
Abstract
Purpose
The purpose of the study was to identify the sex-specific characteristics that predict depression among adult women with diabetes.
Methods
Data from the 2007-2012 National Health and Nutrition Examination Survey in the United States were used to identify the predictors of depression in a large sample of women ages 20 years and older with diabetes (n = 946).
Results
When extrapolated to almost 9 million women in the United States ≥ 20 years of age with diabetes, 19.0% had depression. Female-specific significant predictors of depression included younger age (< 65 years old), less than high school graduation, self-rated fair or poor health, inactivity due to poor health, and pain that interferes with usual activities. Marital status and diabetes-related factors (years living with diabetes, use of insulin, parent or sibling with diabetes) were not significant predictors of depression in adult women with diabetes.
Conclusion
When educating and counseling women with diabetes, diabetes educators should be aware that some of the predictors of depression in women with diabetes differ from those of populations that include both sexes. Depression screening, although important for all women with diabetes, should especially be performed among women with female-specific depression predictors.
Introduction
The prevalence of depression in patients with diabetes has been found to range from 8% to more than 30% and is as much as 3 times greater than in populations without diabetes.1-7 With such a high prevalence, diabetes and depression comorbidity has become an important focus of research and clinical care, with the Dialogue on Diabetes and Depression established in 2007 to support relevant international research and innovations to address it. 8 Of special concern is that depression in people with diabetes has been associated with greater use of health care and higher health care costs,9-12 poorer self-care, less medication compliance and dietary adherence, worse glycemic control, a greater diabetes symptom burden, poorer quality of life, and premature mortality.9,13-23
It is unfortunate that, despite the availability of effective treatment for this comorbidity24,25 and its value in improving diabetes outcomes,26-29 depression is often unidentified and untreated in adults with diabetes.30-32 Recognizing this, regular screening for depression in people with diabetes has therefore been recommended by several professional associations, including the International Diabetes Federation, 33 the American Diabetes Association, 34 and the UK National Institute for Health and Clinical Excellence. 35 Most recent, the US Prevention Standard Task Force recommended regular depression screening in the general adult population, 36 with the understanding that this screening would be implemented with adequate systems in place to ensure accurate diagnosis, effective treatment, and appropriate follow-up. Whereas depression screening is important for all adults, it is particularly essential in persons with diabetes in view of the high prevalence and adverse consequences of diabetes and depression comorbidity. In addition, identifying the characteristics of adults with diabetes who are especially vulnerable for depression has the potential to ensure that persons possessing these attributes are screened and receive much-needed depression treatment.
Research conducted with samples involving both men and women with diabetes in the United States and elsewhere has, in fact, identified various predictors of depression. Among them are sociodemographics, including age, education level, marital status, and race/ethnicity10,37-43; diabetes-related factors, including a family history of diabetes, years since a diabetes diagnosis, and the use of insulin39,41-44; self-perceived physical health 39 ; body mass index7,37,41,43; smoking status38,39,41; pain 7 ; and mobility, functional impairment, and physical inactivity.7,37,40,45-48 In addition, it is notable that almost all of these studies have concluded that among persons with diabetes, depression is significantly more common in women than in men.2,7,10,37,39,41,42,44,48-50 However, the extent to which the predictors of comorbid depression in studies involving both sexes are the same as those found specifically among women has not been adequately explored.
Although there are some studies that have examined the predictors of depression in women with diabetes, these studies have a number of limitations. In 1 such study, the relationship between depressive symptoms and waist-to-hip ratio, dyslipidemia, glycemic levels, and blood pressure was examined among Chinese women at least 40 years of age with diabetes, and no significant trend between depressive symptoms and these potential predictors was found. 51 Although informative, a variety of potentially important demographic and other predictors were not considered in this analysis, nor did the sample include women younger than 40 years. In another large study involving female nurses ages 50 or older, the relative risk of incident clinical depression was examined, comparing women with and without incident diabetes over the 10-year period from 1996 to 2006. 52 When taking into account various demographic and other covariates, results indicated a significant relative risk of developing clinical depression in women with diabetes in an age-adjusted model. However, the salience of these demographic and other covariates in explaining the incidence of clinical depression was not reported. In addition, as the sample consisted of registered nurses who were 94% white and between 50 and 75 years of age, results may not be generalizable to other populations of adult women with diabetes. Other studies of women with diabetes that have focused on the predictors of comorbid depression have been conducted, but they typically involve small samples in diverse cultures and geographic regions, with results that may be specific to women in the regions sampled.53-55
In this article, an examination was conducted to determine the sex-specific characteristics that predict depression among adult women with diabetes. The examination was made using data collected from a large sample (n = 946) of women in the United States from 2007 to 2012, ages 20 years and older, and of various races/ethnicities. Results are extrapolated to the population of women in the United States with diabetes who are at least 20 years of age. The primary research question was whether the salient predictors of depression found in large studies involving both men and women with diabetes are the same or different when considering women alone.
Methods
National Health and Nutrition Examination Survey
Data for the current study were collected in the National Health and Nutrition Examination Survey (NHANES) 2007-2012 conducted by the National Center for Health Statistics, Centers for Disease Control and Prevention in the United States. Involving questionnaires, interviews, direct examinations, and laboratory assessments, the NHANES uses a complex, multistage, probability sampling design to select participants. Sampling weights for each participant are provided that reflect the unequal probability of participant selection, nonresponse adjustment, and adjustment to independent population controls. This enables the reporting of results that assess the health status of civilian, noninstitutionalized adults and children in the United States. The NHANES also provides sample design variables so that unbiased parameter estimates can be obtained and so that significance levels are not overstated when performing analyses. A full description of the design of the NHANES is available on the NHANES website: http://www.cdc.gov/nchs/data/nhanes.
Measures
Diabetes
NHANES 2007-2008, 2009-2010, and 2011-2012 datasets comprised a total sample of 9057 women, 20 years of age or older. The women were classified as having diabetes if they answered “yes” to the question, “Other than during pregnancy, have you ever been told by a doctor or health professional that you have diabetes or sugar diabetes?” A total of 1094 of the 9057 women 20 years of age or older indicated that they had diabetes.
Depression
The NHANES also assessed depression using the evidence-based, 9-item Primary Care Evaluation of Mental Disorders Patient Health Questionnaire (PHQ-9), administered in English or Spanish to NHANES participants ≥ 12 years of age by trained interviewers. Scoring each of the 9 DSM-IV (and updated DSM-5) criteria for major depressive disorder as 0 (not at all) to 3 (nearly every day),56,57 the PHQ-9 has demonstrated excellent reliability and validity in various clinic settings, in general populations, and among diverse ethnic groups.58-64 A score of 10 or more on the PHQ-9 is generally considered clinically significant depression that warrants treatment. 65 Thus, consistent with the NHANES and DSM-IV and DSM-5, adult women with PHQ-9 scores < 10 were categorized as not depressed, and those with scores of 10 or higher as clinically depressed. 66 A total of 946 of the 1094 women ages 20 years or older with diabetes in the NHANES 2007-2012 datasets had PHQ-9 scores that enabled this categorization. These 946 women constitute the study sample.
Potential Depression Predictors
Factors previously identified as significant predictors of depression in samples involving both men and women with diabetes were examined. These included sociodemographics: age group (categorized as 20-44, 45-64, or at least 65 years); education level (dichotomized as less than high school graduation or at least a high school graduate); marital status (dichotomized as currently married or living with a partner or not currently married or living with a partner); and race/ethnicity (categorized as Hispanic, non-Hispanic white, non-Hispanic black, or other [including mixed race]). Potential predictors of depression also included diabetes-related factors: having a parent or sibling with diabetes (no or yes), years living with diabetes (categorized as < 5, at least 5 but < 10, or at least 10 years), and current use of insulin (no or yes). Additional potential predictors of depression included self-perceived physical health (dichotomized as poor or fair vs good, very good, or excellent); body mass index (BMI; categorized as < 25, at least 25 but < 30, or at least 30 kg/m2); smoking status (categorized as never smoked, a former smoker, or a current smoker); frequency with which having pain makes it hard to perform usual activities (categorized as no days, some days, or all days); and mobility, functional disability, and activity, including frequency of inactivity due to poor health (categorized as no days, some days, or all days), and physical activity. This latter factor was conceptualized based on the number of hours that participants reported spending each week on moderate and vigorous activity, with the total hours of metabolic tasks per week (MET hours/week) involving this activity estimated using the MET score assigned by the NHANES.67,68 Participants were categorized as physically active if they had at least 9 MET hours/week and inactive otherwise.
Statistical Methods
Analyses, performed using complex survey sampling software from IBM PASW 21, followed the analytic guidelines provided by the NHANES. 69 In addition to reporting descriptive statistics (ie, proportions), the predictors of depression in adult women with diabetes were examined by using the complex samples logistic regression procedure for a binary dependent variable (ie, clinically depressed = 1 or not = 0).
First, bivariate logistic regression analyses were conducted to determine the independent relationships of each of the potential predictors of depression, together with their odds ratios (ORs), confidence intervals (CIs), and statistical significance. In the case of a potential categorical predictor with k ≥ 3 categories, k – 1 dummy variables were created, with 1 level of the potential predictor designated as the reference category. Because all potential predictors with P < .10 were then to be entered into a multivariate complex samples logistic regression model, 90% CIs are provided for the unadjusted analyses. For categorical variables with k ≥ 3 categories, if any of the dummy variables was significant at the P < .10 level in the unadjusted analyses, all dummy variables for the potential predictor were entered in the multivariate model. Potential predictors were subsequently examined and eliminated according to their least significant contribution in explaining the logarithm of the odds of having depression until only statistically significant predictors remained (ie, P < .05). Adjusted ORs, 95% CIs, and significance levels are provided for this final multivariate model.
Human subjects considerations
As the NHANES is among the sources of public use data approved by the University Committee on Activities Involving Human Subjects at New York University, New York University investigators are able to use the database without review and approval by that committee.
Results
Prevalence of Depression
In all, among the 946 women in the study sample who represented 8 966 922 civilian, noninstitutionalized women in the United States ≥ 20 years of age with diabetes from 2007 to 2012, 19.0% had depression.
Characteristics of Women ≥ 20 Years Old With Diabetes
As can be seen in the first column of Table 1, when accounting for the sampling weights provided by the NHANES, the great majority of the women represented by the sample (87.4%) were either between 45 and 64 years or at least 65 years. Two thirds were high school graduates, and half were married or living with a partner at the time of data collection. Participants represented women of diverse races/ethnicities: 58.4% were non-Hispanic white, whereas 20.0% was non-Hispanic black, 13.5% were Hispanic, and 8.1% were of other races and ethnicities, including of mixed race. With regard to diabetes-related factors, one fourth were taking insulin at the time of data collection, two thirds had a first degree relative (parent or sibling) with diabetes, and most had diabetes for at least 10 years or for < 5 years (43.8% and 36.8%, respectively). The great majority (88.6%) was obese or overweight, with only about one third physically active, engaging in moderate or vigorous activity for at least 9 hours per week. Only a small proportion were current smokers, with more than half indicating that they never smoked and more than one quarter indicating that they had smoked in the past. Many had issues with pain and impaired mobility and function. About half indicated that pain interfered with their usual activities on some days or every day. In all, about half rated their health as fair or poor, and about a third indicated that they were inactive on some days or every day due to poor health.
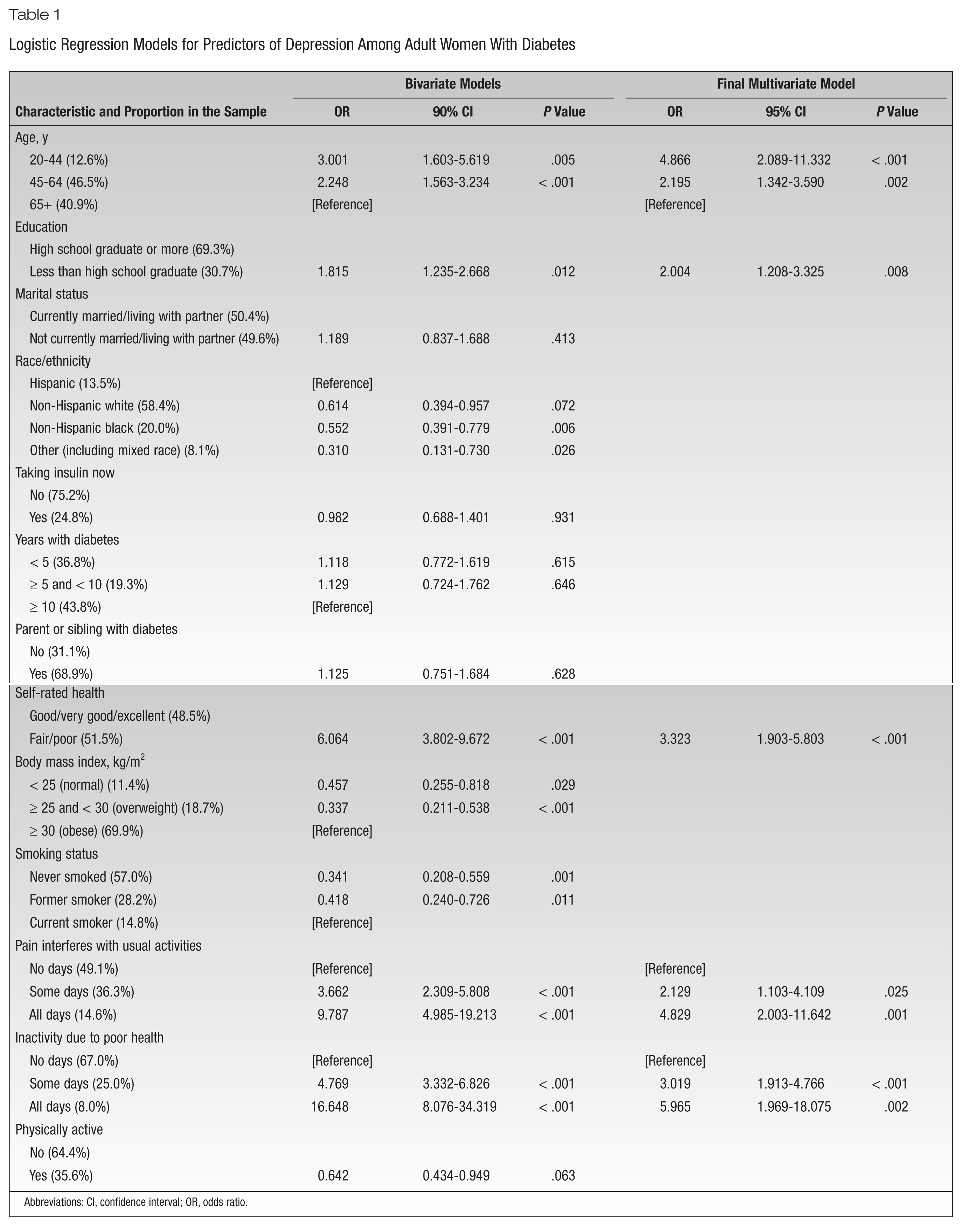
Logistic Regression Models for Predictors of Depression Among Adult Women With Diabetes
Abbreviations: CI, confidence interval; OR, odds ratio.
Bivariate Logistic Regression Results
Bivariate logistic regression analyses identified sex-specific predictors of depression in women with diabetes with P < .10 from among those considered (Table 1). These included younger age (ie, 20-44 years and 45-64 years compared with 65 years or older); less than a high school graduate; Hispanic as compared with non-Hispanic white, non-Hispanic black, and other race/ethnicity, including mixed race; fair or poor self-rated health; BMI in the obese range as compared with BMI in the normal and overweight ranges; being a current smoker as compared with having never smoked or being a former smoker; having pain interfere with usual activities on some days or every day as compared with no days; inactivity due to poor health on some days or every day as compared with no days; and being physically inactive.
Multivariate Logistic Regression Results
All of the potential predictors with P values < .10 identified in the bivariate logistic regression analyses were entered into a multivariate logistic regression model. Having sequentially eliminated all nonstatistically significant potential predictors, those whose P values were .05 or less were retained. As can be seen in Table 1, the following were found to be sex-specific statistically significant predictors of clinical depression in women with diabetes at least 20 years of age, over and above other predictors, together with their ORs, 95% CIs, and P values: 20-44 years of age compared with 65 years or older (OR = 4.866; 95% CI, 2.089-11.332; P < .001); 45-64 years of age compared with 65 years or older (OR = 2.195; 95% CI, 1.342-3.590; P = .002); less than a high school graduate (OR = 2.004; 95% CI, 1.208-3.325; P = .008); rating their health as fair or poor (OR = 3.323; 95% CI, 1.903-5.803; P < .001); having pain interfere with usual activities on some days as compared with no days (OR = 2.129; 95% CI, 1.103-4.109; P = .025); having pain interfere with usual activities every day as compared with no days (OR = 4.829; 95% CI, 2.003-11.642; P = .001); inactivity due to poor health on some days as compared with no days (OR = 3.019; 95% CI, 1.913-4.766; P < .001); and inactivity due to poor health every day as compared with no days (OR = 5.965; 95% CI, 1.969-18.075; P = .002). Race/ethnicity, BMI, smoking status, and physical activity were no longer salient predictors in the multivariate model.
Discussion
Findings indicate that 19% of women ages 20 and older in the United States with diabetes have comorbid depression. This proportion is in concordance with that found in other studies with large samples, such as the 20.9% found in the Translating Research into Action for Diabetes (TRIAD) study that included 4659 women with diabetes who were enrolled in 10 managed care health plans in 7 states. 7
Consistent with research conducted among both male and female adults with diabetes, findings indicate that younger age, less education, self-rated poor health, and pain and physical and functional impairment are significant predictors of depression among adult women with diabetes.7,10,37-42,44-46 Although research involving both adult men and women with diabetes has identified the importance of marital status and various diabetes-related factors (eg, taking insulin, having a family history of diabetes, years living with diabetes) in predicting comorbid depression,10,39,41,43,44 this was not the case when considering women alone, even in the bivariate analyses. However, the bivariate analyses did identify some additional predictors of comorbid depression that had been found in studies with both men and women with diabetes that were not retained in the multivariate model. These predictors included race/ethnicity, high BMI, smoking, and physical inactivity.7,37,39-43,47 The fact that they were not retained in the multivariate model, together with the lack of statistical significance of marital status and diabetes-related factors, highlights important differences in sex-specific predictors in women with comorbid diabetes and depression as compared with predictors in mixed-sex studies.
Coupled with limited education that may reduce healthy behaviors and health-seeking activities in people with diabetes, 70 syndemics theory calls attention to conditions that may exacerbate comorbid diabetes and depression in vulnerable individuals. 71 This theory may help to explain the clustering of conditions that synergistically contribute to depression in adult women with diabetes. In particular, syndemics theory suggests that the physiological interactions of inflammatory health conditions (such as diabetes, together with those that cause pain and functional disability), compounded by the psychological burden of managing diabetes, create specific risk for clinical depression in women. Less education and self-rated poor health may intensify a sense of despair or powerlessness that reduces the prospect for healthy behaviors and lifestyle changes needed for diabetes management, 72 worsening both diabetes and depression symptom burden.
Various limitations regarding this study are acknowledged. Many of the variables are measured on the basis of self-report, with the attendant possibility of misclassification on its basis. This includes the use of self-report to identify women with diabetes. Because analyses were intended to focus on women who were aware of and acknowledged having diabetes, the choice was made to use self-report as a measure of their positive diabetes status. In addition, as providers did not perform clinical assessment for depression in the NHANES, depression was assessed with the PHQ-9 instrument, a reliable and valid tool. It is also acknowledged that analyses did not include all of the potential predictors for depression that have been shown to be significant in other studies involving diabetes–depression comorbidity. In large part, this was due to its lack of measurement in the NHANES (eg, type of diabetes) or its measurement in only a subset of NHANES participants (eg, diet). It should also be noted that the particular variables considered in the research involving potential predictors of comorbid depression among adults with diabetes have varied considerably. As our study did not consider all such potential predictors, the significant factors found in our multivariate logistic regression need to be examined within the context of the predictors considered. One potential predictor, considered in a study by Katon and colleagues 41 but not in the current study, concerns the presence of 3 or more of 7 complications of diabetes (retinopathy, nephropathy, neuropathy, cerebrovascular, cardiovascular, peripheral vascular, and metabolic). In Katon and colleagues’ study, 41 which involved both men and women with diabetes, the association between diabetes complications and depression was statistically significant for men but not for women. Although other literature involving the predictors of depression among men and women with diabetes has not reported the consideration of other interactions of sex and other potential depression predictors, Katon and colleagues’ findings indicate that such interactions are possible and perhaps even likely. This has bearing on the decision to limit the sample in the current study to adult women with diabetes, rather than to include both sexes with diabetes. In particular, the presence of several sex and other potential depression predictor interactions in a sample involving both men and women may not have substantially increased statistical power. With the analyses focusing on determining the predictors of depression among women with diabetes, the study sample involved 6 years of NHANES data that included 946 women with diabetes, thereby providing sufficient statistical power for the analyses. Finally, acknowledgment is made of a limitation in the assessment of the age of participants. All those who were more than 79 years of age were recorded in the NHANES as 80 years old, as the reporting of age for adults 80 years and older was determined to be a disclosure risk. Treating age as a continuous variable for the analyses would therefore have incorrectly reflected the age of these older adults. The age variable was therefore trichotomized, thus retaining some ability to make distinctions among age groups and enabling an interpretation that distinguishes between young, middle-age, and older women. Consistent with the analyses involving depression and diabetes conducted by Egede and colleagues, 10 age 65 was chosen as the lower endpoint of the oldest category in the trichotomized age variable. As other studies involving depression and diabetes that have not measured age as a continuous variable have used age 60 as such a cutoff,38,43 our analyses were repeated, with age groupings recategorized as 20-44 years, 45-59 years, or at least 60 years. Unadjusted results using this new categorization still showed younger age (ie, 20-44 years and 45-59 years compared with 60 years or older) as a significant predictor of depression in women with diabetes, as did adjusted results in the multivariate model. Using the new categorization for age groupings, the same additional variables identified as statistically significant predictors of depression as in the initial age group categorization were also found to be statistically significant predictors in the multivariate model.
Implications for Diabetes Educators
Diabetes educators—whether nurses, dietitians, pharmacists, exercise physiologists, physicians, or mental health professionals—have long been encouraged to address the holistic needs of patients with diabetes. 73 In view of the high prevalence of depression among women with diabetes, the findings of this study demonstrate the importance of their conducting depression screening for the women who they educate and counsel. Findings especially underscore the importance of recognizing the sex-specific characteristics associated with depression among women with diabetes: younger age, less than high school graduation, self-rated fair or poor health, inactivity due to poor health, and pain that interferes with usual activities. This will enable the targeting of especially vulnerable women for screening and depression treatment, recognizing that these female-specific characteristics are not all the same as those identified in populations that include both men and women with diabetes. In particular, multicomponent and intensive interventions that address pain and mobility in tandem with diabetes health education may be needed to address depression, improve diabetes outcomes, and enhance perceptions of health in women with diabetes.
Conclusion
This study provides important findings about the salience of demographic, health-related perception, pain, and inactivity regarding their relationship to depression in adult women with diabetes. Screening and intervention to address these conditions with health promotion treatment are especially needed among this vulnerable group of women.
Footnotes
Funding:
The authors declared no funding from sponsored research. The authors also declared no financial interests related to the research or compensation for preparing the manuscript.