
Abstract
Purpose
The purpose of this cross-sectional, descriptive study was to explore the characteristics of herbal remedy use for diabetes among Latinos/Hispanics with type 2 diabetes.
Methods
A convenience sample of 75 Latino/Hispanic adults with type 2 diabetes was recruited from community-based settings in North Carolina. Data were collected through face-to-face bilingual interviews. Measures included a demographic questionnaire; the Traditional, Complementary, and Alternative Practices Questionnaire; and biophysical indicators of A1C and body mass index.
Results
Sixty-nine percent of the sample reported using herbal remedies for diabetes self-care. Forty-nine herbal products were identified. The most commonly reported products were prickly pear cactus, aloe vera, celery, and chayote. The perceived effectiveness of products varied; some said they helped “a lot” while others noted the development of side effects. Over three quarters (77%) of persons using herbal remedies reported concurrent use with prescribed medications. Also, some participants reported skipping or altering the dose of diabetes medications when using herbal remedies. Most (77%) reported not disclosing herbal remedy use to health care providers.
Conclusions
Diabetes educators and other health care providers need to ask Latino/Hispanic clients about their use of herbal remedies and become knowledgeable about herbal products to provide advice about safety.
The use of herbal remedies by Latinos/Hispanics for diabetes self-care has been identified in several studies.1-6 In fact, Latinos/Hispanics have been reported to consume more herbs than other ethnic groups1,7 and to use herbal products that are unfamiliar to most American health care providers.1,8,9 Herbal remedies are considered to be botanical, natural products that are nonvitamin or nonmineral in content and may consist of a single herb/plant or a mixture of multiple herbs/plants. 10 Latinos/Hispanics report using herbal remedies because they are “natural,” culturally congruent, familiar, accessible, and affordable.4,7,11,12 Some qualitative studies suggest that many Latinos/Hispanics believe that herbal remedies are an effective diabetes treatment and can even cure diabetes.4,5 At the same time, a lack of awareness of possible synergistic or negative interactions between herbs, between herbs and medications, or between herbs and underlying health conditions has been documented among Latinos/Hispanics.13-15 This lack of knowledge places individuals at risk for herb-herb interactions, drug-herb interactions, overmedication, exposure to contaminants, allergic reactions, toxicities, and exacerbation of underlying health conditions.16-18
Literature on the use of herbal remedies by Latinos/Hispanics indicates that they consume many different types of herbs/plants for health concerns and these natural products are ingested in multiple forms, including tablets, capsules, teas, licuados (smoothie-like mixture of natural products), aguas frescas (cold drinks usually made with one herb), and herbs/plants eaten raw or cooked as food.2,4 The use of several culturally based, premixed commercial teas for the treatment of diabetes has been reported by Latinos/Hispanics, including Te Diabetil, Diabe Cure, Diabetina, Te Malabar, and Starbien.8,11,15 Little is known, however, about the dose or frequency of herbal remedies or whether Latinos/Hispanics alter the dose of prescribed diabetes medications to accommodate herbal treatments. Poss et al 4 found that Mexican Americans with type 2 diabetes relied on their own judgment to titrate doses of herbs as part of their diabetes self-care, even when they did not understand the pharmacokinetics and pharmacodynamics of the herbs they ingested
There is little knowledge of the diabetes-related symptoms Latinos/Hispanics treat with herbs or the perceived effectiveness of these traditional modalities. Data on the development of adverse events due to herb ingestion by Latinos/Hispanics are also lacking. Further, prior research suggests that Latinos/Hispanics do not disclose the use of these traditional modalities to their health care providers, nor do health care providers routinely ask about or monitor the use of herbal remedies.2,8,12 Many authors have raised concerns that health care professionals do not have sufficient knowledge to provide advice about safe use of herbal remedies.8,9,19
Given the high prevalence of type 2 diabetes among Latinos/Hispanics 20 and their high rates of diabetes-related complications 21 and hospitalization for uncontrolled diabetes, 22 research is clearly needed to obtain a better understanding of how Latinos/Hispanics use herbal remedies for the management of type 2 diabetes. Therefore, the purpose of this cross-sectional, descriptive study was to explore the use of herbal remedies for diabetes self-care among a sample of Latinos/Hispanics with type 2 diabetes living in the southeastern United States. Specifically, the study assessed: (1) the characteristics of herbal remedy use for diabetes self-care, (2) the perceived effectiveness of herbal remedies and the development of side effects, and (3) Latinos/Hispanics’ attitudes toward herbal remedies for diabetes self-care.
Methods
Design, Sample, and Setting
The data reported here were collected as part of a larger study of self-care practices of Latinos/Hispanics for the management of type 2 diabetes. Convenience sampling was used to recruit Latino/Hispanic men and women (N = 75) in rural and urban areas of central and western North Carolina. Inclusion criteria were (1) self-identification as either Latino or Hispanic, (2) self-reported history of type 2 diabetes for at least 12 months, (3) age 18 years or older, and (4) ability to speak either Spanish or English. Participants were recruited by the first author, who speaks Spanish as a second language, and by two trained, native Spanish speaking, bicultural and bilingual lay research assistants.
Participants were recruited from community clinics, Latino/Hispanic churches of various denominations, an English as a second language class, a migrant farmworker neighborhood, Latino/Hispanic markets, and a Latino/Hispanic health fair. The community clinics provided health care to uninsured, low-income individuals and use a sliding scale for payment. These settings were chosen as recruitment sites because the majority of Latinos/Hispanics in North Carolina (61.1%) lack health insurance 23 and more than 25% of Latinos/Hispanics in the state live in poverty. 24 Multiple methods of recruitment were used, including posting culturally and linguistically appropriate flyers in these community-based settings, making bilingual announcements in churches, and speaking with Latino/Hispanic adults in community clinic waiting rooms and at cultural community events. The study was approved by appropriate administrators in the community-based settings and the Institutional Review Board of the University.
Study Measures
A 32-item author-developed demographic questionnaire was used to capture information on age, gender, medical history pertaining to type 2 diabetes, Latino/Hispanic subgroup status, nativity, length of residence in the United States, spoken language, education, income, marital status, and health insurance. Response options included multiple choice sets or short answers.
Participants also completed the Traditional, Complementary, and Alternative Practices Questionnaire developed by the first author. This 31-item measure assesses the use of herbal remedies, faith-based interventions, traditional healers, and self-medication/self-prescription for diabetes self-care. The measure was developed based on the scientific literature, clinical knowledge, and the 2007 National Health Interview Survey Adult Alternative Health/Complementary and Alternative Medicine Questionnaire. 25 This questionnaire includes both open-ended and multiple choice questions inquiring about herbal remedy practices for diabetes self-care, use of prescribed diabetes medications when consuming herbal remedies, and disclosure of herbal remedy use to health care providers. To assess Latinos/Hispanics’ attitudes toward herbal remedies for diabetes, respondents were asked whether they trust herbs/plants, prescription diabetes medications, or a combination of the 2 most for the treatment of diabetes and which type they believe is safer to use. The demographic questionnaire and the Traditional, Complementary, and Alternative Practices Questionnaire were translated into Spanish and back translated into English by two bicultural native Spanish speakers and the back translations were then compared to the original English versions to ensure semantic accuracy. All study documents and measures were available in both Spanish and English.
Height was measured without shoes in centimeters with a portable stadiometer, and weight was measured in kilograms using a Tanita BWB-800A Class III Digital Professional Body Weight Scale. Body mass index (BMI) was calculated using the standard formula of weight in kilograms divided by height in meters squared. 26 Weight was then characterized based on the standard BMI categories of normal weight (BMI = 18.5-24.9 kg/m2), overweight (25-29.9 kg/m2), and obese (≥30 kg/m2). 26 The Bayer A1CNow+ point of care machine was used to determine A1C level from a finger stick blood sample. The accuracy of the Bayer A1CNow+ point of care machine is reported to be comparable to that of clinical diagnostic laboratories, and it has received National Glycohemoglobin Standardization Program certification.27,28 The maximum A1C result with the Bayer A1CNow+ point of care machine is 13.0%. In this study, all A1C results greater than 13.0% were truncated in the statistical database as 13.10%.
Data Collection and Analysis
All data were collected in face-to-face interviews with the first author or a lay research assistant. The interviews were conducted in Spanish or English in a private area of a community-based site or in the participant’s home, based upon the preferences of participants. Since many Latino/Hispanic immigrants in North Carolina have reported low educational levels, consent forms and all measures were read to participants to increase data validity and to prevent embarrassment about low literacy. 29 A list of hypoglycemic agents and insulin names was available for participants to review to promote accuracy of medication recall. All interviews were completed within 1 hour. At the end of the interview, participants were given a copy of their biophysical indicator results, diabetes educational materials in either Spanish or English from the National Diabetes Education Program,30,31 and a $20 gift card to a local store in appreciation of their time. Data were entered into SPSS version 18.0 (SPSS Inc, an IBM Company, Chicago, Illinois). Descriptive statistics were used to describe categorical variables. Responses to open-ended questions were evaluated using basic content analysis and counts. 32
Results
Characteristics of Participants
Of the 75 participants recruited for the study, most (66.7%) were female and the mean age was 47 years (SD = 11.34). The majority (69.3%) were married or lived with a committed partner and identified as Catholic (64%) or other Christian (28%). All participants were immigrants; the great majority was born in Mexico (85.3%), while others originated from various Central American or Caribbean countries. They had lived on average nearly 16 years (SD = 7.22) in the United States and 12 years (SD = 4.35) in North Carolina. Spanish (72%) was the predominant language spoken at home; however, some participants reported speaking a mixture of English and Spanish (21.3%; n = 16), while others reported speaking a mixture of Mixtec or Tarasco at home and Spanish (6.7%; n = 5). Most (64%) persons rated their ability to speak English as “very poor,” and 1 out of 3 persons rated their ability to write in Spanish as “poor” or “very poor.” Most of the participants were uninsured (86.7%) and 48% reported a family household annual income less than $20,000. The mean number of years of education of participants was 6.08 (SD = 3.82).
Fifty-two percent (n = 39) of the sample had been diagnosed with type 2 diabetes between ages 18 and 39 years, and nearly 23% (n = 17) had been diagnosed between ages 40 and 50 years. The average number of years participants reported having diabetes was 7.59 (SD = 5.40). A majority of participants (68%) reported taking oral hypoglycemic agents for diabetes, and 26.7% reported taking insulin. One-fifth of the sample described taking a combination of oral hypoglycemic agents and insulin. Other prescribed medications taken by participants included statins (52%), angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers (40%), other antihypertensive medications (22.7%), aspirin (17.3%), omega-3 fish oil (8%), antidepressants (5.3%), and fibrates (4%).
Nearly 70% of participants (n = 51) had A1C results greater than 7% (see Table 1). An overwhelming majority (90%) of the sample were classified as either overweight or obese by calculated BMI.
Biophysical Indicators (N = 75)
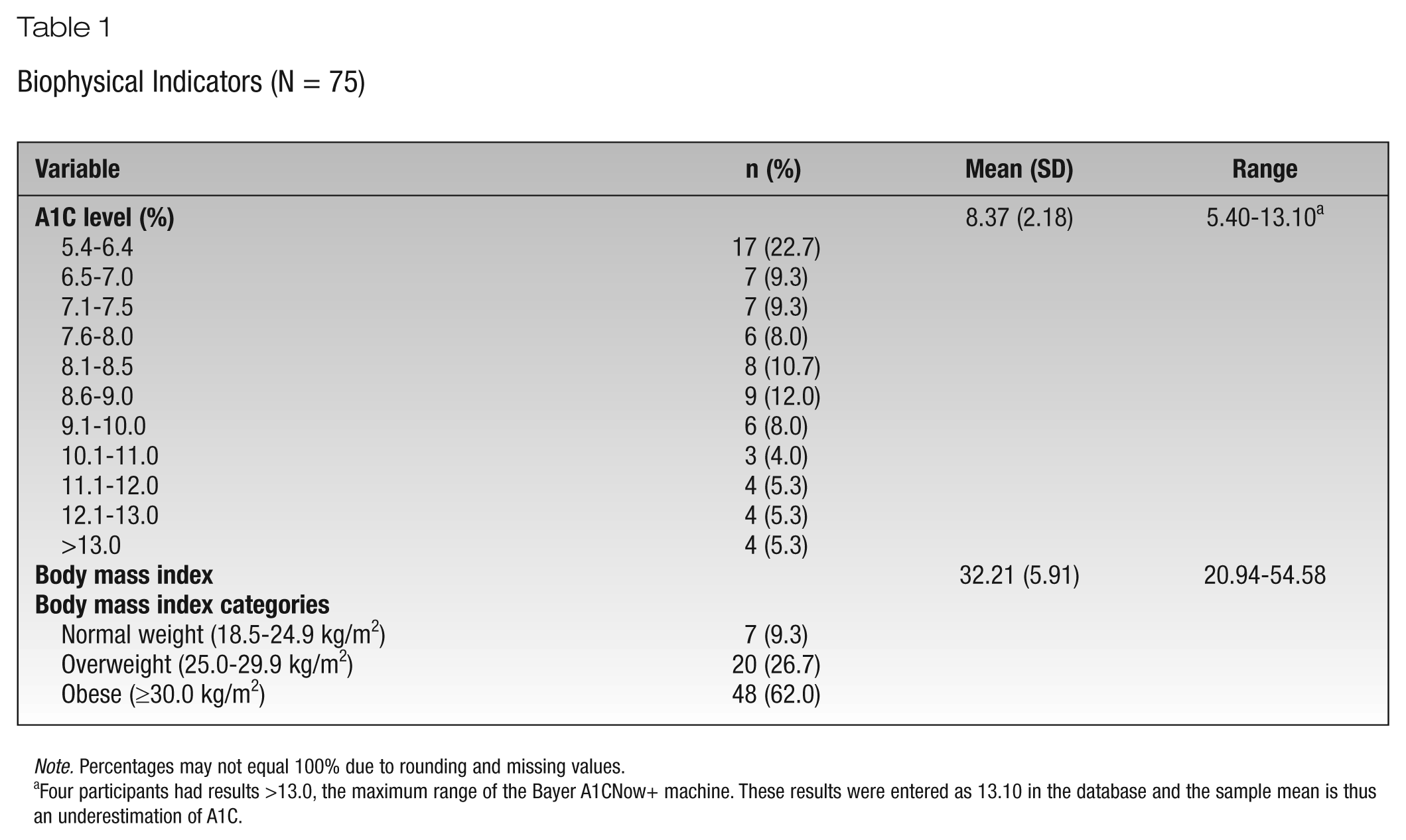
Note. Percentages may not equal 100% due to rounding and missing values.
Four participants had results >13.0, the maximum range of the Bayer A1CNow+ machine. These results were entered as 13.10 in the database and the sample mean is thus an underestimation of A1C.
Use of Herbal Remedies
Fifty-two participants (69.3%) reported currently using herbal remedies for the management of diabetes (see Table 2). Respondents identified 49 herbal remedies and described using from 1 to 9 different remedies simultaneously. These herbal remedies consisted of a variety of vegetable food products, herbs, teas, and commercially packaged products, some not available in the United States. Prickly pear cactus leaves (nopale), aloe vera (salvia or sábila), celery (apio), vegetable pear (chayote), cinnamon (canela), cat’s claw (uña de gato), Herbalife, beets (betabel or la remolacha), bitter gourd/melon (cundeamor or yerba mora), Nin (English translation and ingredients unknown; participants stated that it was a blend of Mexican herbs), horsetail (la cola de caballo), oats (aveno), chamomile tea (té manzanilla), and lemon (limón) were the most frequently reported natural products used.
Alphabetical List of Herbal Remedies and Characteristics of Use

§, information is missing; ?, exact English translation not available; PRN, 2 to 4 times per year as needed.
Sweetener from a plant source.
Various methods of herbal remedy preparation were described by participants. A licuado was the most common preparation reported. Participants described making licuados with 20 different herbal products and mixing the herb/plant with juice, milk, fruit, or other vegetables. A tea was the second most common preparation, used in 19 herbal remedies. Participants also described cooking herbal remedies as food (n = 13), or consuming them fresh (n = 3), or mixing them into an agua fresca (n = 4). Four herbal products were consumed in a pill or capsule formula, and 2 were purchased as a premixed beverage. Arnica was reportedly used as a topical agent for diabetic ulcers or cuts.
Participants described using individualized dosing and frequency schedules, with no standardization for specific herbs/plants. The majority of herbal remedies (n = 33) were used daily, including prickly pear cactus (nopale), aloe vera (salvia or sábila), celery (apio), vegetable pear (chayote), cinnamon (canela), Herbalife, horsetail (la cola de caballo), coconoxtle cactus, and canary seeds (alpiste). Other herbal remedies (n = 20), including bitter gourd/melon (cundeamor or yerba mora), brickellia grandiflora (la prodigiosa), chamomile tea (té manzanilla), lemon/lemon root (limón and raíz de limón), and Blood Sugar Formula, were consumed weekly. A set of 6 herbal remedies were consumed monthly, and 8 products only on an as needed basis of 2 to 4 times per year.
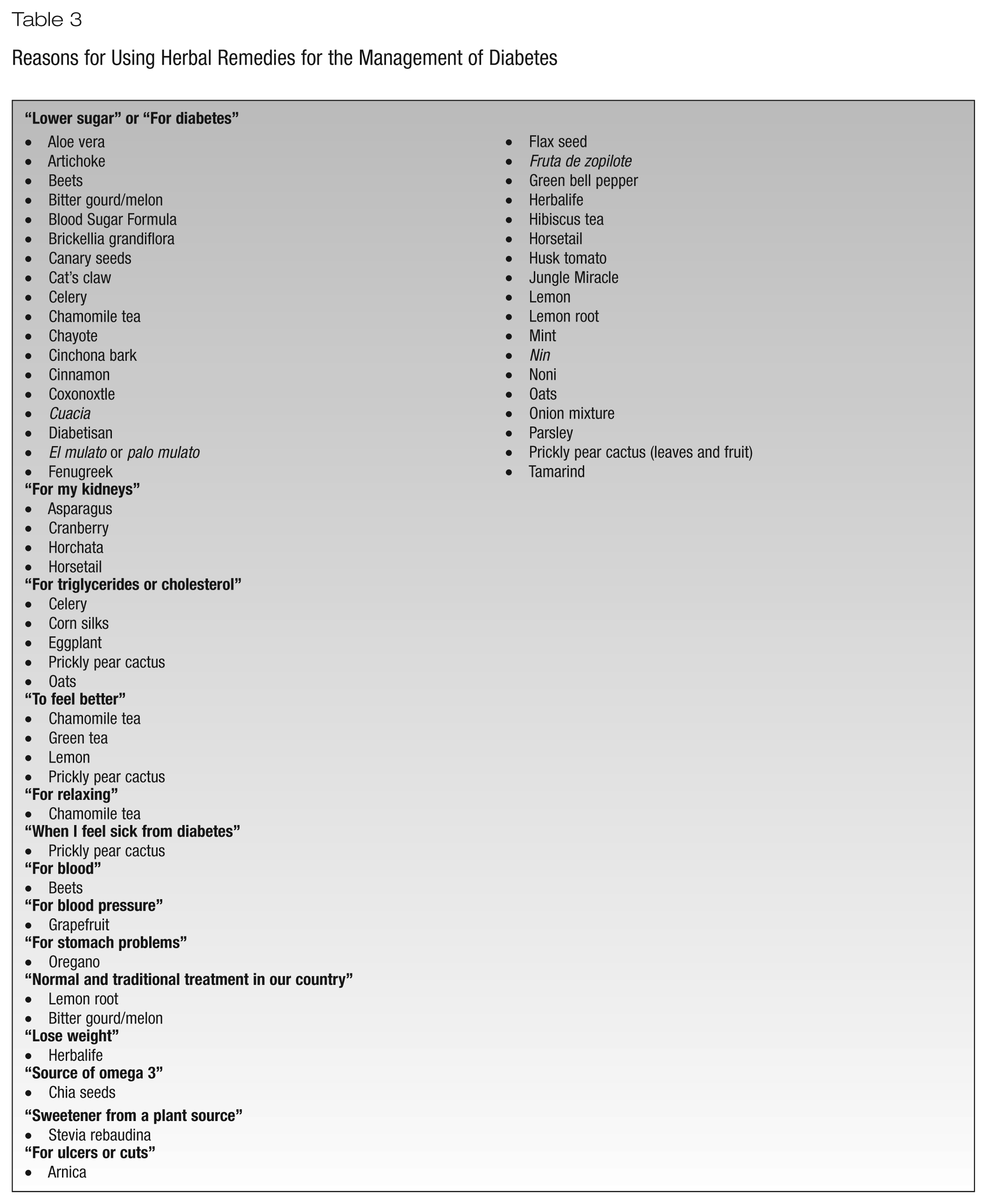
Participants described a variety of reasons for using herbal remedies for the management of diabetes (see Table 3). The most common reasons reported by the majority of participants for most herbal remedies were “lower sugar,” “for diabetes,” “for triglycerides or cholesterol,” “to feel better,” and “for my kidneys.” Less commonly reported reasons for using herbal treatments for diabetes included “normal and traditional treatment in our country,” “for blood pressure,” “for relaxing,” “when I feel sick from diabetes,” and “for ulcers or cuts.” Despite efforts of the first author and research assistants to probe for more specific reasons, such as specific diabetes-related signs and symptoms or effects on daily life, participants only described the purpose of herbal remedies in a general manner. No respondent reported using herbal remedies due to the cost of prescribed diabetes medications or lack of health insurance.
Reasons for Using Herbal Remedies for the Management of Diabetes
Herbal remedies were obtained in a variety of ways. Most were purchased either from a local Latino/Hispanic market (tienda; n = 23) or local grocery store (n = 19). Sixteen of the participants who reported using herbal remedies described acquiring them (n = 13) from their home country. Other sources included health food stores, personal gardens, purchases over the Internet or from a consultant, and a friend living in another state who sent the product in the mail.
The question “How much does this product help you?” was asked to assess the self-perceived effectiveness of herbal remedies for diabetes. Thirty herbal remedies were rated by 52 participants as helping “a lot,” and 21 products were noted as helping “a little” by 45 participants. Fourteen herbal remedies were rated by 19 people as “no change/did not help” and 2 persons reported feeling “worse,” one after using prickly pear cactus and another with cat’s claw. Participants did not describe specifically how these natural products helped their diabetes, even with probing questions about which symptoms improved. The herbs/plants most frequently rated as helping “a lot” were prickly pear cactus (nopale), aloe vera (salvia or sábila), celery (apio), vegetable pear (chayote), cinnamon (canela), and beets (betabel or la remolacha). Herbs/plants rated as “no change/did not help” included eggplant (berenjena), prickly pear cactus (nopale), Herbalife, aloe vera (salvia or sábila), and canary seeds (alpiste).
Respondents also described experiencing side effects from using herbal remedies. Bitterness (n = 6) was the most common side effect associated with the use of lemon, husk tomatoes, bitter gourd/melon, and cuacia. Other side effects included diarrhea (n = 2) from using canary seeds and Herbalife, muscle cramps from Noni (n = 1), blood glucose meter verified hypoglycemia from chia seeds (n = 1), stomach ache from Blood Sugar Formula (n = 1), and back/kidney pain from Herbalife (n = 1).
Two questions assessed the attitudes of all participants regarding the use of herbal remedies for the treatment of diabetes: “Which do you trust more for the treatment of diabetes?” and “Which do you think is safer to use?” Forty-five percent of the sample (34/75) reported trusting more a combination of herbal remedies and prescription diabetes medications for the treatment of diabetes, while 38.7% (29/75) trusted prescription diabetes medications alone and 5.3% (4/75) herbal remedies alone. The majority (52%; 39/75) of the sample considered prescription diabetes medications safer than a combination of herbal remedies and prescription diabetes medications (29.3%; 22/75) or herbal remedies alone (11%; 8/75).
Participants who reported taking herbal remedies for diabetes were asked about alterations in the dose of their prescribed diabetes medications on the days when they used herbal remedies. Forty participants out of 52 reported taking their prescribed diabetes medications as directed on the days they consumed herbal remedies; however, 7 participants reported skipping the dose of prescribed diabetes medications and 4 others reported decreasing the dose of medications on days when they consumed herbal remedies (see Table 4). Further, 77% of participants using herbal remedies (40/52) said they had not disclosed the use of these remedies to their health care providers.
Alterations in Dosing of Prescribed Diabetes Medications When Using Herbal Remedies
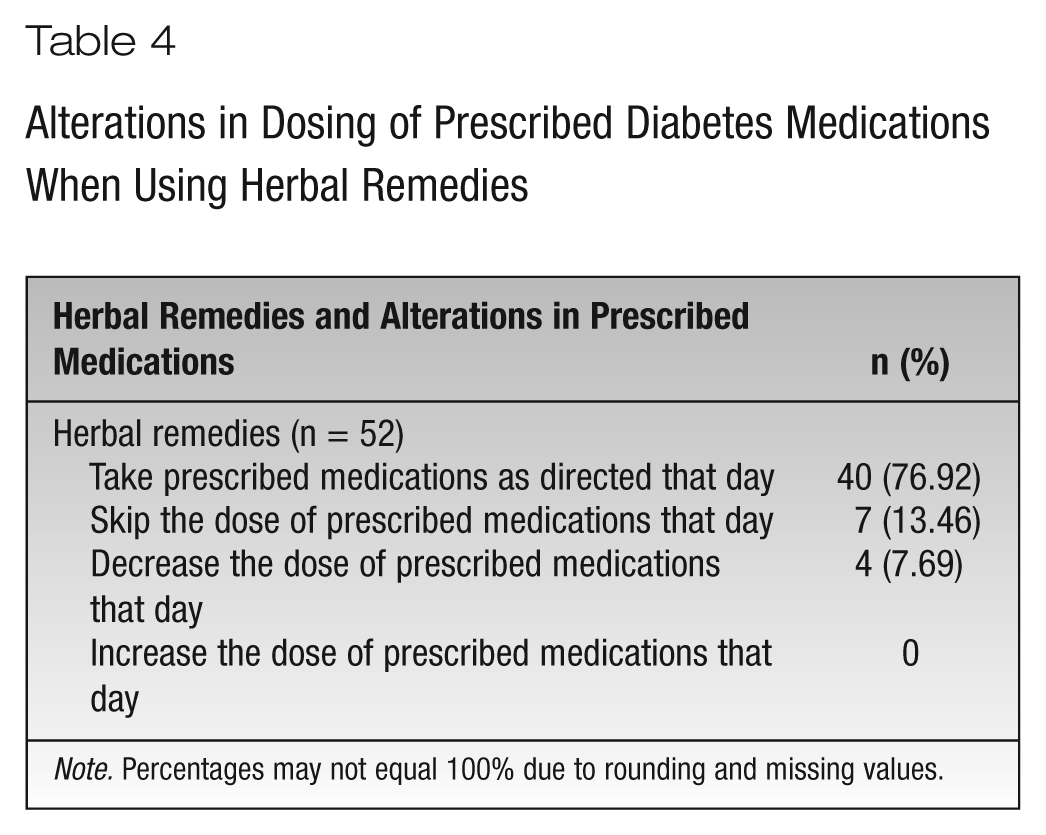
Note. Percentages may not equal 100% due to rounding and missing values.
Discussion
This study explored the characteristics of herbal remedy use for diabetes self-care among Latinos/Hispanics. Those who chose to participate in the study were similar to Latino/Hispanic participants in other studies of diabetes and the use of alternative therapies.2-5,8,15 That is, they were primarily from Mexico, female, similar in mean age, and with limited English proficiency and low rates of health insurance and financial resources. A significant proportion of the participants had an A1C result greater than 7% and was overweight or obese. Despite having lived on average 16 years in the United States and 12 years in North Carolina, this sample of Latino/Hispanic immigrants used numerous culturally based herbal remedies for diabetes self-care. The participants described obtaining these products primarily from settings in their Latino/Hispanic communities in North Carolina. Some of the herbal remedies described, such as prickly pear cactus (nopale), aloe vera (salvia or sábila), and bitter gourd/melon (cundeamor or yerba mora), have been reported in prior studies conducted with Latinos/Hispanics living in Mexico, Texas, and other southwestern areas of the United States.2,4,33 However, respondents described using a variety of herbs/plants not previously reported. These natural remedies included arnica, asparagus, Blood Sugar Formula, canary seeds, celery, chia seeds, cinchona bark, coconoxtle cactus, cranberry, cuacia, eggplant, El Milagro de la Selva, flax seeds, fruta de zopilote, green bell peppers, hibiscus tea, horchata, husk tomatoes, lemon root tea, nin, stevia rebaudina, and tamarind. In fact, the direct English translations and herbal compositions of several of these remedies are unknown.
Consistent with the findings of Poss et al 4 and Johnson et al, 2 this sample of Latinos/Hispanics described consuming herbal remedies in various preparations, including licuados, teas, aguas frescsa, fresh or cooked food, and pills/capsules. Several of these herbal remedies, such as nopales (leaves and fruit), chayote, and celery are also commonly eaten as a vegetable or side dish. However, participants clearly described using these natural products as a diabetes treatment and not as part of their diet. Participants reported using anywhere from 1 to 9 herbal products simultaneously on a daily, weekly, monthly, or as needed basis. The frequency of herbal remedy use has not been previously reported. The individualized dosing schedules indicate a lack of standardization of products, which is similar to findings reported by Poss et al. 4
Understanding how Latinos/Hispanics consume, prepare, and mix herbal remedies, along with the quantity used, is important since this consumption may affect the bioavailability and effects of phytochemicals found in these herbs/plants. For example, recent research with prickly pear cactus, a widely used natural product for diabetes among persons of Mexican origin, has revealed that the hypoglycemic effects of this plant may be different when consumed raw or broiled.17,34 Further, current investigations of the mechanism of action of saponins, the bioactive phytochemicals found in bitter gourd/melon, indicate that the hypoglycemic effects may be influenced by the concentrations of saponin compounds and their ability to stimulate insulin secretion. 35
The reasons participants gave for using herbal remedies for diabetes self-care were only general in nature. Even with probing questions, respondents did not describe using herbal remedies for specific hyperglycemic or hypoglycemic signs or symptoms. Possibly, this vagueness indicates a lack of personal recognition of diabetes-related signs and symptoms or that Latinos/Hispanics may not attribute certain symptoms to diabetes or consider them to be important. Additionally, this may indicate that Latinos/Hispanics conceptualize diabetes differently than American health care providers and perceive diabetes-related signs and symptoms from a non-Western, nonmedical paradigm. For example, Garcia, 36 in a sample of Mexican Americans in Texas, found that participants perceived only fatigue and blurred vision as important symptoms of diabetes and ignored all other symptoms. In another study, Lopez 11 found that Mexican Americans perceived their diabetes to be controlled as long as they were able to maintain their daily roles, not the medically recognized diabetes-related signs and symptoms. A better understanding of how Latinos/Hispanics conceptualize and self-treat diabetes is needed as this information may affect how diabetes educators and other health care providers present diabetes self-management information to clients as well as treatment options.
The perceived effectiveness of herbal remedies for diabetes and the development of side effects among Latinos/Hispanics was explored in this study. Participants perceived most herbal remedies as either helping their diabetes “a lot” or “a little.” However, it is not clear on what basis or change in personal condition that participants rated the self-perceived effectiveness of each product. Several persons described experiencing adverse reactions or side effects from herbal products, but it is unclear what participants meant by “back/kidney pain,” or the development of “muscle cramps” and “stomach ache,” or feeling “worse” with herbal remedies. Only 1 participant reported assessing her symptoms with a blood glucose meter to verify that she was experiencing hypoglycemia after the consumption of chia seeds. This participant explained that she decreased the “dose” of chia seeds based upon her blood glucose meter readings. Her experience of hypoglycemia with chia seeds is similar to the case study of a Mexican man who developed a hypoglycemic reaction to the combination of prickly pear cactus (nopale), glipizide, and metformin. 34 However, it is not clear if the side effects or adverse reactions in this current sample were related to herb-herb or herb-drug interactions or the effects of herbs on underlying health conditions of participants.
Latinos/Hispanics’ attitudes toward herbal remedies for diabetes in relation to prescribed diabetes medications were assessed. More participants reported trusting the combination of herbal remedies and prescribed diabetes medications than those who reported trusting prescribed diabetes medications alone. Only a few participants reported trusting herbal remedies alone for diabetes self-care. The high levels of trust in combination therapy reported among this sample may explain the high level of herbal remedy use. Additionally, this “trust” may explain why most participants reported taking prescribed diabetes medications on the days when they used herbal remedies. Over 50% of participants rated prescription diabetes medications alone as safer than other remedies, but nearly a third of the sample rated the combination of herbal remedies and prescribed diabetes medications as safer. It is unclear whether participants’ trust or perceptions of safety affect their decision to continue, skip, or decrease the dose of diabetes prescribed medications on the days when they consumed herbal remedies.
The majority of participants who used herbal remedies reported not telling their health care provider about this diabetes self-care modality. The lack of disclosure of herbal remedy use found among this sample is similar to that found among a sample of Hispanic and American Indian participants in a study in the southwestern United States. 12 Being unaware of herbal remedy use may contribute to misdiagnosing client symptoms and the development of herb-herb interaction, herb-drug interactions, and toxicities.
Several limitations of this study need to be considered when interpreting the results. This was a small convenience sample recruited in central and western North Carolina. Further, selection bias may have existed since the persons who consented to participate may have been more interested in discussing herbal remedies than those who declined to participate. Validity and reliability testing of the author-developed Traditional, Complementary, and Alternative Practices Questionnaire is currently lacking. Finally, since this was a cross-sectional study, causality cannot be established.
Implications
Despite its limitations, this study has important implications for health care provider education, clinical practice, and research. Diabetes educators and other health care providers must be knowledgeable about the herbal remedies used by Latinos/Hispanics for the management of type 2 diabetes. This will require education in the area of complementary and alternative modalities as well as increased cultural competence and communication skills. The National Institutes of Health National Center for Complementary and Alternative Medicine (http://nccam.nih.gov/) is an excellent resource of reliable information for health professionals. Client-provider dynamics that promote mutual respect and discussion and disclosure of culturally based herbal remedies have the potential to positively affect the health of Latinos/Hispanics with type 2 diabetes. 37
Increased knowledge of the potential for herb-herb and herb-drug interactions and toxicities may assist health care providers to inquire about the use of herbal remedies, better evaluate client complaints and symptoms, and prescribe safe treatments that are both culturally and medically based. With knowledge of the mechanism of actions of phytochemicals and cultural competence, health care providers can negotiate the cessation of unsafe herbal practices and support practices that promote health and prevent illness. Additionally, this information can be used to tailor diabetes education programs for this population.
Further research is needed to strengthen our knowledge of herbal remedies used for diabetes management among Latinos/Hispanics. Studies are needed to identify the chemical structures of herbal remedies, the pharmacokinetics and pharmacodynamics of phytochemicals, dosing, efficacy, and toxicity characteristics. Investigations exploring how Latinos/Hispanics prepare, dose, and ingest herbal remedies may provide a foundation for diabetes educational programs and clinical practice. Additionally, health care providers should not assume that Latinos/Hispanics experience living with diabetes according to medically defined signs and symptoms. Consideration should be given that this population may conceptualize their experience of diabetes from a non-Western, nonmedical paradigm and may present and talk about their condition differently. Qualitative research exploring why Latinos/Hispanics use specific herbal remedies for diabetes and what symptoms or events they are intended to affect may provide insight to improve outcomes for this growing population.
Footnotes
This study was partially funded by the Ruth P. Council Research Grant Award from Sigma Theta Tau International Honor Society of Nursing, Gamma Zeta Chapter. The content is solely the responsibility of the authors and does not necessarily represent the official views of Sigma Theta Tau International Honor Society of Nursing. The authors extend special thanks to the following individuals for their support: Zulema Silva, BA, and Grisel Trejo, MPH, BS.