
Abstract
Purpose
The purpose of this study is to assess the extant literature on instruments used to measure self-efficacy in youth with type 1 diabetes (T1DM) and their caregivers and to critically evaluate these measurements.
Methods
An integrative review (2003-2013) was conducted searching PsycINFO, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and US National Library of Medicine PubMed service (PubMed) databases using key words diabetes, type 1 diabetes, and self-efficacy. The authors reviewed the resulting 294 references for inclusion criteria of (a) sample of youth with T1DM or sample of caregivers of youth with T1DM, (b) description of the self-efficacy instrument as primary research, and (c) the instrument measured self-efficacy specifically related to diabetes management. Forty-five articles out of the initial 294 met criteria.
Results
Of the 45 articles, 10 different self-efficacy instruments were identified. The primary theoretical framework used was Bandura’s social cognitive theory and model of self-efficacy. Most participants were white middle-class T1DM youth. Evaluations to assess validity often were not reported; however, a majority of studies reported high internal consistency of the instruments.
Conclusions
Sample homogeneity could limit the applicability of results to certain patient populations. Further psychometric analysis, including validity assessments, should be conducted in more diverse samples. Development of valid and reliable instruments for measuring self-efficacy that are sensitive to change across a wider caregiver base over time is necessary. While this review examined reliable and valid instruments used in research, future opportunities include evaluation of measuring self-efficacy in T1DM youth exposed to recent advances in diabetes management technologies.
Adhering to rigorous type 1 diabetes (T1DM) management during the complex stages of normal growth and development in childhood and adolescence is a significant challenge that impacts both youth with diabetes and their parents/guardians. Improved intensive therapy options can add to these challenges, as currently available therapeutic advances require self-management. Despite these improvements and a well-established correlation between adequate glucose control and reduced risk of complications, youth with T1DM often fail to meet the suggested A1C targets necessary to mitigate associated risks.1-4 Enhanced diabetes self-efficacy has been linked to improved diabetes self-care and glycemic control and is an important indicator of health behavior changes in youth.5,6 Self-efficacy, or one’s perceived ability to follow a diabetes treatment program, is important to foster in T1DM youth and their caregivers given the demands of diabetes self-management. 7 Therefore, it is important for diabetes educators to understand the concept of self-efficacy and what measures are available to assess self-efficacy in youth with T1DM. The purpose of this integrative review was to identify measurement instruments to assess self-efficacy in youth with T1DM and to evaluate the reported psychometric properties of those instruments.
Theoretical and operational definitions allow for greater understanding and means to measure self-efficacy. 8 A theoretical definition of self-efficacy includes the belief that an individual has the ability to create change by personal actions. 9 In T1DM, operational definitions are informed by data from self-report surveys that assess one’s level of confidence or self-efficacy to accomplish diabetes management tasks, such as blood glucose monitoring, insulin administration, and attention to diet and exercise, in everyday living and in difficult situations that may occur. Self-efficacy is important to capture in youth with T1DM because higher levels of diabetes-specific self-efficacy may result in increased resilience when youth face barriers or challenges associated with diabetes self-management. 6 Therefore, ongoing work to measure and optimize self-efficacy in youth with T1DM is necessary to equip youth to manage this disease long term. This can be particularly important during transition periods across the life span of childhood as diabetes management gradually transitions from parents to older children and adolescents and then becomes the sole responsibility of college-aged youth or young adults living on their own.
Methods
The literature search focused on (1) identifying instruments used to measure the construct of self-efficacy in youth with T1DM and their parents and (2) evaluating the reported psychometric properties of those instruments. For an appropriate literature search, at least 2 different search strategies are necessary according to Whittemore and Knafl’s integrative review methodology. 10 This literature search used PsycINFO, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and US National Library of Medicine PubMed service (PubMed) to obtain applicable articles. Search engines from nursing, psychology, allied health, and medical literature provided the opportunity to assess the measurement of self-efficacy across disciplines. Because of the unique attributes of T1DM disease management in this particular population, the search focused on studies of youth with T1DM. Additionally, the search included articles across all pediatric age groups and their caregivers involved in the care and management of T1DM. International literature that was translated into English was retained because evaluating the concept across geographies could add a valuable cultural perspective. This search included articles measuring specific areas of self-efficacy within diabetes management (healthy eating, being active, monitoring, taking medication, problem solving, reducing risks, and healthy coping, which are the 7 self-care behaviors guiding diabetes education). 11 To obtain a contemporary perspective on available instruments, only primary research published between 2003 and 2013 was included.
Figure 1 presents an overview of the literature search and is a CONSORT flow diagram of the search methodology. 12 The first database search occurred with PsycINFO. An initial search included the terms diabetes and self-efficacy, and an additional search included the terms type 1 diabetes and self-efficacy. The investigators conducted searches with both diabetes and type 1 diabetes to ensure comprehensiveness. Limits of English, last 10 years of publication, and childhood age (birth-17 years) were applied. The age limit for the PsycINFO search ended at 17 instead of 18 years because 18 years and older is classified as adulthood in this search engine. The results were evaluated for applicability, availability, and relevance; a total of 28 articles met inclusion criteria. The second database search occurred with CINAHL and included combined searches with diabetes and self-efficacy as well as type 1 diabetes and self-efficacy. After applying the limits of English, last 10 years of publication, and ages birth-18 years, this search identified 16 articles that met inclusion criteria and were not duplicates from the prior search. A third search occurred in PubMed and included the MeSH terms diabetes mellitus and self-efficacy and then type 1 diabetes and self-efficacy. To add precision to the search, the authors specified the MeSH term self-efficacy as a major term. Adding the limits of English, last 10 years of publication, and ages birth-18 years yielded 1 additional article that was not a duplicate from prior searches. The search provided a total of 45 articles that discussed the use of 10 instruments for measuring self-efficacy in youth with T1DM and/or their caregivers.
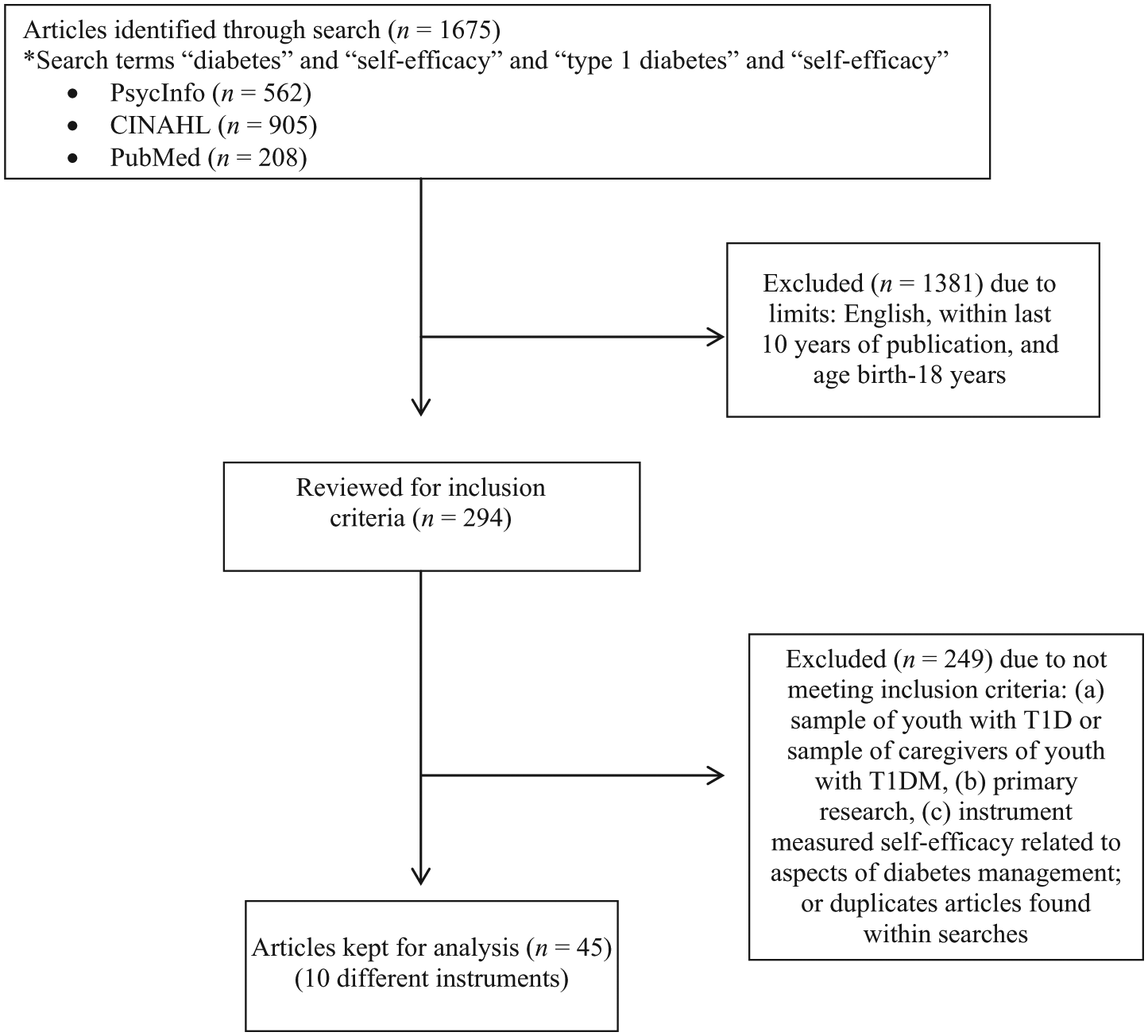
Flow diagram of the search process.
Tables 1 to 3 contain matrices of relevant articles categorized by type of self-efficacy instrument with particular attention to study sample, instrument characteristics, and instrument psychometrics. The Oxford Centre for Evidence-based Medicine-Levels of Evidence was used to evaluate each study based on study design and analysis. 13 Two of the investigators (LR and CJ) evaluated each study to determine the level of evidence and to establish interrater reliability. The level of agreement was 100%.
Instruments Used to Measure Self-efficacy in Type 1 Diabetes (T1DM) Youth and Caregivers a

A table summarizing each study is available from the author.
One study 27 used the Diabetes Management Self-efficacy Scale (DMSES) by Iannotti et al (2004) from paper presented at the Society of Pediatric Psychology National Conference on Child Health Psychology.
Theoretical Framework and Sample Used in Articles Measuring Self-efficacy
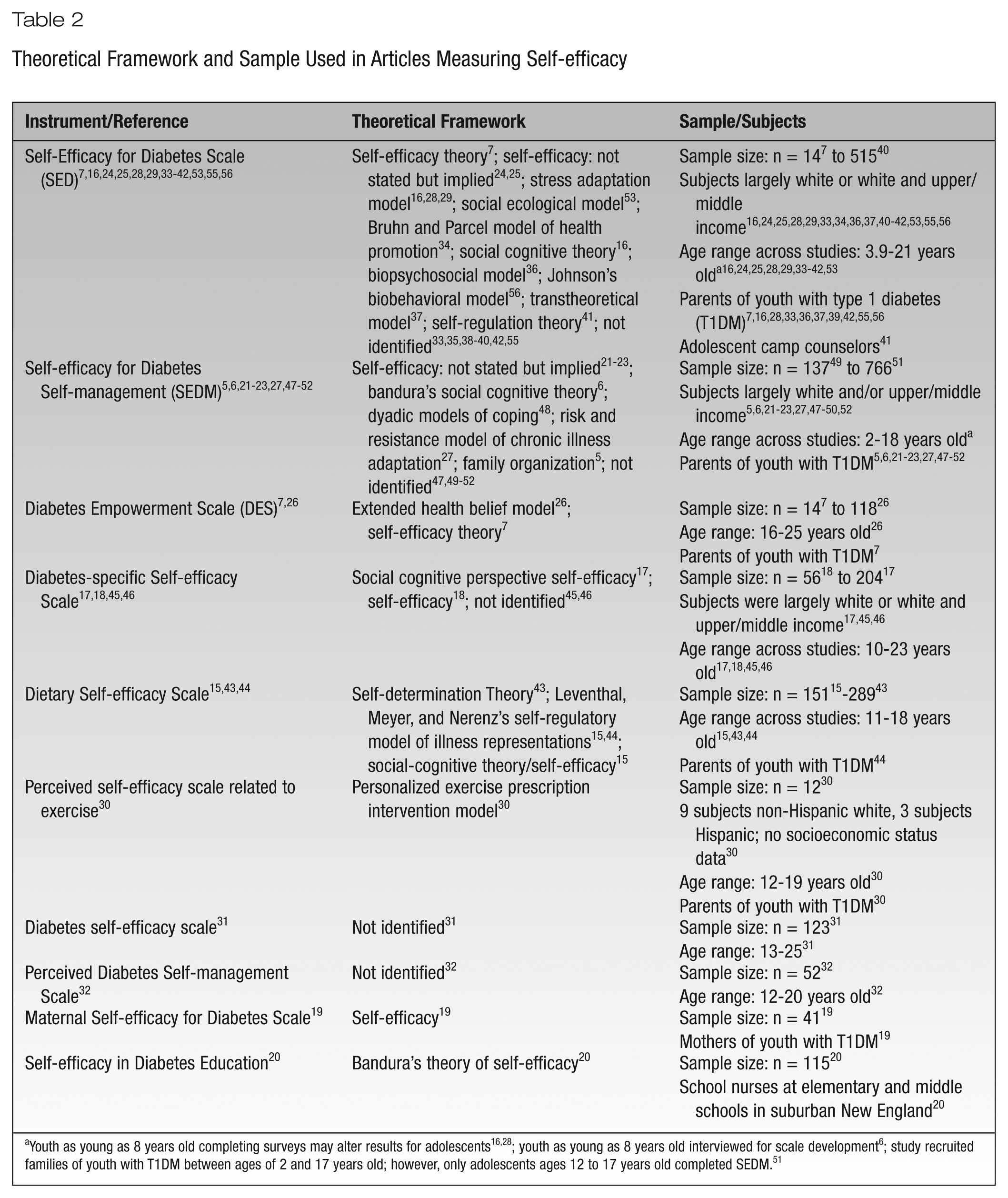
Youth as young as 8 years old completing surveys may alter results for adolescents16,28; youth as young as 8 years old interviewed for scale development 6 ; study recruited families of youth with T1DM between ages of 2 and 17 years old; however, only adolescents ages 12 to 17 years old completed SEDM. 51
Assessment of Instruments Used to Measure Self-Efficacy in Type 1 Diabetes (T1DM) Youth and Caregivers a
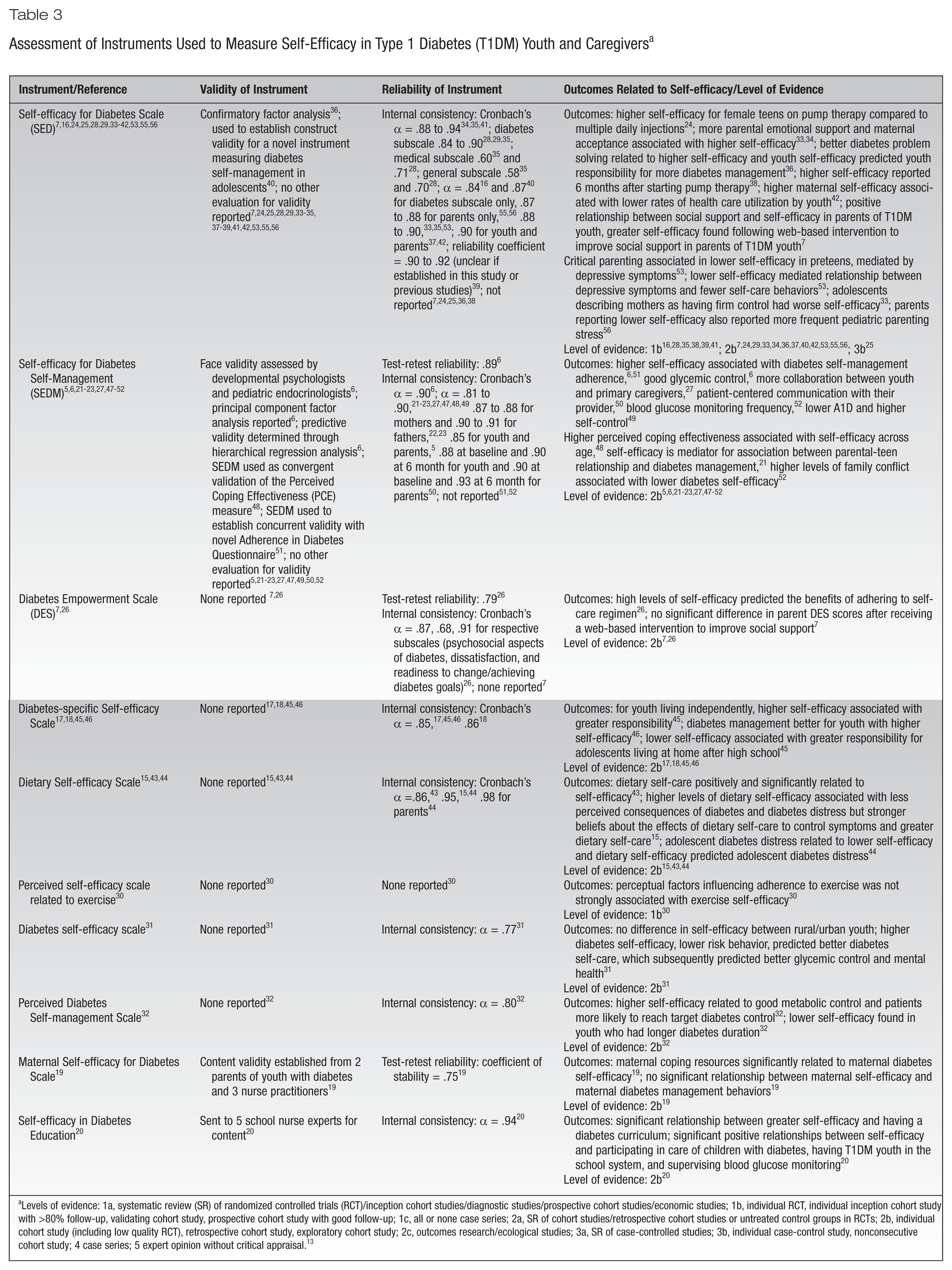
Levels of evidence: 1a, systematic review (SR) of randomized controlled trials (RCT)/inception cohort studies/diagnostic studies/prospective cohort studies/economic studies; 1b, individual RCT, individual inception cohort study with >80% follow-up, validating cohort study, prospective cohort study with good follow-up; 1c, all or none case series; 2a, SR of cohort studies/retrospective cohort studies or untreated control groups in RCTs; 2b, individual cohort study (including low quality RCT), retrospective cohort study, exploratory cohort study; 2c, outcomes research/ecological studies; 3a, SR of case-controlled studies; 3b, individual case-control study, nonconsecutive cohort study; 4 case series; 5 expert opinion without critical appraisal. 13
Results
Research Process
The authors summarized the results based on theoretical frameworks for the respective articles, sample characteristics, instrument descriptions, scoring, and psychometrics (Tables 1 to 3). Table 1 identifies and describes the various instruments and the identified studies, while Table 2 includes information about the theoretical framework and sample in each article, and Table 3 describes the psychometric details of the measurements and outcomes related to self-efficacy.
Theoretical Frameworks
Theory-driven measurement assigns meaning to a research question, clarifies associations between concepts, and gives researchers a guide to explore a specific concept.8,14 A lack of a theoretical framework in instrument development jeopardizes the ability to adequately measure a concept. Despite the importance of a theoretical framework, many of the articles analyzed in this integrative review did not identify a theoretical framework, as indicated in Table 2, column 2.
Of the 28 articles evaluating youth or caregiver self-efficacy that identified or implied a theory, the most common framework was Bandura’s social cognitive theory (SCT) or model of self-efficacy.6,7,15-20 Although not explicitly stated, an additional 5 studies implied Bandura’s model of self-efficacy.21-25
Less common, yet applicable, frameworks included the extended Health Belief Model (HBM), 26 the risk and resistance model of chronic illness adaptation, 27 and the stress adaptation model.16,28,29 Each of these guiding models related to the construct of self-efficacy or patient/family adaptation to chronic disease management.
Sample and Subjects
Since the purpose of this integrative review was to identify self-efficacy measures in youth with T1DM and their caregivers, all identified studies included a sample of children or adolescents or parents/caregivers. Many studies had youth ≥10 years old complete the various instruments; yet, a few had participants as young as 8 years old.16,28 Of the 45 articles in the review, 39 encompassed an adolescent age range of participants5,6,15-18,21-53 (10-18 years old as defined by the American Psychological Association), 54 25 studies included parents as participants,5-7,16,19,21-23,27,28,30,33,36,37,39,42,44,47-52,55,56 and 11 studies measured parental self-efficacy in diabetes management5,7,19,37,42,55,56 or parental confidence in their child.22,23,44,50 One study measuring self-efficacy in diabetes care and education focused on the role of school nurses in diabetes management (including both T1DM and type 2 diabetes), 20 and 1 focused on the role of camp counselors. 41
An analysis of participant demographics revealed that 31 studies had a homogenous sample that included white and/or middle-class participants.5,6,16,17,19,21-25,27-30,33,34,36,37,40-42,45-50,52,53,55,56 Additionally, 10 studies took place internationally, outside of the United States.15,18,26,31,32,35,38,43,44,51
Evaluation of Instruments
This integrative review identified 10 instruments to measure self-efficacy in youth with T1DM and their caregivers. Given the inclusion criteria of articles from the past decade (2003-2013), the initial literature search did not reveal the original articles that described all of the instruments. The following instruments were identified: (1) Self-efficacy for Diabetes scale (SED), (2) Self-efficacy for Diabetes Self-management scale (SEDM), (3) Diabetes Empowerment Scale (DES), (4) Diabetes-specific Self-efficacy Scale, (5) Dietary Self-efficacy Scale, (6) Perceived Self-efficacy Scale related to exercise, (7) Diabetes Self-efficacy Scale, (8) Perceived Diabetes Self-management Scale (PDSMS), (9) Maternal Self-efficacy for Diabetes Management Scale, and (10) Self-efficacy in Diabetes Education (SEDE). Of the 10 instruments, 4 were used in youth,17,18,30-32,45,46 3 were used in youth/parents,5-7,15,21-23,26,27,43,44,47-52 1 was used in youth/parents/camp counselors,7,16,24,25,28,29,33-42,53,55,56 1 was used in mothers, 19 and 1 was used in school nurses. 20 The most commonly used instruments were the original and adapted SED7,16,24,25,28,29,33-42,53,55,56 and the original and adapted SEDM.5,6,21-23,27,47-52 One study used 2 instruments, the SED and the DES, to measure parental self-efficacy. 7
Instrument Description
All instruments used either a Likert-like scale or a semantic differential scale, 57 except the Diabetes-specific Self-efficacy Scale, which used scoring from 20 (F) to 100 (A+) to evaluate perceived self-efficacy. The instruments ranged from 7 to 35 items with 2 of the surveys (SED and DES) consisting of 3 different subscales within the self-efficacy measurement. The SED included subscales for diabetes, medical, and general situations. The 3 DES subscales included managing psychosocial aspects of diabetes, assessing dissatisfaction, and readiness to change/goal setting. While all questionnaires assessed perceived self-efficacy related to confidence in diabetes management, 1 instrument explicitly measured dietary self-efficacy,15,43,44 another measured exercise self-efficacy, 30 and 1 assessed confidence in diabetes education. 20 Surprisingly, only 1 study described modifying an instrument (SED) to incorporate pump therapy. 29 The literature search did not identify other measures that assessed youth self-efficacy related to current technologies, for example, pump therapy or continuous glucose monitoring.
Measurement of Perceptions and Scoring
The instruments’ response categories ranged from 5- to 11-point Likert-like scales and varied as to whether low or high scores indicated less or greater self-efficacy. All articles discussed how scoring related to the level of self-efficacy and/or provided the mean participant scores with the respective instruments. One study using the SEDM survey combined youth and parent scores to evaluate family self-efficacy, 5 although this combination in scoring differed from the original description of the instrument. 6
Method of Administration
The method and site for instrument completion varied, ranging from the clinical or camp setting to completion by mail, the web, or telephone; some studies utilized more than 1 approach. The majority of studies had participants complete the instruments at the time of a medical or study visit.5,16,18,21,23,24,27,28,31,32,35-37,39,40,42,43,47,48,50,52,56 The second most frequent method of administration was via the mail,6,7,15,20,22,26,33,49,55 followed by the web.17,29,45,46,51
Reliability
Most articles reported reliability statistics for the self-efficacy instrument under study. Although certain studies may not have explicitly stated reliability or validity data, the psychometrics from the original studies prior to 2003 were identified; however, caution is warranted when applying these psychometrics to different samples. Most studies using the SED or an adapted version of the scale reported internal consistency for the diabetes-specific subscale16,29,40 or total scale33-35,37,39,41,42,53,55,56 with α values ranging from .84 to .94, indicating a high internal consistency. Cronbach’s α values of .70 and greater are considered acceptable. 58 Other studies using all 3 subscales of the SED reported α values of .84 and .90 for the diabetes subscale, .60 and .71 for the medical subscale, and .58 and .70 for the general subscale.28,35 The original article by Grossman and colleagues cited a Kuder-Richardson coefficient α of .90 for the total scale, .92 for the diabetes subscale, as well as significant intercorrelations among the scales in a study sample of 68 adolescents with T1DM. 59
Studies using the SEDM scale revealed high alpha coefficients ranging from .81 to .93.5,6,21-23,27,47-50 Adapted versions of the SEDM used in parents as well as youth performed well, with high levels of internal consistency for parents (α = .85-.93)5,22,23,50 and slightly lower levels for youth (α = .81-.90).5,22,23,50 The DES demonstrated internal consistency across the 3 subscales of psychosocial aspects (α = .87), dissatisfaction (α = .68), and readiness to change/goal setting (α = .91), 26 which were slightly lower than the original assessments of the total scale (α = .96) and subscales of psychosocial aspects (α = .93), dissatisfaction (α = .81), and achieving goals (α = .91). 60 The Diabetes-specific Self-efficacy Scale reported Cronbach’s α of .8517,45,46 and .86, 18 which was higher than the originally reported .78. 61 The Dietary Self-efficacy Scale also reported high internal consistency with Cronbach’s α of .86 43 and .9515,44 for youth and .98 for parents, 44 while the original Dietary Self-efficacy Scale reported a Cronbach’s α of .94. 62 All but 1 of the studies representing the remaining 5 self-efficacy scales reported reliability information for the current study participants. The study using the Perceived Self-efficacy Scale related to exercise reported reliability coefficients from past studies only. 30 The internal consistencies for the Diabetes Self-efficacy Scale, the PDSMS, and the SEDE survey ranged from α = .77 to .94.20,31,32 The original PDSMS reported a relatively high internal consistency with a Cronbach’s α of .83 in a sample of adults with T1DM or type 2 diabetes (T2DM). 63 Similarly, the original report of Diabetes Self-efficacy Scale had an α of .85 in a sample of adults with T2DM. 64
Test-retest reliability was reported for the Maternal Self-efficacy for Diabetes Management Scale, with a 37% response rate in repeating the measure after 2 weeks and a modest correlation of .75 19 and was reported for the DES with test-retest reliability of .79. 26 In the original study, researchers expanded the SEDM psychometrics by establishing test-retest reliability 6 ; they administered the survey twice in 1 week to 38 youth, revealing a test-retest intraclass correlation coefficient of .89, reflecting the stability of the scale over time. 65 The original Perceived Self-efficacy related to exercise scale also reported reliability using the test-retest method with a result of .989 66 and the original Diabetes Self-efficacy Scale reported a test-retest of .80. 64
Validity
A few of the articles reported content and face validity of the self-efficacy instruments. Content validity was established by consulting school nurses as experts for the SEDE instrument 20 and parents of youth with diabetes plus nurse practitioners for the Maternal Self-efficacy for Diabetes Management Scale.19,67 Similarly, 9 family interviews and consultation with experts in developmental psychology and pediatric endocrinology established face validity for the original SEDM scale. 6
Factor analysis was another approach to establish validity. In 1 article using the SED, the researchers performed a confirmatory factor analysis among variables that included self-efficacy to determine the strength of relationships among the variables. 36 In the original publication of SEDM scale, the authors reported extensive validity metrics, including factor analysis and predictive validity. 6 They identified significant although modest correlations between the SEDM scale and glycemic control (r = .21) and the youth (r = .37) and parent (r = .29) report on the Diabetes Self-management survey. 6 The original article describing the DES reported a single factor for the measure. 61
Other articles described construct, convergent, and concurrent validity. One study used the SED to establish construct validity for the survey measuring diabetes self-management, the Self-management of T1DM in Adolescents. 40 Although not directly related to the validity of the SEDM scale, 1 study used this instrument to establish convergent validity for another measure, Perceived Coping Effectiveness (PCE), 48 and another study used the SEDM survey to establish concurrent validity with an Adherence in Diabetes Questionnaire. 51
To identify other validity assessments, one must evaluate the original articles describing the self-efficacy instruments. The initial article using the SED reported evidence for criterion and construct validity for this measure 59 while the original DES article reported evidence for concurrent validity. 60 The original article describing the PDSMS also reported sufficient establishment of construct validity. 63 Pender and colleagues reported predictive validity, which was established with significant correlations with other variables for the Perceived Self-efficacy Scale related to exercise. 66 The original Dietary Self-efficacy article did not describe a validity assessment. 62
Feasibility of Instrument Use
The identified studies did not readily discuss the feasibility of implementation of the instruments. 8 In some cases, authors identified compensation amounts for study participation or the time required for completion; however, the time reported often involved completion of multiple questionnaires, not just the self-efficacy instrument. Therefore, it is difficult to ascertain how long each measure takes to complete. However, Table 1 lists the number of items per survey. Access to the instrument is another feasibility consideration. On an initial search, the majority of surveys do not seem readily available within the public domain and often require identifying the original article describing the instrument. The following instruments are publicly accessible: The DES is accessible on the Michigan Diabetes Research and Training Center website, 68 and the Perceived Self-efficacy Scale related to exercise 30 and the Diabetes Self-efficacy Scale 31 are available through websites noted in the studies’ reference lists. The SEDM and PDSMS items are listed as tables in the original studies.6,63 Additionally, the original studies describing the Maternal Self-efficacy for Diabetes Management Scale and the SED included the scales as appendices in the articles.59,67
Conclusions
Research Process
Theoretical Issues
Despite the importance of theory-driven research, not all articles in this integrative review on self-efficacy identified a theoretical framework. Instruments based on a theoretical framework and theoretical definition of the concept of interest will ultimately provide a better means to operationalize the concept. 8 Not surprisingly, most studies that did recognize a guiding framework used Bandura’s SCT or the model of self-efficacy. The 6 constructs of the SCT provide a framework for health promotion and chronic disease management to translate health knowledge into positive health outcomes. 9 These health behavior constructs include the following: knowledge, perceived self-efficacy, outcome expectations, goals, perceived facilitators, and impediments. 9 Knowledge and personal motivation will help individuals face challenging situations, which is particularly important in the self-management of chronic disease. 9 Moreover, the SCT highlights how individuals proactively cope and adapt to environmental stressors by relying on personal cognitive and emotional resources. 69 The SCT is a natural framework to explore the concept and measurement of self-efficacy as well as one’s perceived ability to face challenging situations, 70 especially in youth managing the rigors of T1DM while navigating the developmental stages of pediatric growth and development. Additionally, self-efficacy, a central component to the SCT, relates to an individual’s assessment of personal capabilities in a certain situation and the belief that carrying out behaviors will lead to a specific outcome.20,70 Utilizing the SCT or the model of self-efficacy as the underlying framework for development of self-efficacy instruments provides a theoretical overview of how youth with T1DM or their caregivers may carry out specific behaviors related to diabetes management in various scenarios.
Researchers should also consider the social ecological model (SEM) when measuring self-efficacy in youth with T1DM, as 1 study identified through this review did. 53 Similar to SCT, the SEM has been used to guide health promotion and may provide a unique perspective to assess the multifactorial relationships involved in the concept of self-efficacy for youth with T1DM. 71 This widely used framework highlights the potential for dynamic interactions between the individual’s environment and layers of social support. Furthermore, this model would have direct application to evaluating various levels of caregiver self-efficacy particularly as it relates to the youth with T1DM.
Methodological Issues
The prevalence of T1DM in older children is highest in non-Hispanic white youth, 72 as reflected in the homogenous participant pool of predominately white youth in the studies reviewed previously. Thus, the results of this integrative review may not be generalizable to non-white youth with T1DM. Future research should include purposeful sampling of minority youth with T1DM. Additionally, the majority of participants across the reviewed studies were from higher socioeconomic status (SES) backgrounds. This further limits the generalizability of the current assessments of self-efficacy instruments because youth and families from lower SES backgrounds may inherently face more challenges related to financial stressors, additionally impacting self-efficacy. Identifying and testing appropriate measurement instruments to evaluate self-efficacy in these vulnerable populations may be increasingly important to provide greater understanding of the relevance of this concept in all youth with T1DM.
This integrative review identified self-efficacy instruments at the individual, parent, camp counselor, and school nurse level. The SED, SEDM, DES, Dietary Self-efficacy scale, the Maternal Self-efficacy for Diabetes scale, and the SEDE all measure an aspect of caregiver self-efficacy. Instrument selection depends on the specific participant sample and focus. Capturing caregiver self-efficacy is valuable as both family and caregivers outside of the family are an integral part of a youth’s success with diabetes management. Additionally, researchers and clinicians will be able to fine-tune education efforts by identifying gaps in confidence related to aspects of diabetes management for those involved in the care of the child. However, no articles evaluated peer self-efficacy or the perceived confidence of helping a friend manage diabetes in challenging situations. Because support typically shifts from the family system to friends and peers in adolescence, 73 it would be useful to evaluate peer self-efficacy in diabetes management to further guide adolescents through this developmental transition. Furthermore, youth with T1DM often have multiple caregivers beyond the parents or school nurse. Use of self-efficacy instruments to assess confidence levels in T1DM management for grandparents, babysitters, and athletic coaches, among others, may expand the self-efficacy knowledge base and identify essential educational needs of these important caregivers and other key support groups in the community.
Instruments
Methods of Administration, Feasibility, and Psychometrics
There were no major issues identified in administering the 10 instruments to youth or their caregivers, since the majority of surveys were administered during an office visit or by mail. One might not expect different psychometric properties according to response mode, but future research could clarify this issue. Although none of the studies noted the exact time required to complete the respective self-efficacy assessments, time to completion did not appear to be a burden for survey administration. One must also consider that all instruments, except for 3, were administered in English,18,32,51 an important consideration when establishing eligibility criteria. Survey translation would help broaden international access and generalizability. The main feasibility issue in fielding the various surveys is access to the instruments. The research team should consider the need to search for and possibly purchase surveys when developing a study budget.
Most instruments measuring self-efficacy demonstrated internal consistency, a form of equivalence reliability, indicating the items within the instrument conceptually fit with one another. 65 However, it is important to consider that the internal consistency may vary based on the number of response options used in the Likert scale with a higher number of responses resulting in greater internal consistency 74 and that the alpha value may also vary based on the number of survey items. 58 Both the number of Likert options and survey length varied based on the different instruments. Apart from the SED and SEDM, extensive validity assessments for the different instruments were not frequently described. Often, the authors had to revert back to the original article describing the psychometrics of the self-efficacy instrument to obtain validity evidence. Even in these cases, the original sample may have included adults with T1DM or T2DM versus youth with T1DM. The lack of validity data reported in the identified articles is a limitation of the contemporary literature. Validity assessments are paramount to evaluating an instrument’s capacity to measure self-efficacy or the concept of interest within a certain population. 65 During instrument development and refinement, when translating available instruments into different languages, or when using instruments in different patient samples, validity tests reinforce the adequate measurement of self-efficacy. Additional research efforts should establish further psychometric analysis of these instruments in diverse populations of youth with T1DM because the sample homogeneity from the identified articles could limit the applicability of the results.
When evaluating the various self-efficacy instruments identified, it is important to acknowledge that many of the self-efficacy instruments were used in multiple articles highlighting the affinity for use. The SED and SEDM were the self-efficacy instruments most often used in the identified articles. Additionally, several studies from this integrative review revised or adapted the self-efficacy instrument to include a certain population, such as youth-parent dyads for example, which clinicians and researchers should consider when selecting an instrument based on a specific population.
Another element to consider when evaluating self-efficacy instruments for future research and clinical care pertains to the ability to measure self-efficacy in the contemporary era of diabetes technologies. One article described modifying the SED instrument to include current aspects of T1DM (pump therapy), 29 yet a lack of instruments to measure self-efficacy pertaining to current diabetes technology is a pertinent limitation of the available instruments. A caveat to this is that not all articles identified through the integrative review or the original articles describing the instruments included a description of survey items. While advances in diabetes technology aim to improve self-management and glycemic control, it is important to assess an individual’s confidence in the ability to use such devices. Currently available self-efficacy instruments would provide added benefit with the inclusion of assessments of self-efficacy related to technology advancements in the contemporary diabetes era. Alternatively, clinicians and researchers could design instruments to specifically evaluate youth and parent confidence related to using diabetes technologies, such as continuous glucose monitors, which are increasingly relevant with the advent of the Artificial Pancreas Project. 75
Implications
Reliable and valid instruments to measure a concept of interest, such as self-efficacy, are essential for quality research and use in clinical care. The use of well-constructed measurements will confirm potential results and enhance opportunities to generalize findings to populations at large. This review is relevant to research, clinical care, and diabetes education of youth with T1DM because it identified several reliable and valid instruments to evaluate self-efficacy, an important component of diabetes self-management. The available instruments vary in length with respect to the targeted participant age group and whether caregivers are the focus of the assessment. Although certain studies may not have explicitly stated reliability or validity data, the psychometrics were identified in articles published prior to the 2003-2013 timeframe; however, caution is warranted if applying these psychometric properties across time and in different groups. 58
This integrative review identified various gaps that could guide future research and instrument development. This search was restricted to the past decade and thus was not exhaustive. Of particular note is the absence of self-efficacy instruments or proxy reports that focus on peers of youth with T1DM. During the teenage years, adolescents often seek support of friends and peers, with less emphasis on support from the family unit. 73 Therefore, it would be important to assess peer self-efficacy in assisting friends with T1DM in various diverse settings. Additionally, in all youth, and specifically younger children, it would be beneficial to identify valid and reliable instruments to measure self-efficacy in other caregivers, such as grandparents. Such research across other care providers and possibly peers could help to identify knowledge deficits and avenues for education of important groups for social support of youth with T1DM. Future studies are needed to implement self-efficacy measurements in minority populations, as well as international samples, to further assess the psychometric properties of these instruments and to broaden their application to youth with T1DM globally. Additionally, instruments to measure the construct of self-efficacy in the current era of advanced diabetes technologies, including use of insulin pumps and continuous glucose monitoring technologies, appear to be needed. A lack of instruments to measure self-efficacy related to diabetes technologies implies that the available self-efficacy instruments need to be adapted or new instruments need to be developed to be relevant in the contemporary era.
In selecting an instrument to measure self-efficacy in the pediatric population with T1DM and their caregivers, the clinical or research team must contemplate various factors. One must consider the population (ie, youth, parents, school nurses, camp counselors), length of the scale, available psychometric data, availability of the measure, and the particular aspect related to diabetes management that the self-efficacy scale measures (ie, diet, physical activity, general diabetes self-efficacy). Having specific criteria will guide the instrument selection. Additionally, when identifying instruments for use in the pediatric population and in the context of diabetes education, it is important to consider how the concept of self-efficacy can span throughout childhood and at what age youth are able to understand and answer questions related to self-efficacy. Many studies identified in this integrative review had youth ≥10 years old complete the various instruments, including the self-efficacy assessments; however, some studies had participants as young as 8 years old. A final consideration when evaluating instruments for use with caregivers is to determine whether the purpose of the instrument is to assess the caregiver’s own perception of confidence related to diabetes management or whether the instrument assesses the caregiver’s confidence in the child’s self-care, an important component to keep in mind when measuring the construct of self-efficacy.
In conclusion, when selecting an instrument to measure self-efficacy in youth with T1DM and their caregivers, it is important to remember that one’s perceived ability for diabetes self-management reflects a constellation of behaviors. Furthermore, improvements in intensive therapy options can add to self-management challenges as diabetes technologies continue to evolve, reinforcing the need to capture self-efficacy. The evolvement of T1DM technologies will require either making modifications to existing self-efficacy instruments or developing new instruments altogether; evaluation of the psychometric properties of these instruments will be necessary. It is essential to select an instrument that is appropriate, acceptable, feasible, and responsive to both the needs of the patient and the clinician or researcher as well as an instrument that it is valid, reliable, and precise in measurement to ensure clinical and research integrity are maintained.
Footnotes
Acknowledgements
The authors would like to express appreciation to Mathew Gregoski, PhD, and John Dinolfo, PhD, for their guidance and encouragement.
Funding:
This research was supported by the NIH grant P30DK036836. The content is solely the responsibility of the authors and does not represent the official view of this organization.