
Abstract
Objective
The purpose of this study was to investigate screening practices for celiac disease in patients with type 1 diabetes across North America. The research question investigated was whether diabetes centers screen for celiac disease in type 1 diabetes more frequently than other facilities.
Research Design and Methods
A survey with 27 questions on screening practices for celiac disease in patients with type 1 diabetes was designed by experts in celiac disease and diabetes. Surveys were sent by email to diabetes educators and dietitians throughout the United States and Canada between December 2010 and May 2011.
Results
There were 514 respondents from 484 endocrine clinics, diabetes clinics, private practices, community nutrition centers, and inpatient centers. Thirty-five percent of work locations screened for celiac disease, with endocrine clinics reporting screening at the highest frequency (80%). Tissue transglutaminase was the most common screening test used. The most frequently recommended treatment of confirmed celiac disease was a gluten-free diet. However, only 71% of respondents recommended biopsy in patients with positive serologies. Most respondents (55.3%) reported that the gluten-free diet resulted in symptom improvement in the majority of patients.
Conclusions
Staff at endocrine clinics were more likely to suggest screening for celiac disease in patients with type 1 diabetes. Both low screening frequency as well as inconsistency in management of positive celiac disease serological tests indicated an increase in education regarding celiac disease in patients with type 1 diabetes is required. In addition uniform guidelines should be developed.
The association between celiac disease and type 1 diabetes was first noted over 40 years ago1,2 and since then has been established in numerous studies.3-6 Celiac disease and type 1 diabetes are autoimmune diseases that affect genetically susceptible individuals. In celiac disease, the ingestion of gluten, a protein found in wheat, barley, and rye, damages the small intestinal villi causing malabsorption of nutrients. Celiac disease can also affect the hematological, neurological, musculoskeletal, and reproductive systems. This leads to a wide variety of symptoms in patients with celiac disease. Celiac disease can develop at any age. Diagnostic investigations for celiac disease include serological screening tests, tissue transglutaminase (TTG), endomysial antibody (EMA), and deamidated gliadin peptides (IgA and IgG DGP), but small intestinal biopsy is generally required to confirm villous atrophy, the current gold standard of diagnosis. Currently, the only treatment for celiac disease is a strict gluten-free diet.
In type 1 diabetes, the trigger is not known, and damage to the islet cells in the pancreas results in the need for administration of exogenous insulin. Type 1 diabetes generally develops during childhood or young adulthood and treatment includes insulin injections and dietary manipulation. Both celiac disease and type 1 diabetes are associated with HLA class II genes on chromosome 6p21. 7 The prevalence of celiac disease in North America is estimated to approach 1% of the general population 8 and has increased fourfold over the past 50 years. 9 Celiac disease occurs more frequently in type 1 diabetes than in the general population, with estimates varying from 2.4% 10 to 16.4%. 11 The prevalence of celiac disease in patients with type 1 diabetes is on the rise. 12 The risk of celiac disease may vary by age of diagnosis of type 1 diabetes. Results of a multicenter study in Italy found the risk of having both celiac disease and type 1 diabetes is 3 times higher in children diagnosed with type 1 diabetes at less than 4 years of age compared to those greater than 9 years of age. 13
Despite the higher prevalence of celiac disease in type 1 diabetes, there is no consensus on screening patients with type 1 diabetes for celiac disease. 14 The American Diabetes Association recommends screening select patients based on symptoms and treating patients with biopsy-confirmed celiac disease with the gluten-free diet. 15 The International Society for Pediatric and Adolescent Diabetes recommends treating patients with symptomatic celiac disease and comments on the controversy and uncertainty over treating asymptomatic celiac disease in type 1 diabetes.8,16 The North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition recommends routine screening of all children with type 1 diabetes but notes that the treatment may not have an effect on glycemic control. 17 The National Institute of Health Consensus Conference on celiac disease recommends screening of type 1 diabetes patients with symptoms and treating biopsy proven celiac disease. 18 The Canadian Diabetes Association recommends screening patients with symptoms and notes that for those with no symptoms, treatment is controversial. 19
Those that advocate routine screening of type 1 diabetes patients for celiac disease20-22 emphasize that patients with type 1 diabetes may have no symptoms, unrecognized symptoms,5,22 or symptoms that are only recognized retrospectively 23 and that there are complications of untreated celiac disease. Symptoms for celiac disease in patients with type 1 diabetes can include gastrointestinal complaints, failure to thrive, growth impairment or short stature, delayed puberty, anemia, iron deficiency, dental enamel defects, 24 hypoglycemia and a reduction in insulin requirements,25,26 arthralgias, laboratory evidence of malabsorption, and elevated liver enzymes.5,14,27,28 Complications of untreated celiac disease include osteopenia/osteoporosis,29,30 lymphoma,21,31,32 infertility and reproductive disorders, 33 and neurological complications. 34 Adherence to a strict gluten-free diet appears to have a protective effect.21,32,35 Osteoporosis is a complication of both celiac disease29,30,36,37 and type 1 diabetes, 38 posing an increased fracture risk. 5 One study found an increased risk of heart disease in people with both celiac disease and type 1 diabetes 39 compared to healthy individuals. Another study indicated that adults with undetected celiac disease in type 1 diabetes had worse glycemic control and a higher prevalence of retinopathy and nephropathy compared to diabetes patients without celiac disease. 40 Studies vary in their findings of the effects of the gluten-free diet on glycemic control and body weight in type 1 diabetes patients.41,42
Some authors argue against screening programs for celiac disease in type 1 diabetes, 5 claiming the diagnosis can affect quality of life with the long-term outcome of subclinical celiac disease in type 1 diabetes not fully investigated. 5 It is unclear what screening recommendations, if any, are being followed in North America. The objective of this study was to investigate screening practices for celiac disease in patients with type 1 diabetes in various facilities throughout North America. The research question investigated was whether diabetes centers screen for celiac disease in patients with type 1 diabetes more frequently than other facilities.
Research Design
A descriptive research design was utilized to gather information about screening practices for celiac disease in patients with type 1 diabetes. This is the first study looking at what type of screening methods are employed by various health care facilities. The survey was developed by 2 dietitians with expertise in celiac disease, 1 graduate student, and 2 gastroenterologists at the Celiac Disease Center at Columbia University. The survey was administered to dietitians at a Diabetes Center in New York City as well as the Academy of Nutrition and Dietetics (formerly the American Dietetic Association) to comment about clarity of items and content. The final survey included 27 questions addressing screening practices, methods for diagnosis, treatment, work location, and credentials of health care providers.
Data Collection Measures
Surveys were sent by email to diabetes educators and dietitians throughout the United States and Canada, including the Diabetes Care & Education Dietetic Practice Group of the Academy of Nutrition and Dietetics, Dietitians of Canada Pediatric Nutrition and the Diabetes Group, Obesity and Cardiovascular Disease Networks, the Canadian Diabetes Association, as well as the Northern Diabetes Health Network. The study was approved by the Institutional Review Board at Columbia University in December 2010 and was administered online from December 2010 until May 2011. The survey included yes/no and multiple choice answers. For some questions, checking multiple answers was allowed. One question required a written response.
Data Analysis
The chi-square statistic for categorical variables (SigmaPlot 2004 for Windows version 9.01, Systat Software Inc, Chicago, Illinois) was used to compare responders’ answers. Comparisons using the chi-square statistic were made for questions in which only 1 answer could be given from the yes/no and multiple choice question types. The results were tabulated as frequency and significance (P value). Respondents were asked to identify their work location. When more than 1 respondent from 1 location completed the survey, the first responder was accepted and all other responses were omitted. This reduced the total number of respondents from 514 to 484. Table 1 includes common symptoms identified by all respondents (n = 514) for purposes of diagnosing celiac disease. Tables 2 through 4 provide descriptive data from 3 separate questions on the survey from each location (n = 484).
Common Symptoms Identified That Initiate Screening for Celiac Disease (N = 189/514) a
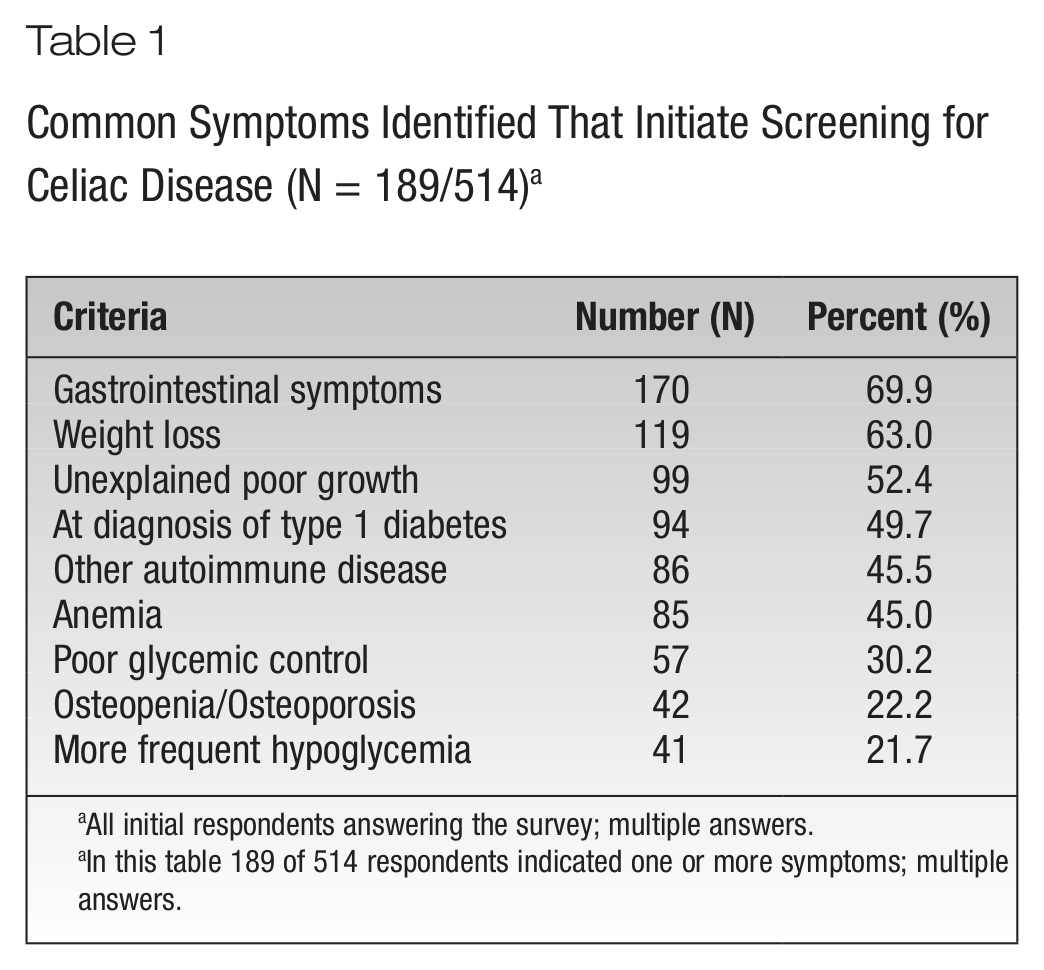
All initial respondents answering the survey; multiple answers.
In this table 189 of 514 respondents indicated one or more symptoms; multiple answers.
Primary Work Location Versus Questions Asked About Celiac Disease Diagnosis
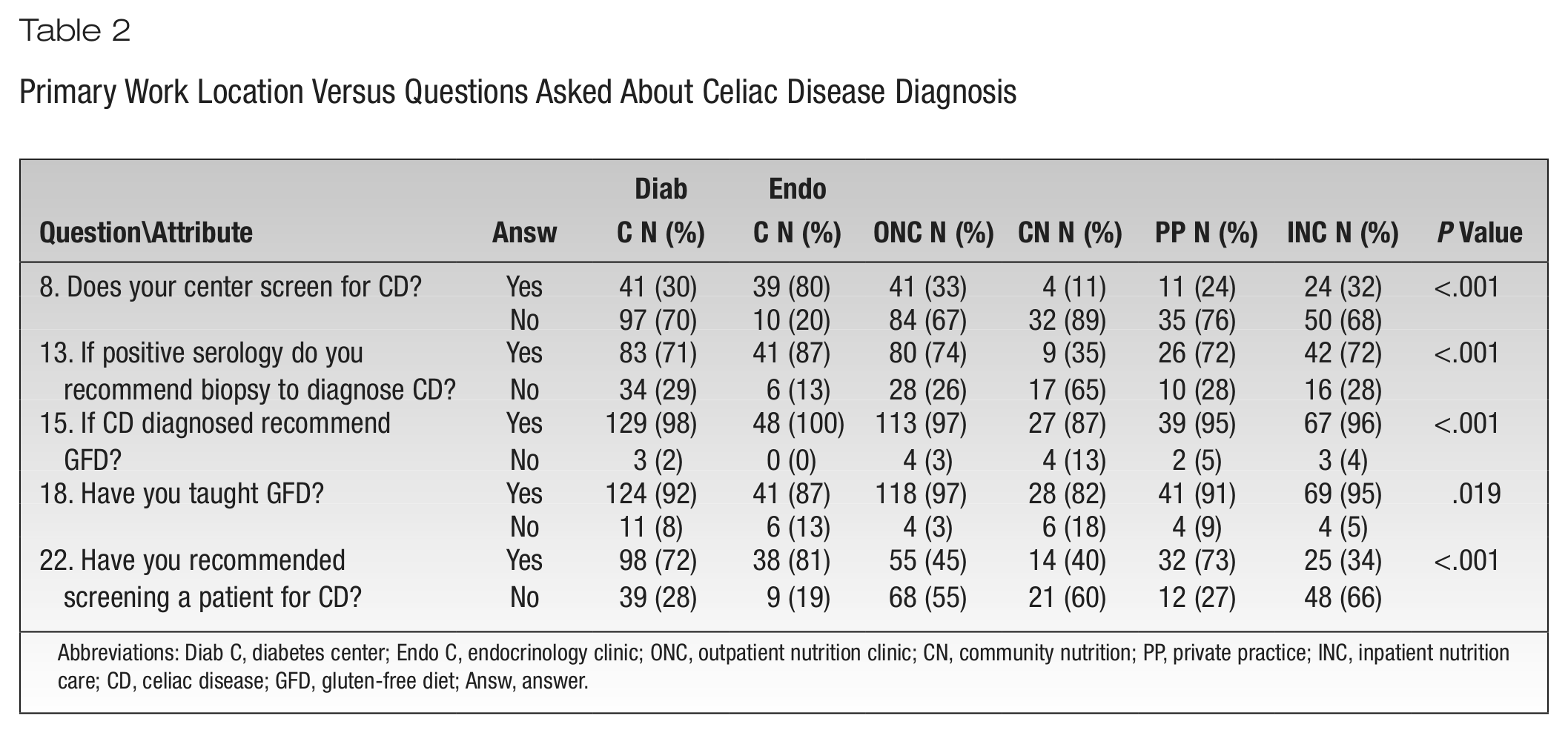
Abbreviations: Diab C, diabetes center; Endo C, endocrinology clinic; ONC, outpatient nutrition clinic; CN, community nutrition; PP, private practice; INC, inpatient nutrition care; CD, celiac disease; GFD, gluten-free diet; Answ, answer.
How Often Do You See People With Type 1 Diabetes Versus Screening Strategies for Celiac Disease?
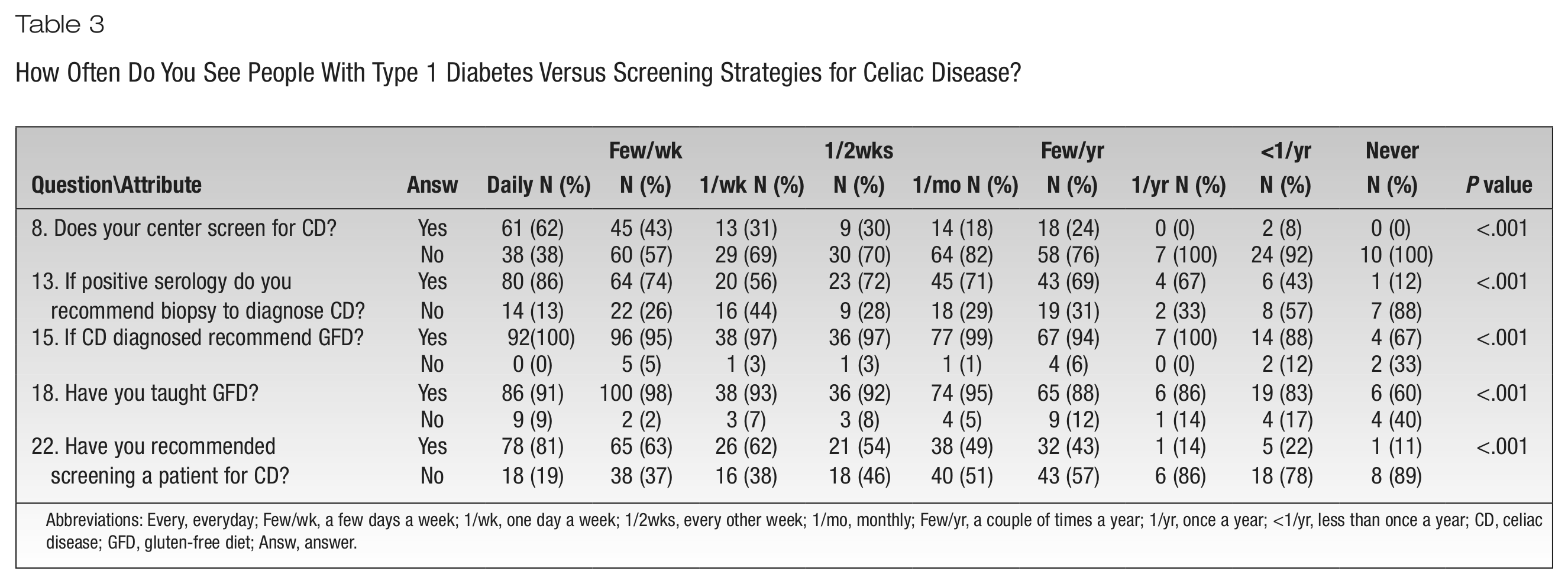
Abbreviations: Every, everyday; Few/wk, a few days a week; 1/wk, one day a week; 1/2wks, every other week; 1/mo, monthly; Few/yr, a couple of times a year; 1/yr, once a year; <1/yr, less than once a year; CD, celiac disease; GFD, gluten-free diet; Answ, answer.
How Often Do You See People Diagnosed With Type 1 Diabetes and Celiac Disease Versus Screening Strategies for CD?
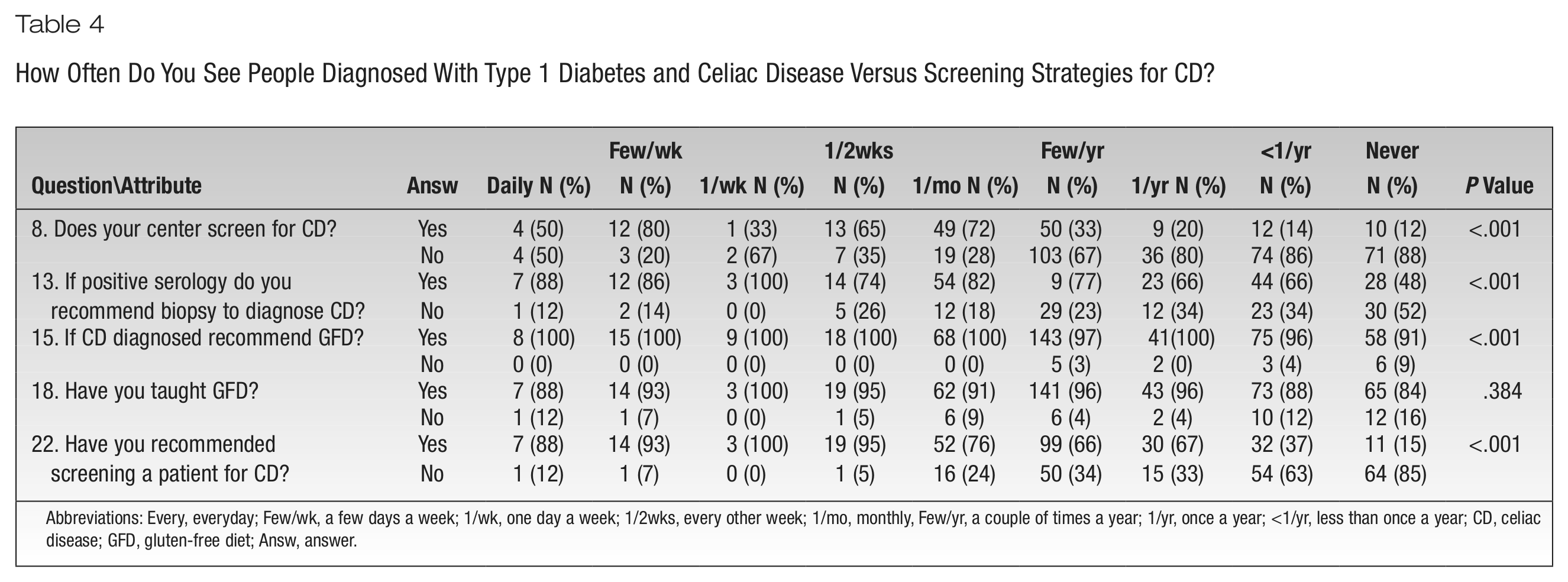
Abbreviations: Every, everyday; Few/wk, a few days a week; 1/wk, one day a week; 1/2wks, every other week; 1/mo, monthly, Few/yr, a couple of times a year; 1/yr, once a year; <1/yr, less than once a year; CD, celiac disease; GFD, gluten-free diet; Answ, answer.
Results
Of the 514 respondents, 45% were registered dietitians, 10% diabetes educators (nurses), and 58% both dietitians and diabetes educators. Ninety-one percent of respondents were located in the United States and 9% in Canada. Within the United States, there were 201 respondents from the Northeast (43.1%), 90 respondents from the Southeast (19.3%), 80 respondents from the Northwest (17.2%), and 95 respondents from Southwest regions of the country (20.4%). Of the 484 total work locations in the United States and Canada from which survey results were obtained, 29.6% were diabetes centers, 28.6% outpatient nutrition clinics, 20.6% inpatient nutrition care, 13.1% endocrine clinics, 10.7% private practices, and 8.3% community nutrition sites. Respondents saw patients with type 1 diabetes more frequently than those with celiac disease and type 1 diabetes, while 42% of respondents saw patients with both diseases once a year or less (vs 8.7% for type 1 diabetes alone).
Out of 514 responders 35.2% report that they do screen for celiac disease. Tissue transglutaminase was the most common screening test used (56.8%) followed by anti-gliadin antibody (28.6%) and anti-endomysial antibody (20.5%). While 26% of respondents did not know which tests were used to screen for celiac disease, a good number (36%) did not answer the screening test question.
Respondents were asked at what frequency they screened for celiac disease and for this question they could give multiple answers. Of those locations that screen for celiac disease (35.2%), 60.4% screened patients that had symptoms and 42.9% were screened at initial diagnosis of type 1 diabetes. Additionally, 17% of respondents screened annually, 6% screen every 2 years, 3.8% screened every 3 years, and 2.7% screen every 5 years. The most common criteria given to screen for celiac disease were gastrointestinal symptoms (Table 1). Only 71.3% of locations recommend a biopsy with positive celiac disease antibodies, but 96.2% recommend treatment with a gluten-free diet. Community nutrition locations were less likely to recommend biopsy and treatment with a gluten-free diet (Table 2). Locations where patients with diabetes were seen more frequently were more likely to screen for celiac disease and recommend biopsy with positive serology (Table 3). At locations where patients with both celiac disease and type 1 diabetes were seen frequently, dietitians were more likely to recommend patients get screened for celiac disease (Table 4).
The diabetes educator who was a dietitian (61.1%) was the most common person to educate patients on the gluten-free diet, followed by inpatient dietitians (16.0%); only 6.9% of gastroenterology dietitians were the educators about the gluten-free diet. Dietitians who work in community nutrition, inpatient nutrition, and outpatient nutrition clinics were less likely to recommend a patient with type 1 diabetes be screened for celiac disease (Table 4).
A majority (74.5%) of survey respondents indicated that less than 25% of patients reported symptoms prior to diagnosis of celiac disease. Respondents reported that most patients improved after starting a gluten-free diet (55.3%); 40.1% of respondents indicated symptoms improved in “some” patients. Only 4.5% of patients were reported to have no symptom improvement. Symptoms that improved included gastrointestinal symptoms (86.6%), glycemic control (33%), and other symptoms (30.5%), and 48.9% answered that patients felt better on the gluten-free diet despite not being aware of symptoms prior to diagnosis of celiac disease.
The effects of the gluten-free diet on glycemic control were not clear; most answered that it varied from patient to patient (67.7%) and some answered that it resulted in improved control (24.4%), 5.6% reported no change, and 2.3% reported it worsened control. Ninety-two percent of dietitians had instructed patients on the gluten-free diet; most had taken steps to learn about the diet and the most frequently utilized resources for learning about the gluten-free diet were the Academy of Nutrition and Dietetics (formerly the American Dietetic Association) and national celiac disease organizations. The majority of respondents (83.8%) agreed with the statement “I am comfortable teaching the gluten-free diet.” Steps taken to learn about the gluten-free diet included lectures (73.2%), workshops (40.4%), books (74.6%), and continuing education self-study courses (49.5%); 8.1% had taken no formal steps to learn about the diet. Effective ways to learn more about the gluten-free diet were noted to be webinars (75.3%), self-study courses (62.7%), lectures (44.7%), and workshops (43.1%).
Discussion
Surveys were sent to dietitians and diabetes educators in the United States and Canada to investigate screening practices for celiac disease in patients with type 1 diabetes. Prior to conducting the survey, investigators considered that diabetes centers would screen for celiac disease more frequently than other facilities. This was not confirmed; it was found that endocrine clinics screened most often. Overall, screening for celiac disease in type 1 diabetes was low. Thirty-five percent of facilities screened patients for celiac disease. The reason for endocrine clinics screening more often is likely related to the diversity of medical conditions that endocrine clinics handle including thyroid illness and Addison’s disease as well as growth issues in children and as a result, they are more accustomed to celiac disease and more comfortable testing for it. Of those facilities that screened for celiac disease, 60% answered “We only screen patients that have signs or symptoms of celiac disease.” For the same question respondents could provide multiple answers—42.9% screen at initial diagnosis of type 1 diabetes, 17% screen annually, 6% screen every 2 years, 3.8% screen every 3 years, and 2.7% screen every 5 years. Such variability reflects lack of uniform guidelines. Respondents reported that less than 25% of patients with type 1 diabetes have classic or recognizable symptoms for celiac disease, however, respondents also reported that the majority of patients had symptom improvement (55.3%) with the gluten-free diet. Only 4.5% of patients were reported to have had no symptom improvement with treatment. Symptoms reported to improve with the gluten-free diet include gastrointestinal symptoms (86.6%), glycemic control (33%), and other symptoms (30.5%). Almost 49% of respondents answered that patients feel better on the gluten-free diet despite not being aware of symptoms prior to diagnosis of celiac disease. With such a heavy emphasis on testing for celiac disease only if symptoms are present, it was not known whether those that specialize in diabetes are aware of the great variety of symptoms patients with celiac disease manifest and how they have changed over the recent decades with a prominent reduction in the classical malabsorptive symptoms. 43
Only 71.3% of facilities recommend biopsy in patients with type 1 diabetes that had positive celiac antibodies. Community nutrition locations were the least likely to recommend biopsy. Treatment with a gluten-free diet was recommended by most respondents for patients diagnosed with celiac disease (96%). Many respondents omitted questions about the types of tests used to diagnose celiac disease, and of those that did respond, 26.5% did not know which tests were used. This could indicate that the dietitians are not recommending celiac screening and/or that the facilities do not have screening protocols. Future studies should query physicians about screening protocols used because dietitians’ and educators’ actions may well reflect the knowledge and opinions of their physician colleagues with whom they work.
When asked whether they had ever recommended someone be screened for celiac disease, 42.6% said no; dietitians in private practice and endocrine clinics as well as respondents who saw patients with both celiac disease and type 1 diabetes more frequently were most likely to recommend someone be screened for celiac disease. Among centers that never encountered a patient with a dual diagnosis of type 1 diabetes and celiac disease (n = 81), 88% did not screen patients for celiac disease. This lack of screening, even in symptomatic patients, will lead to a low likelihood that these centers will encounter a dual-diagnosed patient.
The diabetes educator who was a dietitian was the individual who most commonly instructed patients with type 1 diabetes about the gluten-free diet as opposed to a dietitian who specialized in celiac disease and/or gastroenterology. Ideally, the person teaching the gluten-free diet must have expertise in both celiac disease and type 1 diabetes. Of note, 92% of dietitians that completed the survey had taught the gluten-free diet at some point and had taken steps to learn about the diet. There was however considerable interest in receiving more education on the gluten-free diet.
There were several limitations to the study. The survey was administered in North America; studies of other countries would be useful. The survey was directed at dietitians and diabetes educators (dietitians and nurses) where as a more accurate reflection of the specific screening practices (eg, which serologies are ordered) should include physicians. Respondents were not asked questions about follow-up procedures of patients with both diseases and this should be further investigated to ensure that once diagnosed with celiac disease, patients are seen by both a dietitian and a gastroenterologist with expertise in celiac disease as well as continuing to have diabetes care.
Conclusion and Implications
There are no uniform practices for screening for celiac disease in type 1 diabetes in North America. In fact, screening is not routinely performed. Endocrine clinics were most likely to screen for celiac disease among the many different sites that care for patients with type 1 diabetes. Both the low screening frequency as well as inconsistency in management of celiac disease in patients with type 1 diabetes reflects the inconsistent screening practice guidelines. Screening recommendations should be uniform between advisory bodies. There is likewise a need for additional education of dietitians about celiac disease diagnosis and management in patients with type 1 diabetes.
Footnotes
Contributions:
SS research and developed survey, wrote manuscript, researched data; EC performed the statistical analysis; SC helped to develop survey and edit manuscript; NJ helped to develop survey and edit manuscript; SM performed initial statistical analysis; BL edited survey before sending, edited manuscript; PG edited survey before sending, edited manuscript.
funding
This study was unfunded.