
Abstract
Purpose
The purpose of this study was to examine the feasibility and efficacy of the Diabetes Community Care Ambassador (DCCA) Program, a novel medical-legal community intervention designed to support high-risk youth with type 1 diabetes.
Methods
Study eligibility criteria: ages 3-19 years, A1C ≥8.5% (≥69 mmol/mol) and/or recent diabetic ketoacidosis hospitalization, type 1 diabetes duration ≥1 year, and English- or Spanish-speaking. Eighty-nine youth and their caregivers participated in the 9- to 12-month intervention, which included diabetes education and support through 3 home visits, 1 to 2 school visits, and phone support from a lay health worker, as well as legal support from a medical-legal partnership attorney. Feasibility was assessed; change in A1C was compared in a linear mixed model.
Results
Of the 89 DCCA Program participants, 80% completed the program, with the majority of participants rating their DCCA favorably. Sixty-two percent reported ≥1 unmet legal need, of whom 29% accepted legal counsel. Youth enrolled in the DCCA Program demonstrated an improvement in glycemic control as their mean A1C decreased from 9.71% (83 mmol/mol) at the start of the program to 9.40% (79 mmol/mol) at the end of the intervention period (P = .03). Participants with public health insurance experienced the greatest differential A1C reduction (9.79% to 9.11%, 83 mmol/mol to 76 mmol/mol).
Conclusions
The DCCA Program represents a promising intervention for improving care of high-risk youth with type 1 diabetes. A significant proportion of caregivers of youth reported having an unmet legal need. Participants remained highly engaged and demonstrated improved glycemic control, particularly youth with public health insurance.
The current model for ambulatory diabetes care to children and adolescents has evolved to include a comprehensive multidisciplinary diabetes team of medical providers, diabetes educators, dietitians, psychologists, and social workers with training and expertise in both diabetes and pediatrics.1,2 Despite quarterly visits with a multidisciplinary care team for reevaluation of diabetes management and annual visits focused on a review of dietary knowledge and psychosocial needs, only a minority of youth with type 1 diabetes achieve recommended glycemic targets (A1C <7.5%, <58 mmol/mol),3-5 highlighting the need for innovative solutions to address barriers around diabetes self-management and adherence to treatment regimens.
Traditional pediatric diabetes care in the US is focused on providing diabetes education and self-management assessment primarily in the clinical setting or over the phone. Rarely, if ever, are diabetes management skills assessed and taught in the settings in which they will actually be performed—at home, at school, and in the community—thereby limiting the collaboration between patients, families, school personnel, and diabetes care teams. In addition, social determinants, which are known to greatly influence health, are not consistently addressed by the traditional medical care model.6,7
Different strategies have been employed to overcome limitations of traditional diabetes care. Nonmedical case management has been shown to have some success in increasing clinic visit attendance and reducing health care utilization in youth with diabetes.8,9 Similarly, the use of lay health workers (LHW) has been found to be a promising strategy for improving diabetes outcomes by addressing both individual- and community-level needs.10,11 The majority of LHW diabetes studies enlisting and training community workers to engage with patients and families have focused on the adult diabetes population, with few prior studies addressing the unique needs of children with diabetes. 12
Given that many of the social determinants of health are rooted in legal problems that are potentially remediable, 13 there have also been recent efforts to align legal support and health care through medical-legal partnerships (MLP) to help communities and health care institutions lower barriers to basic needs and combat health disparities.14,15 While MLP support has been shown to be beneficial in the management of chronic disease such as asthma and sickle cell disease, there have been no MLP studies in pediatric diabetes. 16
We designed the Diabetes Community Care Ambassador (DCCA) Program to provide personalized care, beyond traditional care, that worked to address home, school, and medical-legal needs to promote optimal diabetes self-management. The first aim of this study was to evaluate the feasibility and acceptability of a novel diabetes medical-legal community care model that incorporates LHWs to provide home support, school support, and care coordination as well as an MLP attorney to support the identification and management of unmet legal needs. The second aim of this study was to determine the effect of the DCCA Program on glycemic control and diabetes-specific quality of life (DQOL). We hypothesized that participants in the DCCA Program would have a lower A1C and that both youth and their caregivers would report improved youth DQOL compared to the comparison group.
Research Design and Methods
English- or Spanish-speaking participants with type 1 diabetes (aged 3-19 years) with a duration of type 1 diabetes ≥12 months and suboptimal glycemic control, defined as A1C ≥8.5% (≥68 mmol/mol) and/or ≥1 episodes of diabetic ketoacidosis in the last year resulting in hospitalization, were recruited from the population served at the Seattle Children’s Diabetes Clinics who lived in 3 surrounding Washington State counties. Since the LHWs, known in this study as DCCAs, did not have formal or paraprofessional training in the management of psychological disorders, patients with active psychiatric illness or clinical depression were excluded. To strengthen the feasibility study design, patients and families who declined to participate in the DCCA Program were reapproached after DCCA Program enrollment was complete to participate in the traditional care group and served as a comparison group for the study while receiving traditional diabetes care. The Seattle Children’s Research Institute Institutional Review Board approved the study procedures. Both the youth and caregiver were required to consent to and participate in the intervention.
The Diabetes Community Care Ambassador Program
The DCCAs carried out diabetes assessments and education in both the home and school settings. DCCAs were hired from each of the 3 counties from which participants were recruited and underwent more than 100 hours of diabetes and medical-legal training, which included: (1) completing a multiweek diabetes curriculum, (2) shadowing multiple members of the traditional diabetes care team, (3) completing medical-legal training, and (4) shadowing on a statewide intake line and juvenile court hearings.
The DCCAs conducted 3 primary activities: (1) 3 home visits between clinic visits to address participants’ specific self-management goals and assessment of unmet legal needs, (2) 1 visit with school personnel plus a second in-person visit or phone call 1 month later depending on needs of participant and school, and (3) care coordination, which included phone check-ins 2 weeks after home visits and clinic visit reminders as well as support as needed between visits based on participant’s needs and preferences via email or phone. A representation and timeline for the intervention is shown in Figure 1. Home visits, school visits, and phone support continued for 9 to 12 months, with the end of the intervention occurring when a participant had their diabetes clinic visit after their final home visit.
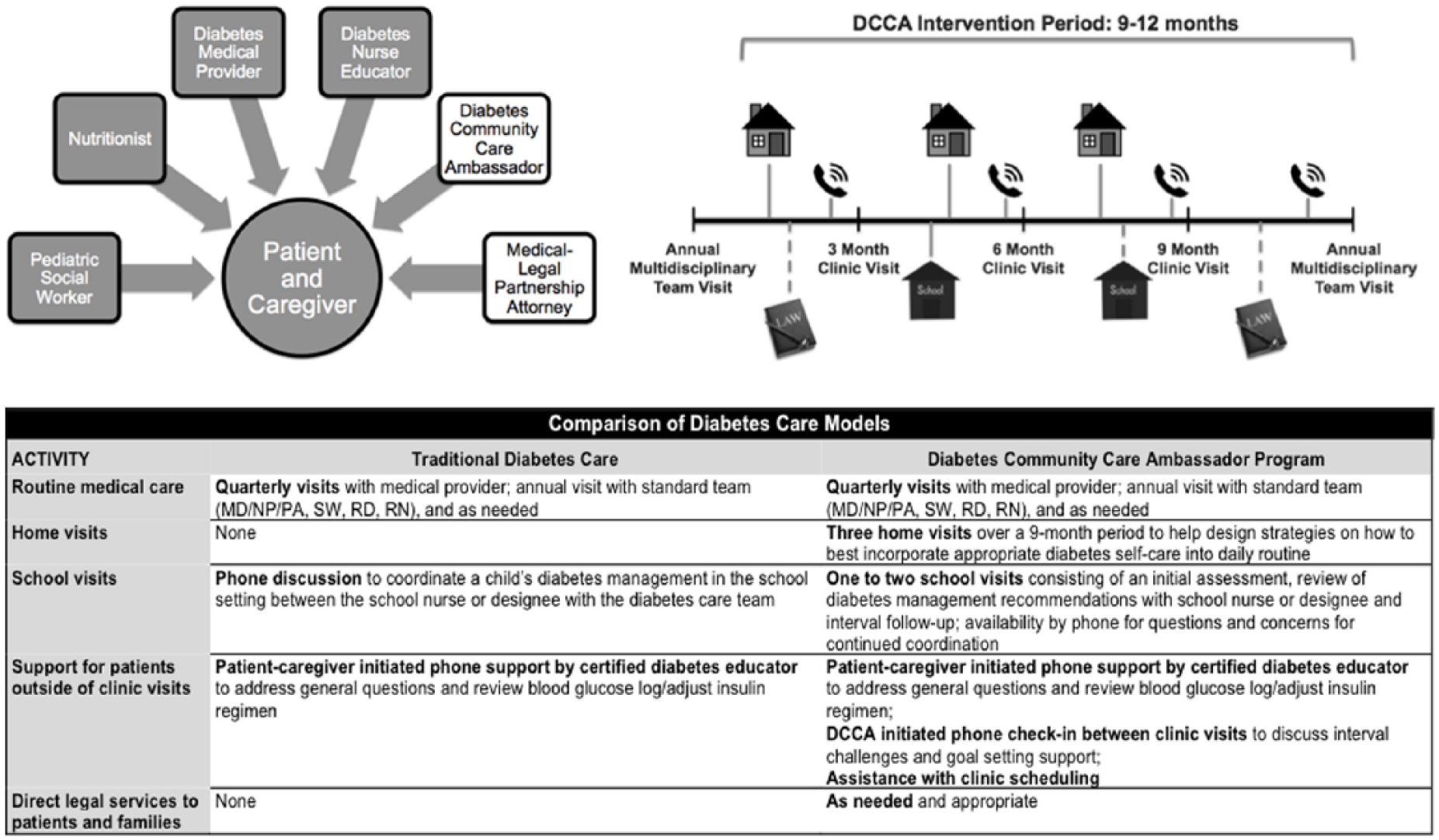
The Diabetes Community Care Ambassador diabetes care team and intervention timeline outlining frequency of home, school, phone, and medical-legal support between clinic visits.
Home Visits
At home visits, DCCAs carried out assessments of diabetes self-management, home environment, and physical activity. Each visit concluded with an identification of key barriers and goals to improve management around the home, identification and distribution of resources and education that were most needed, and confirmation or scheduling of upcoming clinic appointments. After a home visit, DCCAs generated a report of the home visit evaluation highlighting self-care goals that were established and questions for the upcoming clinic visit, which were shared with the youth’s primary diabetes team members.
School Visits
DCCAs conducted an assessment of school diabetes management by meeting in person with a school nurse or designee. School diabetes care evaluation included a review of all diabetes care needed while the child was in school and identification of possible improvements in activities or school schedule that might improve health, including a walk-through of the school lunch and insulin dosing scenario. DCCAs also distributed up-to-date information about diabetes and worked to facilitate communication between the school nurse or designee, the family, and the diabetes care team at Seattle Children’s Hospital.
Medical-Legal Support
The DCCAs were also trained by an MLP attorney to identify home- or school-related legal issues that families may be facing and strategies for assisting families in self-advocacy. Unmet legal needs were also assessed with the Washington MLP questionnaire examining items such as income supports, housing, health insurance coverage, and education. The MLP attorney was available for the DCCAs for consultation purposes. Any outstanding or complex legal issues that could not be addressed by the DCCA or the traditional diabetes care team were referred to the MLP attorney with the family’s consent. The MLP attorney would then provide direct free legal services, ranging from advice and counsel to representation in state court or administrative hearings, depending on the needs of the family.
Measures
Feasibility
Participant refusal, recruitment, and retention were monitored, as were the number of MLP legal referrals offered and accepted by participants. Completion of the DCCA Program was defined as participation in all 3 home visits and recommended school visit(s).
Acceptability
Caregiver experience of working with a DCCA was assessed at the end of the study with overall rating measures and composite trust and communication measures from the validated Consumer Assessment of Healthcare Providers and Systems (CAHPS) survey. 17
Legal Need
Unmet legal needs were assessed with the Washington MLP Questionnaire, which asked caregivers to report the degree of difficulty with income support, housing, health insurance coverage, and education: (1) none, (2) a little, (3) some, (4) a lot. An unmet legal need was defined as a caregiver response of some or a lot to 1 or more items.
Glycemic Control
A1C was collected at routine diabetes clinic visits. The A1C level prior to a DCCA Program participant’s first home visit was used as the baseline A1C. A1C levels measured in clinic after each home visit were recorded for DCCA participants. For the comparison group, baseline A1C was defined as the A1C measurement recorded prior to consent.
Quality of Life
Participants completed the validated 28-item multidimensional Pediatric Quality of Life Inventory 3.0 Type 1 Diabetes Module (Diabetes PedsQL) at baseline and between the 9- to 12-month clinic visits. 18 The Diabetes PedsQL uses a Likert-type response scale (scale, 0-100), with higher scores indicating fewer symptoms or problems, and was completed by both the caregiver and youth ≥10 years old. The youth survey was a self-report of youth quality of life; the caregiver survey was a proxy report of youth quality of life.
Covariates
Participant age, gender, insulin regimen, race/ethnicity, duration of diabetes, and health insurance at time of study enrollment were abstracted from the electronic medical record by trained research staff.
Statistical Analysis
Rates of refusal, enrollment, and retention were summarized, along with DCCA Program completion rate and MLP referral and acceptance rates for the intervention group. Caregiver experience means and standard deviations were calculated.
Primary outcomes (a) A1C and (b) diabetes quality of life were entered into separate linear mixed models to assess group differences in change from baseline (time by group interaction). The model was adjusted for covariates (age, insulin regimen, duration of diabetes, health insurance, and baseline A1C). Repeated measures were accommodated through a random participant effect and an autoregressive error structure. Estimated mean change from baseline and associated 95% confidence intervals were obtained from the models for intervention and comparison groups.
To assess whether participants responded differently to the DCCA Program based on each of the covariates, a series of post hoc analyses was conducted in which the analyses were stratified by each covariate and qualitative differences examined.
Analyses were conducted using Stata 12 (StataCorp), and a 2-sided significance level of P ≤ .05 was considered significant.
Results
Enrollment and Retention Rates
Of 342 eligible youth with type 1 diabetes approached, 109 consented for the DCCA Program (Figure 2). Thirteen percent of interested participants were excluded from the study because of existing mental health conditions or clinical depression identified on PHQ-9 screening. DCCA Program participants were reflective of the Seattle Children’s diabetes patient population (three-fourths white race, one-third public health insurance), and there was no difference in race/ethnicity or health insurance type in patients that consented or declined participation in the study.
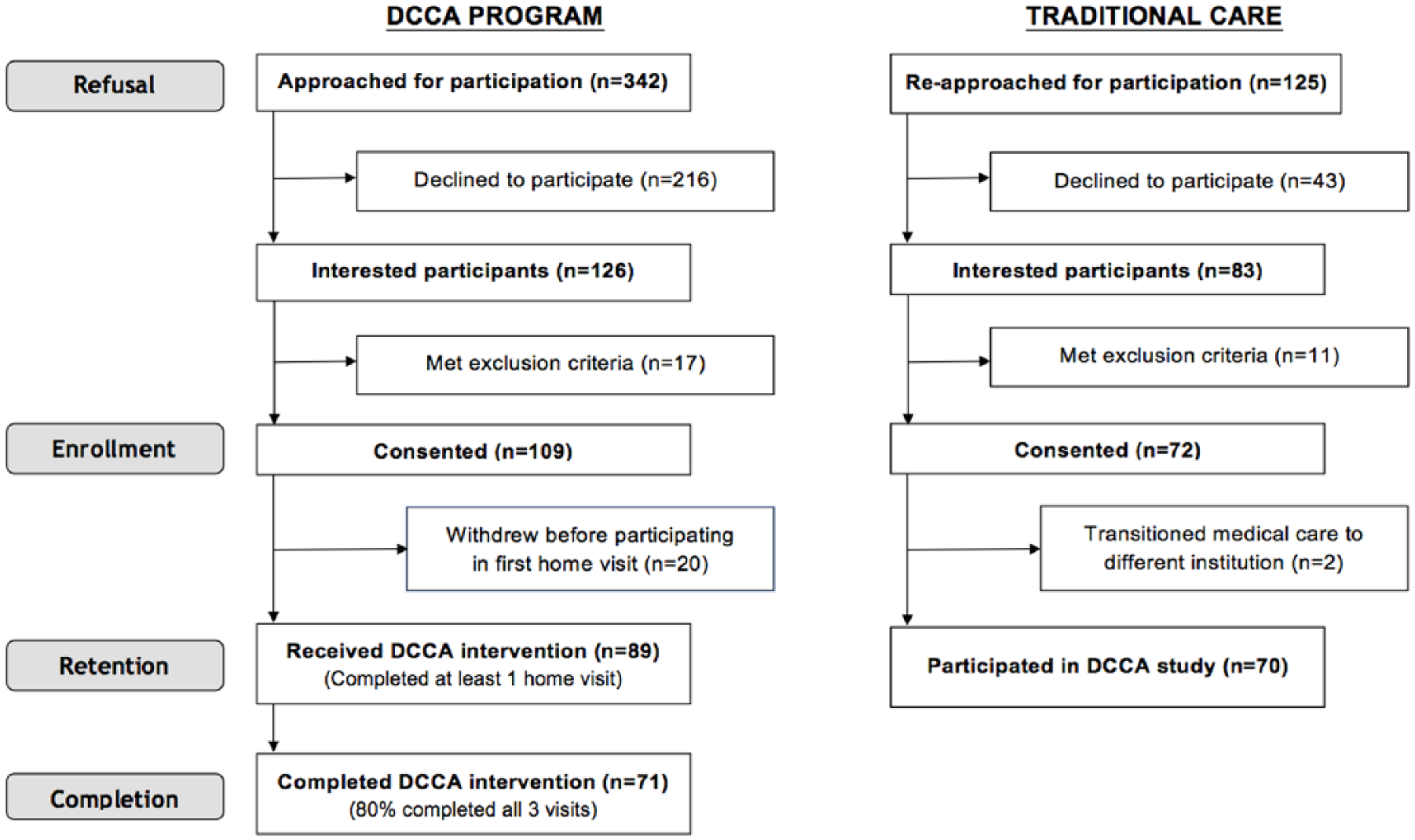
Study enrollment flow chart.
Eighty-nine of the participants who consented to participate in the DCCA Program completed at least 1 home visit with a DCCA. Reasons for not participating in DCCA Program after consent included potential time commitment (n = 6), new family issues such as illness (n = 3), youth no longer interested in participating (n = 3), housing change after consent (n = 2), other caregiver uncomfortable with home visit (n = 1), and lost to follow-up (n = 5).
Of the enrolled participants who met with their DCCA, 80% (n = 71/89) completed the program. Reasons for not completing the program included time commitment (n = 7), having enough support (n = 2), youth no longer interested in participating (n = 2), referral to child protective services (n = 1), and lost to follow-up (n = 6).
Acceptability of Diabetes Community Care Ambassadors
Seventy percent of caregivers (n = 50) who finished the DCCA Program completed the CAHPS survey at the end of the intervention period. Of those respondents, caregivers rated their DCCA highly on a 0 to 10 scale (9.74 ± 0.47 SD) and felt they could trust their DCCA (9.65 ± 0.74 SD). On a 4-point composite scale, caregivers felt DCCAs communicated effectively with participants (3.87 ± 0.23 SD) and were caring (3.84 ± 0.22 SD). Most caregivers (96%, n = 48) stated that they would “definitely recommend” their DCCA to other families with children and adolescents with type 1 diabetes.
Medical-Legal Partnership Referrals
Of the 89 participants enrolled in the DCCA Program, 62% (n = 55) reported at least 1 unmet legal need at the beginning of the intervention (1 unmet legal need = 20, 2 unmet legal needs = 17, ≥3 unmet legal need = 18). Twenty-nine percent of caregivers (n = 16) who were offered an MLP referral accepted legal counsel. Two additional participants who did not report unmet legal needs on the WA MLP Questionnaire also worked with an MLP attorney.
Education concerns were a commonly reported unmet legal need, and half of direct legal services provided addressed school issues (eg, districts failing to provide emergency diabetes care, truancy dispute). The MLP attorney provided legal representation beyond advice and counsel most often in the areas of education, including a successful appeal of a finding of truancy based on a district’s failure to excuse diabetes-related absences and requesting public accommodations under the Americans with Disabilities Act.
Glycemic Control
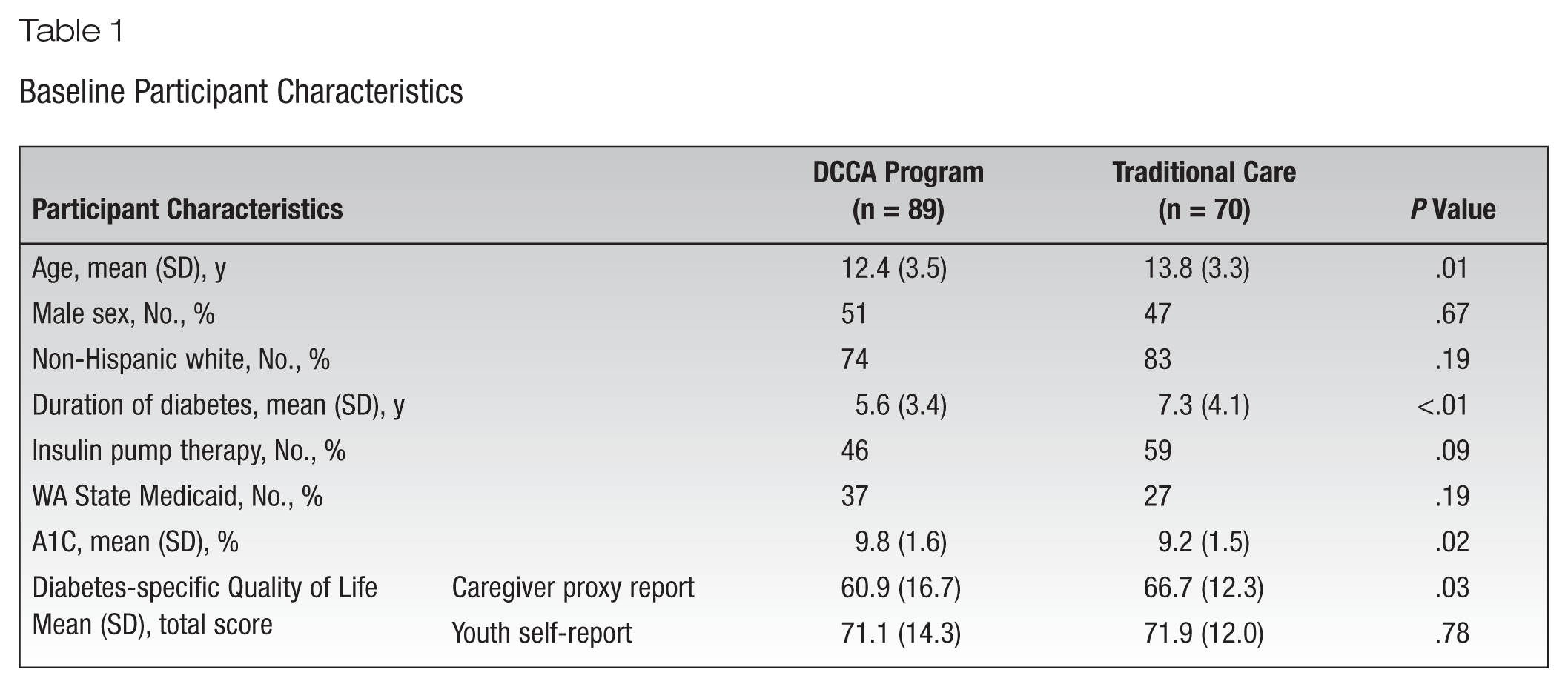
A total of 159 participants (89 DCCA Program, 70 traditional care) were included in the analyses (Table 1). Compared with participants in the traditional care group, participants enrolled in the DCCA Program were younger (P = .01), had a shorter duration of diabetes (P < .01), and had a higher baseline A1C (P = .02).
Baseline Participant Characteristics
Participants enrolled in the DCCA Program exhibited significantly greater reduction in A1C over the course of the study compared to the traditional care group (P < .01). The adjusted mean A1C for the DCCA Program participants improved from 9.53% (81 mmol/mol) to 9.22% (77 mmol/mol) (difference = −0.31%, 95% CI, –0.58 to –0.04, and –3.4 mmol/mol, 95% CI, –6.3 to –0.4) while the adjusted mean A1C for the traditional care group worsened from 9.39% (79 mmol/mol) to 9.66% (82 mmol/mol) (difference = 0.27%, 95% CI, −0.03 to 0.57, and 3.0 mmol/mol, 95% CI, −0.3 to 6.2) over a similar time period.
DCCA Program effectiveness at improving A1C differed qualitatively based on insurance type (Figure 3). Among participants insured by WA Medicaid, the adjusted mean A1C for those enrolled in the DCCA Program improved from 9.56% (81 mmol/mol) to 8.89% (74 mmol/mol) (difference = −0.67%, 95% CI, –1.14 to –0.21, and –7.3 mmol/mol, 95% CI, –12.5 to –2.3) compared with an adjusted mean A1C in the traditional care group that changed from 9.45% (80 mmol/mol) to 9.75% (83 mmol/mol) (difference = 0.30, 95% CI, −0.26 to 0.86, and 3.3 mmol/mol, 95% CI, −2.8 to 9.4). The change in glycemic control was statistically significant between participants with public insurance in the 2 groups (P = .02). There was no significant difference in change in glycemic control, however, between participants with private insurance in the 2 groups (P = .13). Among participants with private health insurance, the adjusted mean A1C in participants enrolled in the DCCA Program changed from 9.50% (80 mmol/mol) to 9.42% (79 mmol/mol) (difference = −0.08%, 95% CI, –0.39 to 0.24, and −0.9 mmol/mol, 95% CI, −4.3 to 2.6), while the adjusted mean A1C in the traditional care group changed from 9.38% (79 mmol/mol) to 9.63% (82 mmol/mol) (difference = 0.25%, 95% CI, –0.10 to 0.61, and 2.7 mmol/mol, 95% CI, −1.1 to 6.7). No differences in intervention effectiveness for improving glycemic control over time were found to be associated with gender, race/ethnicity, age, duration of diabetes, or insulin regimen. In addition, there were no significant differences in treatment effect by covariate strata.
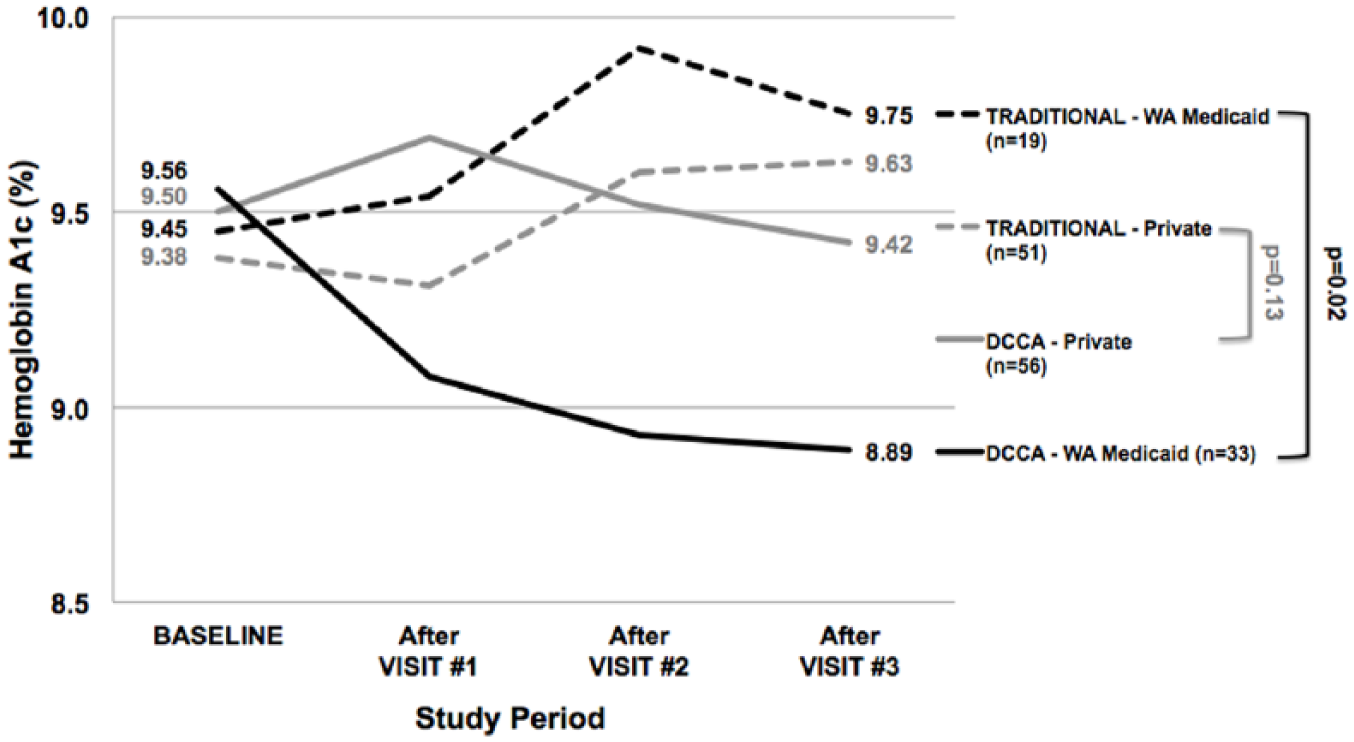
Change in mean adjusted A1C estimated from a linear mixed model stratified by intervention group and insurance type.
Discussion
This study uniquely demonstrates the feasibility of integrating both a DCCA and an MLP attorney into a diabetes care team and successfully providing home-based assessment and education, school care coordination, and medical-legal support. To our knowledge, this is the first study to incorporate both a LHW and an MLP attorney into a pediatric diabetes care team. Further, the DCCA Program represents a promising intervention to support high-risk youth with type 1 diabetes and their families as participants who worked with a DCCA experienced improved glycemic control, particularly those children and adolescents with public health insurance.
The enrollment rate for the DCCA Program suggests that the intervention is feasible, though the lower than anticipated number may reflect the intensity of the intervention, including caregiver and youth comfort with participating in home visits. Similarly, many eligible patients may have been hesitant about school visits since a sizeable percentage of youth choose not to disclose their diabetes condition at school. 19 Given that approximately 1 in 8 eligible families interested in participating in the DCCA Program were excluded due to mental health comorbidities known or identified through PHQ-9 screening, the inclusion of potential psychological support in future studies of this proof of concept care model should be considered.
The high program completion rate (80%) after the youth and caregiver had their first home visit with their DCCA indicates that participants found the additional home and school diabetes support and care coordination beneficial. This, along with the overwhelmingly positive caregiver experience, suggests that DCCAs working in the community can be effective members of the diabetes care team. The results of this study further support the use of community health workers and lay leaders as a means to overcome disparities and assist in the delivery of diabetes self-management education, as well as diabetes support services. 1
In contrast to the traditional model of diabetes care, the DCCA model worked to better identify and address medical-legal barriers, particularly in the school setting, that can pose significant challenges in the management of childhood diabetes. 20 A critical dimension to the DCCA Program was providing all participants in the program free access to an MLP attorney and training each DCCA to identify legal issues that may affect a youth’s health. The finding that a significant proportion of caregivers of youth with type 1 diabetes report having an unmet legal need highlight the potential value of medical-legal support in pediatric diabetes care.16,21 Further, it suggests that improved screening for modifiable social needs may be an avenue for improving health of youth with diabetes. 22
This study adds to the evidence that pediatric patients with chronic disease may potentially benefit from individualized assistance with medical self-management and unmet legal needs, as well as health care system navigation, with the help of nonmedical personnel.23-25 Findings suggest that the incorporation of a DCCA and an MLP attorney may particularly serve as a means of improving outcomes for youth with type 1 diabetes in underserved populations given the significant improvement in glycemic control for participants with WA Medicaid. Publicly insured children have been shown to experience inequities in access to care, utilization, and unmet medical needs.26-28 With personalized home visits and legal support, the DCCA care model offers the potential to overcome disparities and traditional barriers to management such as lower levels of health literacy or education and difficulties negotiating relationships with providers or health care organizations. 29 In addition, home visits reduce the logistical barriers with meeting with the diabetes care team due to issues around transportation, child care, and clinic schedules. 30
An additional barrier for optimal diabetes management in youth is the lack of adequate support in the school setting, where children and adolescents typically spend one-third of their day.20,31,32 The intervention worked to facilitate appropriate care of participants by meeting and working with the school nurse or designee to confirm the school management plan of each youth in the DCCA Program. By doing so, the DCCAs were in a position to investigate if student self-care was compromised in school and address issues with adequate communication between parents and school personnel, which has been shown to impact parental and youth confidence in school management.19,33 Similarly, the school visits likely increased school nurse or designee comfort with facilitating school diabetes management and may have positively influenced youth by having an improved support system. 34 Finally, free access to an MLP attorney ensured that the legal rights of students with diabetes were being met by the school administration.35,36
This study’s results did not show a significant improvement in caregiver-reported or patient-reported DQOL. While it is worth noting that the sample size for the survey analysis was small and may be susceptible to selection bias, the DQOL results highlight the need for additional work to increase DQOL in youth. The finding that youth in the DCCA Program reported lower DQOL at the end of the intervention suggests that the inclusion of ample psychosocial support should be considered when implementing interventions that attempt to target and improve diabetes self-care and diabetes-specific family interactions. 37 More formal and frequent discussion of health-related quality of life in the home visits, for example, may be one way to impact psychosocial well-being and satisfaction with care. 38
There are limitations to this study. This was a pilot study that was designed to assess the feasibility of incorporating a DCCA and an MLP attorney into the pediatric diabetes care team and confirming the interest of youth and caregivers to participate in home and school visits through the recruitment of a large sample of youth with poorly controlled diabetes. While the quasi-experimental design of the pilot was beneficial in terms of assessing feasibility and enhances the likelihood of success of a future randomized control trial, additional work is required to confirm efficacy of this care model. Second, even after adjusting for baseline differences between the 2 groups, the lack of random assignment of participants may limit the generalizability of the results to a larger population. Third, while the participants in the DCCA Program mirror the institution’s broad clinic population, further work is needed to evaluate whether this type of intervention would be beneficial in different demographics. Finally, generalizability may also be limited for diabetes care teams without the infrastructure to support communication with and training of DCCA personnel or medical-legal partnership teams.
Implications
Findings suggest that DCCA and MLP personnel can be successfully integrated into the diabetes care team. Among youth with type 1 diabetes with suboptimal glycemic control, a community care model with medical-legal support designed to provide additional support in the home and school settings resulted in reduction in improved glycemic control, particularly in youth with public health insurance. Larger, randomized control studies should further investigate the efficacy of this care model in youth with diabetes.
Footnotes
Acknowledgements
The authors express their gratitude to Anne DuLong, Carol Jenkins, Jessica Jensen, Jennifer Lowe, Lindy MacMillan, Amanda Rutledge, Annette Quayle, and Lisa Schmidt for their contributions to the development and management of this program. In addition, we want to thank Natalie Beauregard, Katherine Cochrane, Neil Panlasigui, Michael Pascual, and Katherine Velasco for their efforts with study recruitment and data collection for this study.
Funding:
Supported by the Washington State Office of the Attorney General.