
Abstract
Purpose
The purpose of this study was to explore the level of physical activity, barriers to physical activity, and strategies used to meet physical activity goals in people with type 2 diabetes (T2DM).
Methods
A descriptive, cross-sectional design was used in a sample of 75 adults with T2DM enrolled in a worksite diabetes disease management program (WDDMP). Participants self-reported the length of time they engaged in moderate-intensity physical activity, the frequency of general and specific physical activity, and barriers to participating in physical activity.
Results
Participants who chose to work on physical activity as part of their diabetes self-management had a higher stage of change for physical activity and participated in more general and specific physical activity than did those participants who did not choose to work on physical activity. Participants who were active reported fewer barriers to physical activity and chose to work on more self-care areas to control their diabetes than did those participants who were inactive.
Conclusions
Participants who chose to work on physical activity participated in more general and specific physical activity and had a higher stage of change for physical activity. Stage of change affects physical activity. While results provide support for the stages of change construct of the transtheoretical model of change, the results do not support that the WDDMP assisted participants in achieving their physical activity goals.
More than 18 million people in the United States have diabetes, and another 7 million people are believed to be undiagnosed. 1 Diabetes often leads to chronic complications, including heart disease and stroke, hypertension, blindness, kidney disease, and nervous system disease. 1 In 2007, the total annual economic cost of diabetes was estimated to be $174 billion, with $116 billion in direct health care costs and $58 billion from lost productivity. 2 These costs represent 1 out of every 5 health care dollars spent in the United States that year. 2
People with diabetes need to learn a variety of behaviors such as meal planning, physical activity, and blood glucose monitoring to manage diabetes. 3 The extent to which people with type 2 diabetes (T2DM) manage their disease is significant because maintaining blood glucose levels as close to normal as possible has been found to reduce the incidence of chronic complications. 4 Benefits from regular physical activity for people with diabetes include improvement of glycemic control, decreased risk for cardiovascular disease, loss of body fat, increased physical fitness, and enhanced psychological well-being. 5 While emotional stress and depression can negatively affect diabetes management, 3 physical activity fosters psychological well-being by its antidepressant effects, antianxiety effects, and increased resilience to stress 6 and may actually improve adherence to the diabetes management plan. 3 While people with diabetes may understand the importance of physical activity as part of their diabetes self-management plan, they often face barriers in starting and maintaining a physical activity program. 7
Barriers to starting and maintaining a physical activity program include the following: no time to fit activity into their schedule, health problems prevent exercising, difficulty in controlling diabetes while exercising, don’t like to exercise, no place to exercise,8,9 physical activity is boring, special equipment is needed, 8 lack of family support, and not viewing exercise as important. 10 After a physical activity goal is identified, individuals need to choose the type of activity in which they want to participate. People with diabetes need assistance not only in developing a physical activity plan but also in overcoming barriers to initiating and maintaining their physical activity plan.
When assisting individuals with diabetes in initiating and maintaining a physical activity program, the clinician must help the individual to understand the effect that physical activity has in controlling diabetes and why it is an important part of a diabetes self-management plan. Once a person is ready to take action and start a physical activity program, realistic individualized goals need to be clearly identified. Generic prescriptions for physical activity do not provide specifics about how to become active and how to do it safely. Also, the types of physical activity the individual likes need to be considered. 11 Once activities are chosen, the individual needs to start the program slowly and gradually increase the intensity and duration to prevent injury. Once the initial physical activity goals are met, goals may be adjusted to increase physical activity duration and intensity.
Disease management is “a system of coordinated health care interventions and communications for populations with conditions in which patient self care efforts are significant.” 12 Maintaining or improving members’ health to reduce treatment costs is a goal of disease management for payers. 13 Worksite health promotion programs have historically reduced absenteeism, increased employee retention, reduced health care costs, and increased employee satisfaction. 14 Education regarding management of diabetes often improves quality of life and reduces costs of treatment. Outcomes of disease management programs include significant decreases in fasting blood glucose15,16 and A1C. 17
The theoretical framework chosen for this study was the transtheoretical model of change (TTM). The TTM postulates that an intentional change in acquiring health-promoting behaviors involves the person progressing through the 5 stages of change: precontemplation, contemplation, preparation, action, and maintenance.18-20 When assisting a person in establishing a physical activity program, clinicians must apply different strategies as the individual moves through the different stages of change. The TTM model guides the development of behavior change interventions. 19
The purpose of this study was to explore the level of physical activity, barriers to physical activity, and strategies used to meet physical activity goals in people with T2DM. Three hypotheses were tested during this study. Hypothesis 1: Participants who have chosen to work on physical activity will have a later stage of change for physical activity than those participants who have not chosen to work on physical activity. Hypothesis 2: Barriers to physical activity will be greater for individuals in the early stages of physical activity adoption compared with individuals in the later stages of physical activity adoption. Hypothesis 3: Beneficial strategies will be greater in later stages of change for physical activity.
Methods
Design
A descriptive, cross-sectional, correlational research design was used to identify the stage of change for moderate-intensity physical activity and to identify barriers to obtaining moderate-intensity physical activity in participants with type T2DM. Participants with T2DM enrolled in a worksite diabetes disease management program (WDDMP) completed self-report questionnaires on demographic data, stage of change for physical activity, frequency of engaging in general and specific physical activity, and barriers to physical activity.
Sample and Setting
The study population consisted of people with T2DM who were participants in a WDDMP offered by a manufacturing company located in the Midwestern United States. Participants in the WDDMP included management employees/retirees, hourly employees/retirees, salaried employees/retirees, or spouses of employees/retirees. The study convenience sample consisted of the 600 people participating in the WDDMP and who met the inclusion criteria.
The WDDMP is a voluntary program whereby health educators assist the person with diabetes to set realistic goals for diabetes self-management and offer suggestions for behavior change and coping strategies to meet the identified goals. Once an individual agrees to be in the WDDMP, a registered nurse makes an introductory telephone call during which health history information is gathered including the individual’s readiness to change behavior with regard to physical activity, healthy eating, healthy coping, foot care, and understanding numbers (blood pressure, cholesterol, glucometer numbers, and A1C). A baseline profile is sent to the participant with a hard copy of WDDMP standards. The WWMP standards is a document that describes how physical activity, healthy eating, healthy coping, foot care, and understanding numbers affect diabetes; it also provides examples of how an individual may start to implement self-management behavior changes. The WWMP standards are based upon the American Diabetes Association standards of medical care. In the first follow-up telephone call, the health educator (a registered nurse or registered dietitian) asks what self-management behaviors the participant wants to work on (eg, physical activity, reducing blood pressure, reducing A1C, etc) and discusses how the participant can start to make changes. The health educator starts to stimulate an interest about lifestyle changes the participant can make and may discuss barriers to making these lifestyle changes. Instead of focusing on delivering initial DM education, the health educator facilitates self-management of diabetes. The frequency of telephone calls is negotiated between the health educator and the participant—the frequency may be every 2 weeks or every 6 weeks. The WDDMP offered by a Midwest manufacturing company assists its participants in meeting their diabetes self-management physical activity goals.
The sample was one of convenience. All participants in the WDDMP who met the inclusion criteria were recruited through a mailing that consisted of 2 letters. The first letter from the physician overseeing the WDDMP served to introduce the research study. The second letter from the investigator explained the purpose of the study, participation requirements, and how to indicate interest of participation. If interested in participating in the study, the participant completed and returned a response form. Packets containing the study materials were sent to potential participants, and the study materials could then be completed at a convenient time and then returned.
Inclusion criteria for this study included participation in the WDDMP for 3 months or longer; diagnosis of T2DM; age at least 18 years; ability to speak, comprehend, and write in the English language; absence of a serious illness that would impair participants from engaging in moderate-intensity physical activity; and ability to give informed consent. Exclusion criteria for this study included residence in a facility where the individual was not responsible for self-management of diabetes.
Procedure
Prior to the beginning of this study, approval for the study was obtained from the Rush University Institutional Review Board and the Bradley University Committee on the Use of Human Subjects in Research. Participants were informed of the proposed study through a mailing from the WDDMP and were invited to participate. Returning the response form from the initial mailing and returning the completed questionnaires implied consent.
Measures
Demographic information
Participants self-reported gender, age, race, educational level, height, weight, employee/retiree/spouse classification, type of diabetes, number of years diagnosed with diabetes, type of diabetes medication used, and self-management behaviors they were currently working on.
Stage of change
The stage of change for physical activity was assessed using the Physical Activity: Staging Algorithm, a 4-item instrument sent via e-mail from W. Velicer (personal communication, July 17, 2003). Each of the 4 questions was answered in a yes-no format. Individuals were categorized into 1 of 5 stages of change using the scoring guide from W. Velicer (personal communication, October 22, 2003). Kappa index of reliability of this instrument over a 2-week period was 0.78 21 and 0.81. 22
Self-management of physical activity
The Summary of Diabetes Self-Care Activities Physical Activity Subscale (SDSCA PAS) is a 2-question, self-report measure that determines the frequency of engaging in general and specific physical activity over the preceding 7 days.23,24 This subscale contains 2 questions. Question 1: On how many of the last 7 days did you participate in at least 30 minutes of physical activity? (0-7 response). Question 2: On how many of the last 7 days did you participate in a specific exercise session (such as swimming, walking, or biking) other than what you do around the house or part of your work? (0-7 response). Scoring for the physical activity subscale included determining the mean number of days for each type of activity.
Barriers
Barriers to physical activity were measured by the Barriers to Self-Care Scale Physical Activity Subscale (BSCS PAS). Eight items were added to the original 8-item subscale; content validity was obtained by computing the content validity index (CVI) based on the evaluation by 2 content experts. A CVI of 0.93 was calculated with a 4-point rating scale. 25 The resulting scale contained 16 items where participants responded using a 7-point Likert scale. Cronbach’s alpha for the revised scale was .704.
Data Analysis
Data were managed using Statistical Package for Social Science (SPSS), version 14, statistical program. Data were cleaned after entry and before analysis. Frequency data were calculated to describe demographic data, stage of change, general and specific activity, and barriers to exercise. Independent samples t tests were analyzed to determine statistical significance of the participants’ stage of change with general and specific physical activity, barriers to physical activity, and self-care activities.
Results
Letters of invitation were sent to 600 individuals enrolled in the WDDMP who met the inclusion criteria. Study materials were sent to 87 individuals (87/600 = 14.5%) who indicated interest in participating in the study. Seventy-five participants (75/600 = 12.5%) returned study materials that could be used for analysis. Characteristics of the sample are listed in Table 1.
Demographic Characteristics a
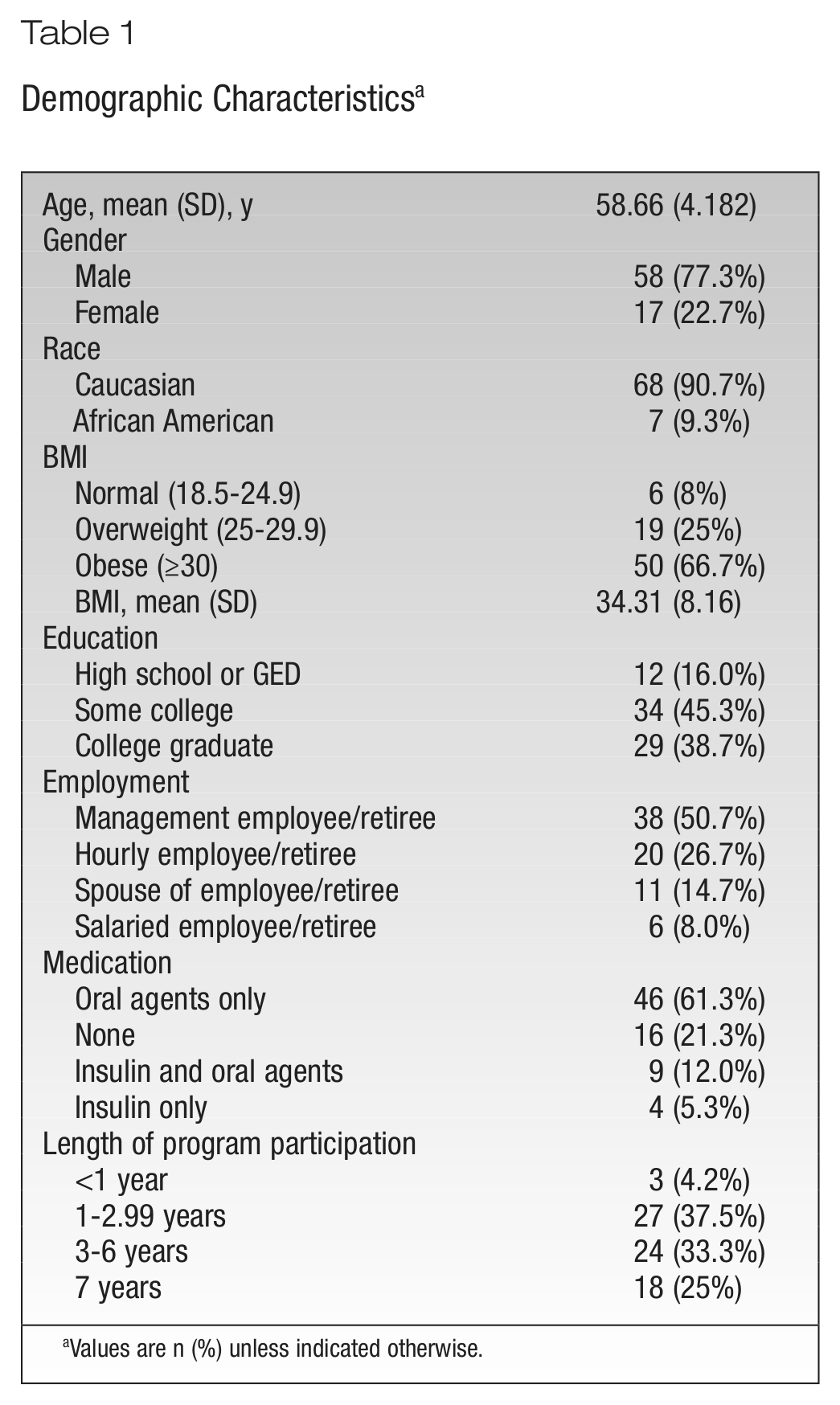
Values are n (%) unless indicated otherwise.
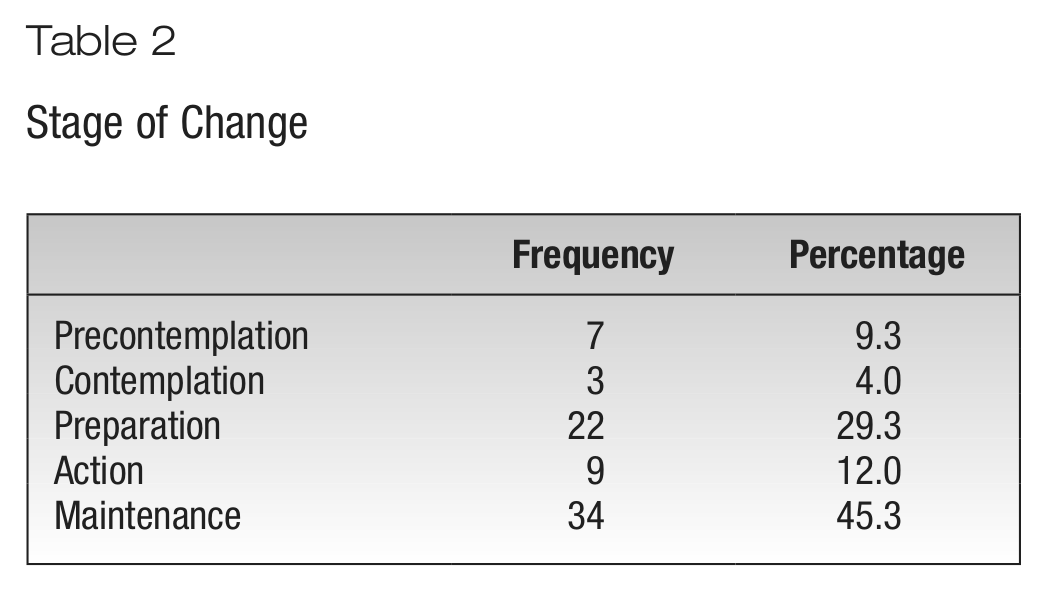
Stage of change for physical activity was measured by the 4-item Physical Activity Staging Algorithm. Nine participants were in the action stage and 34 participants were in the maintenance stage of change. Forty-three (56.3%) participants were physically active. Categories of stage of change for study participants are listed in Table 2.
Stage of Change
The SDSCA PAS measured the frequency of participation in general and specific physical activity over the preceding 7 days. Item 1 measured the number of days the participant participated in general physical activity, which includes activities such as walking the dog, vacuuming, and raking leaves. Results of general physical activity frequency include 21.3% of participants exercising 2 days or fewer, 32% exercising 3 to 5 days, and 46.7% exercising 6 or 7 days per week. Item 2 measured the number of days the participant participated in a specific physical activity session, such as swimming, walking, biking, or an aerobics exercise class. Results of specific activity frequency include 31.1% exercising 2 days or fewer, 35.2% exercising 3 to 5 days, and 33.8% exercising 6 or 7 days per week.
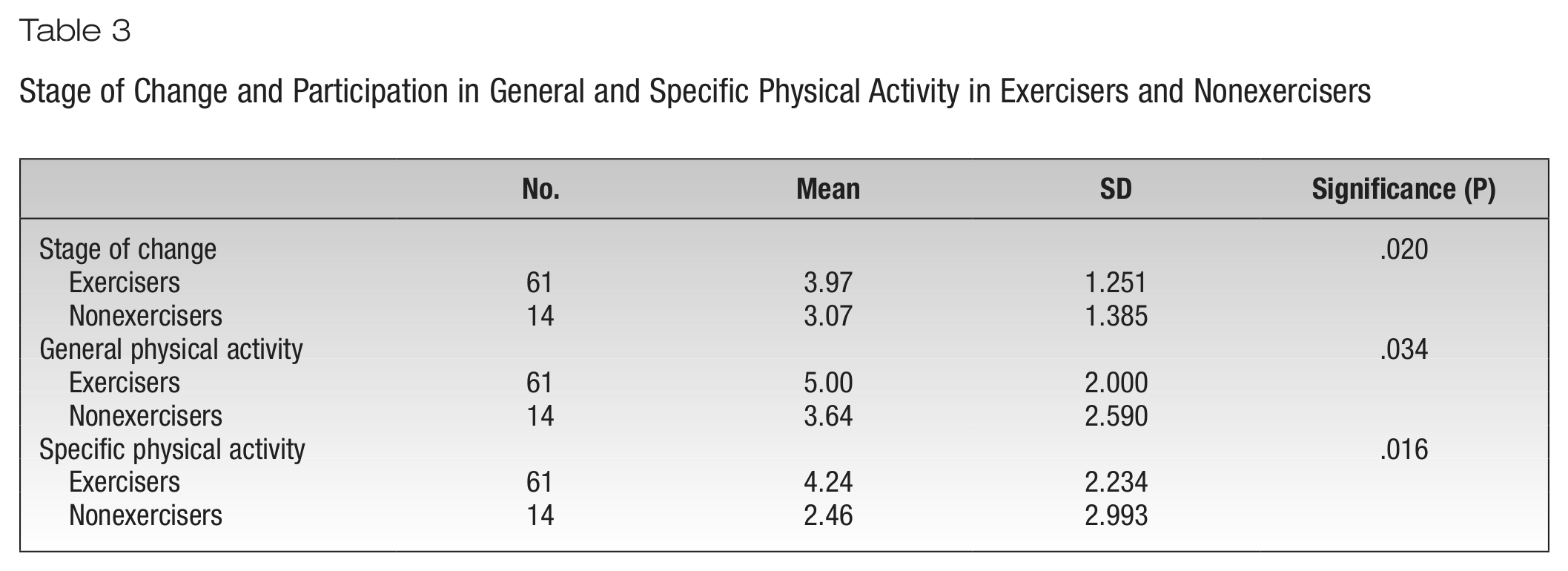
Participants indicated whether they had selected exercise as part of their diabetes self-management in the WDDMP. Independent samples t tests were conducted to determine whether there were differences in the means for physical activity of those participants who chose to work on physical activity (exercisers) compared with those who chose not to work on physical activity (nonexercisers) as part of their diabetes self-management. Participants who chose to work on physical activity (exercisers) participated more often in general physical activity (P = .034), participated more often in specific physical activity (P = .016), and had a higher stage of change for physical activity (P = .020) than those participants who chose not to work on physical activity (nonexercisers). Results for the independent samples t tests are displayed in Table 3. Hypothesis 1 was supported by the data.
Stage of Change and Participation in General and Specific Physical Activity in Exercisers and Nonexercisers
Barriers to physical activity were measured by the BSCS PAS. Since 4 participants did not answer 1 of the items from the BSCS PAS, the mean values of the 3 different items were substituted for the missing data to allow missing cases to be included in the final analysis. Question 12, “I think about how participating in physical activity could change how I manage my diabetes,” is a positive statement, whereas the remaining 15 items in the scale were negative statements. Question 12 was recoded to account for this difference. The reliability coefficient for the 16-item BSCS PAS is 0.704.
A 1-way ANOVA, followed by the Tukey method of multiple comparisons, was conducted to determine whether barriers to physical activity were greater for participants in the early stages of physical activity compared with participants in the later stages of change for physical activity. The means of the perceived barriers to engaging in physical activity were significantly different between the groups (F4,70 = 10.905, P < .001). To isolate the source of the differences, Tukey’s B test was used (critical difference = 1.45, P = .05). The harmonic mean sample size was 7.551 and was used to calculate the critical difference. Results of Tukey’s B test, however, revealed that there were no significant differences between any of the groups. However, the group sizes were not equal and type I error levels are not guaranteed.
A new variable was created to separate those participants who were not physically active according to the Physical Activity Staging Algorithm from those participants who were physically active. An independent samples t test was conducted to determine whether there were differences in the mean barriers scores between the 2 groups. There was a significant difference between the means of the 2 groups (t73 = 5.682, P < .001). The mean barriers of the physically active group were significantly lower (mean = 1.5969, SD = 0.355) than the mean barriers of the inactive group (mean = 2.4471, SD = 0.789).
Independent samples t tests were also conducted to determine whether there were differences in the mean score of general and specific activities between the 2 groups. Results of independent samples t tests revealed that participants who were physically active participated in more general physical activities (t73 = −6.677, P < .001). The general physical activity mean for the physically active group was significantly higher (mean = 5.95, SD = 1.112) than the mean of the inactive group (mean = 3.13, SD = 2.196). Participants who were physically active also participated in more specific activity (t72 = −8.016, P < .001). The specific physical activity mean of the active group was significantly higher (mean = 5.35, SD = 1.602) than the mean of the inactive group (mean = 1.97, SD = 2.025). Hypothesis 2 was supported by the data.
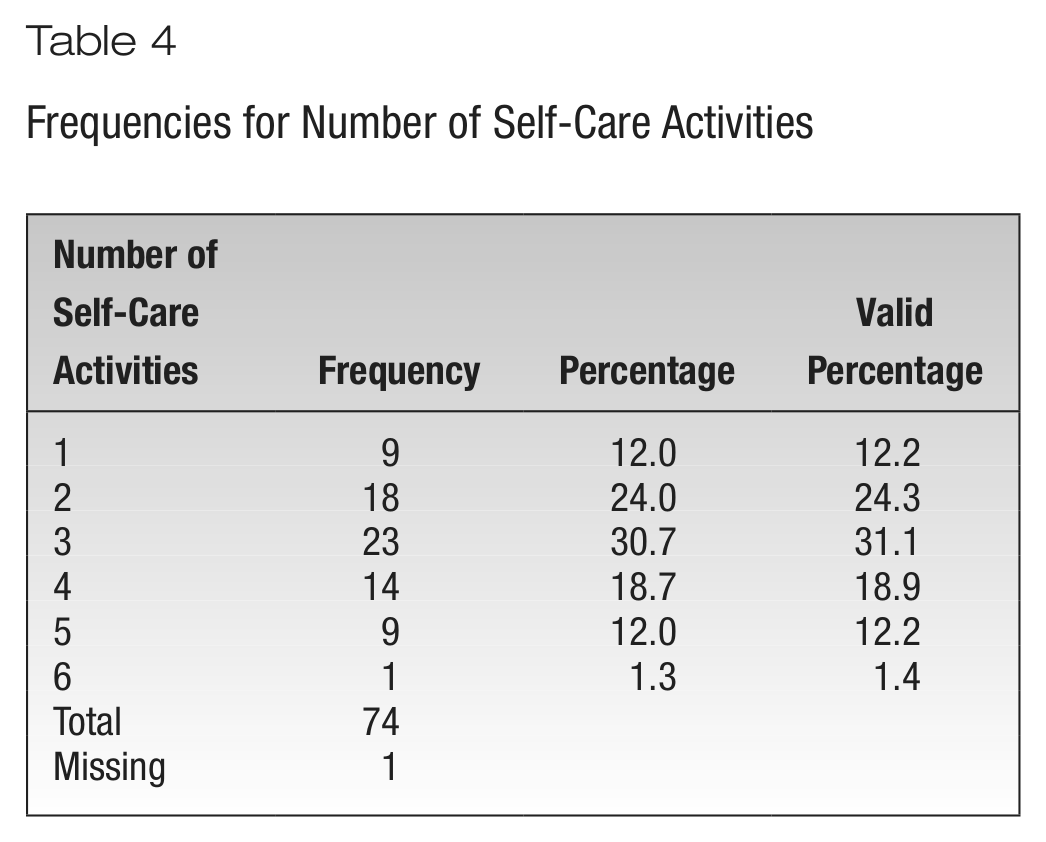
Another new variable was created to describe the number of self-care activities a participant chose to work on. The following values were assigned: 1 = 1 self-care activity, 2 = 2 self-care activities, 3 = 3 self-care activities, 4 = 4 self-care activities, 5 = 5 self-care activities, and 6 = 6 self-care activities. Table 4 lists the results of frequencies conducted for the number of self-care activities.
Frequencies for Number of Self-Care Activities
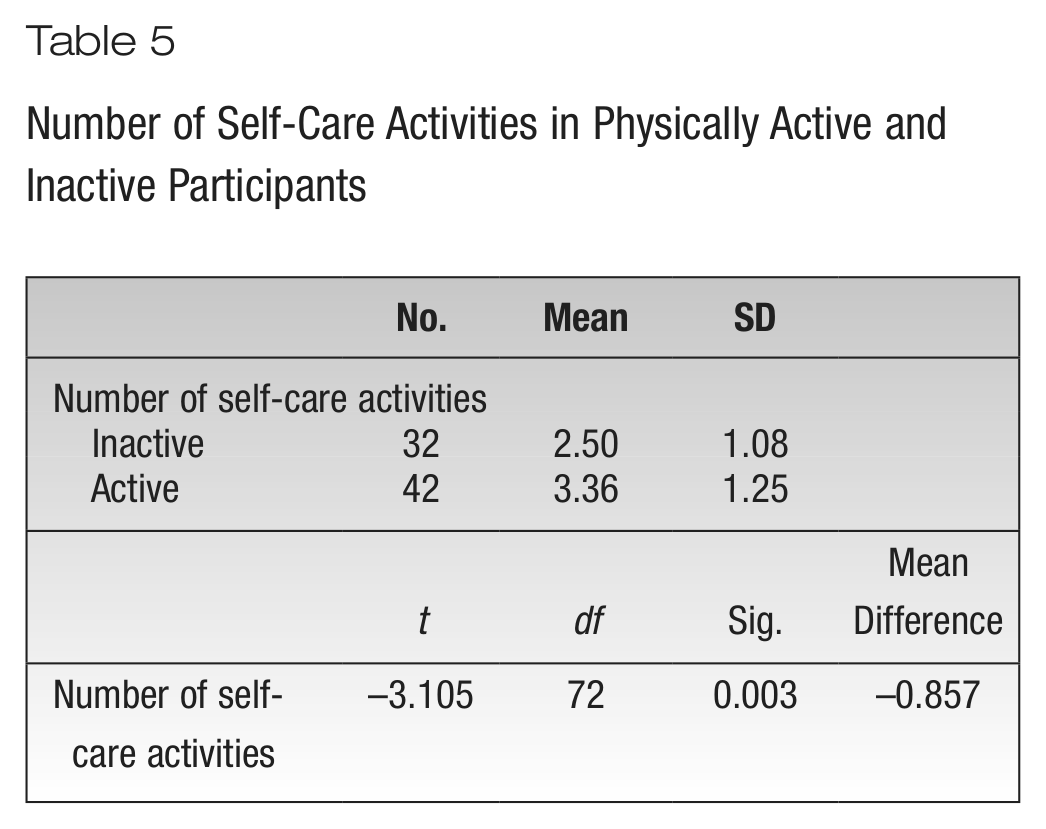
A 1-way ANOVA was conducted to determine whether participants in the later stages of change for physical activity used more self-care management strategies than those participants in earlier stages of change for physical activity. The means were not significantly different between the different stages of change (F4,69 = 2.471, P = .053). An independent samples t test was then conducted to determine whether there were differences in the mean of self-care activities between participants who were physically active and those who were inactive. There were significant differences between the 2 groups (t72 = −3.105, P = .003). The mean self-care activities of the active group was significantly higher (mean = 3.38, SD = 1.246) than the mean of the inactive group (mean = 2.50, SD = 1.078). Results of the independent samples t test are displayed in Table 5. Hypothesis 3 was supported by the data.
Number of Self-Care Activities in Physically Active and Inactive Participants
Discussion
People with diabetes need to learn a variety of behaviors to manage their disease. While physical activity is an important component of diabetes self-management used to improve control of blood glucose levels, it is often difficult for people with diabetes to start and maintain a physical activity program. The WDDMP offered by a Midwestern manufacturing company assists participants in meeting their diabetes self-management goals. In this study, participants who chose to work on physical activity as part of their diabetes self-management were more active, participated more often in general physical activity, participated more often in specific physical activity, and had a higher stage of change for physical activity than those participants who did not choose to work on physical activity.
Regarding stage of change for physical activity, 34 (45.5%) participants were in the maintenance stage and 9 (12.0%) were in the action stage, resulting in 57.3% of participants engaged in physical activity. An additional 22 (29.3%) participants were in the preparation stage and were intending to start physical activity in the next month. Given that the sample was primarily male, Caucasian, and well-educated, it was not surprising that 57.3% of the participants were engaged in physical activity. In a cross-sectional study of 23,283 adults, physical activity was higher in respondents who were male (P < .001), were white (P < .001), had higher levels of education (P < .001), and had higher income levels (P < .001). 26 In a longitudinal study to explore the patterns in physical activity behaviors of 1614 Canadians with type 2 diabetes, men participated in more leisure-time physical activity than did women (P < .01). 27
Hypothesis 1 was supported by the data. Participants who chose to work on physical activity (exercisers) as part of their diabetes self-management had a later stage of change for moderate-intensity physical activity than did those participants who did not choose to work on physical activity (nonexercisers) (P = .02). The exercisers also reported engaging in significantly more general physical activity (P = .034) and in more specific physical activity (P = .016) than did the nonexercisers over the previous 7 days. Other studies found similar results where participants in the action and maintenance stages of change reported more minutes of vigorous and moderate activity than did participants in the preparation and contemplation stages of change (P < .001) 28 ; there were large differences between stages for exercise behavior (P < .001), 29 and contemplators regularly exercised vigorously during more months (2.19 months) than did precontemplators (0.89 months). 30 Results of this study support the stage of change construct of the TTM.
Item 12 of the BSCA PAS (“I think about how participating in physical activity could change how I manage my diabetes”) had the highest mean (2.99). Physical activity can lead to hypoglycemia, especially in those participants exercising at the peak time of insulin or in those participants who take oral agents, such as sulfonylureas and meglitinides, which stimulate the pancreas to secrete insulin. Since 61.3% of the participants were receiving oral agents and an additional 12% were receiving insulin and oral agents, hypoglycemia was a realistic concern for them. Items 5 (“I feel sore and stiff”) and 6 (“I think about how much time it takes to participate in physical activity”) had the second highest mean (2.76). Item 10 (“I am discouraged from participating in physical activity by others”) had the lowest mean (1.17). It makes sense that participants in this study scored this item low since they made the decision to participate in the WDDMP. Health educators explain the effect that physical activity has in managing diabetes, offer participants guidance in choosing appropriate physical activity, and assist them in working to overcome barriers to physical activity. Items 8 (“I think about the cost of necessary equipment or fees for participating in physical activity”) and 13 (“I do not have a safe place to participate in physical activity”) had means of 1.46 and 1.24, respectively. The means of these items could reflect the participants’ employment status, in terms of whether they were working for or retired from a company that compensates employees through a competitive salary/retirement and health benefit package.
Barriers to physical activity were greater for those participants in the early stages of physical activity adoption compared with those participants in the later stages of physical activity adoption. The contemplation group had the highest mean (2.69) for barriers. Participants in this stage had been thinking about starting a physical activity program and were actively considering the benefits and barriers of engaging in physical activity. The precontemplation group had a lower mean (2.63) than the contemplation group; participants in the precontemplation group had no intention of changing their physical activity behavior in the future and therefore had not considered barriers. Those participants in the maintenance stage for physical activity had the lowest mean (1.57) score for barriers. Those people who had been exercising for 6 months or more had fewer barriers.
Although barriers to physical activity were greater for participants in the early stages of physical activity adoption compared with participants in the later stages of change, the differences were not significant. Since the groups were not equal in size, assumptions of the 1-way ANOVA were violated and type I error levels are not guaranteed. Therefore, a variable was created to identify a participant’s activity level; those who were not physically active (precontemplation, contemplation, and preparation stages) were identified as “inactive” and those who were physically active (action and maintenance stages) were identified as “active.” Those participants who were active had significantly lower mean barriers scores than those participants who were inactive (P < .001). These findings are similar to those found by others.31,32 Given that the sample was primarily male, Caucasian, well-educated, and exercising, those participants have overcome many of the barriers to physical activity. Results from this study also provide support of the TTM for physical activity.
Hypothesis 3 was supported by the data. A variety of behaviors are often implemented by people with diabetes in order to manage their disease. Those participants who were in the later stages of change for physical activity chose to focus on more self-care areas to work on to control their diabetes than did those participants who were in earlier stages of change.
Limitations
Convenience sampling, data collection via self-report, selection bias, and cross-sectional design are limitations of this study and reduce the generalizability of the findings.
Implications
Innovative strategies need to be developed and implemented in a variety of settings to meet the self-management needs of people with diabetes mellitus. A Midwest manufacturing company has developed a WDMMP in an effort to reduce the complications of diabetes mellitus and to reduce the health care costs associated with this disease. The knowledge and experience of diabetes educators would benefit other employers in the planning and implementation of a WDMMP. In this type of program, diabetes educators assist the person with diabetes mellitus to set realistic goals for diabetes mellitus self-management and offer suggestions for behavior change and coping strategies to meet individualized goals. The interactions with WDMMP participants do not need to be face to face but can be done via the telephone at a time that is agreeable with the participant.
The results of this study indicate that diabetes educators working in diabetes education/disease management programs can be particularly mindful that people who are contemplating increasing physical activity might be more successful if perceived barriers to physical activity and ways to manage them are specifically addressed.
Recommendations for Future Research
Recommendations for future research include targeting individuals who are nonexercisers (those at most risk and in the earlier stages of change for physical activity) for participation in an intervention study where data are gathered at baseline and at other times during the intervention to determine whether the intervention (the WDDMP) was effective in increasing physical activity. Measuring additional outcomes such as A1C, blood pressure, body mass index, and levels of stress to determine the effect of physical activity would also be helpful. Future studies that address these recommendations will provide diabetes health educators with more knowledge and tools to assist people with diabetes in the management of their disease.
Footnotes
Acknowledgements
No financial support was received for the study. The author thanks Jacklyn Ruthman, PhD, RN, for her assistance with statistical analysis.