
Abstract
Purpose
Patients with low literacy, low numeracy, and/or linguistic needs can experience challenges understanding diabetes information and applying concepts to their self-management. The authors designed a toolkit of education materials that are sensitive to patients’ literacy and numeracy levels, language preferences, and cultural norms and that encourage shared goal setting to improve diabetes self-management and health outcomes. The Partnership to Improve Diabetes Education (PRIDE) toolkit was developed to facilitate diabetes self-management education and support.
Methods
The PRIDE toolkit includes a comprehensive set of 30 interactive education modules in English and Spanish to support diabetes self-management activities. The toolkit builds upon the authors’ previously validated Diabetes Literacy and Numeracy Education Toolkit (DLNET) by adding a focus on shared goal setting, addressing the needs of Spanish-speaking patients, and including a broader range of diabetes management topics. Each PRIDE module was evaluated using the Suitability Assessment of Materials (SAM) instrument to determine the material’s cultural appropriateness and its sensitivity to the needs of patients with low literacy and low numeracy. Reading grade level was also assessed using the Automated Readability Index (ARI), Coleman-Liau, Flesch-Kincaid, Fry, and SMOG formulas.
Conclusions
The average reading grade level of the materials was 5.3 (SD 1.0), with a mean SAM of 91.2 (SD 5.4). All of the 30 modules received a “superior” score (SAM >70%) when evaluated by 2 independent raters. The PRIDE toolkit modules can be used by all members of a multidisciplinary team to assist patients with low literacy and low numeracy in managing their diabetes.
Poor health literacy and numeracy are known barriers to optimal diabetes management. Health literacy has been defined as “the degree to which individuals have the capacity to obtain, process, and understand basic information and services needed to make appropriate decisions regarding their health.” 1 Patients with low literacy levels have lower disease-specific knowledge, report lower quality of life, and have poorer health-related outcomes—even after adjustment for potential confounders such as education and socioeconomic status.1 -10 Poor health literacy is independently associated with worse diabetes knowledge, self-management, and glycemic control (A1C).6 -12
Despite the strong correlation between literacy skills and quantitative skills, 13 people with adequate verbal literacy skills often demonstrate poor numeracy skills. 14 Numeracy has been defined as “the ability to understand and use numbers in daily life.” 12 Health numeracy is defined as “the individual level skills needed to understand and use quantitative health information, including basic computational skills, ability to use information in documents and non-text formats such as graphs, and ability to communicate orally.” 15 Health numeracy is particularly important for patients with diabetes because diabetes self-management requires both basic and complex multistep mathematical skills, such as interpreting blood glucose monitoring, counting carbohydrates, and applying a correction scale for dosing insulin. In recent studies, low health numeracy has been significantly associated with worse diabetes self-management, worse perceived self-efficacy, and A1C that is above goal. 11
Low health literacy and numeracy are common among racial and ethnic minorities, particularly Hispanic/Latino patients, 15 who are at an increased risk for diabetes 16 and are more likely to have worse clinical outcomes and more diabetes complications than non-Hispanic/Latino patients.17 -20 The National Adult Literacy Survey and the National Assessment of Adult Literacy found that approximately 65% of Hispanic/Latino adults surveyed had basic or below-basic literacy skills. 13 Therefore, efforts to address the needs of patients with limited health literacy and numeracy should place special emphasis on Hispanic/Latino patients by tailoring education to meet their needs.
Prior research has shown that modifications to traditional models of diabetes teaching and counseling that accommodate patients with limited health literacy and numeracy can improve diabetes-related behaviors and outcomes.21 -24 David Baker developed a conceptual model to demonstrate the relationship between individual capacity, health literacy, and health outcomes. While individual capacity cannot easily be modified, the complexity of the printed and spoken messages that are presented to patients can be modified to facilitate comprehension, improve confidence, and, ultimately, effect a change in behavior. Thus, literacy-sensitive education materials and communication should focus on simplifying health information by using plain language, simple text, ample white space, and behavior-oriented images. The use of literacy-sensitive materials has been shown to improve comprehension for patients with low and high literacy levels.23,25 However, the majority of health education materials have not been evaluated for suitability of use in low-literacy populations. Moreover, when items have been formally evaluated, many materials have been found to be unsuitable or only marginally suitable.26 -28
Effective patient education relies not only on patients’ understanding of diabetes self-management information but also on whether patients actually integrate treatment recommendations into their daily self-management routine. Patient-provider interactions are most successful when patients are well-informed and actively participate in their care. 29 Health care providers may use shared goal setting with a patient to collaboratively establish priorities for the patient’s self-care routine. Shared goal setting allows for intentional conversations about which behaviors the patient is willing and able to change, creating an opportunity to increase the patient’s confidence to incorporate the behavior changes necessary to reach his or her treatment goals. 30 Shared goal setting also provides a way to document patient education and improve communication among the diverse members of the patient’s health care team to facilitate more efficient and effective patient education. 31 The use of structured goal setting with diabetes patients in a primary care setting has been shown to significantly improve A1C. 30
Development of the PRIDE Toolkit
The Partnership to Improve Diabetes Education (PRIDE) toolkit was developed to be a comprehensive set of diabetes education materials intended to assist English- and Spanish-speaking patients in managing their diabetes. The basis for the PRIDE toolkit was the previously validated Diabetes Literacy and Numeracy Education Toolkit (DLNET), which was developed by the authors’ team in 2007 24 ; the American College of Physicians Foundation’s Living with Diabetes Guide 32 ; and the American Association of Diabetes Educators (AADE) 7 Self Care Behavior Topics. 33 As recommended in the American Diabetes Association (ADA) and AADE National Standards for Diabetes Self-Management Education, the revised materials (1) were adapted for cultural influences, (2) included education about comorbidities, (3) were designed to be interactive, (4) include action-oriented behavioral goals and objectives, (5) address functional health literacy, and (6) address the patient’s ability to afford treatment. 34 The PRIDE toolkit expands on the team’s previous work by adding a focus on shared goal setting for health behavior change, addressing Spanish acculturation, and expanding the number of modules to include additional diabetes-related subjects such as blood pressure, cholesterol, medication adherence, and depression, among others. Additionally, the PRIDE toolkit contains 3 educational modules created by Becton Dickson and Company that the authors found to appropriately address the needs of patients with low literacy and numeracy.
The PRIDE toolkit modules are available at http://www.mc.vanderbilt.edu/root/vumc.php?site=CDTR&doc=37816.
The toolkit content, format, and design were determined by a multidisciplinary team of experts in literacy, numeracy, health behavior, and diabetes, including physicians, registered dietitians, certified diabetes educators, a nurse practitioner certified in advanced diabetes management, and a behavioral psychologist. The principles outlined in the Suitability Assessment of Materials (SAM) by Doak et al 35 (see Table 1), which aid in the development of materials for low-literacy patients, were used to inform the text, layout, and formatting of each module. Following review and revisions of each module by the team, feedback was solicited through cognitive interviews with patients and providers on the usability and appropriateness of the material prior to finalization.
Reading Grade Level and SAM Results for PRIDE Modules a
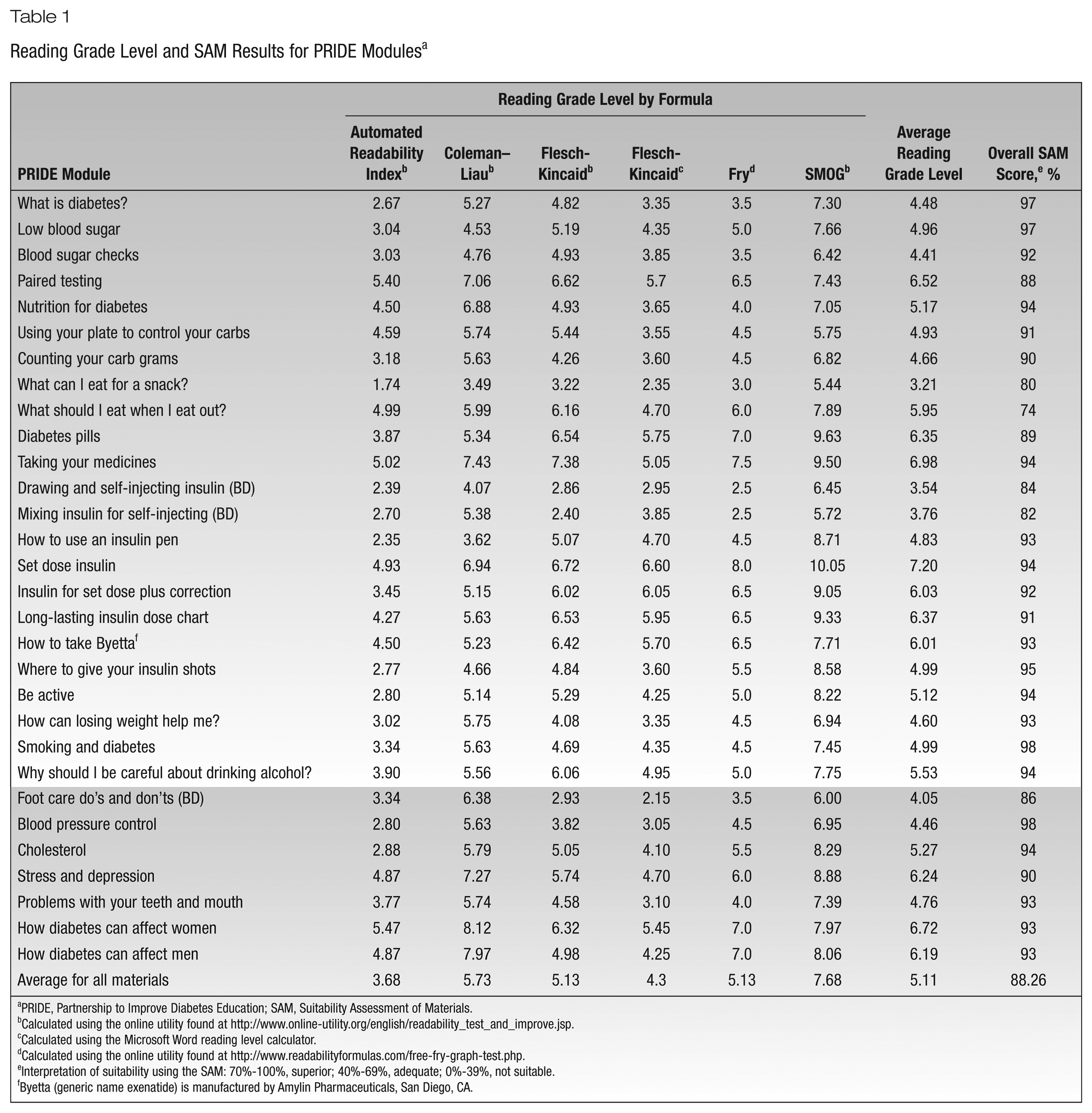
PRIDE, Partnership to Improve Diabetes Education; SAM, Suitability Assessment of Materials.
Calculated using the online utility found at http://www.online-utility.org/english/readability_test_and_improve.jsp.
Calculated using the Microsoft Word reading level calculator.
Calculated using the online utility found at http://www.readabilityformulas.com/free-fry-graph-test.php.
Interpretation of suitability using the SAM: 70%-100%, superior; 40%-69%, adequate; 0%-39%, not suitable.
Byetta (generic name exenatide) is manufactured by Amylin Pharmaceuticals, San Diego, CA.
The PRIDE modules were created as part of a cluster randomized controlled trial in which study participants are patients with type 2 diabetes who receive care in underresourced communities. Thus, 6 of the original DLNET modules that addressed topics more relevant to patients with type 1 diabetes or those treated with intensive insulin therapy were omitted. The remaining 18 original handouts were revised, and new topics covering oral health, diabetes in women, diabetes in men, stress and depression, alcohol consumption, blood pressure, cholesterol, medication adherence, self-injecting insulin, smoking cessation, weight loss, and paired testing were added for a total collection of 30 modules.
The PRIDE modules are designed to be used interactively between a health professional and a patient. Each module begins with a title page. Often the title is in the form of a question to engage learners (Figure 1). For example, the blood pressure module is titled “Why should I care about blood pressure?” The next portion of the module gives a brief description of the problem and why the information is important, followed by the specific behaviors that will help manage the problem (Figures 2 and 3). The last page of each module is used for shared goal setting (Figure 4). This page contains 1 or 2 blank lines that can be used to write in a goal of the patient’s choice followed by a list of behavioral goals appropriate for the topic addressed in the module.
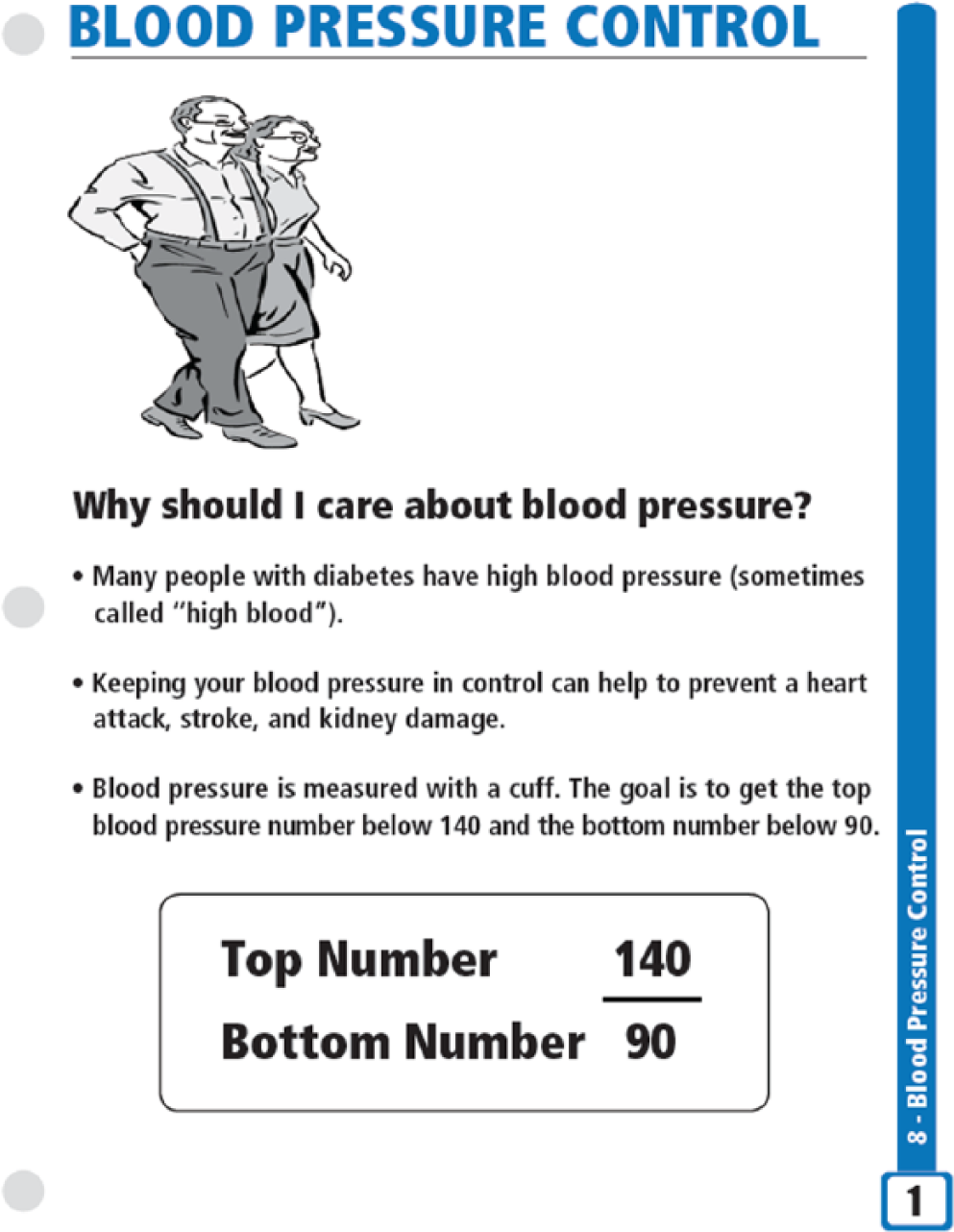
Example of the title page and description of the problem.
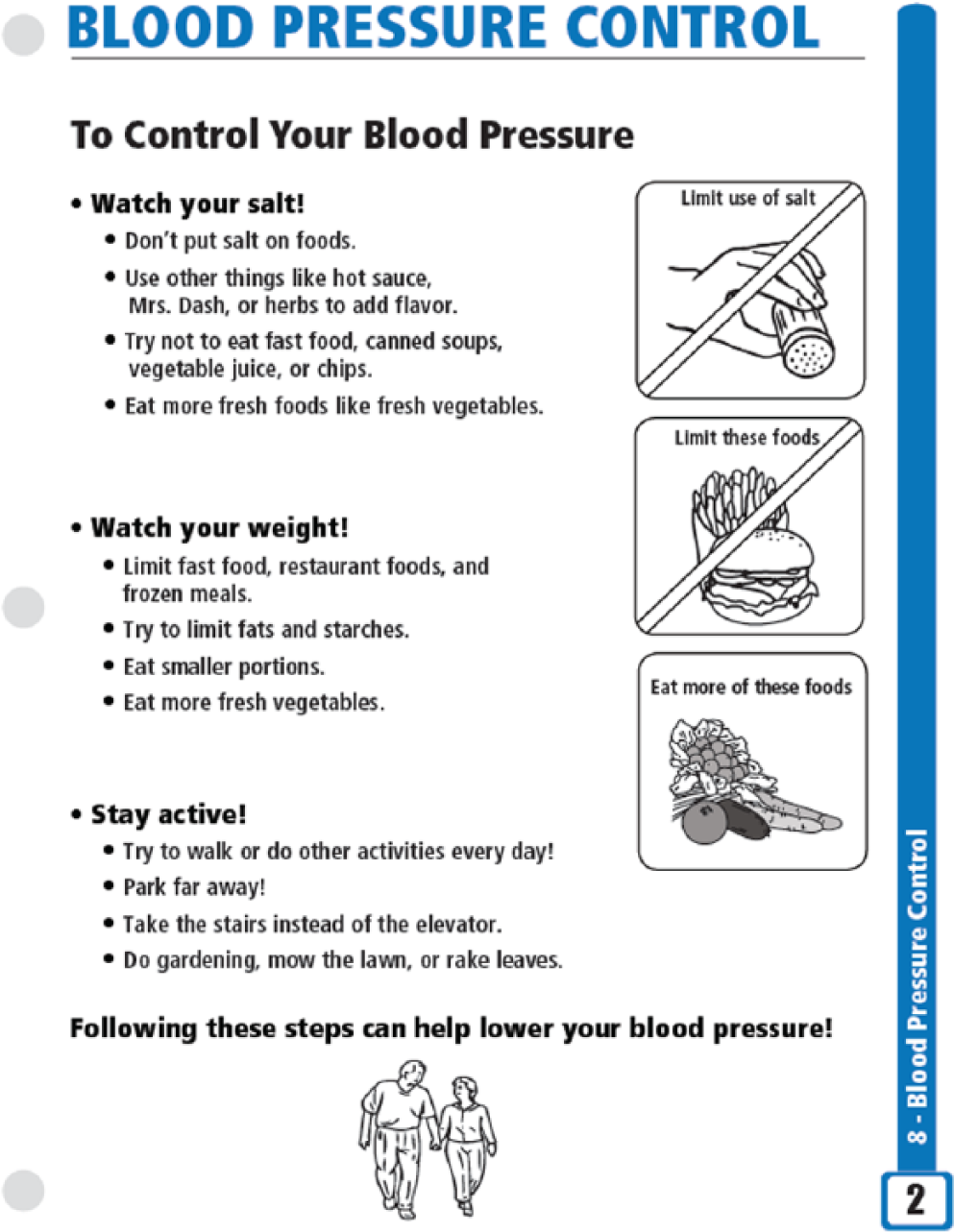
Example of behaviors to help manage the problem.
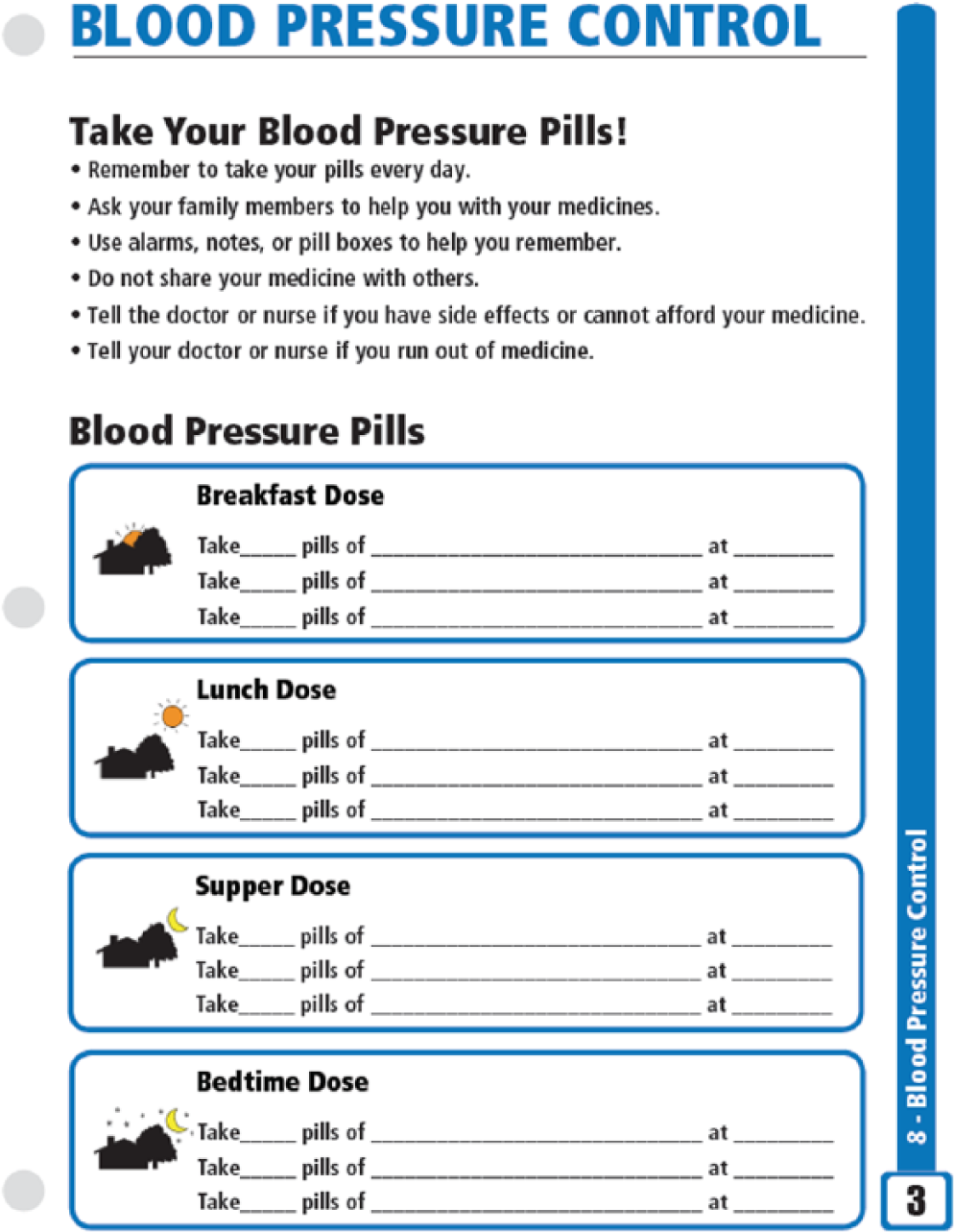
Example of how to implement behavior changes.
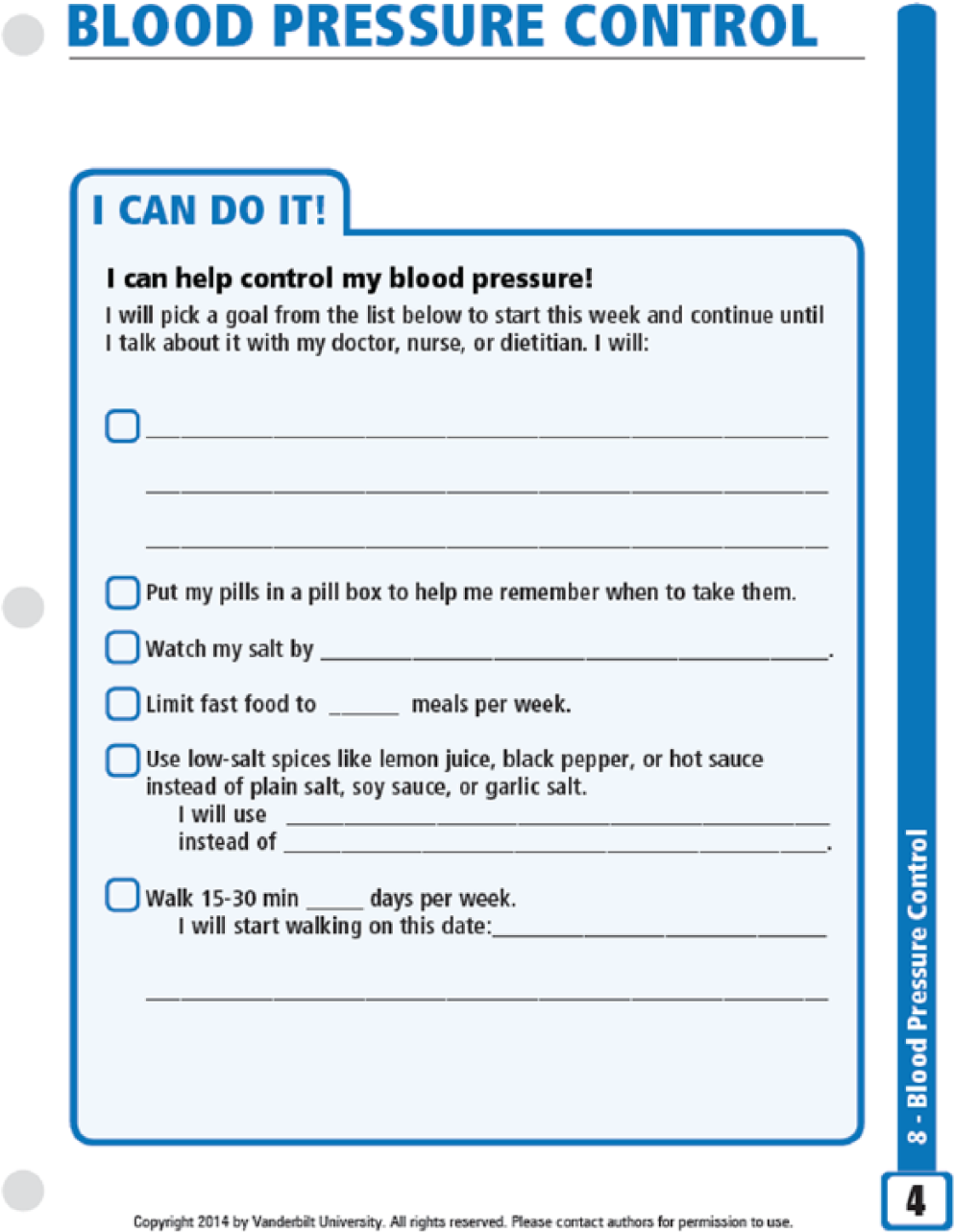
Example of shared goal setting.
The modules were grouped into 12 categories: general information about diabetes, blood glucose monitoring, nutrition information, oral diabetes medication, insulin and exenatide (these modules were originally created for use with public health department patients for whom the only glucagon-like peptide-1 (GLP-1) agonist covered on formulary was exenatide), lifestyle management and behavior change, foot care, cardiovascular risk factors, coping with stress and depression, oral health, women’s health, and men’s health.
As suggested by the Institute of Medicine and in other literature, 36 it is vital for literacy-based interventions to reduce health information complexity. This was accomplished in the PRIDE toolkit by using plain language to convey key messages, keeping all text simple, incorporating the maximum amount of white space, and including behavior-oriented images and pictograms. Simple line drawings were used for visual images. To further address low literacy and numeracy, the team used color coding including traffic light images, accurately sized plates that outline recommended portion sizes, worksheets on food label interpretation, pictures of medications, and specific graphics to enhance accurate timing of medications and medication adherence.
Each module incorporates components specifically intended to enhance effective patient-provider communication and interaction. The modules are each organized in a way that assists the provider in covering the material in a systematic and logical manner. The content itself can act as a cue and reminder to providers of specific treatment goals. Through the Vanderbilt Center for Diabetes Translational Research, the content of the PRIDE toolkit will be reviewed and updated indefinitely, for as long as the toolkit is in use. In addition, the materials address important socioeconomic and community-level barriers that can impede diabetes self-management. For instance, the medication adherence module addresses medication affordability, difficulty with prescriptions, and common beliefs that hinder medication adherence. 37 Finally, the page on shared goal setting invites and supports active patient-provider dialogue and negotiation.
The additional education modules on common diabetes comorbidities were developed for the PRIDE toolkit to address the risk for morbidity and mortality contributed by factors such as stress, high blood pressure, and high cholesterol. This is particularly important because cardiovascular diseases (CVDs) are the primary cause of mortality for people with diabetes. 38 Moreover, women with diabetes are 3 times more likely to develop CVDs than women without diabetes, and men with diabetes are twice as likely to develop CVDs than men without. 39 Thus, it is important to educate diabetes patients on the risks of these comorbid conditions and on how to prevent or manage the conditions through daily self-care routines.
Development of the Spanish PRIDE modules was an iterative process that solicited input from experts in health literacy, acculturation, and psychosocial factors relevant to the care of Hispanic/Latino patients with diabetes. Prior quantitative and qualitative work with our local Hispanic/Latino population revealed many barriers to adequate diabetes control, including limitations of health literacy and numeracy skills. We translated dietary content with special attention to choosing food products most likely to have shared relevance across Hispanic/Latino subgroups. As with the English version, these modules were refined using feedback from cognitive interviews with Spanish-speaking diabetes patients (Figure 5) to ensure that content was both linguistically and culturally relevant.
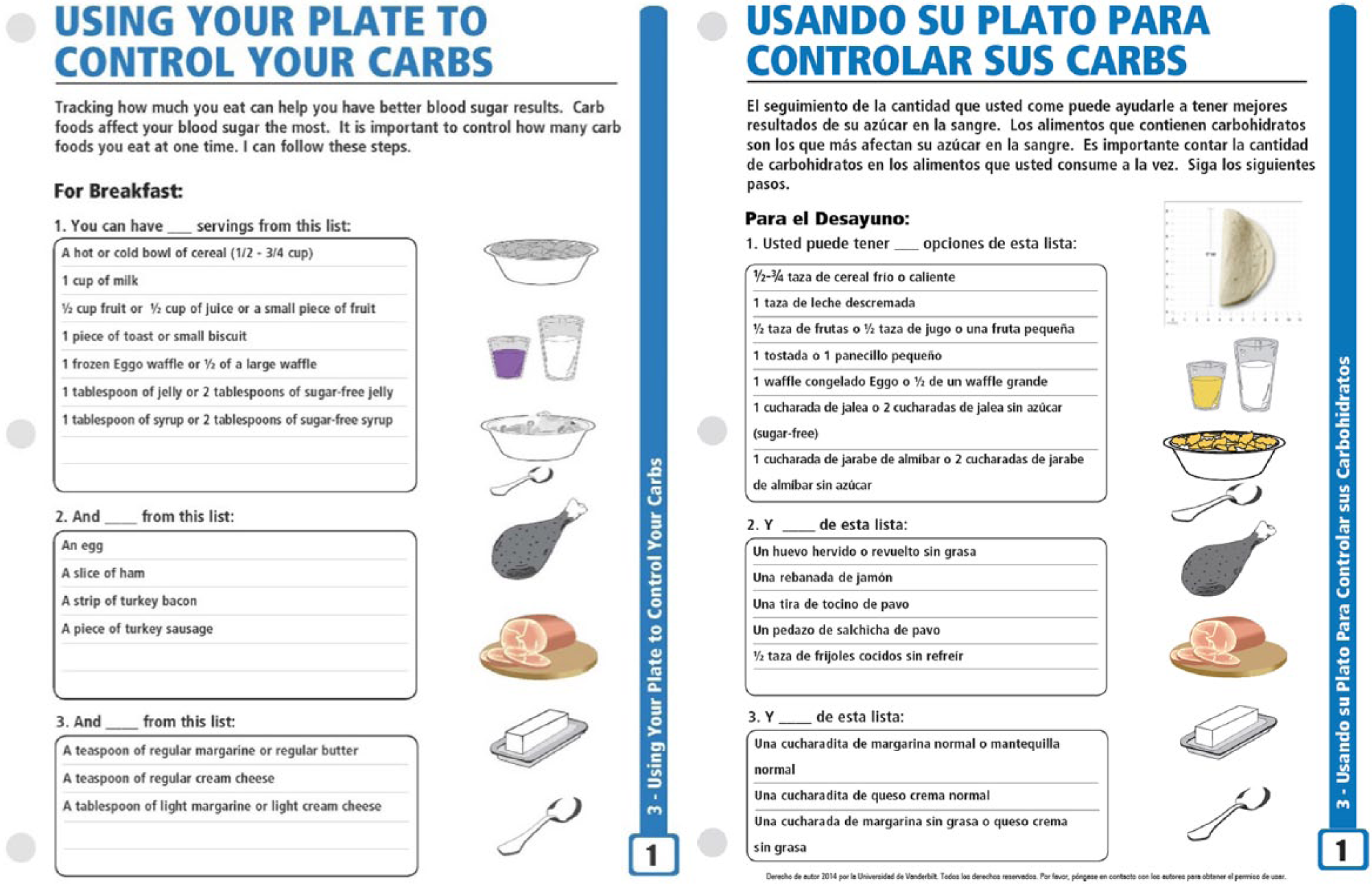
Example of Spanish acculturation.
Evaluation of the PRIDE Toolkit
The 30 PRIDE toolkit modules were each evaluated using the SAM instrument. The SAM was developed by Doak et al 35 in 1993 and aids in determining the deficiencies of educational materials that may reduce their appropriateness for low-literacy patients. 35 Since its development, the SAM has been used by numerous other authors to evaluate different patient education materials,26,28 For the SAM, raters score each material separately in 22 items divided into 6 categories. These categories include content, graphics, layout and typography, learning stimulation and motivation, and cultural appropriateness (see Table 1). 35 Materials are scored 0, 1, or 2 points (not suitable, adequate, and superior, respectively) for each item for a total possible score of 44. The total point score calculated as a percentage determines whether, overall, the material is superior (70%-100%), adequate (40%-69%), or not suitable (0%-39%).
Each English and Spanish module of the PRIDE toolkit was evaluated using the SAM by 2 independent raters.
To evaluate the reading grade level of each module, 2 online instruments40,41 and Microsoft Word’s reading level calculator were used to determine the Flesch-Kincaid, Coleman-Liau, SMOG, Fry, and Automated Readability Index (ARI) reading grade levels. The online instruments require the text to be in a very specific format; thus, a plain text document was created with no special formatting or graphics. Most bulleted and numbered lists were removed and converted into sentences with as few adjustments as possible to the text in order to most accurately reflect the bulleted lists. Lists of individual words were not considered in the analysis. All text from graphics, tables, and diagrams was removed. The resulting plain text document was analyzed using the 2 online instruments and Microsoft Word. As recommended by Doak et al, 35 the reading grade level calculated with the Fry formula was used to calculate the SAM score. Mean reading levels and standard deviations were calculated for all modules, and analyses were performed using Stata 10.1 (College Station, Texas).
Results of the Suitability Assessment of Materials and Readability Evaluation
The mean SAM score for all modules of the PRIDE toolkit is 91% (SD 5.45; range, 74%-98%), and the mean readability level is 5.3 (SD 1.03; range, 3.2-7.2). Overall, the lowest SAM score received by any of the 30 individual modules was 73% (32/44 points). All 30 modules received a superior overall rating from both raters before averaging. The average SAM score, reading grade level by formula, and average of all reading grade level results for each module are presented in Table 2. For 26 of 30 modules, the total SAM scores by the independent raters were within 1 point of one another (of 44 total points). For 2 modules, the raters’ scores differed by 2 points; and for 2 modules, the raters’ scores differed by 4 points.
Suitability Assessment of Materials (SAM) Categories
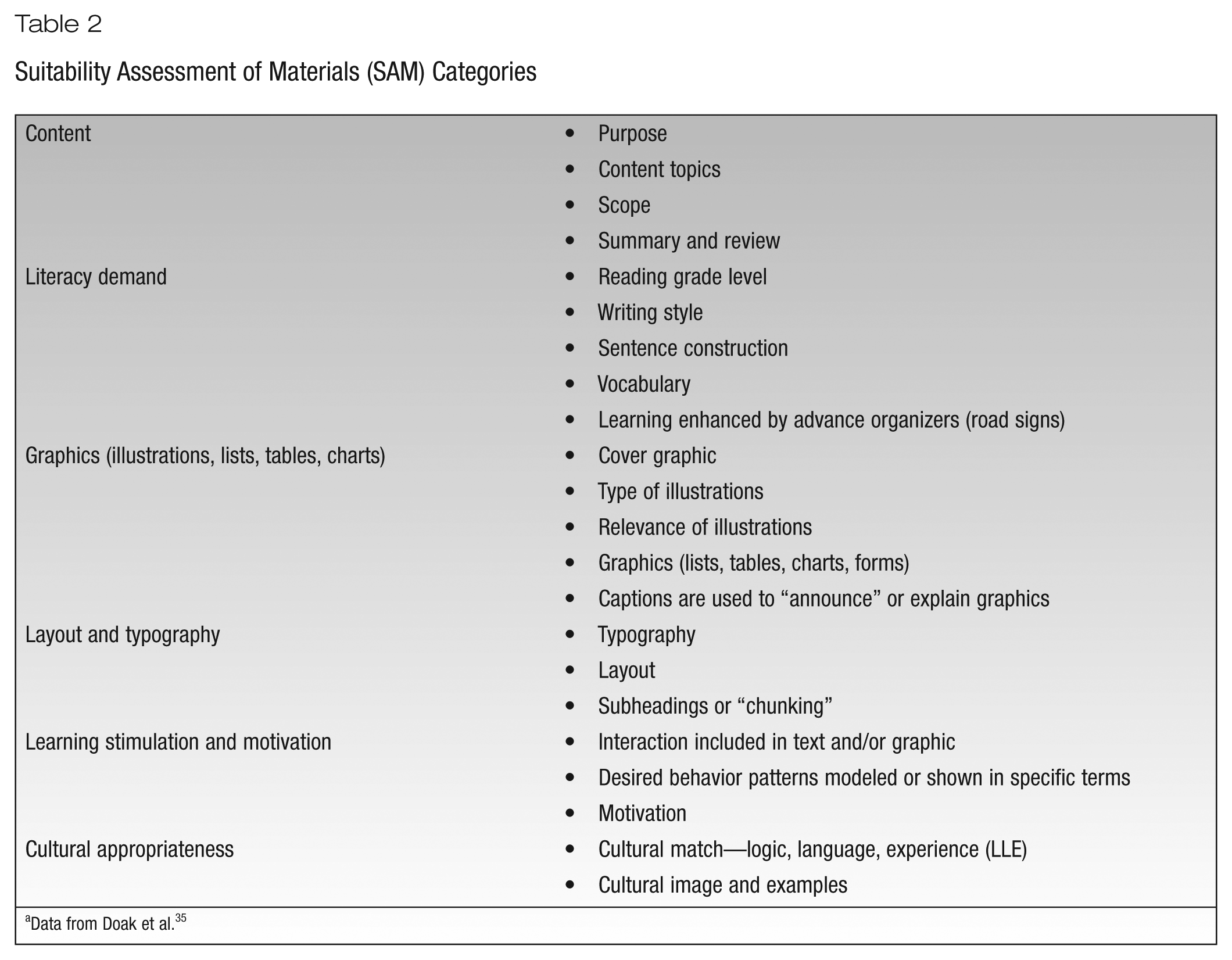
Data from Doak et al. 35
The average reading grade level for all 30 PRIDE modules was lowest (3.7) when calculated with the ARI formula and highest (7.7) when calculated with the SMOG formula. The module What Can I Eat for a Snack received the lowest average reading grade level (3.2). In contrast, the module Set Dose Insulin received the highest average reading grade level (7.2).
In the content category of the SAM, all 30 modules scored very well. Points were deducted from some modules for minimal or missing summaries. In the literacy demand category, all modules received a superior score for both writing style and vocabulary. When the Fry method was used to obtain the reading grade level, all modules scored at or below an eighth-grade level, and more than half (19 modules) scored at or below a fifth-grade level (superior rating). None of the modules received a nonsuitable rating (ninth grade or above).
In the graphics category, 28 of 30 modules scored well. Points were most commonly deducted for the cover graphics. Both the What Can I Eat for a Snack? and the What Should I Eat When I Eat Out? modules scored poorly in the graphics category because they contained only charts and tables and no other graphics or pictures. In the layout and typography category, 29 of 30 modules received a superior score for both the layout and typography. Several modules lost points for having longer lists without subheadings.
In the learning stimulation and motivation category, 27 of 30 modules received a superior score throughout. Each of the 3 BD low-literacy modules that were incorporated into the PRIDE toolkit had some points deducted from the interaction and motivation subcategories.
Finally, in the cultural appropriateness category, 27 of 30 modules received a superior rating. Three modules (Counting Your Carb Grams, What Should I Eat When I Eat Out?, and Problems With Your Teeth and Mouth) had points deducted because the raters noted opportunities to further adapt the Spanish version of the materials.
Discussion
The PRIDE toolkit was designed to assist both diabetes patients and diabetes providers by improving patient education, patient-provider communication, and sensitivity to the needs of English- or Spanish-speaking patients. Additionally, the modules specifically address important socioeconomic and psychosocial barriers to optimal diabetes management, such as medication adherence, which are more likely to affect patients with low literacy and numeracy. 42 Toolkit topics are addressed in individual modules, which allows for a customized, patient-centered approach to diabetes education while providing a consistent format across the comprehensive span of materials.
The cultural backgrounds and experiences of English- and Spanish-speaking patients are significantly diverse. Thus, providers must remain sensitive to each patient’s unique background when using the toolkit modules. The shared goal setting portion of each toolkit module provides an opportunity for providers to further tailor patient education to the patient’s specific priorities and concerns. Intentional discussions with patients to set collaborative goals can help to identify barriers to behavior change and effective self-management of diabetes while improving the patient’s self-efficacy for behavior change.
The ultimate determination of the effectiveness and utility of these low literacy and culturally sensitive materials must be based on rigorous testing. The PRIDE toolkit is currently being tested in a cluster randomized controlled trial of an intervention intended to improve diabetes care for a multiethnic population receiving care in underresourced communities.
Clinical Applications
The PRIDE toolkit modules are designed to be used by various members of a multidisciplinary diabetes care team in a primary care or diabetes specialty setting. The layout of the modules can prompt providers to address important but potentially overlooked aspects of diabetes education. Module layout can also assist clinicians in clear communication by providing a logical sequence for teaching about specific topics. Each module’s focus on shared goal setting can help facilitate clear and effective patient-provider communication, which can ultimately enhance behavior change and improve clinical outcomes.
The PRIDE modules encourage a comprehensive approach to diabetes education by addressing AADE- and ADA-recommended diabetes topics as well as common diabetes comorbidities such as hypertension and dyslipidemia.33,43 English and Spanish materials can be used side by side to facilitate communication with Spanish-speaking patients in language-discordant settings. Last, although developed with specific sensitivity for diabetes patients with low literacy and numeracy, education materials with improved readability and cultural sensitivity can be appreciated by most patients regardless of their education and socioeconomic status.
Conclusion
The PRIDE toolkit contains 30 low-literacy and low-numeracy diabetes education modules. Content was based on the AADE 7 Self Care Behavior Topics and ADA/AADE National Standards for Diabetes Self-Management Education. The content and formatting of each module is literacy-sensitive, and all modules were translated into Spanish and culturally adapted for Hispanic/Latino patients with diabetes. The PRIDE toolkit builds on the DLNET tools by adding an emphasis on shared goal setting, addressing the needs of Spanish-speaking patients, and including information on a more comprehensive set of diabetes-related topics.
A limitation of this study is the fact that no SAM assessment was done on the Spanish version of the toolkit materials. However, we would anticipate that the SAM results would be very similar since the layout and content of both sets of materials are the same.
The SAM was used to evaluate each module’s suitability for individuals with low literacy as well as its cultural appropriateness. The toolkit materials’ superior SAM ratings and the low reading grade levels indicate that the PRIDE modules are sensitive to the needs of English- or Spanish-speaking diabetes patients with low literacy and numeracy skills.
Footnotes
Acknowledgements
The PRIDE Study Team: Kenneth A. Wallston, PhD, School of Nursing, Vanderbilt University, Nashville, TN; Shari Barto, MBA, CCRP, Institute for Medicine and Public Health, Vanderbilt University, Nashville, TN; Rosette J. Chakkalakal, MD, MHS, Division of General Internal Medicine and Public Health, Department of Medicine, Vanderbilt University, Nashville, TN; David G. Schlundt, PhD, Department of Psychology, Vanderbilt University, Nashville, TN; Sunil Kripalani, MD, MSc, Division of General Internal Medicine and Public Health, Department of Medicine, Vanderbilt University, Nashville, TN; and Anne Sizemore, MA, CMI, Institute for Medicine and Public Health, Vanderbilt University, Nashville, TN.
Funding:
This research study, The Public-Private Partnership Addressing Literacy-Numeracy to Improve Diabetes Care, is funded by a grant (5R18 DK083264) from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) of the National Institutes of Health (NIH).