
Abstract
Purpose
The purpose of this study was to explore the everyday barriers to and practices of low-income patients managing their diabetes.
Methods
The study team conducted semistructured qualitative interviews with 20 patients with type 2 diabetes who were receiving care at safety-net clinics in Southern California. Transcripts were analyzed using grounded theory to identify emergent themes across participants.
Results
Participants described managing diabetes with limited financial resources as often a game of balance and negotiation, whereby purchasing healthy foods is abandoned because of a more pressing concern in their life. Although participants described strategic attempts at incorporating healthy dietary practices for diabetes management into their daily decisions, these efforts were significantly impeded by the existence of persistent and seemingly insurmountable barriers.
Conclusions
Although the challenges that low-income patients face in managing their diabetes may seem insurmountable at times, there are several ways that health care providers can help reduce the burden of these challenges, including tailoring their recommendations to incorporate the everyday socioeconomic environment of patients and engaging in clear, open communication with patients.
“Individualization is the cornerstone of success.”
1
The organizing principle underlying diabetes management is increasingly shifting away from an emphasis on standardized measures of adherence toward an individualized, patient-centered approach.1-5 Patient-centered care incorporates the needs, preferences, and values of patients as key factors in clinical decisions 6 and emphasizes the patient as an equal partner in determining the best treatment. 7 Open communication between patients and their health care providers is a critical component of patient-centered care and collaborative decision making.8,9 In the context of diabetes management, patient-centered care has been shown to have a positive effect on patient satisfaction,10,11 self-care practices,12-14 and clinical outcomes such as glycemic control.15,16 However, the majority of diabetes care practices occur outside the clinic walls in the everyday dietary, lifestyle, and self-care decisions of patients. This reality supports the need for health care providers to understand and incorporate the social, economic, and environmental supports and constraints that patients face each day when recommending the best treatment path. 2 This is particularly important for diabetes care among low-income patients.
For low-income patients, the everyday management of diabetes can be riddled with challenges including inconsistent access to health care, lack of access to affordable healthful foods, limited transportation, and lack of safe housing.17-21 These barriers have been documented by numerous studies22-27; however, disparities among low-income populations continue to persist. In an effort to explore why, this study used qualitative methods to examine the everyday practices of low-income patients struggling to manage diabetes amid competing economic demands. Qualitative research methods are well suited for understanding the lived experience of diabetes self-care because they capture the detailed perspective of individual patients often missed by surveys alone and help to identify shared experiences across patients. 28
Methods
Research Design
The qualitative data presented in this article were collected as part of a larger mixed-methods research study designed to test the efficacy of a behavior support intervention for diabetes management among underserved patients with poorly controlled type 2 diabetes (hemoglobin A1C ≥8.0). The research team designed the study to have 2 central components: (1) a 2-group randomized controlled trial (RCT), and (2) in-depth interviews with 10% of participants enrolled in the trial. In the RCT, patients with type 2 diabetes mellitus were recruited from 3 academic primary care practices (n = 22) and 1 community-based safety-net clinic (n = 179) that provides care for the poor and uninsured in the Los Angeles, California, area between August 2008 and November 2009 (N = 201).
Participants randomized to the experimental group received a behavior support intervention package consisting of a 24-minute educational video and workbook designed to increase patient knowledge and awareness of various ways to manage diabetes. Additionally, participants in the experimental group received up to 5 telephone sessions with a trained diabetes educator focused on addressing individual difficulties and needs for diabetes management. Participants in the control group received an educational brochure on diabetes self-care developed by the National Institutes of Health. The study collected several clinical measures including baseline and 6-month hemoglobin A1C levels as well as demographic data from each participant. The design and outcomes of the RCT are described in greater detail elsewhere 29 ; however, it should be noted that the study did not find a significant effect in favor of the experimental intervention. The study was reviewed and approved by the UCLA Institutional Review Board (ClinicalTrials.gov Identifier: NCT00668590).
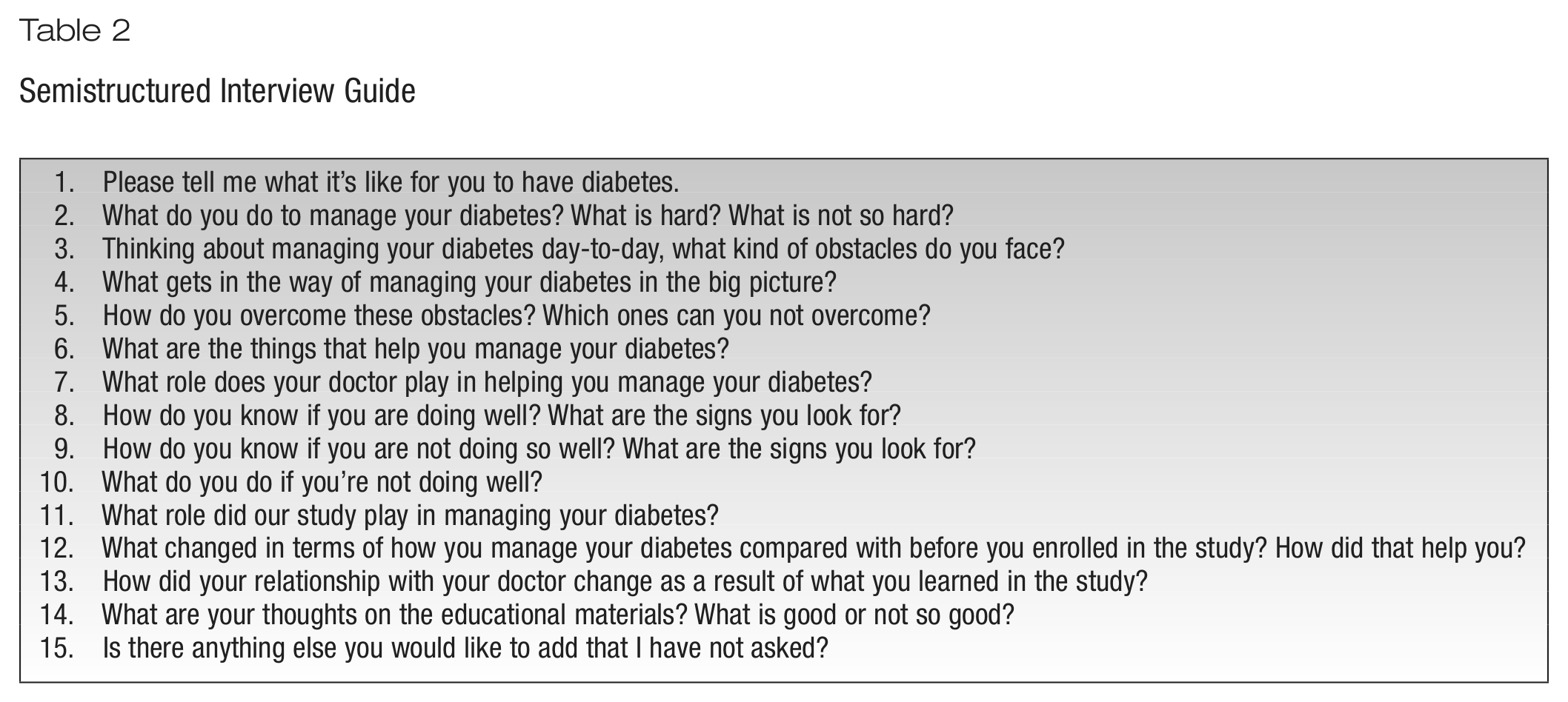
The research team designed the qualitative component of the study to explore the everyday practices of low-income patients managing their diabetes. The research team randomly selected 10% (n = 20) of research participants as potential candidates for the qualitative interviews. Table 1 describes the demographics and average hemoglobin A1C levels of interview participants. The research assistant (V.U.) approached each participant at the completion of the last clinic visit for the RCT and asked whether he or she would be willing to be interviewed. All patients approached for the interview agreed to participate. A 2-page, semistructured interview guide (Table 2) was developed outlining broad, open-ended questions allowing participants to describe daily diabetes self-management from their perspective while also ensuring consistency of topic areas among interviews. Interviews lasted on average 37 minutes. All interviews were digitally recorded and transcribed by research assistants with previous transcription experience. A research assistant (V.U.) conducted the majority of the interviews in English after receiving interview training from an experienced qualitative researcher (D.L.F.). Additionally, the qualitative team supervised and reviewed all interview activities (S.G.M., D.L.F.). Four interviews were conducted in Spanish by a bilingual research assistant and translated into English following transcription.
Interview Participant Demographics and A1C levels
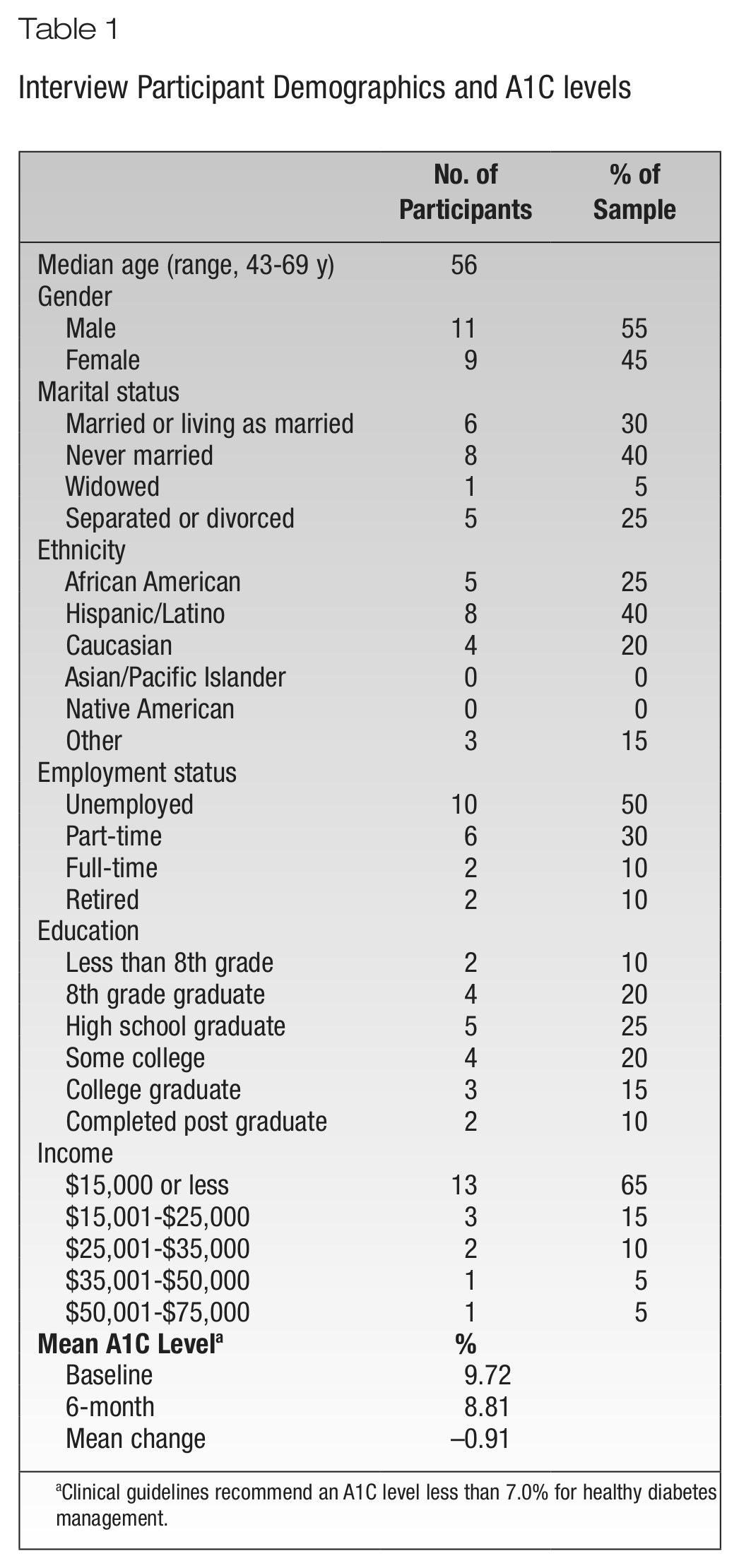
Clinical guidelines recommend an A1C level less than 7.0% for healthy diabetes management.
Semistructured Interview Guide
Qualitative Data Analysis
Drawing from grounded theory, the analytic team used a constant comparative method to analyze interview transcripts. 30 Analysis involved 2 levels of coding (open and axial) to identify recurrent conceptual themes and codes in the interview transcripts. During the open coding stage of analysis, the analysis team (K.A.S.R, S.G.M., C.K.T., V.U.) carefully read through the interview transcripts in order to identify, label, and organize the data into categories. Using these categories—or codes—the research team created the coding dictionary.
In the second level of coding, the team reviewed the transcriptions again and, using qualitative data analysis software (Atlas.ti), applied the codes to narrative passages that best illustrated the meaning of each code. This software helped to facilitate analysis (rather than conducting analysis independently) by allowing the analysis team to organize the data by codes and then produce analytic reports based this organization. In the final stage of analysis, the team reviewed the analytic reports to identify emergent themes across participants based on frequency and demonstrative intensity of quotations.
Results
Participants described managing diabetes with limited financial resources as often a game of balance and negotiation, whereby purchasing healthy foods is abandoned because of a more pressing concern in the participant’s life. Although participants described strategic attempts at incorporating healthy dietary practices for diabetes management into their daily decisions, these efforts were significantly impeded by the existence of persistent and seemingly insurmountable barriers. Additionally, the strategies described by participants differed at times from suggested dietary guidelines for diabetes management, which include incorporating sources of lean protein and fresh produce into one’s diet and eating smaller meals throughout the day rather than skipping or eating large meals. 31 Described strategies and barriers are discussed in the sections below.
Persistent Barriers
Competing demands
Many participants viewed purchasing healthy, often more expensive, food as an unrealistic option due to their difficult financial situation. As one participant stated “[when] push comes to shove, maintaining a picture perfect diabetic diet and lifestyle is not realistic.” In their everyday lives, participants reported needing to prioritize certain expenses such as paying bills or rent over purchasing more expensive foods: You don’t worry about purchasing healthy food when your primary concern is being able to purchase food. [My] priorities have been maintaining food and shelter. Paying the bills kind of has to come first because . . . if not, then it just spirals down the drain because . . . if I get kicked out of the shop then I am screwed. Then [my] health would really go down.
Other participants reported that the cost of fruits and vegetables added to the pressures of maintaining consistent healthy food intake. As described by the participant below, it is sometimes necessary to make sacrifices around healthy food intake, including skipping meals to purchase basic households items needed to survive: Fruits and vegetables are not cheap. And for someone that is not making a lot of money or does not have a lot of money to buy fresh fruits on a daily basis for 30 days a month and . . . they have to maintain their other essentials such as toothpaste, toilet paper, socks, shoes, rent, utilities, how is that? There is no way. . . . Sometimes you have to starve yourself. You have to miss a meal. That’s the way it is.
Many participants reported that lack of sufficient income to care for all parts of their life created additional stress and worry. Patients reported that financial stress amplified the physical and mental effects of living with diabetes and, as this participant stressed, had a direct impact on his physical health. “I’m thinking what am I going to do? The money I have is not enough. This affects me emotionally. Sometimes it will give me headaches and my sugars go up.”
Cycles of food availability
Participants described experiencing cycles of food availability often attributable to unreliable and limited sources of income—whereby periods of food abundance were followed by periods of food scarcity, forcing them to use management strategies to endure each period. The majority of participants did not have full-time employment and survived by securing part-time (often temporary) work and/or enrolling in government assistance programs. The following account illustrates the effects of this intermittent cycle on food choices at different periods throughout the month: If I had more money I wouldn’t worry so much about getting the food that I need, like the fruits and the vegetables . . . because that would be easier to get if I didn’t have to watch every cent that I spent. And usually . . . towards the middle and end of the month [when] I get my checks, I am eating whatever we can find.
In addition to reducing food as money became scarcer, several participants described engaging in overconsumption at periods immediately following receipt of income or as a reward to paying all necessary household bills.
When I finally get my rent paid . . . which is usually by the 5th, it’s kind of like I take the 6th off and then I spend the day in bed and just kind of celebrate. It’s kind of like “ahh . . . I got the f***ing rent paid” and those are some [of] the days I end up going out and getting ice cream or doing something like that.
For this participant and others, they expressed understanding of the negative impact these decisions may have on their diabetes management. However, they still engaged in these “reward” behaviors to celebrate financially surviving another month.
Time, money, and the temptation of unhealthy foods
In the process of speaking with participants, several intersecting factors—including time and the temptation of unhealthy foods—repeatedly arose as playing a significant role in poor eating habits and the inability to manage diabetes well. As one participant explained, “Time management is my obstacle. It’s trying to get all this stuff in to take care of me and to do what I have to do in everyday life.” Participants described the routine of diabetes self-care as overwhelming and eating as yet another obstacle to overcome because it takes time and knowledge to both prepare and select healthy food. As another participant clarified, “it is a lot easier to pick something up and get it on the way to go.” Even though fast food options are typically unhealthy, participants described being drawn to the convenience and price, as they could get seemingly much more caloric value for the cost. As this participant noted: Well yes . . . moneywise, it’s kind of hard because the fruits and vegetables are not cheap, so if you don’t have a steady income to buy what you need as far as fruits and vegetables and even the proteins that you need to have, then you are going to say yes to that quick hamburger that is on sale at McDonald’s for 99 cents. You are going to say yes to all the deals that are out there because that’s what’s available.
As these quotations illustrate, low-income patients are faced with significant, persistent barriers that are tied to environmental, economic, and social factors. However, amid these barriers, our participants also described strategic practices they used in attempting to manage their diabetes.
Strategic Practices
Although diabetes management was challenging, many participants reported strategic practices that they used to improve their dietary choices and manage their diabetes. Participants understood the need to eat more healthy foods; however, because of the costs, participants reporting reducing daily food consumption rather than revising overall eating habits to include more healthy food items as staples in their diets: The food . . . the budget and buying healthy food—that’s kind of hard, but it is easier to control because . . . if I don’t have anything really healthy, I just eat a little bit instead of eating a whole bunch [of unhealthy food] like I used to.
Another participant explained that when he does not have the “special things” (ie, healthier foods) he simply eats less (unhealthy) food. “Eating, sometimes it’s a little problem to have money to buy stuff you know, but I’m trying . . . if I don’t have the special things that I have to eat, I have [to] correct myself. I eat less.”
Participants reported not only reducing food intake but also monitoring their blood glucose less in order to reduce the total cost associated with purchasing these materials. As this participant described, “I don’t have the money. . . . I have to find something else to control. . . . For example, if I have to check my blood 3 times per day, I only check [it] once a day.”
In addition to reducing costs in monitoring materials, participants described bargain grocery shopping including buying food at discount stores instead of traditional supermarkets as an attempt to improve diabetes management with limited financial resources. However, as one participant illustrates in the next excerpt, participants chose not only to bargain shop for reduced prices but also to purchase less healthy food to reduce food expenditures: I’m always looking for a bargain. Sometimes there are things that I just can’t buy so I do without them. . . . Sometimes I go to the store and want to buy some meat; I see that the better quality [leaner] portion is more expensive, so I will buy the cheaper one even if it has a little more fat.
This practice is an example of how strategic choices made to reduce food costs—in this case buy fattier meat because it was cheaper—often went against the recommended dietary guideline to eat sources of lean protein. Other practices described, such as skipping meals and eating smaller portions of unhealthy food rather than improving overall dietary habits, are other examples of strategic practices potentially detrimental to long-term diabetes self-care.
Discussion and Implications
This study presents qualitative data detailing the persistent barriers faced as well as the complex and strategic ways that low-income patients attempt to incorporate dietary change as part of their overall diabetes management. Although the challenges that low-income patients face in managing their diabetes may seem insurmountable, there are several ways that health care providers can help reduce the burden of these challenges, including tailoring their recommendations to incorporate the everyday socioeconomic environment of patients. Recently, there has been a shift in the general recommended approach to diabetes management away from standardized adherence measures to more patient-centered or individualized care. 1 This new shift calls for more flexible views on the long-standing measurement of diabetes management—A1C levels—and asks providers to assess, through open communication, the socioeconomic context of patients in establishing dietary and lifestyle recommendations as well as setting glycemic targets.2,32
This study supports these shifts and highlights how an approach built on patient-centered communication may help providers identify the challenges and constraints that individual patients face each day in managing their diabetes. While in-depth interviews are not feasible within the constraints of the clinical encounter, health care providers can facilitate open communication by engaging in behaviors (such as listening and not interrupting, expressing empathy, and asking about patient’s beliefs and preferences) that invite patients to express their concerns and experiences managing diabetes.33-36 When appropriate, providers may also find asking direct questions about patients’ social and economic situations to be the best route to gathering information. This information can be used to tailor the treatment in ways that best match the recommended guidelines and patient’s lifestyle. Treatment guidelines for low-income patients may require health care providers to compromise their ideal treatment guidelines slightly; however, as evidenced by recent research, flexibility and individualization of guidelines may actually have better health outcomes for patients with diabetes.2,32 Moreover, the act of compromise—based on open, informed communication—may be a key step in creating a partnership between patients and providers.
The results of this study also suggest that health outcomes are not always representative of the time a patient has invested in his or her health. As evaluated by standardized measures, the patients interviewed have poorly managed diabetes, and by some models—such as the health capital model—it may be assumed that these participants are not investing as much time in their diabetes management as are those with better outcomes. 37 However, as is shown by the strategic practices reported by our participants, they are putting significant time and thought into trying to improve their diabetes management regardless of whether these are recommended practices. Persistent barriers such as lack of access to affordable healthful foods in low-income areas may be significantly affecting the payoffs that these participants see in terms of health outcomes. 38 Providers should tailor their recommendations to incorporate the socioeconomic environment of patients to improve the likelihood that patients will be able to incorporate recommended changes and turn time invested into more successful health outcomes. However, as discussed above, this is predicated upon collaborative communication between physicians and patients in which patients are able to communicate the financial barriers they face. Although both patients and physicians have a role to play in facilitating open communication, patients face significant cultural and structural barriers to communicating with their physicians.39,40 Health care providers have the opportunity to initiate and encourage communication from patients by being strong role models of open communication themselves. 33
Limitations
This research is limited in several ways. Results are based on a small sample of 20 participants, and thus these findings cannot be generalized to another location or population. However, the intensity and detail of participants’ experiences in this study provide preliminary data that may be used to design a larger, controlled study to test the experiences described in this study across different low-income populations. Another limitation is the data represented here are patient-reported. This study could be strengthened with the incorporation of observations or tracking of dietary practices as well as documenting of the purchasing practices. Last, this study did not assess the neighborhoods in which participants live. Although numerous studies show that low-income neighborhoods in Los Angeles have fewer healthful food options, this study cannot empirically support patients’ claims to having little access to healthful foods in their lived environments.
Conclusions
Although the majority of diabetes self-care decisions occur outside of the clinical encounter, the clinical encounter is a unique opportunity for the patient and health care provider to come together to share their experiences and expertise and decide together the best treatment plan. This is reliant upon open, collaborative communication between the provider and the patient, which for low-income patients includes sharing information about any financial barriers that may impede their ability to follow recommended guidelines. Not incorporating an understanding of the patient’s everyday social, economic, and environmental factors into the clinical encounter is a missed opportunity for health care providers to facilitate truly patient-centered care and potentially improve the health and quality of care received by the patient.
Footnotes
Acknowledgements
We would like to thank Meghan C. Halley for her insightful review and suggestions on ways to improve this manuscript. Additionally, we would like to thank the Robert Wood Johnson Foundation, the Informed Medical Decisions Foundation, and the University of California, Los Angeles, Resource Centers for Minority Aging Research Center for Health Improvement of Minority Elderly for their support of this study.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Robert Wood Johnson Foundation and the Informed Medical Decisions Foundation. Neither funder had any role in the design, conduct, analysis, or write-up of the research reported. Carol M. Mangione also received support from the University of California, Los Angeles, Resource Centers for Minority Aging Research Center for Health Improvement of Minority Elderly (RCMAR/CHIME under NIH/NIA Grant P30-AG021684), and the content does not necessarily represent the official views of the NIA or the NIH.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.