
Abstract
Diabetes self-management training (DSMT) improves diabetes health outcomes. However, low numbers of patients receive DSMT. Using virtual environments (VEs) for DSMT is an innovative approach to removing barriers for patients. The purpose of this paper is to describe the experience of health professionals and diabetes educators establishing and teaching DSMT in a VE, Diabetes LIVE© (Learning in Virtual Environments), and the implications for future use of VEs in DSMT. It was found that providing DSMT in a VE preserves real-time interaction between patients and educators. To facilitate ongoing patient learning and engagement, the DSMT curriculum was expanded beyond the core content as “Above and Beyond” topics. Using a VE for DSMT presents challenges and opportunities. Challenges include overcoming technological barriers and improving comfort levels to orient educators and patients to the functionality of the VE. Opportunities include overcoming barriers to reaching patients, particularly given the diabetes epidemic and relatively small number of diabetes educators. Using a VE also affords a simulated community for experiential learning. VEs may become powerful tools for diabetes and other health educators to reach patients. Ongoing education and support are vital to successful self-management of chronic disease.
Despite the established benefits of diabetes self-management training (DSMT), low numbers of patients with diabetes receive DSMT, and the Centers for Disease Control and Prevention reports that only 57% of people with diabetes have ever attended DSMT.1-3 Li et al 4 found that in 2011-2012, only 6.8% of 95 555 privately insured participants living in the United States received DSMT within 12 months of diagnosis. Similarly, Strawbridge et al 5 reported that 5% of the 110 064 Medicare beneficiaries diagnosed with diabetes received DSMT. Even though participants in both of these studies were eligible for DSMT, rates of participation were low. Barriers to DSMT include a lack of access to programs, a low rate of referral to DSMT by providers, and patients’ unawareness of the value of DSMT.1,6 In a national survey involving 502 individuals with diabetes who had not received DSMT, respondents most frequently identified “not needing DSMT” and “not being able to fit DSMT into their schedule” as barriers to obtaining DSMT. 7 Patients living in rural and/or underserved areas have less access to Certified Diabetes Educators (CDEs). A lower likelihood of receiving diabetes education could increase health disparities for patients living in these areas.8,9 Last, the supply of CDEs overall is not expected to keep up with the global demand created by the growing diabetes epidemic.10,11
Given the increasing prevalence of diabetes, the benefits of DSMT, the projected shortage of diabetes educators, and the low uptake of DSMT by persons with diabetes, innovative, widely accessible, and evidence-based methods of providing DSMT are needed. The development of web-based DSMT has begun to broaden the reach of DSMT beyond that of in-person, on-site, or office-based programs, and web-based DSMT has been successfully implemented in research settings. 12 As of 2013, 84% of adults in the US population reported having internet access and 73% had a high-speed connection, making web-based education delivery increasingly accessible for patients.13,14 Web-based DSMT improves glycemic control and diabetes knowledge when compared with usual care12,15 and has the advantage of providing convenient access for the participant and the educator and enabling the participant to self-pace his or her progression through educational materials. Furthermore, participants in web-based programs report satisfaction with this mode of DSMT delivery.16,17
However, not all internet- and web-based DSMT programs are the same. For example, some web-based programs allow for asynchronous interaction, providing participants with access to educational resources (eg, videos, podcasts) or blogs but not real-time interaction with other persons or educators. Synchronous internet-based programs occur in real time and allow for enhanced engagement, attention, and feedback. 18 Virtual environments (VEs), which are real-time computer-generated 3D representations of a contrived or natural environment running over the internet, 19 are an example of synchronous online interactive communities. 20 VEs can create a sense of social presence that can enhance interaction and knowledge retention for persons engaging in the VE. 19 The technical development and components of the VE, including the costs associated with the development of the program referred to in this paper, are fully described in another manuscript (C.M.J. et al, unpublished data). A randomized controlled trial (RCT), Diabetes LIVE© (Learning in Virtual Environments) (NHLBI 1R01-HL 118189-01), is ongoing to investigate the efficacy of DSMT that is delivered through either a traditional website format or a VE; outcomes being studied are healthy eating, physical activity, and clinical outcomes in individuals with type 2 diabetes. 21 The present article describes a VE in which health care professionals teach DSMT via Diabetes LIVE and discusses implications for the future use of VEs for teaching patients with diabetes.
Description of LIVE
Diabetes LIVE is a virtual environment created in the likeness of an island resort community that is home to a fitness center, clothing outlet, pharmacy, bookstore, restaurant, reflection garden, farmer’s market, grocery and convenience stores, and a classroom for the DSMT sessions. Participants and educators self-represent as avatars (a digital representation of a human). Participants in the research study and diabetes educators interact with each other in real time online through verbal or text communication. 21 Participants can move their avatar around the island 24/7 to browse diabetes resources, engage in interactive activities such as reviewing the nutritional content of foods on menus from various fast food venues available in the restaurant or in the grocery store, play games designed to increase diabetes knowledge, attend DSMT, and access the discussion forum. The discussion forum, accessed by clicking on icons located across the island, is similar to a blog and allows for asynchronous text communication between educators and participants or participant to participant.
DSMT Curriculum in Diabetes LIVE
Basic DSMT
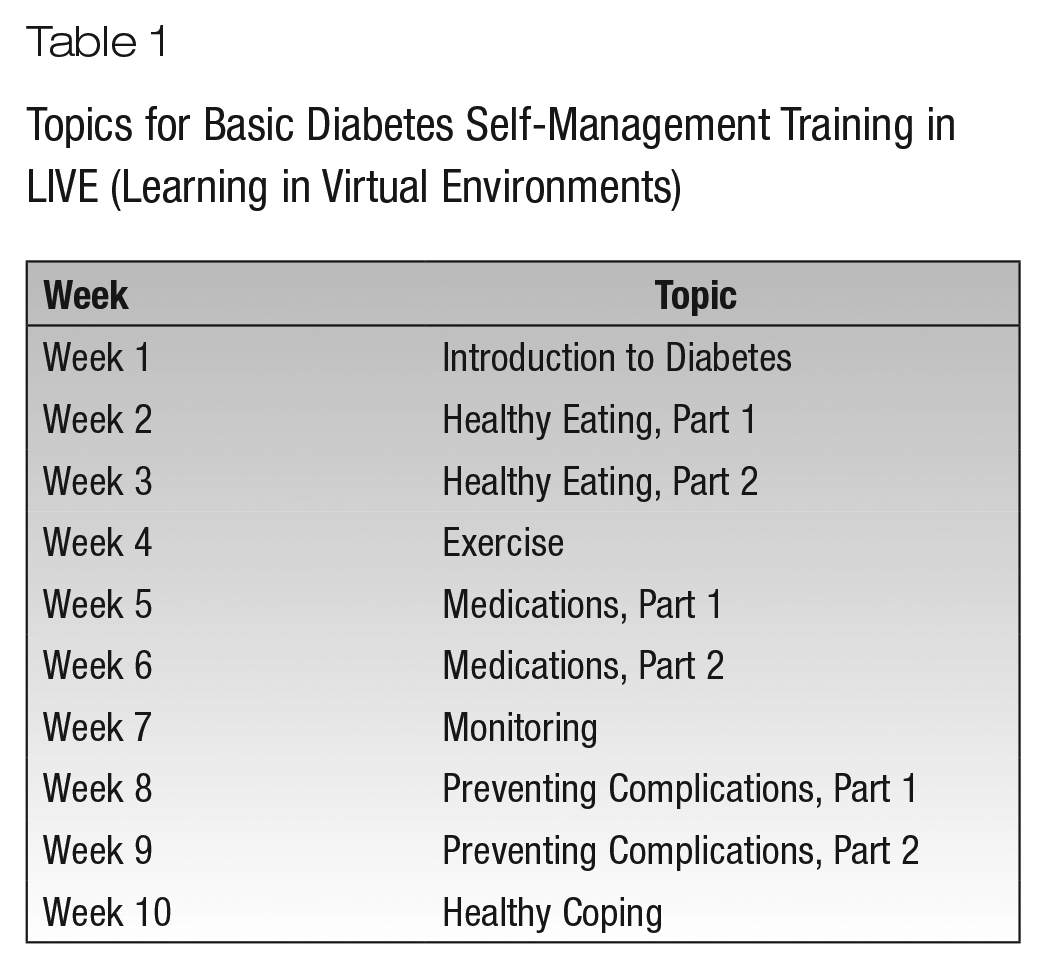
In 2014, diabetes educators, consisting of 2 clinicians from urban areas around New York City and Connecticut and 3 clinicians from urban areas in North Carolina, developed 12 one-hour Diabetes Self-Management Education (Basics of Diabetes) classes based on the American Diabetes Association and American Association of Diabetes Educators (AADE) curricular framework, which covers 7 major self-care behaviors: healthy eating, taking medication, monitoring, being active, problem solving, reducing risks, and healthy coping. 22 Session 1 of the series, Introduction to Diabetes, provided an overview of type 2 diabetes and goals for care followed by content pertaining to the AADE’s 7 self-care behaviors as listed in Table 1. Synchronous courses 60 minutes in duration were taught by nurse practitioners with extensive diabetes management experience and experienced CDEs. A CDE registered dietitian also taught classes and provided advice on nutrition education content. Throughout the study, the diabetes education team met virtually (ie, in the LIVE site or by web conference call) to collaborate, plan, evaluate, and modify the DSMT program.
Topics for Basic Diabetes Self-Management Training in LIVE (Learning in Virtual Environments)
Above and Beyond the Basics of Diabetes
Diabetes educators developed an additional set of classes, titled the Above and Beyond Series, to promote engagement of participants in the virtual classroom for an additional 13 weeks. These classes built on the knowledge learned in the Basics of Diabetes classes. The diabetes educators brainstormed topics of interest, considered participant input, and then evaluated the nature of questions during the Basics of Diabetes classes to create presentations and discussion content for the following topics: What’s New With Diabetes?; Cardiovascular Risk and Diabetes; Myths About Diabetes; Diabetes Then and Now; Your Blood Pressure and Diabetes; A Guided Tour of the ADA Website; Diabetes Medications: What’s Right for You?; Making Lasting Lifestyle Changes; Complementary and Alternative Diabetes Treatments; Navigating Diabetes Research; An Owner’s Guide to the Pancreas; Fad Diets; and Apps, Gadgets, and Gizmos for Diabetes (Table 2).
Topics for Above and Beyond With Diabetes Classes in LIVE (Learning in Virtual Environments)
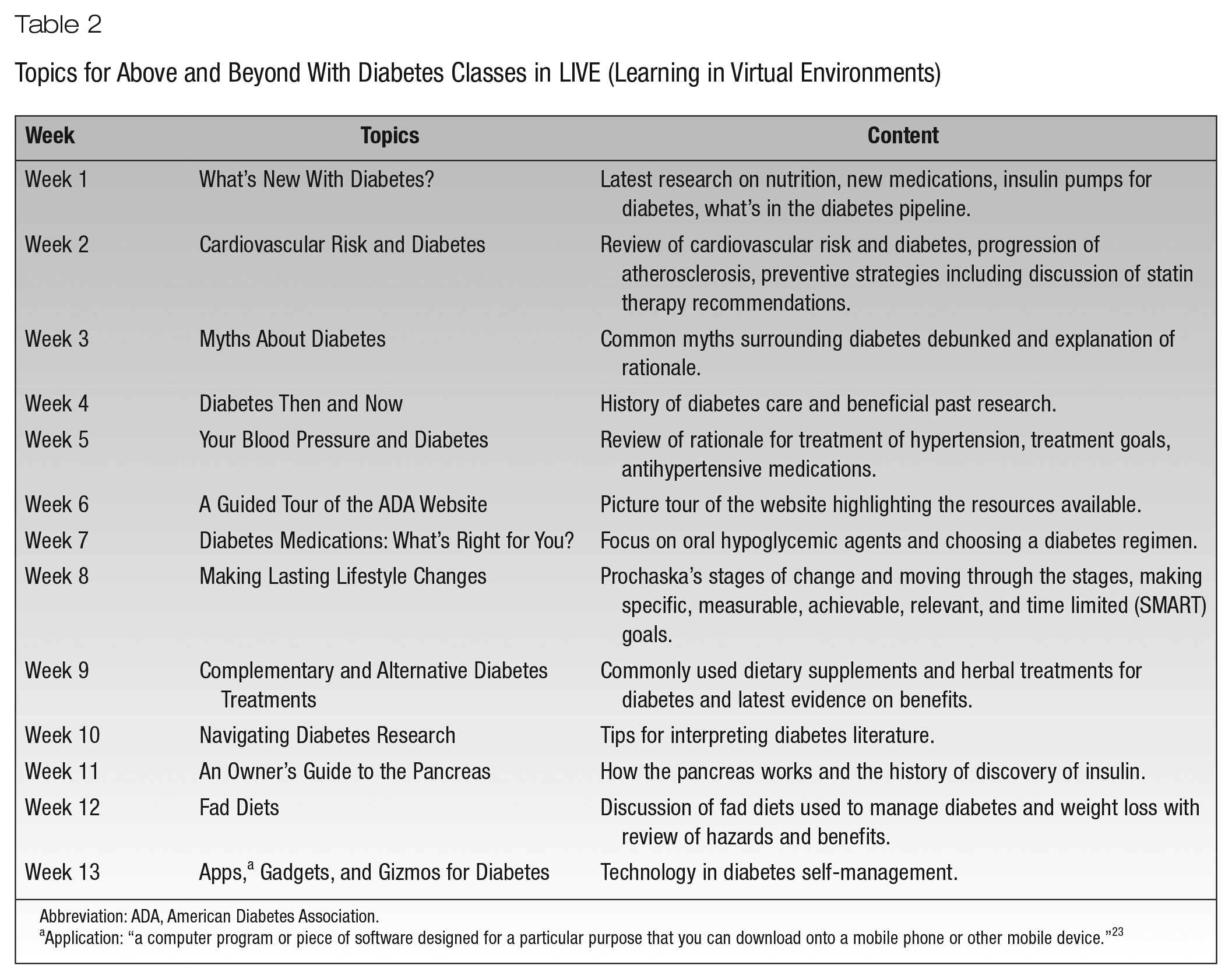
Abbreviation: ADA, American Diabetes Association.
Application: “a computer program or piece of software designed for a particular purpose that you can download onto a mobile phone or other mobile device.” 23
As an example, the content of the Navigating Diabetes Research class included a description of the different types of research (eg, RCTs, descriptive studies) and the principles for interpreting diabetes research findings presented in newspapers, in magazines, or on TV news programs. Examples of research conducted with small sample sizes or specific ethnic groups were presented, and participants were asked to identify the factors that affect generalizability of findings. Participants enjoyed discussing the meaningfulness and validity of presented research topics with each other and the educator. The Above and Beyond Series was designed to generate more discussion of topics relevant to diabetes self-management and to help participants become engaged health consumers.
Educator Orientation
While all of the educators were experienced in DSMT, most were unfamiliar with teaching in VEs. Learning the mechanics of moving an avatar required practice. Competencies required for teaching in VEs included being able to navigate an individual avatar, learning the functionality of creating a class session, and adjusting audio controls for optimal voice settings, as well as familiarity with all of the general functionality of the VE to assist participants troubleshoot any minor technical issues.
Those with experience teaching in the VE (a team leader and one of the study’s primary investigators) conducted an orientation for the educators. Preparing the educators for teaching in the VE and establishing a high comfort level with the technology required significant practice on the part of the individual educators and one-on-one training sessions with the study team over a period of 3 months. The necessary practice and training were related to degree of naivety and comfort level with online technologies and interactive virtual environments.
The educators’ orientation was an iterative process and eventually involved meeting in the VE for demonstrations. This was instrumental in helping educators assimilate to the VE. Having the support of educators with VE teaching experience and being able to observe LIVE classes before teaching independently lessened anxiety and bolstered confidence for educators new to VEs. For the initial classes in the VE, the programmers of the site and experienced educators from the team were in class or on call to troubleshoot or step in if the assigned educator had any technical or user issues during class.
Being adept at maneuvering the avatar around the site became important as the educators began “walking” with class participants to different areas in LIVE during and after classes for continued interactive learning and exploration of the site. For example, after the class on the topic of diabetes medications, the educator and class participants visited the virtual pharmacy to review common over-the-counter cold and flu medications (Figure 1). These virtual field trips appealed to participants and provided opportunities for learning how to navigate the VE, accessing resources, and, in this case, understanding the ingredients in over-the-counter medications and identifying any drug-drug interactions with diabetes medications. Educators prepared for these field trips before class by confirming the class topic and examining the available resources in LIVE (eg, books, menus, food items, videos), and some educators performed a trial session before class without participants to identify issues and determine the steps needed to navigate with ease from beginning to end of the field trip. Time required to prepare the content and overall strategy for these field trips ranged from 30 to 60 minutes.

Diabetes educator and participants on a virtual field trip to the pharmacy.
Educators used a password-protected learning management system (Sakai) for sharing materials and communicating with the education team. The Sakai software platform includes a class and discussion forum sign-up schedule and a repository for class presentations. Class field notes are also kept here, and these provide details about class attendance, level of engagement among participants, and any other issues with the site or class.
Logistics of DSMT Delivery
Participants were queried at enrollment by study staff as to their preference for class scheduling and then again intermittently during subsequent classes and with follow-up emails. Based on participant consensus, classes were held during the evening as late as 8 p.m. on weekdays or weekends, typically twice weekly. The VE with its 24/7 availability allows for a patient-centered approach when scheduling classes. Furthermore, educators, who might not be available or might prefer to teach during the late evening or on the weekend, may embrace the idea of teaching at these times if they are able to teach from home in a VE.
Media boards, similar in appearance to billboards, are located at the LIVE island’s main locations (Lobby, Plaza, Food Court), and these advertise the class schedule, date, time, and topic of each class. Email reminders to participants are sent twice weekly by the study staff and include information about the upcoming class.
On the date of a scheduled class, the educator logs into the VE site before class to create a session and sends an invitation to participants to enter the class. The educator avatar displays PowerPoint slides or web content on the media board in the front of the auditorium-style classroom. Figure 2 provides an image of an educator teaching a class in the VE. Communication among the educator and participants is primarily by synchronous voice (headset and microphone) or occasionally by use of text communication functions. The educator’s avatar can also move about the classroom to socialize with participants. Before beginning the topic of the week, the educator responds to questions related to the prior week’s content.

A virtual diabetes self-management training class.
Teaching Approach
Similar to educators teaching in other environments (eg, classroom, web), educators teaching in the VE seek to engage adult participants in active learning. Consequently, the educators embrace a teaching approach based on the learning theory of constructivism and apply these principles during all synchronous diabetes education classes, during field trips around the VE, and in the discussion forum.
Constructivism, particularly relevant to the community of diverse learners in the VE, views teachers as facilitators of learning rather than providers of content or knowledge and frames learning as socially constructed and collaborative. 24 In the VE, participants can attend synchronous classes at any point in the schedule rather than having distinct entry and completion points. They can choose to attend a basic and advanced session every week, follow a schedule of classes sequentially from start to finish, or skip classes and rejoin a week or two later. With rolling enrollment and a flexible curriculum, there may be a core group of participants with varying levels of diabetes expertise attending weekly classes and new participants joining on a regular basis. Opportunities for new or veteran participants to share experiences with each other and socially construct knowledge are increased in the VE. Additionally, participants engaged in the VE receive education and ongoing social support over the course of the year of participation.
Another salient feature of the constructivist approach is that learners construct their own meaning, in this case around the self-management of diabetes, rather than memorize correct or incorrect answers. 25 Group interaction is encouraged before and after class sessions. The educators allow participants to answer questions if possible, and responses are reviewed for accuracy. Participants come to realize that there may be more than one solution to a problem and numerous options for individualizing self-management. For example, after a class on the topic of exercise, participants and the educator walk their avatars to the fitness center to view a video on isometric exercises. The video illustrates that there are several types of exercises that qualify as isometric. The ability to validate what is discussed in class in what appears to be a real-life setting with real-time visual cues and multiple options for meeting the recommended exercise requirements supports the constructivist approach.
Furthermore, the educator in the VE considers and respects a learner’s experience and prior understanding of issues or problems, which is also a principle of adult learning theory. 26 When needed, the educator moves from the role of facilitator to that of a resource provider or advisor. 27 Educators frequently use the role of advisor or resource provider when responding to participants’ posts in the discussion forum or in class when inaccurate information is brought forth. Although educators provide no medical advice or treatment, they frequently need to clarify or respond to a confusing post, usually about over-the-counter or herbal therapies or food.
Challenges of Teaching in the VE
Regardless of topic, mode of delivery, or environment, engaging participants in learning and sustaining their engagement are challenging. 28 Initially, the VE overcomes these challenges by providing a platform and content that are new and interesting. Over time, the environment must remain fresh and dynamic to promote continued interest.
To that end, the team developed advanced content, revised classes, listened to participants for their ideas (eg, developed the complementary and alternative therapy lecture based on participant feedback), added games such as Jeopardy, and created field trips. Even with these efforts, sustaining engagement is difficult and requires a commitment to reevaluating content and the teaching approach on a regular basis.
Another challenge that educators face when teaching in the VE is the loss of face-to-face communication. As a result, neither the educator nor class participants can acknowledge or assess nonverbal communication such as physical gestures (eg, raising the hand to speak, pointing to a specific object on a slide to make a point, making eye contact), facial expressions of emotion (eg, smiling, furrowed brow), and all other nonverbal expressions and body language. In contrast, educators engaging with participants in the real world can, and often do, use nonverbal expression to evaluate emotions (eg, interest, confusion) and participants’ understanding of what it being said or discussed. Research has supported that students’ nonverbal facial expressions have been significantly positively associated with both their emotions and their level of comprehension. 29 Accordingly, educators teaching in the VE need to enhance other methods of communication (eg, verbal communication, visualization using props, or the creation of mental images) to compensate for the loss of nonverbal communication between the educator and class participants. 30
To improve communication among educators and participants attending class in the VE, educators used the following techniques: (1) accentuating intonation when speaking (eg, to convey excitement), (2) using encouraging probes (eg, “tell us about that” or “great point” or “thank you for sharing that information”), (3) addressing participants by name and asking all participants whether they had anything to share about a specific experience, and (4) being attentive to the display of the participant’s name and a corresponding icon above his or her head that indicates the participant is speaking. These techniques were also helpful to facilitate equality in classroom discussion time and engagement by all participants rather than allowing a subset of the class to monopolize the conversation. In addition to these techniques, educator skills in group facilitation were helpful in engaging participants and overcoming many communication issues.
Last, the system functions the best with high-speed broadband internet access to avoid a lot of “freezing” or difficulty rendering the environment. This requirement has not impeded the enrollment of participants in urban, suburban, and some rural areas to date, but we will explore reach and dissemination in future research. As broadband internet expands exponentially in the United States, we anticipate this will not be an obstacle.
Implications for Diabetes Educators and Practice
Traditionally, DSMT classes have been limited by access to a qualified CDE, access to a physical location for classes, transportation issues, and/or the location of the at-need population. Some of the largest diabetes populations are in rural outreach areas. 31 VEs can help overcome this obstacle. In a VE, a single nurse practitioner or CDE can teach diverse groups of individuals across geographic boundaries simultaneously.
In this study, participants from North Carolina, New York, and Connecticut, who might not have interaction with their peers, met and mingled in the VE. The diversity of diabetes class groups (eg, rural, suburban, and urban residents) provides opportunities for participants and educators to share information about diabetes initiatives and support services. For example, during one class, a participant from one geographic area discussed his involvement in a walking group in North Carolina that was also available in other states including New York. Subsequently, participants engaged in a lively discussion about the program. Additionally, educators had the opportunity to acquaint patients with national diabetes organizations as well as advocacy opportunities and events at the state level. Learning in a VE encourages individuals of different ages, educational levels, and cultures to engage with one another based on the shared common denominator: diabetes.
In the VE, participants often help each other based on their own experiences, answering questions and offering tips for better use of the VE. As a result, they build relationships, become invested in their environment, and develop a sense of ownership. For example, one participant shared her experience of visiting the virtual fitness center to watch the exercise videos. The participant explained to the other participants how she downloaded and saved the videos on her personal computer for later use and was able to show them the videos and downloading in real time.
Because classes held in the VE are recorded, even participants who do not attend the LIVE class have the opportunity to listen to and view the class inclusive of all the participant discussion and displayed materials. Participants who have previously attended the class have the opportunity to review it at their convenience and at their own pace. This feature, unique to the VE, increases access to DSMT enriched by all of these discussions and may improve recall of knowledge necessary for self-management. 32
Similar to other learning environments, the VE gives individuals the choice of what they share with others. However, unlike real-world learning environments, the VE provides anonymity because individuals self-represent using their avatars with a screen name. This anonymity seems to provide a comfort level among VE peers that facilitates their willingness to share facts about their diabetes and self-management that they may otherwise be hesitant to reveal. 33 For example, someone who has been diagnosed with diabetes for a number of years may be reluctant to ask a question for fear that he or she should know the answer already.
Another valuable feature of the VE typically not available for diabetes educators teaching and participants attending DSMT in real-world settings is the discussion forum. The discussion forum stimulates ongoing engagement, a sense of community, and social support among participants and serves as a repository for supplemental class materials (eg, copies of PowerPoint slides, links, handouts, or PDFs of relevant information). 20 Educators monitor forums daily, respond to participants’ posts and questions, and post a “tip of the week.” The tip of the week usually has some relevance to current events. For example, in the summer, posts might include advice on skin cancer prevention; during the holidays, tips on stress management and recipes; or during American Diabetes Month, a list of local events. These posts convey a sense of connectedness between the VE and the real world. More important, if participants are uncomfortable asking something in the LIVE class, they are free to post questions in the forum. For example, some participants used the forum to seek information about medication assistance programs and to ask for suggestions about how to make healthy food choices while living on a fixed income.
Likewise, participants can use the discussion forums to reinforce information and practice skills from class sessions. As an example, one participant posted findings from a research study that examined the accuracy of physical activity trackers and the effectiveness of trackers on increasing walking frequency. Because all participants in this study are using physical activity trackers, this research was especially relevant to the participants engaged in DSMT in the VE. The educator provided feedback about strengths and weaknesses of the research findings, which served as additional reinforcement of what was discussed in the Navigating Diabetes Research class.
The VE also provides the ability to stimulate real-world learning without the time and expense of travel. Participants can log-in for an evening class 5 minutes prior to the start of class from the privacy of their home. Nonthreatening practice and skill-building sessions can occur immediately after the didactic portion of the class. In addition, participants can log in any time to explore, practice behaviors or skills, and access resources.
On a virtual field trip, the educator and class participants can “walk” to restaurants immediately after completing a nutrition or advanced carbohydrate counting class, sit down, and practice ordering from menus in various fast food and chain eateries. The menus change monthly, so participants may “eat” at Burger King on one visit and Red Robin on the next. Asking questions of the restaurant staff while out for a relaxing dinner can be intimidating and frustrating for some individuals with diabetes. However, doing these things with a diabetes educator and group in a VE can provide practice experiences and build confidence so participants are better equipped to handle the scenario in real life.
Educators working with patients with diabetes understand that many patients dine out and eat fast food. Data from the National Health and Nutrition survey indicated that between 2007 and 2010, people consumed 11.3% of their calories from fast food. 34 Additionally, eating more meals away from home including fast food has been associated with increased body mass index and the consumption of fewer fruits and vegetables, 35 which can negatively influence glycemic management. Thus, the option of having menus from fast food and other chain restaurants in this setting gives patients opportunities to learn how to make healthful food choices.
Other examples of field trips include going to the pharmacy after the medication class, clicking on the visual image of a medication like glyburide, and then clicking on a link to the medline.gov website to read more information about the medication. Participants liked learning where to find medication information in lay language and from reputable government websites, which for some was a new and informative experience. During all activities in the VE, educators reinforced the importance of being an informed and engaged consumer.
In real-world environments, people with diabetes often receive solicited or unsolicited advice from friends, family, neighbors, coworkers, and others. Sometimes people with diabetes alter their self-care based on peer advice. 36 An advantage of the VE is that trained diabetes educators have the ability to monitor peer interaction in class and in the forums. If a myth or false information is shared, the educator can use this as a teachable moment. For example, participants have made posts about herbal supplements that have not been studied or have been found to be ineffective. In situations like this, educators can step in to provide accurate information and advise participants to discuss supplements with their health care providers.
Conclusions
Teaching DSMT in the VE presents a different set of advantages and challenges compared with other methods for DSMT delivery. Diabetes educators require guided orientation to teaching in the VE initially, but once acclimated they easily navigate this setting. Challenges include sustaining engagement, maintaining positive group interactions, and teaching without the benefit of observing students’ body language and demeanor. Benefits include reduced barriers for access to DSMT, increased diversity of patient groups, the provision of ongoing professional and peer support, and the relative anonymity afforded in the VE. VEs have been associated with the ability to create a feeling of presence in a setting that is known to enhance learning. 37
Additionally, while low health and/or numeracy issues pose challenges related to both diabetes care and related competencies,38,39 the VE provides a visually appealing presentation of information and allows ample time before, during, and after class to ask questions and problem-solve. Thus, the VE addresses print and oral literacy limitations and provides multiple opportunities for clarification and reinforcement of information.
Teaching and learning in the VE provide diabetes educators and participants with numerous options for receiving information about diabetes self-management and for understanding and reviewing that information. Using this type of media to deliver and engage persons in DSME is feasible and provides the potential for diabetes educators to reach a large population. Future research plans include examining models of dissemination and sustainability, including cost, and translating the program to meet the DSME needs of non-English-speaking people.
Footnotes
Acknowledgements
Dr Reagan was at the New York University Rory Meyers College of Nursing, and Dr Johnson (PI) at the Duke University School of Nursing when the study was conducted.
Conflict of Interest:
No competing financial interests exist.
Funding:
National Heart, Lung, and Blood Institute #1R01-HL118189-01.