
Abstract
Purpose
The purpose of this study was to determine antidepressant use among Mexican Americans (MA) and non-Hispanic (NH) blacks and whites with type 2 diabetes and depressive symptoms.
Methods
A secondary data analysis based on National Health and Nutrition Examination Survey (NHANES) 2005-2012 cohort data included 560 noninstitutionalized civilian MA, NH black, and NH white adults with type 2 diabetes and depressive symptoms. Unadjusted and adjusted 2-way ANOVA models evaluated whether there was a difference in the use of antidepressants by depressive symptom level across race/ethnic group.
Results
Whites were more likely than blacks and MA to be on antidepressant treatment (whites: 41.7%, blacks: 27.1%, MA: 24.2%) and on serotonin-norepinephrine reuptake inhibitors (SNRI) (whites: 8.1%, blacks: 2.9%, MA: 2.4%). However, there was no difference in the use of other drug classes or antidepressant use by depressive symptom level across racial/ethnic group. Followed by tricyclic antidepressants (TCA), selective serotonin reuptake inhibitors (SSRI) were the most commonly used drug class overall. Approximately 30% of subjects were on antidepressants and among those, 80% were on one antidepressant, all others on 2 or more.
Conclusions
Racial/ethnic differences were observed in the use of antidepressant treatment but not when depressive symptom levels were incorporated in the analyses. Further studies on the effectiveness of different antidepressants in diabetes outcomes minorities are needed.
Approximately 8% of Americans had moderate to severe depressive symptoms between 2009 and 2012. 1 Some studies suggest the proportion of depression among those with diabetes is almost twice as high as those without it.2,3 The proportion of major depression among those with both conditions has been found to be 11%. 2 While 31% of patients may have clinically relevant depression, projections indicate that nearly half of patients with diabetes have undiagnosed depression.2,3 While the directional association between diabetes and depression is still unclear, it is well documented that having both conditions at the same time is worse than having each illness alone.2,3 Diabetics with depression are at a much higher risk of having poor glycemic control and diabetes self-care behaviors (ie, medication adherence, diet and exercise), complications, disability, mortality, and increased health care use and costs. 3 They also have reduced work productivity and quality of life. 3
Reports of depression by racial/ethnic group in the general population are limited. One national study found non-Hispanic (NH) whites (with or without diabetes) were more likely to have no depressive symptoms compared to NH blacks and Hispanics. 1 However, another study among retired Americans found that after adjusting for sociodemographic, health, and economic factors, African Americans were less likely to have major depression compared to whites. 4 Studies evaluating whether there are differences in depression rates by racial/ethnic group among those with diabetes are inconclusive. Proportions of depression among black and Hispanic minorities are either higher, lower, or the same when compared to whites.2,3,5-8
Both depression and diabetes clinical guidelines emphasize the need for routine screening of depression among those with diabetes.9 -12 Even though they highlight the need for special treatment considerations among those with diabetes, they do not give specific pharmacotherapy recommendations. Given the number of antidepressants available and their adverse effect profile, careful selection of these agents is warranted. Important considerations include effects on blood glucose, body weight, blood pressure, and renal function as well as coexisting medical conditions. 10
One national study reported that 11% of Americans with or without diabetes take antidepressants and NH whites are more likely than NH blacks and Mexican Americans (MA) to be taking at least one antidepressant (13.6%, 3.9%, 2.7%, respectively). 13 Only one regional study evaluated depression treatment rates among racial/ethnic minorities with depressive symptoms and diabetes. 5 This study concluded that African Americans in the northeastern United States were less likely than whites to receive treatment. There was no difference between whites and Latinos.
A national study evaluating the use of antidepressant treatments among racial/ethnic minorities would inform health care providers whether disparities exist and if their treatment approach should be modified. Therefore, the following research questions were assessed: (1) Is there a difference in the use of antidepressant regimens among MA, NH blacks, and NH whites with type 2 diabetes and depressive symptoms in the United States? (2) Is there a difference in the use of antidepressant regimens by depression level across race/ethnic group?
Methods
Research Design and Study Participants
The National Health and Nutrition Examination Survey (NHANES) is designed to assess the health and nutritional status of the United States civilian noninstitutionalized population. A major program of the National Center for Health Statistics, NHANES is unique as it combines interviews and physical examinations including laboratory tests on a cross-sectional basis. The NHANES interview data provide self-reported participant history of diabetes and medication use, and physical examinations conducted by trained medical staff. The questionnaire component includes a depression screener that uses the Patient Health Questionnaire (PHQ-9), an instrument for screening, diagnosis, and monitoring of depression. PHQ-9 scores of 5, 10, 15, and 20 represent mild, moderate, moderately severe and severe depression, respectively. 14 Mexican American and black persons have been oversampled since 1999 to increase the reliability and precision of estimates of health status indicators in this group. The National Center for Health Statistics Institutional Review Board approved the protocols for the conduct of NHANES and obtained informed consent from all participants.
This study was a secondary data analysis of survey participants who reported being NH white or black or MA, who had been given a diagnosis of diabetes by a provider at age of 20 years or older and had a PHQ-9 survey score of 5 or greater at the time of survey interview. To produce estimates with greater statistical reliability for demographic subdomains like sex-age-race and ethnicity, cohorts 2005-2006, 2007-2008, 2009-2010, and 2011-2012 were combined. 15
Study Outcome
The main outcome was antidepressant treatment use defined as being on any antidepressant (ie, selective serotonin reuptake inhibitors (SSRI), serotonin modulator, serotonin-norepinephrine reuptake inhibitors (SNRI), tricyclic antidepressants (TCA), monoamine oxidase inhibitors (MAOI), bupropion, and/or mirtazapine). All antidepressant medications were extracted from the prescription medication file, which provides a list of generic names of prescription medications used within 30 days prior to the survey date.
Data Analysis
Statistical analyses were conducted using IBM SPSS Statistics, version 24 (IBM Corp, Armonk, NY). All estimates in this study are nationally representative of the civilian, noninstitutionalized, US population of adults aged 20 years or older meeting study criteria and have been adjusted for complex sample design and nonresponse bias. 15 The chi-square and one-way analysis of variance (ANOVA) tests were used to compare categorical and continuous parameters describing socio-demographics, clinical history and biometrics, health care use and access, drug use by class, and number of medications across race/ethnic groups. A 2-way ANOVA was used to test whether there were differences on antidepressant use by racial/ethnic group (main effect). The interaction of the PHQ-9 score depression level and race/ethnic group was also evaluated on antidepressant use. For this study, 2 depression level categories were created, one with PHQ-9 scores from 5 to 9 (mild) and the second 10 or more (moderate to severe). These analyses were adjusted for gender, age, education, income, insurance coverage, body mass index, waist circumference, number of years with diabetes, and cohort year. Both TCAs and SNRIs may also be used to treat diabetic neuropathy so analyses will be adjusted for this parameter. Diabetic neuropathy was defined as having tingling or numbness in hands or feet. A 2-sided alpha of .05 was used to determine significance in all statistical comparisons. Data are described using proportions, means, standard errors, and 95% confidence intervals (CI), where appropriate.
Results
A total of 560 subjects were included in the study. Data analyses reveal several differences in sociodemographics, clinical history and biometrics, health care access, and glycemic control across race/ethnicity (Table 1). None of the patients in the study reported having diabetic neuropathy. The proportion of MA, NH blacks, and NH whites with mild or moderate/severe depression did not differ across groups (P = .297; Table 1). Overall, close to one-third of participants were on antidepressant therapy (30.1% unadjusted, 31.0% adjusted).
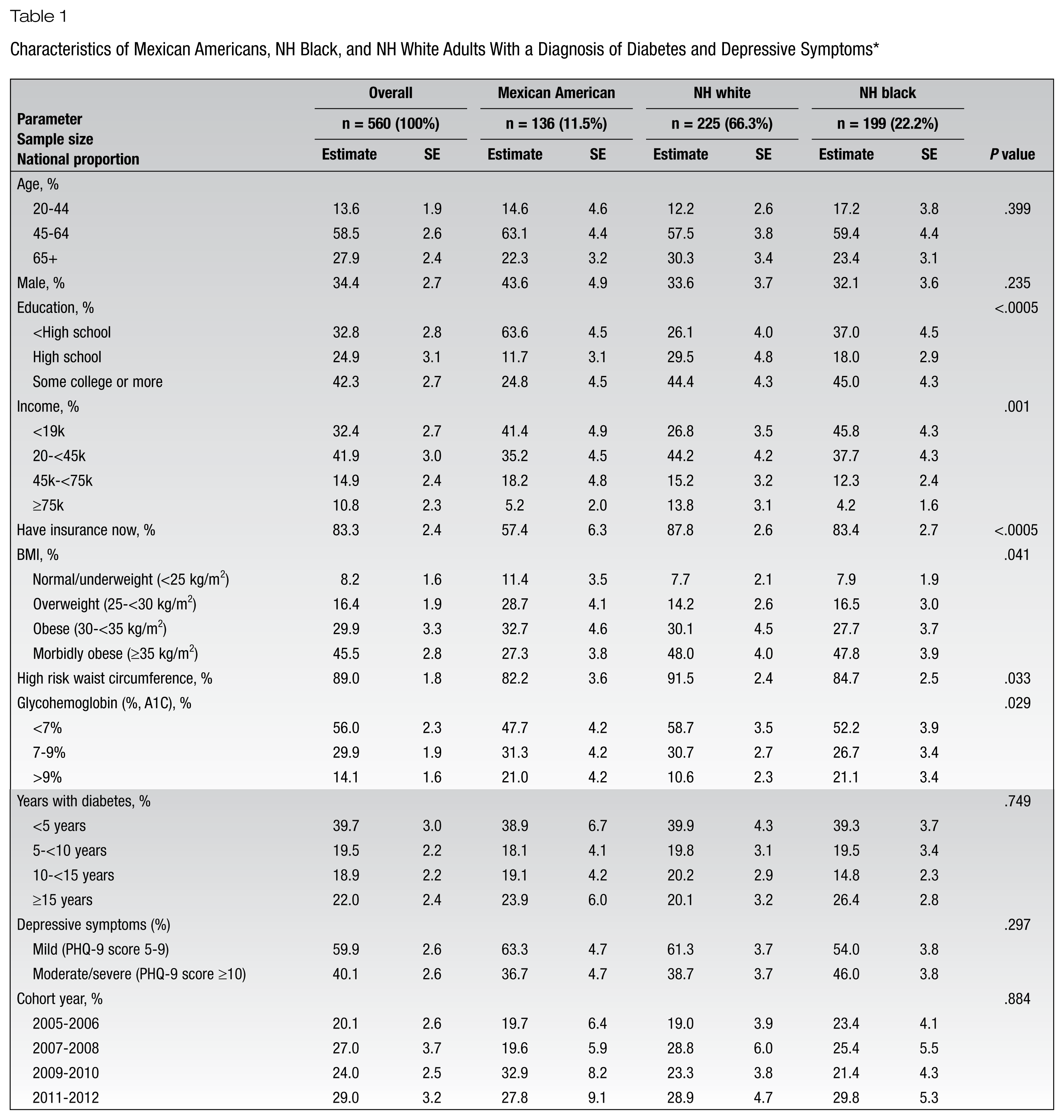
Characteristics of Mexican Americans, NH Black, and NH White Adults With a Diagnosis of Diabetes and Depressive Symptoms*
Outcomes by Race/Ethnic Group
The proportion of MA and blacks on antidepressant therapy was statistically lower compared to whites (adjusted: 24.2% [95% CI 15.7-32.7%], 27.1% [95% CI 20.3-34.0%], and 41.7% [95% CI 33.2-50.1%], respectively; P = .02).
No difference in the number of antidepressant medications was observed across race/ethnic groups (P = .377; Figure 1). Among those on antidepressant therapy, 82.2% were on one antidepressant (MA: 90.6%, whites: 82.0%, blacks: 78.8%), 17.2% were on 2 antidepressants (MA: 7.6%, whites: 17.3%, blacks: 21.2%) and 0.6% on 3 or more antidepressants (MA: 1.8%, whites: 0.6%, blacks: 0.0%).
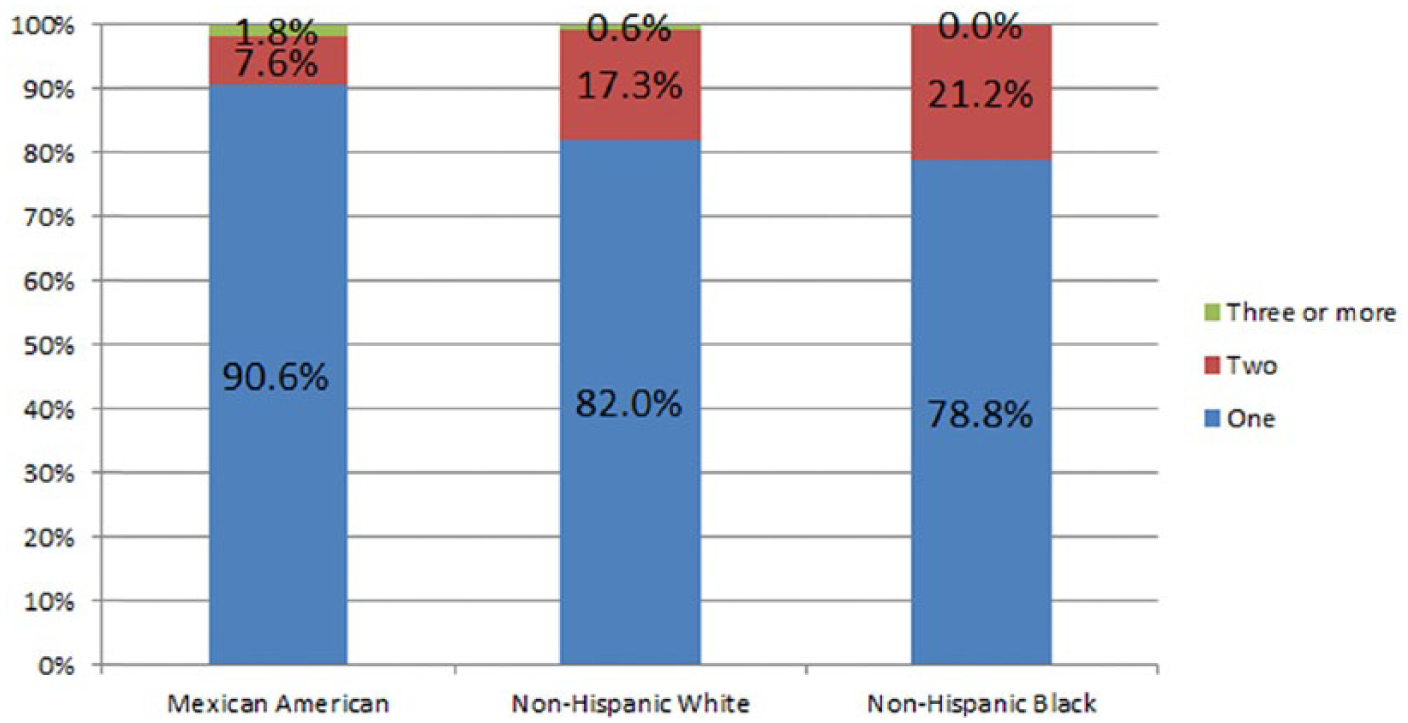
Distribution of the number of antidepressants by race/ethnic group among patients on antidepressant treatment. Antidepressant drug classes represented in the graph include selective serotonin reuptake inhibitors (SSRI), serotonin-norepinephrine reuptake inhibitors (SNRI), serotonin modulators, tricyclic antidepressants (TCA), monoamine oxidase inhibitor (MAOI), bupropion, and mirtazapine. There was no relationship between number of antidepressants and race/ethnic group (P = .377).
There was a statistically significant difference in the use of SNRIs across race/ethnicity but not in the use of SSRIs, serotonin modulators, TCAs, MAOIs or other antidepressants (bupropion and mirtazapine; Figure 2). SNRI use was 2.4%, 8.1%, and 2.9% among MA, whites, and blacks, respectively (P = .018). SSRIs were the most commonly used drug class (MA: 16.4%, whites: 23.6%, blacks: 14.0%, followed by TCAs (MA: 2.4%, whites: 8.1%, blacks: 5.4%), SNRIs, serotonin modulators (MA: 1.2%, whites: 4.5%, blacks: 3.3%), other antidepressants (MA: 2.8%, whites: 1.8%, blacks: 3.8%) and MAOIs (0% for all race/ethnic categories) but there was no statistically significant difference across race/ethnic group (P > .05 for all).
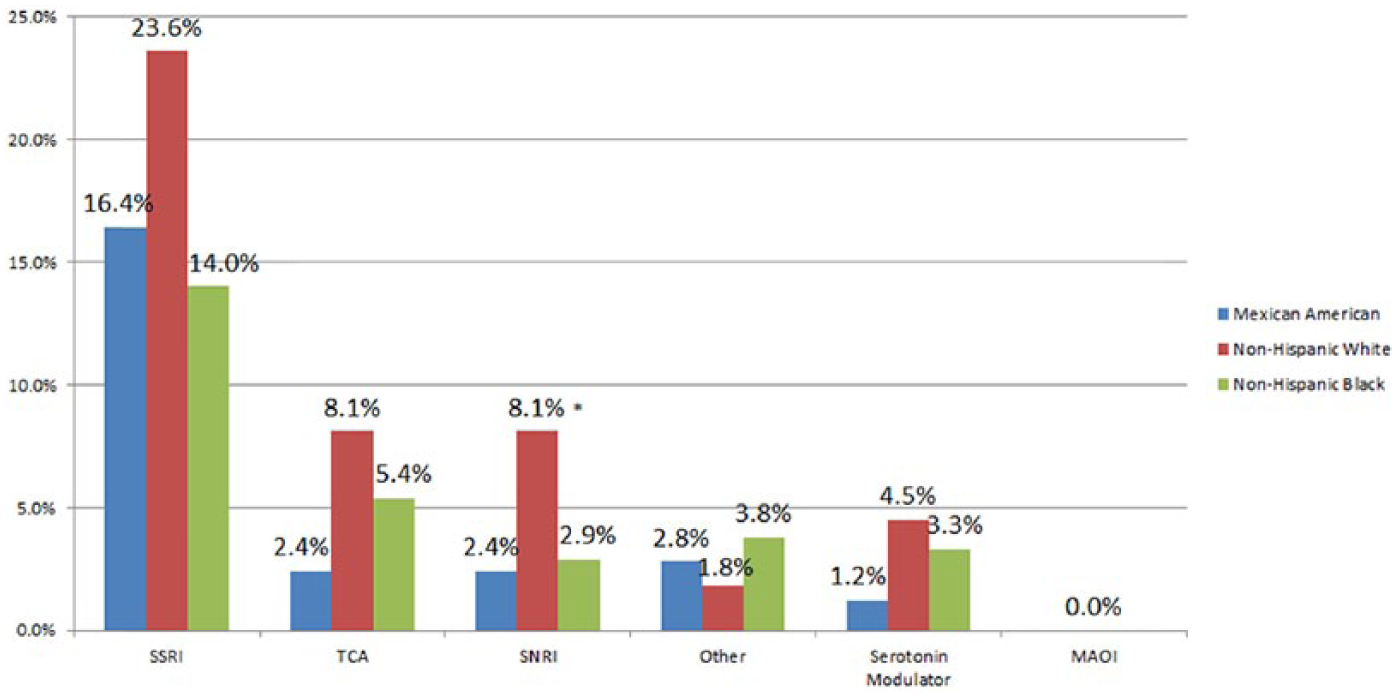
Distribution on antidepressant drug classes by race/ethnic group. SSRI, selective serotonin reuptake inhibitors; TCA, tricyclic antidepressants; SNRI, serotonin-norepinephrine reuptake inhibitors; Other, other antidepressants such as bupropion, and mirtazapine; MAOI, monoamine oxidase inhibitor. *P = .018.
Antidepressant Use by Depression Level and Race/Ethnic Group
The use of antidepressant therapy was statistically the same by depression score level across racial/ethnic group (unadjusted, P = .455 shown in Figure 3). After adjusting for the specified sociodemographic and clinical factors and cohort year, there was no statistical relationship in the model (adjusted, P = .402).
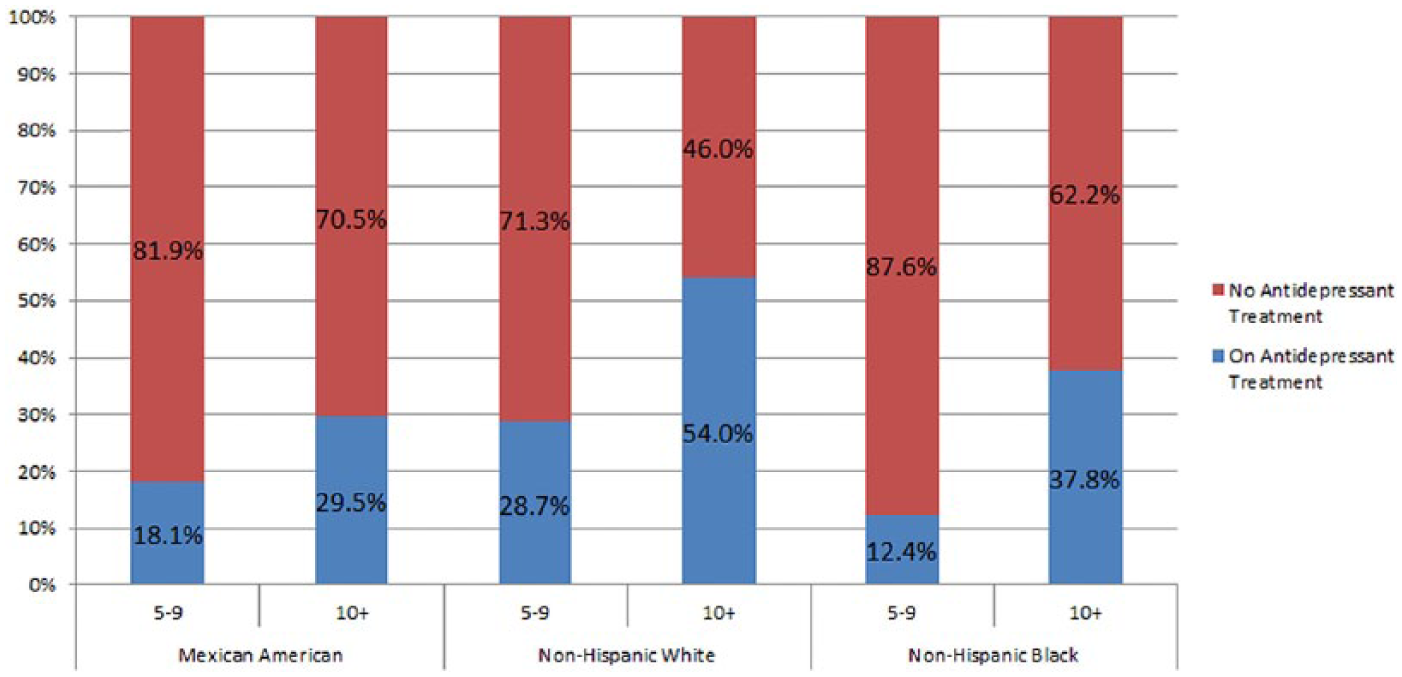
Percentage of subjects on antidepressant treatment and no antidepressant treatment by Patient Health Questionnaire (PHQ)–9 score level and race/ethnic group (unadjusted). Drug classes for those on antidepressant treatment included selective serotonin reuptake inhibitors (SSRI), serotonin-norepinephrine reuptake inhibitors (SNRI), serotonin modulators, tricyclic antidepressants (TCA), monoamine oxidase inhibitor (MAOI), bupropion, and mirtazapine. There was no statistical relationship between the use of antidepressants and PHQ-9 score level across race/ethnic groups (P = .455). There was no significant relationship after adjusting for gender, age, education, income, insurance coverage, body mass index, waist circumference, number of years with diabetes, and cohort year (P = .402).
Discussion
This is the first pharmacoepidemiologic study evaluating antidepressant use among NH blacks, NH whites, and MA with type 2 diabetes and depressive symptoms. Close to one-third of our study population was on antidepressant treatment, and compared to blacks and MA, whites were more likely to be treated. Approximately 18% of study subjects were on SSRIs, and this was the most commonly used drug class. SNRIs were the only drug class in which use was statistically different across racial/ethnic groups, and in this case was highest among whites. This may be due to the higher proportion of insured participants among whites. Among those on antidepressant therapy, over 80% were on one medication, the rest on 2 or more, and no disparities were observed. No difference in levels of depressive symptoms or in the use of antidepressants by level of depression across racial/ethnic group were observed.
The primary literature reports mixed evidence regarding racial/ethnic disparities in the prevalence of depression and depressive symptoms, but we found no differences in this national study. Furthermore, this report supports published evidence that has found whites to be more likely than minorities to be on antidepressant treatment.
SSRIs were the most commonly used drug class in this study population, which is consistent with published reports of the most commonly prescribed antidepressants. 16 However, several reviews have concluded that the efficacy of the different antidepressants is generally comparable both in and across the drug classes in any phase of the patient’s depression. This is quite important because one of the most important aspects of selecting pharmacotherapy for the treatment of depression is its adverse effects profile. Some antidepressants may have higher incidences of weight gain (eg, mirtazapine), whereas others may even produce weight loss (eg, bupropion), which may have an effect on improving glucose control and reducing diabetic complications (eg, sexual dysfunction). 17 The American Psychiatric Association guidelines on the treatment of depression provide further insight. They suggest collaborating with primary care physicians when initiating an antidepressant or making significant dosing adjustments if fluctuations in fasting blood glucose occur. 10 Furthermore, it is noted that the use SSRIs may be preferred over TCAs, which may be associated with poorer glycemic control, but it fails to mention other commonly used antidepressant classes such as SNRIs, serotonin modulators, or more specially bupropion. 10 This study showed TCAs were the second most commonly used medication class in patients with diabetes and depression. This goes against guideline and more recently published recommendations; however, the possibility of TCA or SNRI use for the treatment of diabetic complications (eg, diabetic peripheral neuropathy) could not be ruled out. 18 Though data are lacking for the effects of other antidepressants on specific diabetic outcomes, this opens an avenue for important and impactful research to be conducted. Furthermore, effectiveness outcomes measuring benefits on diabetes self-care behaviors, quality of life, functional status, health care expenditures, and their differences across racial/ethnic groups should be evaluated.
Several limitations of this study deserve mention. First, this study used cross-sectional data. PHQ-9 scores were taken in one day and may not be representative over an extended period of time. The antidepressant use reported by patients was of 30 days prior to survey participation but may change over time based on patient-specific needs. Second, subjects may have been misclassified as not having depressive symptoms because their current treatment is effective and may have been excluded from this study. Third, all questionnaire-based data including diabetes diagnosis and prescription medication use were self-reported and may be incorrect or influenced by recall bias possibly yielding misclassifications. However, one study showed that patient self-report of diabetes history and medication use is accurate when compared to medical records. 19 Fourth, antidepressant dose strengths were not available, so dose maximization could not be evaluated as a treatment quality outcome. Fifth, medication use behavioral data were not available and may play a significant factor in depression. Sixth, even though diabetic neuropathy is prevalent, none of the participants reported having a history of this condition so appropriate adjustments in the analysis for the use of TCAs and SNRIs could not be conducted. Seventh, even though analyses were adjusted for cohort year, several new brand-name and generic medications became available during data collection time and may have changed medication use patterns. Eighth, these results are only representative of the US noninstitutionalized civilian adults meeting study criteria.
Implications/Relevance for Diabetes Educators
Among subjects with a diagnosis of diabetes and depressive symptoms, NH whites were more likely than NH blacks and MA to be on antidepressant treatment. There was no difference on antidepressant use by depressive symptom level across racial/ethnic group. Close to one-third of subjects were on antidepressant treatment and 80% were on one antidepressant. Except for SNRI use being higher in whites, there were no other differences in drug class use across racial/ethnic group. SSRIs were the most commonly used drug class and were followed by TCAs. It is important that diabetes educators consider the effects that antidepressant drug classes or individual antidepressants may have on diabetes outcomes in this patient population.
Footnotes
Acknowledgements
There are no conflicts of interest to disclose. Dr Alexandra Perez takes full responsibility for the work as a whole, including the study design, access to data, and the decision to submit and publish the manuscript. Thank you to Dr Joshua Caballero for reviewing the manuscript.
No funding was requested for this study.
No financial disclosures for any of the authors.
Author Contributions
Drs Perez, Cabrera, and Gutierrez designed the study, analyzed the data, and wrote and edited the manuscript. Dr Valdes designed the study, and wrote and edited the manuscript.