
Abstract
Purpose
The purpose of this study is to describe the characteristics and technology training needs of underserved adults with type 2 diabetes mellitus (T2DM) who participated in a health information technology (HIT) diabetes self-management education (DSME) intervention.
Methods
The baseline physiological, psychosocial, and technology use characteristics for 220 adults with poorly controlled T2DM were evaluated. Intervention participants received a 1-time intervention training, which included basic technology help, introduction to the Mobile Diabetes Detective (MoDD) website and text message features, and account activation that included subject-specific tailoring. Four additional on-site sessions for participants needing computer or Internet access or technology support were made available based on need. Data regarding on-site visits for usual care were collected. Data were analyzed using descriptive statistics and bivariate analysis.
Results
The participants were predominately Hispanic and female with a baseline mean A1C of 10% (86 mmol/mol). Only half of the participants regularly used computers or text messages in daily life. The average introductory MoDD training session lasted 73.6 minutes. Following training, approximately one-third (35%) of intervention participants returned for basic and MoDD-specific technology assistance at their federally qualified health center. The most frequently reported duration for the extra training sessions was 30 to 45 minutes.
Conclusions
Training and support needs were greater than anticipated. Diabetes educators should assess technology abilities prior to implementing health information technology (HIT) diabetes self-management education (DSME) in underserved adults. Future research must invest resources in technology access, anticipate subject training, and develop new training approaches to ensure HIT DSME use and engagement.
Optimizing health-related behaviors is a fundamental aspect of effective management for people living with type 2 diabetes mellitus (T2DM). 1 To acquire the knowledge and skills needed to facilitate lifestyle changes and confidently make daily self-management decisions, formal diabetes self-management education (DSME) is recommended at diagnosis and as needed thereafter.2,3 Unfortunately, participation in DSME remains low,4,5 particularly for the medically underserved, broadly defined as those of racial/ethnic minorities 6 and low-income populations, 7 with lower health literacy, who experience higher disease prevalence, 8 poorer glycemic control, 9 and increased rates of diabetes complications. 10
Findings of a systematic review identified access, competing demands, language, literacy, and cultural differences 11 as reasons why adults with T2DM referred for DSME do not participate. One way to overcome these common barriers to DSME participation is by using health information technology (HIT) to deliver DSME in more convenient and accessible settings. 12 Pooled findings from a recent systematic review and meta-analysis of 11 randomized controlled trials (RCTs) of HIT DSME interventions in the medically underserved demonstrated that HIT DSME was efficacious; compared with controls, intervention subjects improved glycemic control at 6 months, with smaller but sustained improvement at 12 months. 13 This level of glycemic improvement is similar to that achieved following DSME delivered face-to-face in low-income minority14,15 and general population studies.16,17 Well-designed HIT interventions also have the potential to address obstacles specific to the medically underserved by tailoring DSME content to literacy, language, and culture.
While increased technology use by racial/ethnic minorities and low-income populations 18 make HIT DSME an increasingly viable way to increase DSME attendance and improve outcomes, little is known about these groups’ actual skills and ability to use cellular phone and computer technologies that may be prerequisite to engaging with DSME delivered by HIT.13,19 Few studies have reported the time and level of support required to assist underserved adults to use HIT DSME, leaving educators, clinicians, and administrators unsure of the feasibility of real-world implementation. To develop and incorporate effective HIT DSME into routine clinical use, it is critical to understand the technology capabilities of the intended patients and caregivers and the level of training required for engagement. This study addresses these gaps in 2 ways: (1) the general and technology-related characteristics of underserved adults with T2DM receiving their primary care in a federally qualified health center (FQHC), who participated in the Mobile Diabetes Detective (MoDD) trial, are described, and (2) their technology training needs and lessons learned throughout the study intervention period are reported.
Research Design and Methodology
Study Design and Randomization
This cluster RCT was conducted in eight FQHCs located in the New York City metropolitan area that are part of Clinical Directors Network (CDN) primary care practice-based research network (PBRN). 20 In a cluster RCT, the randomization occurs by groups of subjects instead of individual subjects. For this study, 4 FQHCs were randomly assigned to the technology intervention plus usual care, and 4 were randomly assigned to usual care alone. To balance the number of subjects, recruitment targets were uniform for all FQHC sites. Intervention subjects received instruction on how to use MoDD for the active intervention period of 4 weeks. After 4 weeks, intervention subjects had the option to continue MoDD use until the final follow-up visit at 12 months. The nonprofit PBRN CDN assisted with FQHC and subject recruitment, retention, data collection, and study logistics.
Control Group
The control group received usual care at their respective FQHC. Usual care included primary care services with access via provider referral to on-site extended services such as dental care, behavioral health, and chronic care management services. Exact extended services offered varied by site. Diabetes-specific services included education from a health educator or nutritionist, monitoring of glycemic control and care management, progression of complications related to diabetes, and appointments with an endocrinologist, podiatrist, and ophthalmologist.
Mobile Diabetes Detective Intervention
MoDD, a tailored HIT DSME intervention, was created by user-centered participatory design. 21 Diabetes education content for MoDD was developed by a team including diabetes educators and tailored for language, low health literacy, and culture. 22 MoDD guides the user through the process of diabetes problem solving and self-management via an interactive website accessed by an Internet-enabled computer or tablet. A text message feature allows subjects to enter daily blood glucose (BG) values (instead of via computer) and sends preset text reminders to remind subjects to check their BG values. To effectively use all features of MoDD, a cell phone with text messaging and a computer or tablet with Internet access are needed.
Subjects begin by logging their BG values before and 2 hours after meals and other key times throughout the day. Once 5 values for a given time point are recorded (eg, before breakfast), BG averages are computed. With this information, subjects identify specific time points where they have the hardest time with glycemic control and browse a set of MoDD suggestions for actionable ways to modify their self-care behaviors. Through the process of identifying self-management barriers, exploring alternatives, evaluating these options through simple experiments and goal setting, and monitoring outcomes, MoDD guides subjects through personally meaningful problem solving using principles of discovery learning. Perceptions of MoDD subjects’ user experience and engagement with MoDD have been reported elsewhere. 23
Participants
Subjects were recruited through referral by heath center providers, direct mailings, posted fliers, and by approaching adults with a T2DM diagnosis who were checked in and waiting for their appointments. Inclusion criteria required that subjects be adults (≥18 years old) with T2DM, have poor glycemic control (A1C of ≥8.0% [64 mmol/mol]), be a patient of the FQHC for at least 6 months, have had documented prior DSME at the FQHC, be proficient in either English or Spanish, own a basic cell phone, and either have access to a computer with Internet or be willing to come to the FQHC to use MoDD website features at a computer kiosk at least once a week. Adults with severe cognitive or communication impairment, pregnancy, other severe illness such as advanced-stage heart failure or cancer undergoing active treatment, or plans to leave the FQHC within the next 12 months were excluded from study participation.
The institutional review boards at Columbia University Medical Center (CUMC), CDN, and New York University Lutheran Family Health Center approved the study. Written informed consent was obtained from all study subjects in their preferred language (English or Spanish) prior to study participation. All subjects were compensated for their time, receiving $15 at the baseline visit with graduated compensation to $35 at the 12-month study visit to encourage study completion. For study-related text message fees, all subjects received $10. Finally, to assist with the increased frequency of checking BG values during the 4-week intervention period, all subjects received a 1-month supply of BG test strips.
Study Procedures
At the baseline visit, all subjects completed a demographic questionnaire, 4 diabetes-related questionnaires, a screening for depressive symptoms, and a survey of technology use habits. Information on each measure is presented subsequently. The baseline visit for subjects at FQHCs randomized to MoDD concluded with the CDN research coordinator scheduling a 1-hour individual training session. A CUMC research team member (E.M.H. or L.M.) conducted all MoDD training sessions, which included an introduction to MoDD-specific features, MoDD tailoring, and setting up a MoDD account. Figure 1 depicts the organization of each session. Spanish- and English-language versions of the training packet used for the MoDD portion of the session can be found in the supplementary appendix (http://journals.sagepub.com/doi/suppl/10.1177/0145721717737367). During MoDD account activation, subjects completed a 1-time online assessment that included readiness to change health behaviors (2 questions based on the transtheoretical model) 24 and ability to read food nutrition labels (5 questions from the Diabetes Nutrition Knowledge Survey [DNKS]). 25 Subject responses were used to tailor MoDD content and motivational messages. Activation of the subjects’ MoDD account initiated the 4-week intervention period. The CDN research coordinators recorded the duration of the training session and specific topics addressed during the session. One week after training, the CUMC researcher initiated a follow-up call with each subject to answer questions and to encourage MoDD use.
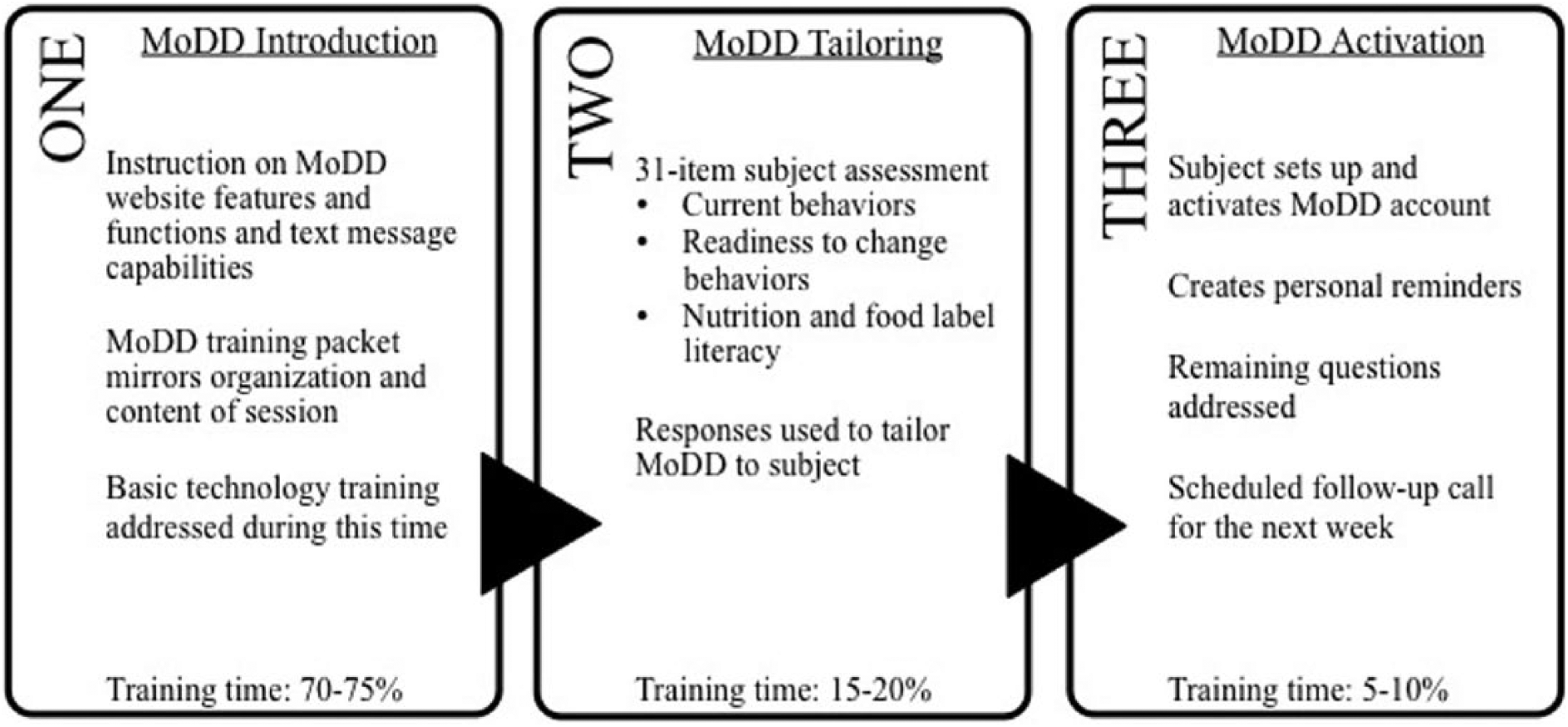
Mobile Diabetes Detective intervention training session components.
During the intervention training session, subjects were given a helpline telephone number that they could call anytime. To facilitate subject computer access, installation of a computer kiosk was planned at each intervention FQHC. However, 2 months following study initiation, coordinators received requests from subjects for more in-depth technology assistance than a kiosk or helpline could offer. To accommodate subject needs, the study protocol was modified to offer interested subjects weekly appointments with coordinators at their FQHC during the 4-week active intervention period. Research coordinators recorded the duration of all weekly subject computer use appointments using 5 categories broken into 15-minute increments for the first hour and >60 for appointments lasting 1 hour or longer. Free-text comments were recorded regarding subjects’ technology ability and the focus of activities during their session.
Measures
Measures were collected either in person using paper surveys at the subjects’ respective FQHC or via telephone interview by a bilingual research coordinator. All study measures were available in English and Spanish. For the measures not available in Spanish, a certified Spanish-language translator completed both forward and backward translations. Each measure is briefly described below.
Demographic Questionnaire
This questionnaire is a 17-item investigator-developed instrument. Items include age, race/ethnicity, primary language, education, employment, income, and living arrangements.
Problem Areas in Diabetes
The Problem Areas in Diabetes (PAID) is a 20-item survey that measures diabetes-related emotional distress using a 5-point Likert-type scale. Responses to PAID questions range from 0 to 4 (0 = no problem to 4 = a serious problem). The scale has established validity and clinical utility in adults with T2DM 26 and is sensitive to change over time. 27 Psychometric properties of the Spanish version PAID demonstrate high reliability (α = .96). 28 PAID scores were converted to a 100-point scale by multiplying the total score by 1.25. Scores of ≥40 indicate patients who need additional attention since they might be experiencing emotional burnout. 26
Summary of Diabetes Self Care Activities
The Summary of Diabetes Self Care Activities (SDSCA) is a 12-item survey about the frequency of diabetes self-care behaviors during the past week. Questions are grouped by the following self-care topics: general diet (2 questions [2]), specific diet (2), exercise (2), BG monitoring (2), foot care (1), medications (1), and smoking status (1). Mean scores per topic area were computed with scores ranging from 0 to 7. The SDSCA has established validity and reliability of its English 29 with the Spanish-language version reporting internal consistency of 0.68, individual item test-retest reliability between 0.51 and 1.00, and high levels of conceptual and content validity. 30 In this study, the SDSCA question regarding medication adherence was not used because of reported low test-retest reliability. 29
Diabetes Problem Solving Inventory
The Diabetes Problem Solving Inventory (DPSI) assesses diabetes problem-solving skills in response to 9 self-care scenarios. Following each scenario, the subject is asked how he or she would respond if faced with a similar situation. Each response is scored between 1 (a very poor strategy) to 5 (an excellent strategy). The 9 scenario scores are averaged for an overall summary score. 31 The DPSI has been validated with diverse samples as a reliable and consistent measure of individuals’ diabetes problem-solving ability. 32 An overall score ≤3 was considered as indicative of poor diabetes problem solving. Prior to study implementation, the research team and research coordinators were trained regarding scoring of scenarios.
Diabetes Self-Efficacy Scale
The Diabetes Self-Efficacy Scale is an 8-item, 10-point Likert-type scale measure (0 = not at all confident to 10 = totally confident). The scale demonstrates high internal consistency in both the English- and Spanish-language versions (0.84 and 0.85, respectively) and sensitivity to change at both 6 and 12 months. 33 Item scores are averaged to create a final score, with scores ranging between 1 and 10.
Patient Health Questionnaire–2
The Patient Health Questionnaire–2 (PHQ2) is a 2-question screening tool that identifies depressive symptoms and need for further evaluation. Final scores range between 0 and 6, with a score of ≥3 indicating that depressive symptoms are present. The PHQ2 has a sensitivity of 79% and specificity of 86% for any depressive disorder and a sensitivity of 87% and a specificity of 78% for major depressive disorder. 34
Technology Use Survey
A 26-item technology use survey was developed by the research team based on the Pew Research Center technology survey. 18 Multiple-choice questions ask about ownership of, access to, and frequency of use of cell phone, computer, and Internet technologies. Frequency of use is reported as daily, less frequently (than once a day), or never.
Medical Records Review
Laboratory (A1C, fasting lipid levels), physiologic (blood pressure), and anthropometric (height, weight, and body mass index [BMI]) values, along with medication profile, diabetes diagnosis date, and prior diabetes education type, were obtained through review of medical records. Medications were captured by brand and generic names and reported by classifications (insulin, oral diabetes agents, blood pressure, and cholesterol). Diabetes education was reported as individual or group based.
MoDD Intervention Tailoring Assessment
The MoDD tailoring assessment included 2 questions that addressed readiness to change nutrition and exercise habits. Subjects responding to both questions as “ready to take action in the next 30 days” were categorized as being ready to change health behaviors. 35 Five DNKS questions were used to assess subjects’ ability to read food labels. 25 Results were categorized into either poor (score ≤3) or adequate (score ≥4) food label literacy.
Data Analysis
All data were entered into REDCap, a secure web application for managing data. 36 All surveys were scored as described above. Data were analyzed using descriptive statistics and bivariate analyses using χ2, Fisher exact, and Student t test to examine differences between the intervention and control groups. Continuous data are presented as mean ± standard deviation and categorical variables as frequencies and proportions, unless otherwise specified. SAS 9.3 statistical software (SAS Institute, Carey, NC) was used for all data analyses.
Results
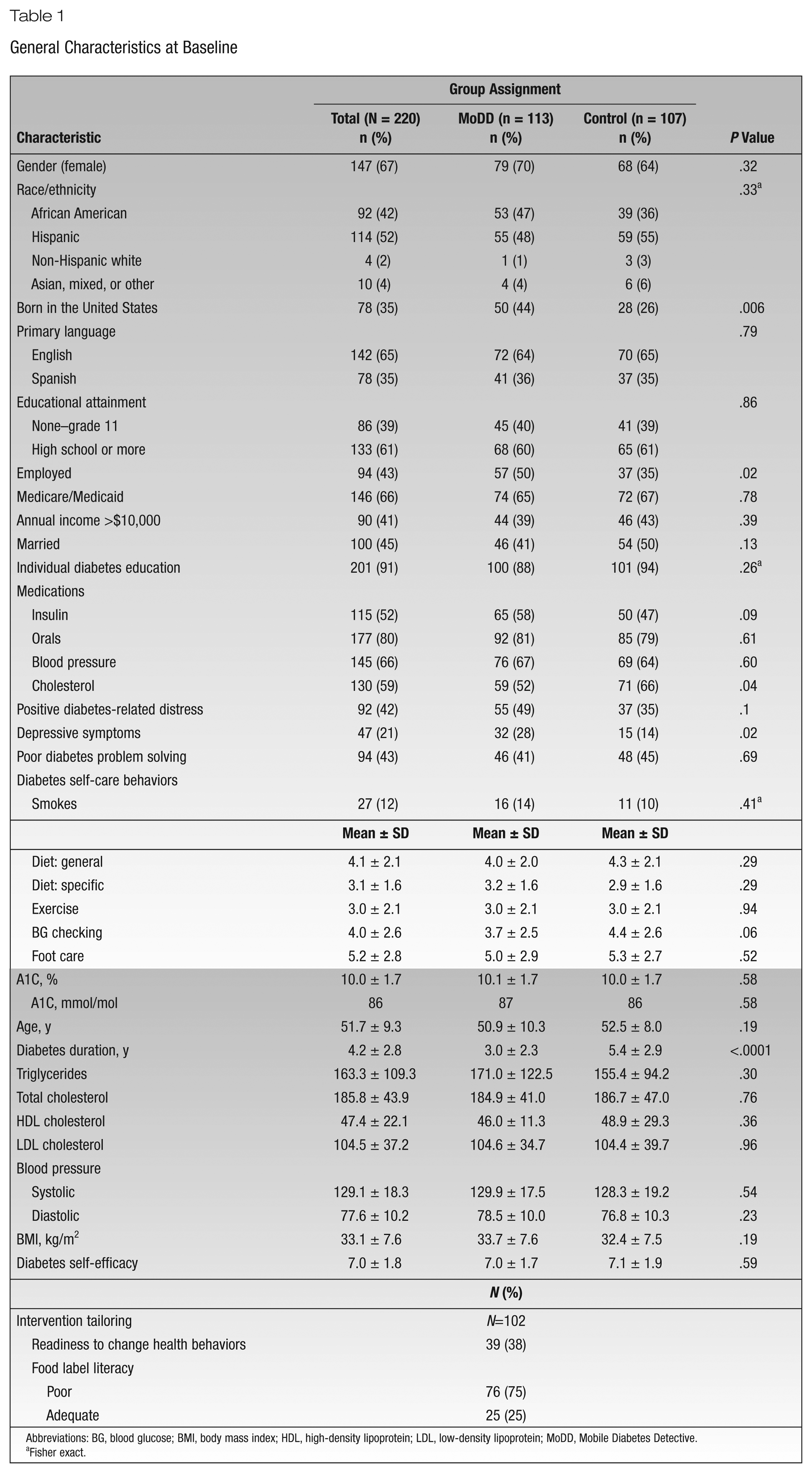
A total of 220 adults were enrolled in the study between January 2014 and April 2015. General characteristics of the sample are presented in Table 1. The sample was predominately female (67%) and Hispanic (52%), with a mean age of 51.7 ± 9.3 years. More than one-third of subjects (39%) had not finished high school, almost half (41%) reported yearly annual incomes of less than $10,000, and two-thirds (66%) received health insurance through either Medicare or Medicaid. On average, the sample had lived with diabetes for 4.2 ± 2.8 years, had poor glycemic control (A1C 10.0 [86 mmol/mol] ± 1.7%), and was obese (BMI of 33.1 ± 7.6 kg/m2). Subjects reported high diabetes self-efficacy (7.0 ± 1.8), and 1 in 5 (21%) reported depressive symptoms. Forty-two percent of subjects demonstrated poor diabetes problem solving.
General Characteristics at Baseline
Abbreviations: BG, blood glucose; BMI, body mass index; HDL, high-density lipoprotein; LDL, low-density lipoprotein; MoDD, Mobile Diabetes Detective.
Fisher exact.
Compared to the intervention group, control subjects had lived with diabetes longer (5.4 ± 2.9 vs 3.0 ± 2.3 years, P < .0001). Fewer control subjects reported depressive symptoms (14% vs 28%; P = .02), were born in the United States (26% vs 44%; P = .006), and had either part- or full-time employment (35% vs 50%; P = .02). A greater proportion of the control group was prescribed medications for lipid control (66% vs 52%; P = .04).
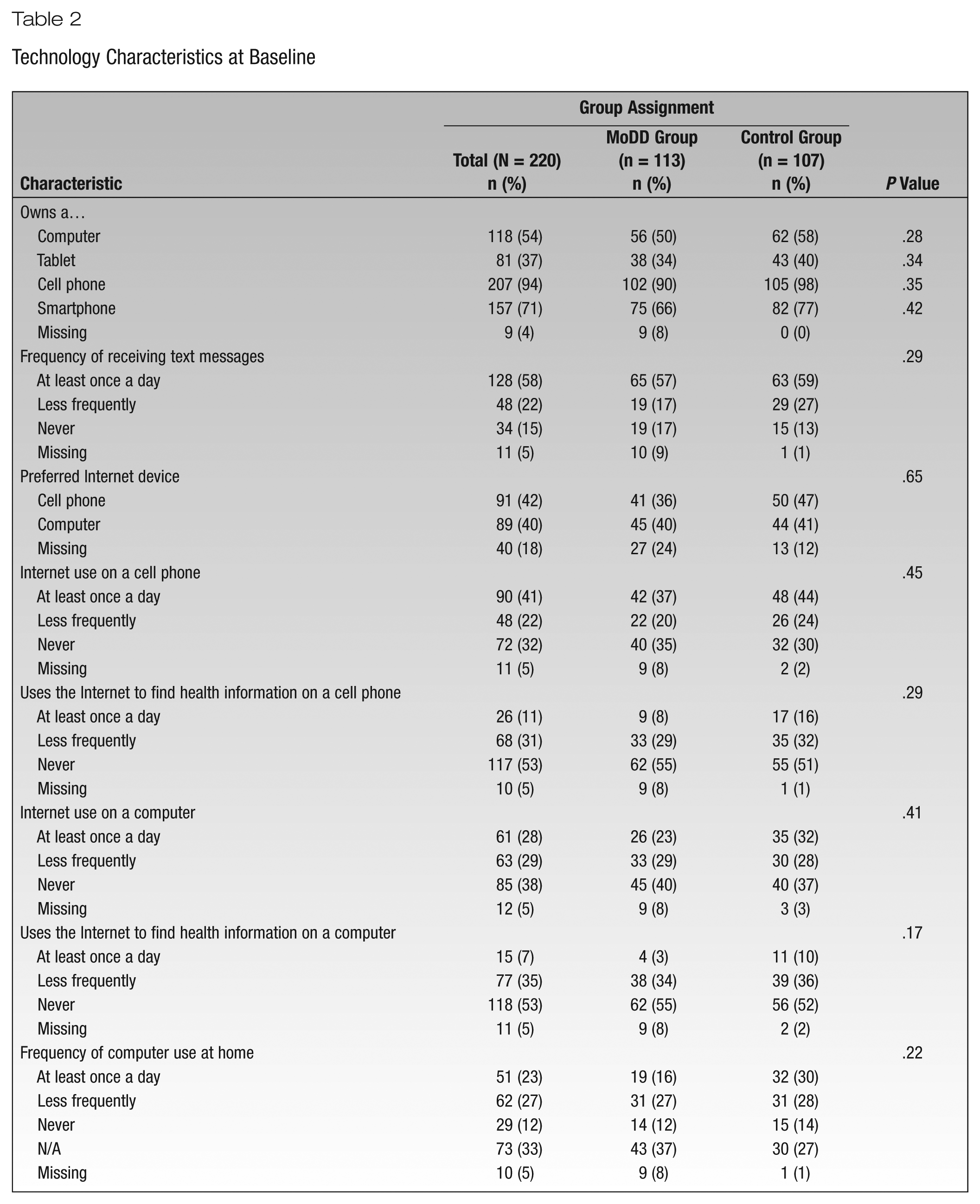
Technology use characteristics of the sample are depicted in Table 2. Technology ownership was high, with most of the sample owning a cell phone (94%) and/or a smartphone (71%). Approximately half (54%) owned a computer. Most reported receiving text messages at least once a day. Cell phones were reported as the most preferred device to access the Internet, with 41% of subjects doing so at least once a day. Using the computer to access the Internet was less frequent, with more than one-third (38%) reporting never accessing the Internet this way. Most (88%) reported rarely or never using the Internet to find health information.
Technology Characteristics at Baseline
Most intervention subjects (90%, n = 102) completed the initial MoDD intervention training session. The average training session was 73.6 ± 21.3 minutes. Responses to the tailoring questions demonstrated that most (75%) subjects had difficulty interpreting a food label, and approximately one-third (38%) reported readiness to change their health behaviors. Most subjects who completed training (85%) were successfully reached for their follow-up call.
Approximately one-third (n = 35) of intervention subjects returned to the FQHC at least once to obtain additional help or use the computer to access the MoDD website (Figure 2). Of the subjects who came for at least 1 extra appointment, 40% came only once and 37% came 3 times. Figure 3 illustrates the length of the sessions. Duration during the first and fourth sessions most commonly lasted between 15 to 45 minutes. The average duration for the second and third sessions was longer, with coordinators reporting more visits lasting 45 minutes to more than an hour. The most frequently reported training session duration overall was 30 to 45 minutes (27%).
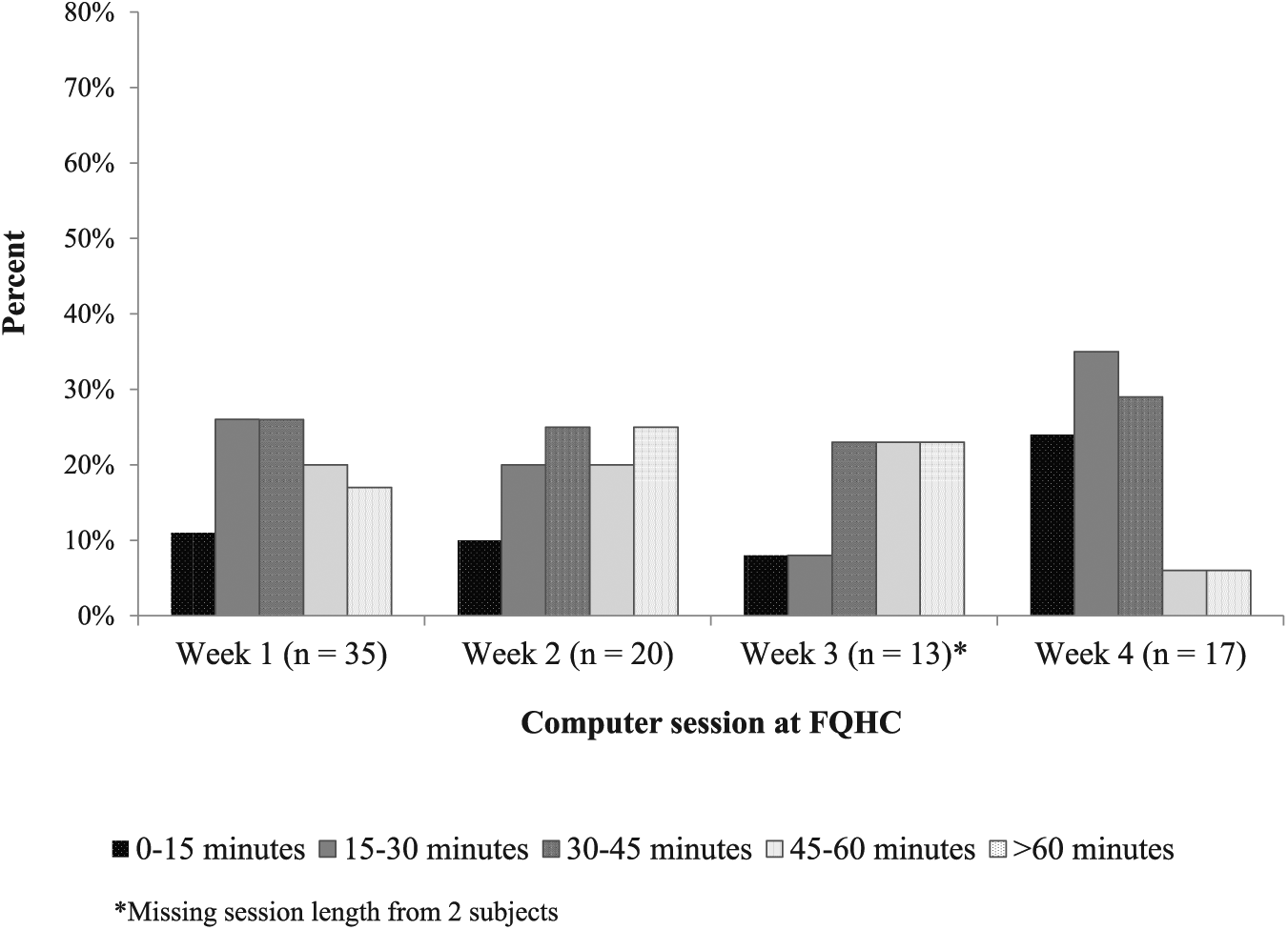
Length of Mobile Diabetes Detective computer sessions.
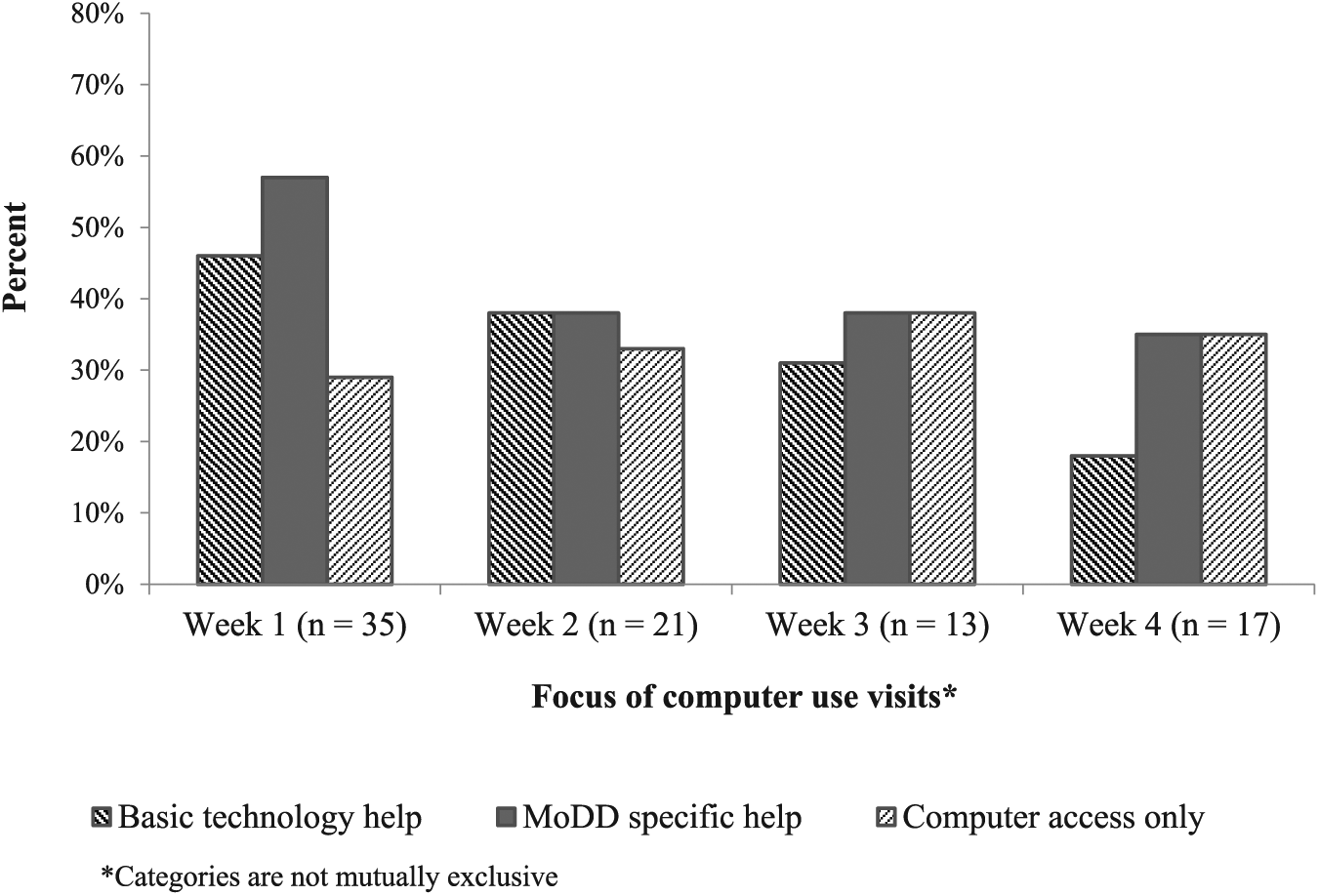
Type of help needed during computer sessions.
Figure 4 shows the most common activities completed during the session. Subjects frequently needed both basic technology and MoDD specific help. At the first session, subjects required help with basic tasks (eg, opening an Internet browser, entering the website URL, using a mouse, etc) and specific help using the MoDD intervention website (eg, selecting a goal, setting reminders, etc). Over the 4-week period, the need for basic help diminished, and subjects’ ability to work alone increased. Across visits, subjects spent most of their time logging their BG values and setting goals. Setting reminders occurred the least often.
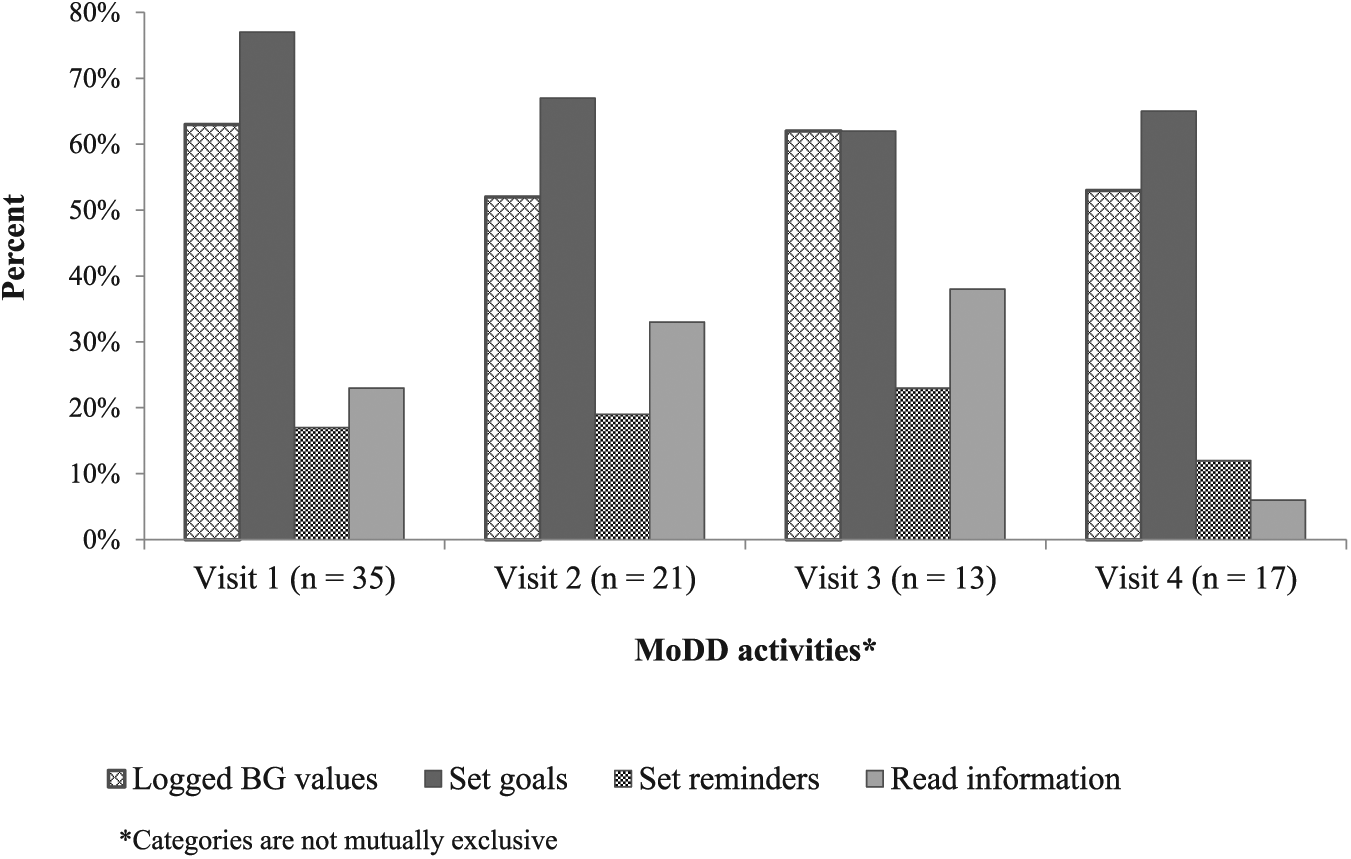
Focus of Mobile Diabetes Detective use during computer sessions.
Discussion
This study presents baseline demographic, clinical, and technology use characteristics from 220 urban underserved adults with poorly controlled T2DM enrolled in the MoDD RCT and describes their technology training and access needs during the intervention phase. At baseline, subjects reported high technology ownership and moderate technology usage. Surprisingly, this did not translate into subjects’ having sufficient skills to independently use MoDD after a 1-time intervention training session, necessitating the creation of additional computer sessions at the FQHCs with a research coordinator. Over the 4-week active intervention phase, subjects’ technology abilities improved, with many transitioning from needing basic help to eventually requiring help only with MoDD or even working independently.
While reports of technology use or training needs of underserved adults are limited, our findings are consistent with the literature. Czaja and colleagues 37 examined the usability of an online personal health record (PHR) in a sample of 54 subjects with low health literacy. While most (94%) of these urban, adult subjects reported prior computer/Internet experience, used a computer multiple times a week (75%), and had Internet access at home (63%), only 20% of subjects regularly used the Internet to get health information. Similar to our study findings, after 1 training session on basic technology skills and an introduction to the PHR, subject ability and PHR task performance was low, showing the need for further training.
Starren and colleagues 38 examined the installation of the home telemedicine unit (HTU) by registered nurses (RNs) in a telemedicine intervention with a sample of 1665 underserved elders with diabetes. A sample of 5 RNs was interviewed about the HTU installation process and any patient-related factors affecting the session. Results showed that RNs perceived patient education and training to be the primary focus of their visits and the most critical factor to improving the patient experience. RNs also described subjects as wanting more education and training. 38 These findings resulted in the development and evaluation of 3 HIT training approaches (unassisted using a manual with written directions only, face-to-face using a manual, or assisted by telephone with the manual) in a sample of 109 subjects who requested extra HTU assistance. Face-to-face training with the manual was preferred. 39 A final study explored the feasibility of a remote HTU training approach in 2 subjects who had previously requested extra assistance. The researchers found this approach resulted in a measureable change in subjects’ ability to complete technology tasks required for intervention participation. 40 Collectively, these studies reinforce our findings that despite ownership and prior technology experience, multiple technology training encounters are needed for members of communities with less HIT experience. They also present different approaches to provide HIT training to the underserved and, along with the MoDD training activities, provide preliminary insights into various ways to deliver technology training.
By identifying technology use behaviors of the underserved, educators and decision makers are better prepared to adopt relevant HIT DSME and anticipate and address training needs. The technology characteristics of our sample illustrate the growing ownership, use, and comfort of minorities and low-income adult populations with cell and smartphone technologies. In its next iteration, MoDD could leverage this opportunity by providing a companion application (app) to be downloaded on smartphones. However, planning for tailored and ongoing hands-on training in advance remains an integral step to ensure optimal use.
The lessons learned during this study emphasize the importance of basic technology training when implementing an HIT intervention to groups just starting to engage with daily technology use. MoDD study inclusion criteria regarding technology access/ownership were believed to be sufficient to ensure the sample entered the study with adequate technology access and ability. Therefore a 1-time intervention training session augmented by telephone support was thought to be able to support MoDD engagement; however, this was not the case. Once the need for further training became clear, the research team responded quickly by implementing extra assistance—onsite computer sessions at the FQHC. While these sessions worked well for some subjects, barriers to participation were similar to those identified for in-person DSME. Subjects had to come to their FQHC and negotiate their competing obligations and priorities to participate. Research coordinators offered sessions on weekdays during hours the FQHCs were open (often from 8
Collectively, these findings highlight the importance of anticipating the technology access and training needs for underserved adults to successfully use HIT self-management interventions. A clear lesson learned from the MoDD study is that technology ownership does not indicate continuous access or a level of technology ability for underserved populations. This points to the importance of offering technology access and multiple training encounters to support HIT DSME use. Future research employing HIT interventions targeted for the underserved should describe subject training needs and training approaches used to identify and develop best practices.
Limitations
This study has several limitations. These data do not reflect a representative sample of all low-income, racial/ethnic minority adults with T2DM and may not be generalizable to other settings. Many of the measures relied on self-report, which always has a potential for bias or inaccuracy. The technology measure created for this study was investigator developed and not previously validated. Finally, information was not collected for subjects who did not attend the weekly technology training sessions; information on why these subjects did not participate would have added meaningfully to the analysis. However, this study has strengths. This is the first article to describe technology ownership, usage, and ability in a diverse sample of underserved adults with T2DM enrolled in an HIT DSME intervention and will provide guidance for implementation of HIT interventions in diverse low-health literacy populations.
Conclusions
This study contributes to the growing body of evidence that points to the ability and needs of the underserved, who often face increased diabetes health disparities, to be successful in adopting and implementing HIT DSME interventions. These findings provide valuable insight regarding what training and technical resources are needed for members from these communities to be prepared for active use and engagement with HIT DSME. Future research needs to expand this knowledge by reporting the technology usage habits and abilities of these populations along with developing technology training approaches and solutions to develop best practices.
Implications for Diabetes Educators
Evidence has shown that HIT DSME interventions for the medically underserved improve glycemic control similar to in-person DSME and have the potential to increase access, reach, and impact. 13 Diabetes educators play a crucial role in the selection and implementation of HIT DSME. This study shows the importance of having diabetes educators continually assess their patient populations’ technology ownership, use, and ability to identify well-suited technology to augment current education/services. This will also allow diabetes educators to anticipate resources required for technology training and select an appropriate training approach.
Footnotes
Acknowledgements
The authors would like to thank CDN Research Coordinators Sandra Monroy, Idara Umoh, Santa Jimenez, Genevieve Lalanne, Carrie Goodman, Jennifer Rodriguez, and Ajeenah Haynes for their hard work and assistance. The authors also thank Brownsville Multi-Service Family Health Center, Joseph P. Addabbo Family, Metropolitan Family Health Center, Morris Heights Community Health Center, NYU Lutheran–Caribbean Family Health Center, NYU Lutheran–Family Physician Health Center, NYU Lutheran–Park Slope Health Center, and NYU Lutheran–Sunset Park Health Center.
Funding:
This work was supported by the National Institute of Nursing Research Training grant NINR T32NR007969 and the National Institute of Diabetes and Digestive and Kidney Diseases grant R01DK090372
Supplementary material is available online with this article.
Compliance With Ethical Standards
All procedures performed with human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study prior to participation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.