
Abstract
Purpose
The purpose of the study was to determine whether there are any race-related disparities in the prevalence of provisions for diabetes education in primary care clinics for patients with diabetes and prediabetes.
Methods
A retrospective cross-sectional study of 3967 patients aged 14 to >89 years with prediabetes and diabetes. Medical record data from patient encounters within primary care clinics at a large academic medical health system between July 1, 2008, and July 31, 2013, were used to determine rates of referral for diabetes education by race. Multivariate logistic regression models were used to assess associations between race and referral to diabetes education. Separate regression models were computed for patients who were prediabetic and diabetic. Adjusted models included age, sex, A1C, health care utilization, smoking, and diagnosis for depression, hyperlipidemia, hypertension, vascular disease, and obesity.
Results
Compared to that of white patients, a significantly higher prevalence of African American patients with prediabetes were referred to diabetes education, and this association was also observed in patients with diabetes. In fully adjusted models, white patients with prediabetes were significantly less likely to be referred.
Conclusions
Being African American independently increased the likelihood of referral for diabetes education in patients with prediabetes and patients with diabetes. After adjusting for patient comorbidities and risk factors, this association remained significant for patients with prediabetes. Additional research is needed to determine if provider beliefs and attitudes regarding race and diabetes education account for this association.
The prevalence of diabetes in the United States continues to rise, with 8.3% of the population being diagnosed with it in 2010. 1 Additionally, 35% of US adults have been diagnosed with prediabetes, and that prevalence increases to 50% in adults aged ≥65 years. Diabetes is known to affect minorities at higher rates; African American patients are nearly 80% more likely to receive a diagnosis of diabetes as compared to white patients.
Racial disparities in diabetes care and outcomes are well documented in the medical literature. 2 African American patients with diabetes are less likely than white patients to achieve glycemic, cholesterol, and blood pressure goals and receive recommended screening and preventative measures.3-9 African American patients are also more likely than white patients to develop poor long-term diabetic outcomes, including diabetic retinopathy, chronic kidney disease, and lower extremity amputations.2,10-13
National guidelines for diabetes management recommend that health care providers refer all such patients—that is, with either diabetes or prediabetes—for self-management education and ongoing support.14,15 The benefits of diabetes education are well documented in the literature and are associated with improved short-term outcomes and reduction in health care costs.16-22 Despite these benefits, referral rates for diabetes education remain low.23-26 There are limited existing reports of race disparities in referral to diabetes education, and the data are inconsistent.23-28 A 2011 survey of Canadian primary care providers reported referral rates to diabetes education programs of 46% and 39% for patients with diabetes and prediabetes, respectively. 23 In a 2005 secondary analysis from the National Ambulatory Medical Care Survey from 1997 to 2000, African Americans were more likely than whites to receive exercise and diet counseling during primary care office visits, but this difference was no longer seen when isolated to patients with diabetes. 27 Similarly, Peek et al analyzed data from the 2002-2004 National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey and observed no difference in lifestyle counseling or referral among African American and white patients with diabetes. 25 The recent DAWN2 study also observed no difference in self-reported diabetes education among African American and white, non-Hispanic patients. 28 However, Brown-Guion et al found that being African American independently increased the likelihood of diabetes education referral. 29 Furthermore, in addition to inconsistent results, the majority of literature has been limited to provider or patient self-reported diabetes referral.23-25,27-29
The Diabetes Prevention Program study showed that lifestyle education to lose weight and increase physical activity reduced the development of type 2 diabetes by 58% during a 3-year period, and this reduction was even greater among adults aged ≥60 years, at 71%. 30 The Diabetes Prevention Program study also found that prevention or delay of type 2 diabetes with lifestyle intervention was effective in all racial and ethnic groups studied, including African Americans and whites, and has been shown to persist for at least 10 years. 31 Despite the growing evidence for the need for patient education, limited data exist regarding the frequency of referral for education in patients with prediabetes or if the racial disparities are seen in the referral rates.
To elucidate the potential of race disparities in referral to diabetes education, documented referrals from medical records of a large academic primary care system were used to determine if there was a difference in diabetes education referral rates between African American patients and white patients. Analyses were computed separately for patients with prediabetes and diabetes.
Method
Patient Population
Data were obtained from an electronic medical record database of 27 225 primary care patients associated with approximately 110 providers. This Primary Care Patient Data Registry captures all clinic encounters from family medicine and general internal medicine at a large academic medical health system located in the St Louis, Missouri, metropolitan area. Clinics include 1 urban and 2 suburban sites. Patients who had at least 1 encounter (eg, office visit, procedure visit, or clinical support) between July 1, 2008, and July 31, 2013, are included in the registry. In the cohort as a whole, 59.4% of patients are white; 34.6%, African American; 4.1%, other race; and 2.0%, unknown. In the entire cohort, 6.8% were <18 years old; 39.7%, 18 to 40 years; 32.7%, 41 to 60 years; and 20.8%, ≥61 years.
For the present study, those with missing race and/or sex information (n = 1655) were excluded, resulting in 25 570 patients available for analysis. Sufficient statistical power precluded contrasting difference by race other than white compared to African American race. Patients were then selected who had an ICD-9-CM code indicating a diagnosis for diabetes (250.x0, 250.x2), as were all patients who had either an ICD-9-CM code of 790.29 or a glycated hemoglobin (A1C) value of 5.7% to 6.4% (39-46 mmol/mol), indicating a diagnosis of prediabetes—all of which resulted in a study population of 3967 patients aged 14 to >89 years (30.3% with prediabetes, 69.7% with diabetes).
Design
Patients were coded as having been referred to diabetes education if they had 1 or more of the following institution-specific referral orders placed: referral to dietitian, referral to family and community medicine clinical pharmacist, or referral to diabetic education.
Covariates hypothesized to be associated with referral for diabetes education and race included demographic variables age and sex as recorded in the medical record, A1C control, health care utilization, depression, hyperlipidemia, hypertension, vascular disease, obesity, and smoking status. Duration of diabetes and socioeconomic status are also hypothesized to be associated with referral for diabetes education and race; however, this information is not available within the electronic medical record database and therefore was excluded.
Demographic covariates included age and sex. A1C was classified as controlled (A1C < 7.0%, 53 mmol/mol), uncontrolled (A1C ≥ 7.0%, 53 mmol/mol), or unknown. Health care utilization was measured by the average number of clinic visits per month computed for each patient and was modeled as a binary variable measuring high utilizers (the top 25th percentile of average clinic visits per month) versus nonhigh utilizers (the lower 75th percentile). Diagnosis was included if it was the primary reason for at least 1 clinic visit during the study period. ICD-9-CM codes were used to define the presence of depression (296.2, 296.3, 311), hyperlipidemia (272.0-272.4), hypertension (401), and vascular disease (402-405, 410-417, 420-429, 430-438) at any time in observation period. Obesity was defined by body mass index (≥30.0 kg/m2) and/or an ICD-9-CM diagnosis (278.00). Smoking status was obtained from patient social history or an ICD-9-CM diagnosis for nicotine dependence (V15.82, 305.1) and categorized as never, past, or current. To be considered a case for depression, the patient must have had at least 2 ICD-9-CM diagnoses for depression within a 12-month period.
Analysis
The entire observation period was treated as a cross-sectional study. The prevalence of demographics and covariates were calculated and compared between African American (n = 2166) and white (n = 1801) patients using chi-square for categorical variables and independent samples t tests for continuous variables. Similarly, comparisons were made between African American and white within diabetes diagnostic strata (prediabetes or diabetes). Prevalence of covariates was also calculated and compared between those referred and not referred to diabetes education using chi-square or independent samples t tests. Crude bivariate odds ratios (ORs) and 95% confidence intervals (CIs) were assessed using binary logistic regression for each covariate and referral to diabetes education. Full multivariate logistic regression models calculated adjusted ORs and 95% CIs for all covariates, overall and stratified by prediabetes and diabetes. Due to variations in patient risk factors for prediabetes and diabetes (eg, change in body mass index) and because referral included dietary education not restricted to diabetes, we chose not to order the events in a survival framework. Thus, we modeled associations treating the data as a cross section.
Results
As shown in Table 1, of the 3967 eligible patients, 30.3% met criteria for prediabetes, and the remainder were diagnosed with diabetes. Of 2166 African American patients, 24.2% had prediabetes and 75.8% had diabetes, which was a significantly (P < .0001) higher prevalence of diabetes compared to white patients, of whom 37.7% had prediabetes and 62.3% had diabetes. A larger percentage of African American patients were referred to diabetes education when compared to white patients (14.8% vs 10.0%, P < .0001). A smaller percentage of African American patients had A1C values controlled when compared to white patients (33.7% vs 40.4%, P < .0001).
Characteristics of Primary Care Patients With Prediabetes or Diabetes, by Race a
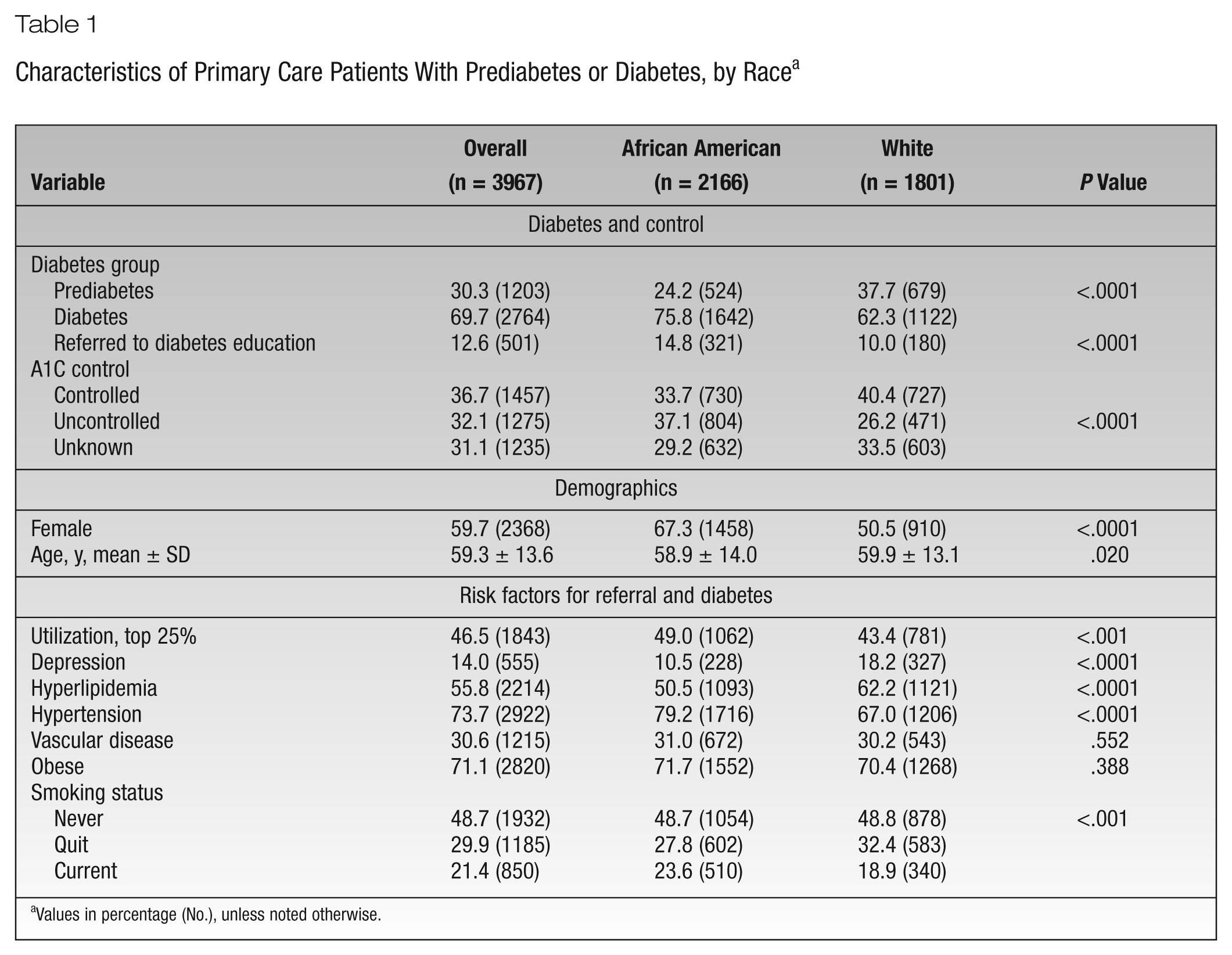
Values in percentage (No.), unless noted otherwise.
A disproportionate percentage of African American patients compared to white patients were female (67.3% vs 50.5%, P < .0001). African American and white patients were nearly the same age, on average, but large sample size resulted in the mean difference being statistically significant. A higher proportion of African American patients compared to white patients were in the highest quartile of health care utilization (49% vs 43.4%, P < .001). Compared to white patients, African American patients had a lower prevalence of depression and hyperlipidemia (P < .0001) and a higher prevalence of hypertension (P < .0001). Last, current smoking was more common among African American than white patients (23.6% vs 18.9%, P < .001). The prevalence of vascular disease and obesity was similar across race.
Table 2 shows the distribution of patient characteristics by race stratified by prediabetes and diabetes. Nearly twice the percentage of African American patients with prediabetes were referred to education compared to white patients with prediabetes (8.6% vs 4.0%, P < .001). More African American patients with diabetes were referred to diabetes education (16.8% vs 13.6%, P < .05). Among patients with prediabetes, African American patients were more often female (P < .001) and on average younger (P < .001). African American patients compared to white patients with prediabetes were more often high health care utilizers (P < .001), less likely to have depression (P < .01) and hyperlipidemia (P < .001), more likely be obese (P < .01), and more likely to currently smoke (P < .05).
Characteristics of Primary Care Patients by Race, Stratified by Prediabetes and Diabetes (N = 3967) a
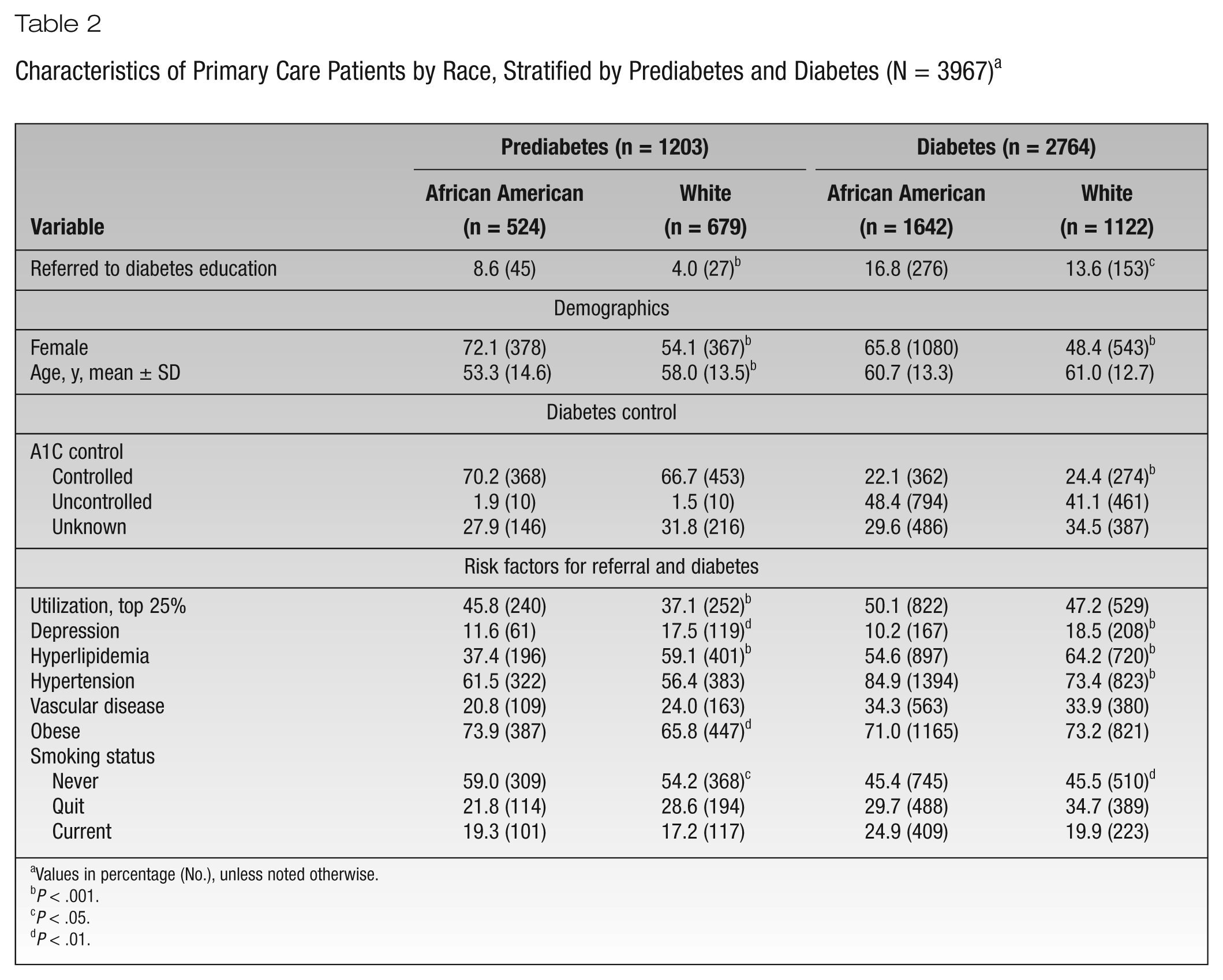
Values in percentage (No.), unless noted otherwise.
P < .001.
P < .05.
P < .01.
Among those with diabetes, African American compared to white patients were more often female (P < .001), less likely to have depression (P < .001) and hyperlipidemia (P < .001), more likely to have hypertension (P < .001), and more likely to currently smoke (P < .001). African American patients with diabetes were less likely to have controlled A1C compared to white patients (22.1% vs 24.4%, P < .001).
Bivariate associations between patient characteristics and referral to education are shown in Table 3. White patients compared to African American patients were significantly less likely to receive a referral (OR, 0.64; 95% CI, 0.53-0.78). Patients with diabetes compared to those with prediabetes were 2.89 times (95% CI, 2.23-3.74) as likely to have a referral. Having uncontrolled compared to controlled A1C was significantly associated with receiving a referral (OR, 2.51; 95% CI, 2.0-3.14). With each year of increasing age, there was a 2% decreased odds of referral (OR, 0.98; 95% CI, 0.98-0.99). Patients who were high utilizers, obese, and diagnosed with depression or hypertension were all significantly more likely to receive a referral (OR range: 1.30-2.46). Last, patients who quit smoking were less likely to receive referral (OR, 0.77; 95% CI, 0.61-0.96) as compared to those who never smoked.
Characteristics and Bivariate Associations of Primary Care Patients With Prediabetes or Diabetes by Referral to Diabetes Education (N = 3967) a
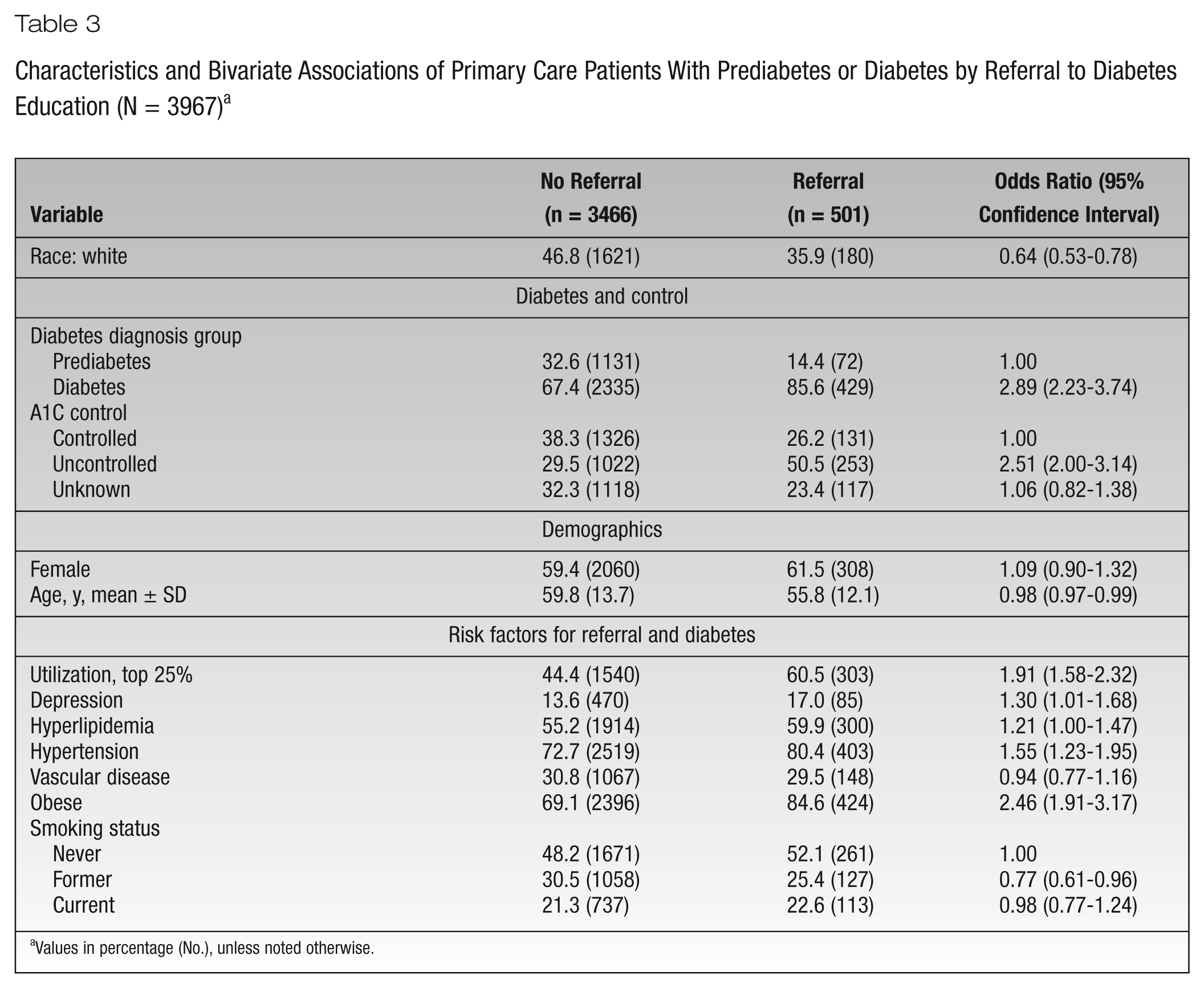
Values in percentage (No.), unless noted otherwise.
Results of multivariate logistic regression models estimating the association between race and other patient characteristics are shown in Table 4. Three models are reported separately—namely, for all patients, for those with prediabetes, and for those with diabetes. For the sample as a whole and after adjusting for all covariates, white compared to African American patients were significantly less likely to receive a referral to diabetes education (OR, 0.75; 95% CI, 0.61-0.93). Other factors positively associated with referral in the entire cohort included being diagnosed with diabetes compared to prediabetes (OR, 2.41; 95% CI, 1.78-3.27), high health care utilization (OR, 1.71; 95% CI, 1.39-2.10), being diagnosed with hypertension (OR, 1.36; 95% CI, 1.04-1.78), and obesity (OR, 1.82; 95% CI, 1.40-2.38). Increasing average age was associated with lower odds of referral (OR, 0.97; 95% CI, 0.96-0.98).
Multivariable Logistic Regression: Adjusted Associations of Patient Characteristics With Referral to Diabetes Education—Overall and by Diabetes Diagnosis Group a
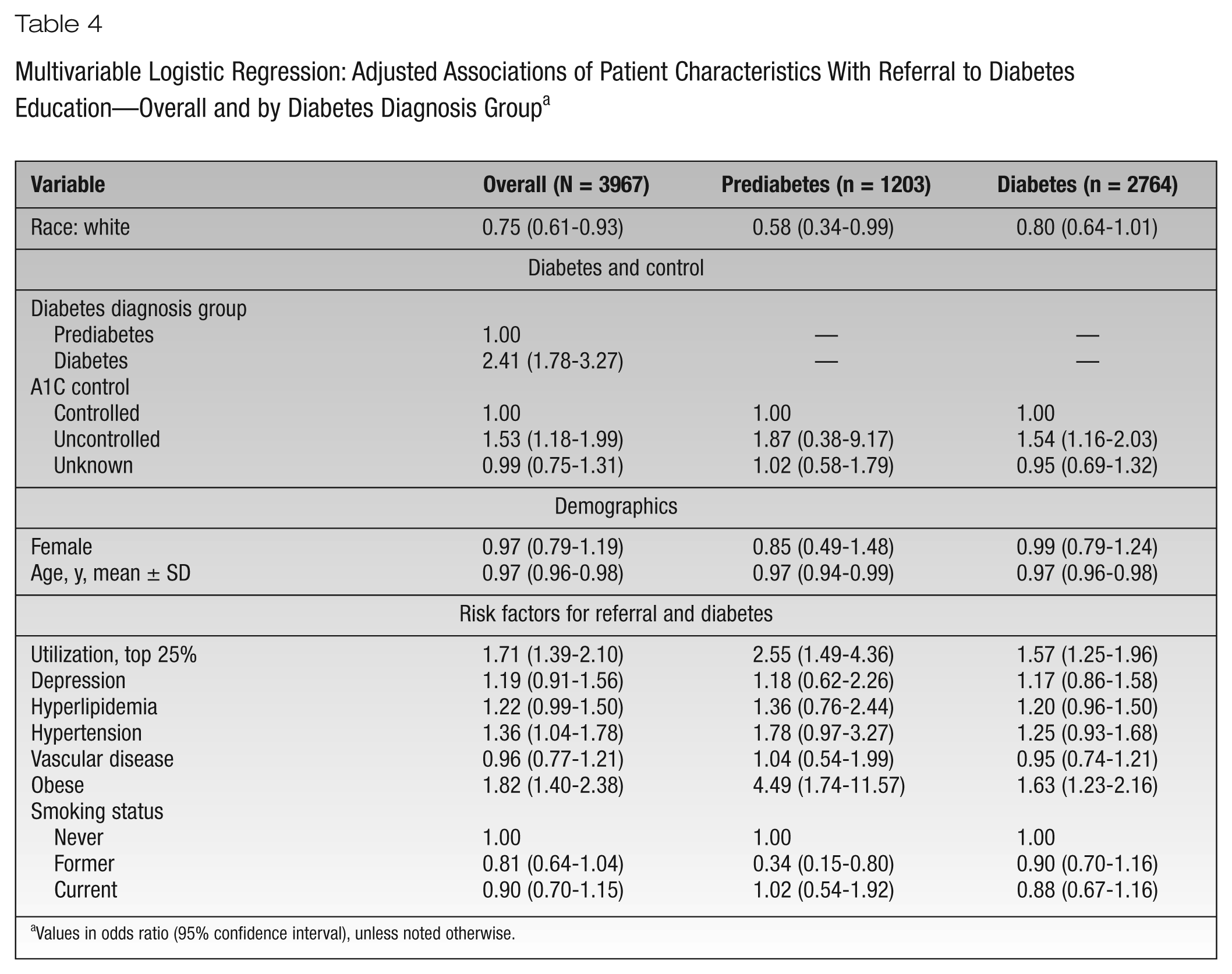
Values in odds ratio (95% confidence interval), unless noted otherwise.
Among patients with prediabetes and after controlling for covariates, white compared to African American patients were significantly less likely to receive a referral (OR, 0.58; 95% CI, 0.34-0.99). High utilization (OR, 2.55; 95% CI, 1.49-4.36) and obesity (OR, 4.49; 95% CI, 1.74-11.57) remained significantly and positively associated with referral. Older age remained significantly associated with lower odds of referral (OR, 0.97; 95% CI, 0.94-0.99), and persons who had quit smoking had a significantly lower odds of referral (OR, 0.34; 95% CI, 0.15-0.80) as compared to those who had never smoked.
Among patients with diabetes and after controlling for covariates, race was no longer significantly associated with referral (OR, 0.80; 95% CI, 0.64-1.01). Similar to the patients with prediabetes, older mean age remained inversely associated with referral (OR, 0.97; 95% CI, 0.96-0.98). Also, high utilization (OR, 1.57; 95% CI, 1.25-1.96) and obesity (OR, 1.63; 95% CI, 1.23-2.16) remained significantly associated with referral. Last, among patients with diabetes, having uncontrolled versus controlled A1C was significantly associated with referral (OR, 1.54; 95% CI, 1.16-2.03).
Conclusions
In a cohort of 3967 primary care patients diagnosed with prediabetes or diabetes, a significant race disparity for receiving referral to diabetes education was observed. Among patients with prediabetes, white patients were significantly less likely to receive referral for education (OR, 0.58). However, among those with diabetes, the magnitude of the association between race and referral decreased and was no longer significant (OR, 0.80) after adjusting for patient characteristics and comorbidities. The greater odds of referring African American patients with prediabetes to education remained significant after adjusting for other factors associated with referral, such as comorbid disease, obesity, and smoking status; thus, the association does not appear to be explained by greater comorbidity or greater prevalence of risk factors in African American patients. The association is not due to greater contact with providers because even after adjusting for high health care utilization, a racial disparity in referral for prediabetic patients remained.
Our results are consistent with the limited literature on race disparities and health education. The current results extend the current literature, especially in regard to the referral patterns for patients with prediabetes. Additionally, our results may be a more accurate measure of race disparity because documented referral to education as recorded in the electronic health record was used rather than self-reported referral. Any potential bias associated with patients’ ability to understand instructions or accurately recall encounters is overcome in our analysis.
It is unknown why a reverse disparity was identified in the current study. Economic or educational status was not included as a variable for this particular cohort, as it was not available within our electronic medical record data, but it could be hypothesized that providers’ referral patterns were dictated by their own beliefs of which patients would be more likely to manage diabetes devoid of education or financial resources. Reimbursement for diabetes education is a significant issue in the United States and could be linked to the lower provider referral rate; however, our site offers diabetes education to the majority of patients at little or no out-of-pocket cost, as it is a bundled service as part of our primary care program. An additional possibility could be lack of referral documentation. Furthermore, provider awareness of well-established disparities concerning diabetes management in African Americans could have contributed to the diabetes referral rate as well.
In addition, very few studies have addressed provider behavior regarding prediabetes diagnosis and treatment. Literature suggests that patients who meet the criteria for prediabetes are not necessarily documented as such within the medical record and that less than half of those are treated. 26 Our study showed similar findings among patients with prediabetes having only a 12.6% referral rate for diabetes education. In addition, our study revealed that there may be delays in updating diagnoses in the medical record, as indicated by the small number of patients identified within the prediabetes group with an uncontrolled A1c. Moreover, this suggests that there is a great deal of improvement to make in providers adopting a proactive approach to treatment of patients with prediabetes. Such efforts may limit the further progression to diabetes and slow the diabetes epidemic in the United States.
The missing A1C value is a potential limitation if its absence is associated with referral and race in a systematic and different direction from patients without missing data. Although we adjusted for missing data, we conducted additional sensitivity analysis by removing all subjects with missing A1C values. The smaller sample size resulted in broader confidence limits (OR, 0.84; 95% CI, 0.66-1.07), but the OR measuring the association between race and referral was similar to that obtained for the full sample (OR, 0.75; 95% CI, 0.61-0.93) and would not change our conclusions.
The broad age range of the patient cohort, 14 to >89 years, increases generalizability of the results. However, we recognize that very young patients may be managed differently when deciding on referral to diabetes education. Therefore, a sensitivity analysis removing the 6 patients under the age of 18 years was conducted, and results of regression models did not change.
Implications/Relevance for Diabetes Educators
Overall, the diabetes education referral rate for this study was surprisingly low when considering the large burden that diabetes contributes to society. As a result of this study, it is evident that further exploration into provider behaviors in diabetes intervention programs and its relationship with race need to be studied. In addition, it appears that a systemwide process change, such as making diabetes education referral a default action in the electronic chart, may be beneficial in improving diabetes care.
Footnotes
Contribution Statement
D.R.H-A. and E.F.C. conceived the study. J.S. performed all data extraction. J.F.S. oversaw the design and analyses of the study. D.R.H-A., E.F.C., J.S., and J.F.S. participated in data analysis planning, interpretation of study findings, and drafting and revising the manuscript for publication. J.F.S. is the guarantor of this work and, as such, has full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Conflicts of interest:
No potential conflicts of interest relevant to this article were reported.
Funding:
An educational grant from the Mindlin Foundation provided partial support for J.F.S.’s contribution.