasma knife (coblation). Complete tumor removal was achieved with minimal blood loss, and her cough improved markedly. No recurrence was noted at 6 months. This case provides a valuable clinical reference for the minimally invasive management of similar lesions.
Keywords
Case Presentation
A 72-year-old female patient presented with a 10-year history of persistent cough. She denied dysphagia, globus sensation, hoarseness, nausea, vomiting.Video laryngoscopy revealed a pinkish, smooth-surfaced, round mass on the right aryepiglottic fold.The mass changed position with phonation, showed no obvious infiltration or destruction, and partially obscured the glottic area (Figure 1).Physical examination findings other than laryngoscopy were unremarkable. No masses were palpable in the neck, and no facial paralysis was observed.1-3 The patient refused to undergo any imaging examinations but consented to intraoperative frozen section and postoperative immunohistochemical analysis. Laryngoscopic findings: A round mass located above the glottis at the posterior margin of the right aryepiglottic fold(1a);On expiration, the mass obscures the supraglottic region(1b); The tumor base originates from the posterior margin of the right aryepiglottic fold(1c)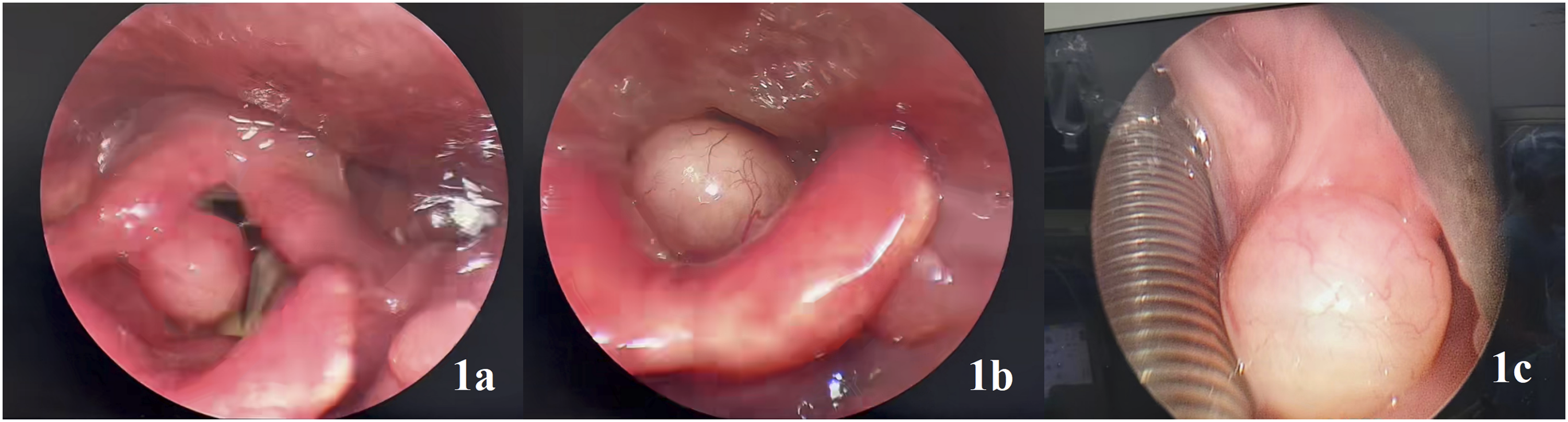
The patient had a medical history of hypertension and self-reported carotid artery plaque, for which she was receiving regular pharmacologic treatment with amlodipine, candesartan/hydrochlorothiazide, rosuvastatin, and ezetimibe.
Family history: Father deceased (cerebral infarction), mother deceased (lung cancer). Two brothers deceased (coronary heart disease and lymphoma, respectively). No family history of genetic or hereditary diseases.
Based on the clinical manifestations and laryngoscopic findings, a preliminary diagnosis of a laryngeal mass (likely benign) was made. Differential diagnoses included granular cell tumor, hemangioma, lymphangioma, lipoma, leiomyoma, which can be distinguished by intraoperative frozen section and postoperative immunohistochemical (IHC) analysis.
Surgical Method
Surgical approaches for laryngeal masses include transoral, transcervical, and combined techniques. In recent years, transoral laser microsurgery and transoral robotic surgery have also been reported for selected laryngeal lesions. In the present patient, the tumor was located on the right aryepiglottic fold, well-defined, and with good mobility, making it suitable for a transoral approach. Therefore, the decision was made to perform endoscopic transoral resection using a low-temperature plasma knife (coblation) under general anesthesia.
Surgical Procedure
Under general anesthesia, a laryngoscope was inserted to expose the glottis. Endoscopic examination revealed a round, well-circumscribed tumor located in the supraglottic region, specifically at the posterior margin of the right aryepiglottic fold. The tumor was gently grasped with a cup forceps and retracted medially. Coblation was then used to dissect precisely along the tumor margins, achieving complete en bloc resection. Hemostasis was obtained with an epinephrine-soaked cotton pad. The total estimated intraoperative blood loss was approximately 1 mL.
Postoperative Results
The resected specimen measured approximately 1.2×1.0 cm (Figure 2A). Histopathological and immunohistochemical analyses confirmed a benign spindle cell mesenchymal tumor consistent with schwannoma (S-100 and SOX10 positive, focal CD34 expression, Ki-67 1%). To prevent postoperative bleeding and laryngeal edema, the patient received nasogastric tube feeding for 7 days. Postoperatively, her chronic cough improved markedly, facial nerve function was House-Brackmann grade I, and swallowing function was normal. At 6-month follow-up, laryngoscopy showed well-healed mucosa with no tumor recurrence(Figure 2B and C). Postoperative condition: Complete resected tumor specimen (2a); At the one-month postoperative follow-up, the mucosa of the wound surface had recovered well (2b, 2c)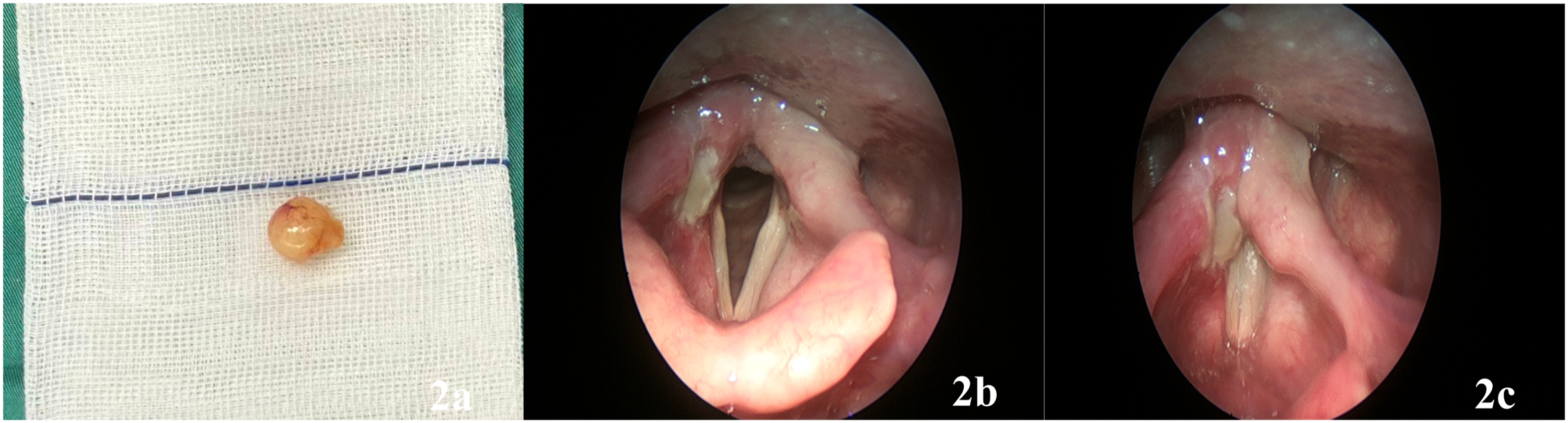
Discussion
Schwannomas are benign, slow-growing, encapsulated peripheral nerve sheath tumors derived from Schwann cells, histologically defined by Antoni A (cellular, palisading) and Antoni B (loose, myxoid) areas, with diffuse S-100 and SOX10 positivity. 1 They account for only 0.1–1.5% of all benign laryngeal neoplasms. 2 A systematic review by Wong et al reported a mean age of 48 years, and the false vocal fold as the most common primary site. 3 Complete surgical excision offers excellent prognosis, but recurrence remains possible. Several immunohistochemical markers have been investigated as potential predictors of recurrence or aggressive behavior in schwannomas. A meta-analysis of vestibular schwannomas confirmed that higher Ki-67 indices correlate with recurrence or progression after surgery. 4 In the present case, the tumor showed a Ki-67 proliferation index of approximately 1%, well below the proposed threshold of 4.85% for predicting peripheral nerve sheath tumor relapse. Moreover, strong and diffuse SOX10 expression was preserved, which is considered favorable, as loss of SOX10 expression has been associated with increased anaplasia and higher relapse risk. 5 The absence of necrosis, mitotic activity, and significant nuclear atypia further supports the benign nature and low likelihood of local progression after complete resection. Given these features, no adjuvant therapy was administered, and the patient is undergoing regular follow-up.
1. “Deceptive” Laryngeal Disorders: Why do Middle-Aged Women Present Mainly With a Single Long-Term Cough?
The patient’s long-standing (10-year) cough as the sole symptom is noteworthy, as hoarseness or dysphagia—typical “alarm” signs of laryngeal neoplasms—were absent. 6 This unusual presentation may be related to the complex anatomy of the supraglottic larynx.Sensory innervation of the supraglottic larynx is provided almost exclusively by the internal branch of the superior laryngeal nerve (IbSLN). 7 The IbSLN gives off three divisions, with its middle branch running along the aryepiglottic fold—the exact tumor location in our patient—which is richly supplied with mechanoreceptors and chemoreceptors. 8 Activation of these receptors initiates the cough reflex arc via the IbSLN and vagus nerve to the nucleus tractus solitarius. Mechanical stimulation of the supraglottic area produces cough exclusively dependent on an intact superior laryngeal nerve. 9 Thus, a small tumor in the aryepiglottic fold can mechanically trigger cough without affecting the vocal folds or recurrent laryngeal nerve, explaining the absence of hoarseness. Furthermore, schwannomas grow exceptionally slowly-consistent with the patient’s decade-long unchanged dry cough—indicating chronic, low-grade mechanical stimulation of IbSLN terminals without motor nerve invasion.
From a clinical teaching perspective, this case reinforces two critical lessons. First, an isolated chronic cough, even without classic laryngeal symptoms, should not be automatically attributed to benign causes such as postnasal drip, asthma, or reflux. Up to 61% of patients with chronic cough and a normal chest radiograph harbor an underlying laryngeal lesion, and although most are benign, malignancy must be ruled out. 10 Second, laryngoscopy should be performed early in any patient with unexplained chronic cough, and submucosal lesions must be considered even when the overlying mucosa appears normal—so-called silent supraglottic neoplasms are known to delay diagnosis.
2. Transoral Coblation for Aryepiglottic Schwannomas: A Comparative Review of Surgical Techniques
For schwannomas located in the aryepiglottic fold, a variety of surgical approaches are available. These can be broadly categorized into: (1)open transcervical approaches (e.g., laryngofissure), (2)transoral laser microsurgery(TLM), (3)transoral endoscopic non-laser techniques, including cold-steel microsurgery, radiofrequency coblation, and transoral robotic surgery (TORS). Compared with traditional open surgery, the advantages of transoral coblation are clear. A laryngofissure approach typically requires a tracheostomy for airway protection and carries the risk of postoperative vocal fatigue and dysphonia. Although it may be necessary for voluminous or deeply invasive tumors, the procedure inevitably injures overlying laryngeal mucosa and compromises normal laryngeal architecture. 11 In contrast, coblation performed through the natural orifice leaves no external scar, avoids tracheostomy, and enables rapid recovery of voice and swallowing. 12
A more nuanced comparison is between coblation and CO2 laser—the current reference standard for transoral laryngeal surgery. While CO2 laser is effective, it has limitations in hemostasis and produces a zone of thermal damage up to 500 μm wide. 13 Coblation, using a bipolar radiofrequency field at 40–70 °C, induces minimal collateral thermal spread (<100 μm) while providing simultaneous cutting and coagulation. 14 This difference is clinically relevant in the aryepiglottic fold, where preservation of sensory innervation (via the internal branch of the superior laryngeal nerve) and motor function is paramount. Recent literature has begun to advocate coblation for laryngeal schwannomas. Wang et al concluded that transoral endoscopic excision, particularly when performed with coblation, is highly recommended for its excellent visualization and ability to completely excise the tumor. 15 In a canine vocal fold model, coblation resulted in complete re-epithelialization by postoperative day 7 with no injury to the underlying vocalis muscle, and less inflammation than that reported for CO2 laser. 16 Moreover, in a histopathological comparative study, coblation achieved thermal damage depths comparable to CO2 laser, and for a benign encapsulated schwannoma, minor irregularities at the cut edge do not affect complete resection or recurrence. 17 Compared with TORS, coblation offers similar advantages of a transoral route but with significantly lower cost, shorter learning curve, and broader availability, making it a more cost-effective option for benign lesions. 18 The present case aligns with these findings: coblation provided a blood-less surgical field, allowed meticulous separation of the tumor from the aryepiglottic fold, and permitted immediate extubation.
3. Limitations and Outlook
This report has several limitations. First, the patient declined preoperative MRI or CT, which could have better defined the tumor’s extent and its relationship with the paraglottic space. However, intraoperative findings confirmed a well-encapsulated lesion that was completely excisable. Second, longer follow-up is ongoing, although the benign biological behavior of this tumor suggests a low risk of late recurrence. Third, regarding the technique itself, coblation may be less suitable for highly vascular or paraglottic-extending tumors. Despite these limitations, transoral low-temperature coblation remains a safe, effective, and highly minimally invasive option for aryepiglottic schwannomas. It offers oncologic safety comparable to CO2 laser, with potentially superior hemostasis and a favorable tissue-sparing profile. We recommend that coblation be considered alongside CO2 laser as a first-line transoral technique for these rare benign tumors.
Supplemental Material
Footnotes
Acknowledgments
The case report was written by Xiaoxiao Luo, Hangzhou, China. The contributions of each author are as indicated in the “Author Contributions” section.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or series of cases.
Consent to Participate
The patient in this case report has provided written informed consent. The patient confirmed and agreed to the conduct of research, publication, and the use of her photos and other case data. The signed written informed consent form was documented in the patient’s medical record.
Consent for Publication
The patient is aware and agrees that the article may be published in an open access manner. The signed written informed consent form was documented in the patient’s medical record.
Author Contributions
Concept and design:Xiaoxiao Luo. Acquisition, analysis, and interpretation of data:Xiaoxiao Luo,Liya Ren,Pengkai Liao. Drafting of the manuscript: Xiaoxiao Luo. Critical revision of the manuscript for important intellectual content: Xiaolin Cao; Jing Li.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed receipt of the following financial support for the research,authorship, and/or publication of this article: This work was supported by the Construction Fund of Key Medical Disciplines of Hangzhou (Clinical Research and Evaluation, grant No. 2025HZGF04); and the West Lake Pearl Special Support Talent Fund (grant No. 50247) to Jing Li (3841).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data in this article: images, imaging data, etc., can be obtained by sending an email to:
Supplemental Material
Supplemental material for this article is available online.