
Abstract
Purpose
The purpose of the study was to determine the impact of educational text messages on diabetes self-management activities and outcomes in patients with painful diabetic peripheral neuropathy (pDPN).
Methods
Patients with pDPN identified from a large integrated health system who agreed to participate were randomized to 6 months of usual care (UC) or UC plus twice-daily diabetes self-management text messages (UC+TxtM). Outcomes included the Pain Numerical Rating Scale, Summary of Diabetes Self-Care Activities (SDSCA), questions on diabetes health beliefs, and glycated hemoglobin (A1C). Changes from baseline were evaluated at 6 months and compared between groups.
Results
Demographic characteristics were balanced between groups (N = 62; 53% female, mean age = 63 years, 94% type 2 diabetes), as were baseline measures. After 6 months, pain decreased with UC+TxtM from 6.3 to 5.5 and with UC from 6.5 to 6.0, with no difference between groups. UC+TxtM but not UC was associated with significant improvements from baseline on all SDSCA subscales. On diabetes health beliefs, UC+TxtM patients reported significantly increased benefits and reduced barriers and susceptibility relative to UC at 6 months. A1C declined in both groups, but neither change was significant relative to baseline.
Conclusions
Patients with pDPN who receive twice-daily text messages regarding diabetes management reported reduced pain relative to baseline, although this change was not significant compared with usual care. In addition, text messaging was associated with increased self-management activities and improved diabetes health beliefs and total self-care. These results warrant further investigation.
Introduction
Chronic distal symmetric sensorimotor polyneuropathy, also known as diabetic peripheral neuropathy (DPN), is the most common of the diabetic neuropathies that are frequent complications of diabetes. 1 Diabetic peripheral neuropathy represents a spectrum from asymptomatic to the presence of a variety of neuropathic pain symptoms with severity that ranges from mild to severe. In the presence of pain, the condition is known as painful DPN (pDPN), which has an overall prevalence of 20% in patients with diabetes and 40% to 50% in those with DPN. 2 It is well established that pDPN is associated with a substantial patient-reported burden related to reductions in function, productivity, and health-related quality of life (HRQoL) as well as an economic burden resulting from increased health care resource use, with greater burdens at higher pain severity.3-5 The importance of recognizing DPN and pDPN in patients with diabetes was highlighted in a recent position statement that provides recommendations for its screening, diagnosis, and management, relying on a multimodal approach that includes glucose control, lifestyle modification, and pharmacologic management of pain. 6
Symptom onset generally starts in the feet, and patients with chronic pDPN are at subsequent risk for foot ulceration, infection, and amputation; pDPN is the leading cause of nontraumatic lower limb amputation in industrialized countries. 7 To reduce the risk of these sequelae, the American Diabetes Association (ADA) recommends that all patients with diabetes be screened for DPN at diagnosis and at least annually thereafter. 8 However, pDPN tends to be underdiagnosed and undertreated, 9 most likely as a result of misperceptions among patients as well as health care providers regarding the cause and management of pDPN. 10
Research suggests that patient-targeted initiatives promoting self-care management as part of collaborative care strategies can improve health outcomes in patients with chronic diseases including diabetes. 11 With the increasing use of communication technologies such as mobile phones and text messaging services, these modalities have been evaluated as a method to enhance diabetes self-management and outcomes such as medication adherence and glycemic control. Reviews and meta- analyses have reported inconsistent results with regard to the benefits of mobile phones and text messages for improving outcomes, likely as a result of heterogeneity in study methodologies and outcomes evaluated.12-17
In a small pilot study (N = 18) using a single cohort pre-post pilot design to evaluate a diabetes self-management support program that included text messaging, improved process measures were observed, including feeling capable of managing diabetes, number of foot self-exams per week, and self-reported diabetes medication adherence. 18 When a care management component was added and evaluated in a larger study of similar design (N = 74), the 6-month text messaging intervention was associated with improved self-reported diet in the past 7 days, increased blood glucose testing in the past 7 days, and overall satisfaction with care. 19 It was also associated with reduced feelings of being overwhelmed, reduced feelings of failure for diabetes routine, increased motivation to perform self-care, and reduced depression about life with diabetes. Using a similar population to understand the behavioral processes driving these effects, another study reported that the intervention had a broad impact on patient attitudes, knowledge, and ownership of diabetes and resulted in greater self-efficacy and self-care. 20
Because of the importance of foot care as part of adequate management of pDPN, similar interventions using text messaging may be of benefit to patients with this condition. However, such interventions have not been evaluated among pDPN patients. Given the increasing interest in pragmatic clinical trials for guiding evidence-based approaches to patient management,21-23 the purpose of this study was to determine the impact of educational text messages 19 on diabetes self-management activities and outcomes among patients with pDPN.
Methods
Research Design
This pragmatic trial was designed to assess the feasibility and effectiveness of educational text messages on diabetes self-management activities as an adjunctive intervention to usual care in patients with pDPN. The study was pragmatic in the sense that it enrolled a population that reflected real-world eligibility for the evaluated intervention, the intervention was delivered in the usual care setting, and the primary outcome was directly relevant to participants. 24 The main research question was to determine whether daily diabetes self-management text messages reduced self-reported pain among patients with pDPN. Secondary research questions addressed the impact of these text messages on diabetes health beliefs, quality of life, self-management activities, and control of glycated hemoglobin (A1C) in this population.
To address these questions, patients with pDPN meeting inclusion criteria were enrolled and randomized to receive either usual care (UC) or usual care plus twice-daily text messages (UC+TxtM). Patients likely to have pDPN were identified by querying the electronic data warehouse of a large integrated health system using the Hartsfield algorithm. 25 This algorithm identifies patients who have 1 or more ICD-9 codes consistent with peripheral neuropathy and excludes those with nondiabetic etiologies. For this study, the algorithm was modified to include use of chronic pain medications to expand the pool of potential study participants. This modification enabled identification of a larger number of patients who were likely to score ≥3 on the validated ID Pain neuropathic pain screening questionnaire. 26 A score ≥3 suggests the presence of neuropathic pain and was a study inclusion criterion. Exclusion criteria included rheumatoid arthritis, polyneuropathy due to alcohol or other diseases, end-stage renal disease, cancer, positivity for human immunodeficiency virus, viral hepatitis, blindness, dementia, and/or pregnancy.
For the patients identified using the modified Hartsfield algorithm, permission was obtained from their PCP or endocrinologist to mail study information to determine interest in study participation. A research nurse made up to 3 telephone calls to conduct screening among those who expressed interest. Subjects who reported bilateral foot pain and scored ≥3 on the ID Pain questionnaire qualified for in-person screening. In addition to a positive ID Pain score, patients were required to have decreased distal sensation and/or unequivocal decreased or absent ankle reflexes based on neurologic examination during the in-person screening. 27 Patients were also required to be English speakers and have a cell phone capable of receiving text messages.
The study duration was 6 months, consistent with the maximum duration of other text messaging studies that were identified from a PubMed literature search (search terms text, message, and diabetes with limits of years 2013-2015 and English language) and reported study durations that ranged from 1 month to 6 months.28-35
The study received Institutional Review Board/Ethics Committee approval and was performed in accordance with the Declaration of Helsinki; all patients provided written informed consent prior to participation. Patients who completed the surveys at baseline and 6 months received a $50 Target gift card on each occasion.
Setting
This study was conducted in an integrated health system located in a large metropolitan area. The health system is comprised of 4 hospitals and over 100 outpatient centers, including 25 primary care offices. All subjects receive care at 1 of the primary care offices. Patients who expressed interest and qualified through telephone screening were invited to a centrally located primary care office for additional in-person screening.
Interventions
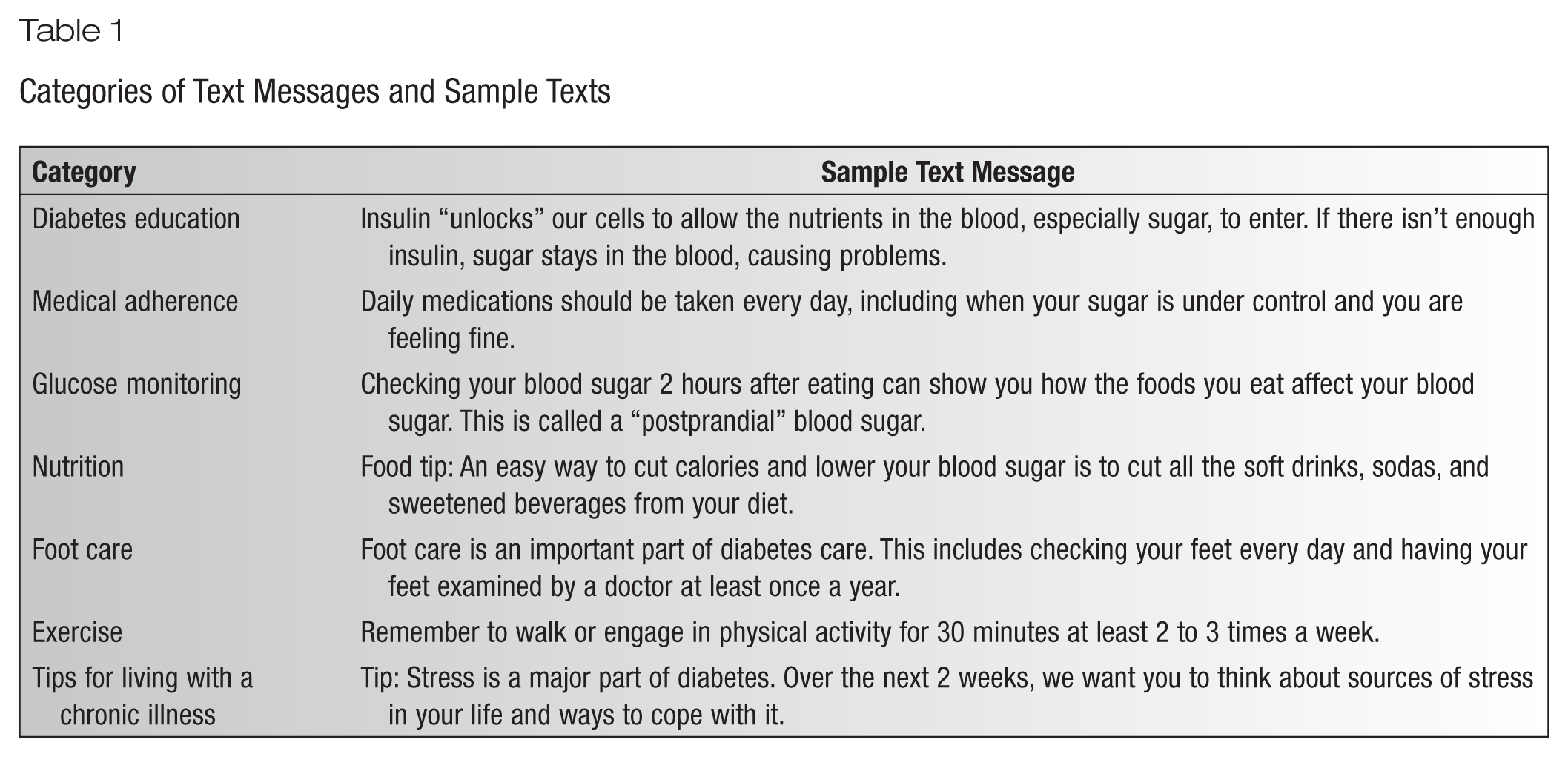
Subjects were randomized to either the intervention group of twice-daily text messages in addition to usual care or the control group of usual care without texting intervention. The text messages, which were programmed weekly into the text messaging function of Microsoft Outlook, were used to provide education, prompts, and reminders regarding important topics related to diabetes, including medication adherence, glucose monitoring, nutrition, exercise, and living with a chronic illness. These messages were originally developed by a multidisciplinary team of physicians, diabetes educators, and researchers.19,20 For the present study, an additional 18 text messages were developed to emphasize individual foot care and increase the likelihood that subjects would discuss foot concerns with their physician. Approximately 1 out of every 5 text messages focused on topics related to foot care (Table 1).
Categories of Text Messages and Sample Texts
Since not all physicians are familiar with the diagnosis and management of pDPN, 10 a 1-page information sheet was sent via e-mail to all primary care physicians (PCPs) and endocrinologists within the health system prior to study subject recruitment. The purpose of this sheet, which described the classic features of pDPN and illustrated the treatment algorithm, was to help ensure that all physicians who cared for patients in the study had access to appropriate pDPN treatment guidelines, thereby increasing the likelihood that subjects who inquired about treatment received appropriate therapy.
Outcome Measures
Outcome measures were administered at baseline and 6 months after initiating the interventions. The primary efficacy endpoint was change in self-reported pain severity measured using the 0-10 Pain Numerical Rating Scale (NRS; 0 = no pain, 10 = intolerable pain). 36 Secondary endpoints included the following patient-reported outcomes: Summary of Diabetes Self-Care Activities (SDSCA) measure 37 ; 5-dimension, 5-level EuroQoL (EQ-5D-5L) 38 ; the Morisky 4-Item Self-Report Measure of Medication-Taking Behavior 39 ; and questions regarding diabetes health beliefs. 40 In addition, the clinical variable of A1C was determined at both timepoints.
The SDSCA assesses diabetes self-management during the past week using 10 questions that comprise 4 subscales (diet, exercise, blood glucose monitoring, and foot care) with responses of 0 to 7 that reflect number of days each of the subscale activities was performed. 37 Higher scores on the SDSCA indicate better self-management, and a total score is derived from the sum of all subscales. A separate question on smoking is also part of the questionnaire.
The EQ-5D-5L is a generic measure of HRQoL with a recall period of “today” that includes a visual analog scale (VAS) of current health status (0 = worst health state, 100 = best health state) and 5 dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) with 5 levels of impairment responses (1 = no problem with activity, 5 = unable to do activity). 38 The individual dimensions were evaluated at baseline and 6 months by dichotomizing the responses into “no problems” and “any problem.” In addition, the Crosswalk Index Value Calculator was used based on the US value set to calculate a population preference-weighted EQ-5D-5L health index score.41-43
The Morisky 4-Item Self-Report Measure of Medication-Taking Behavior provides an indication of adherence to medications for the specifically evaluated condition, which in the current analysis was stated as “diabetes medication,” based on yes (=0)/no (=1) responses to 4 questions. Responses are summed to give a range of scores from 0 to 4, with higher scores indicating poorer adherence. 39
Questions on health beliefs not only included perceptions of medication benefits (how adherence will benefit health) and barriers (adverse events and other factors contributing to nonadherence) but also susceptibility (beliefs on consequences of nonadherence), perceived disease severity, self-efficacy (ability to manage their disease), and locus of control (ie, to what extent disease was controlled by the patient, other individuals, or chance). 40
Statistical Analysis
Within-group changes from baseline at 6 months were evaluated using paired t test and McNemar’s test for means and proportions, respectively. Between-group differences were compared using an analysis of covariance model of the outcome measure at 6 months, with treatment group as predictor and baseline measure as a covariate. 44 All analyses were conducted using SAS version 9.3 (SAS Institute, Cary, NC). Statistical significance was set at P < .05.
Results
Figure 1 presents subject identification, enrollment, and retention. A total of 69 patients were enrolled and randomized. Demographic characteristics were balanced between groups (Table 2). Patients were predominantly female (52.2%), with a mean age of 61.9 years, and had primarily type 2 diabetes (91.3%) with a mean duration of 15.1 years. Of the 40 patients randomized to UC+TxtM, 4 patients withdrew, and 1 was lost to follow-up. In the UC group, 1 patient withdrew, and 1 patient was lost to follow-up. Among those who completed the study, the demographic and clinical characteristics remained balanced between the groups, and there were no differences between those who completed and did not complete the study.
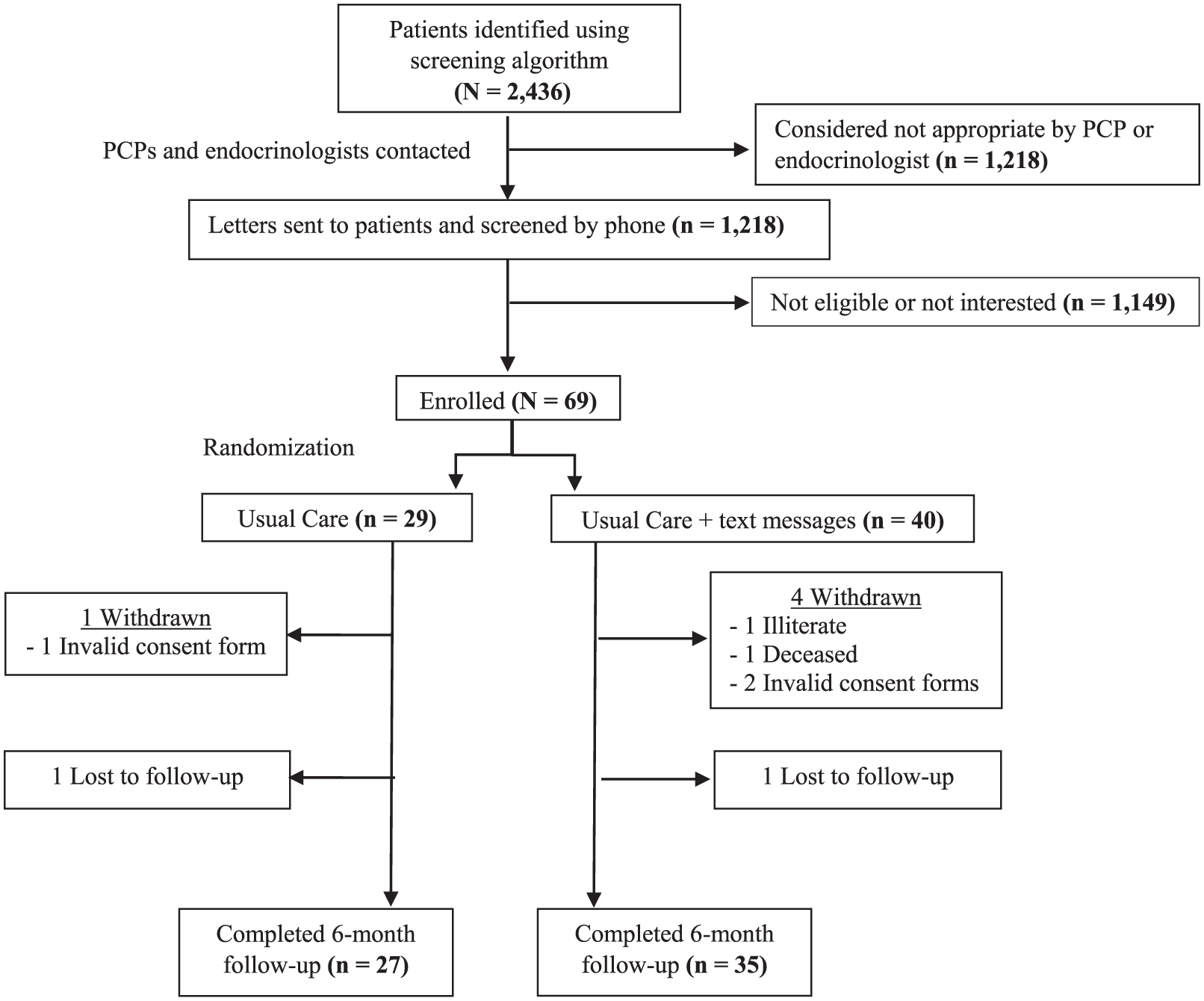
Subject identification, enrollment, and retention.
Demographic and Clinical Characteristics of Randomized Patients
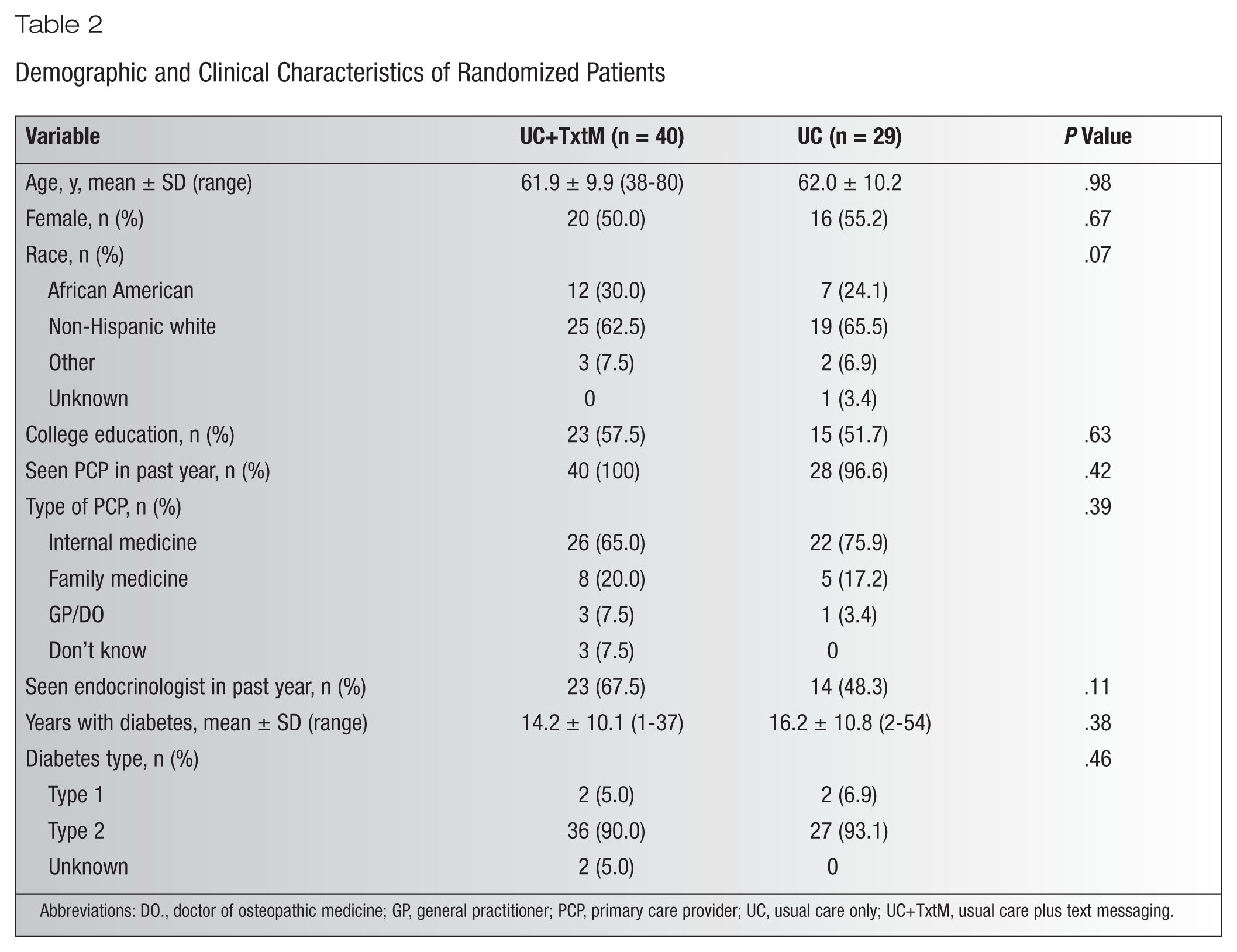
Abbreviations: DO., doctor of osteopathic medicine; GP, general practitioner; PCP, primary care provider; UC, usual care only; UC+TxtM, usual care plus text messaging.
As shown in Figure 2, the mean pain severity score significantly decreased from baseline at the 6-month timepoint among patients in the UC+TxtM group, from 6.3 to 5.5 (P = .03), but not in the UC group, from 6.5 to 6.0 (P = .24). However, the difference between treatments at 6 months was not significant (P = .48) after adjusting for baseline pain score.
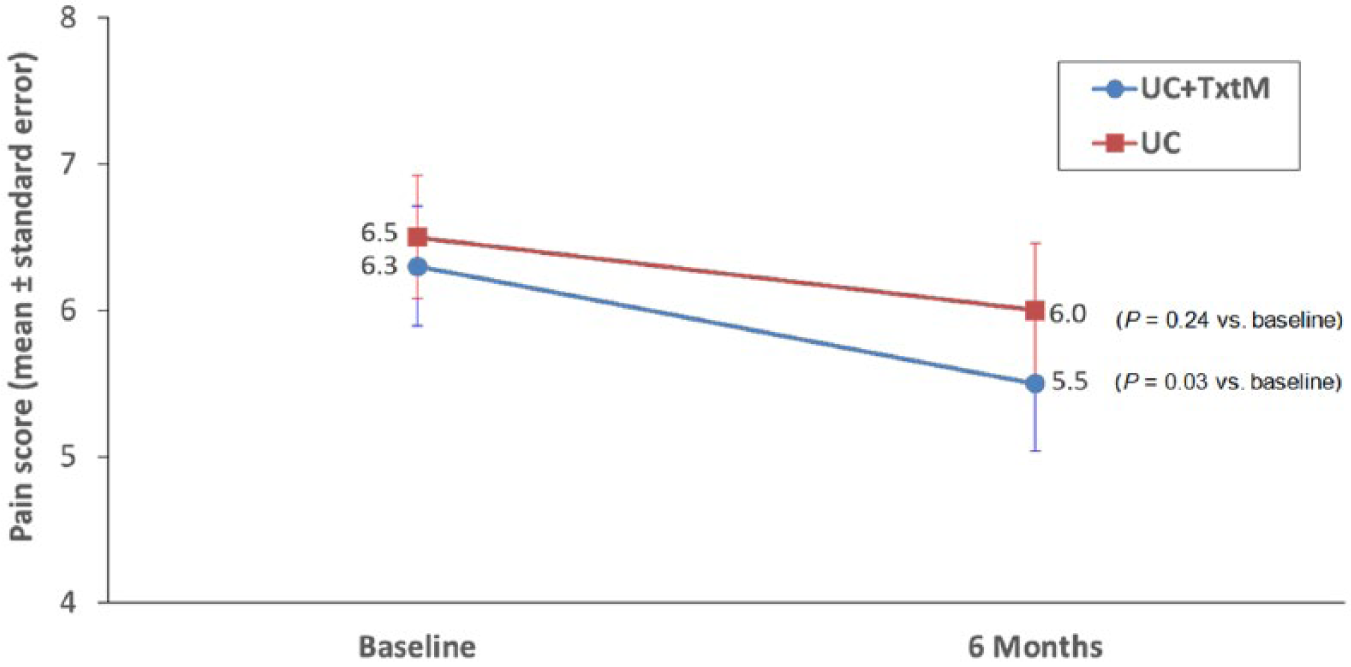
Self-reported pain at baseline and 6 months.
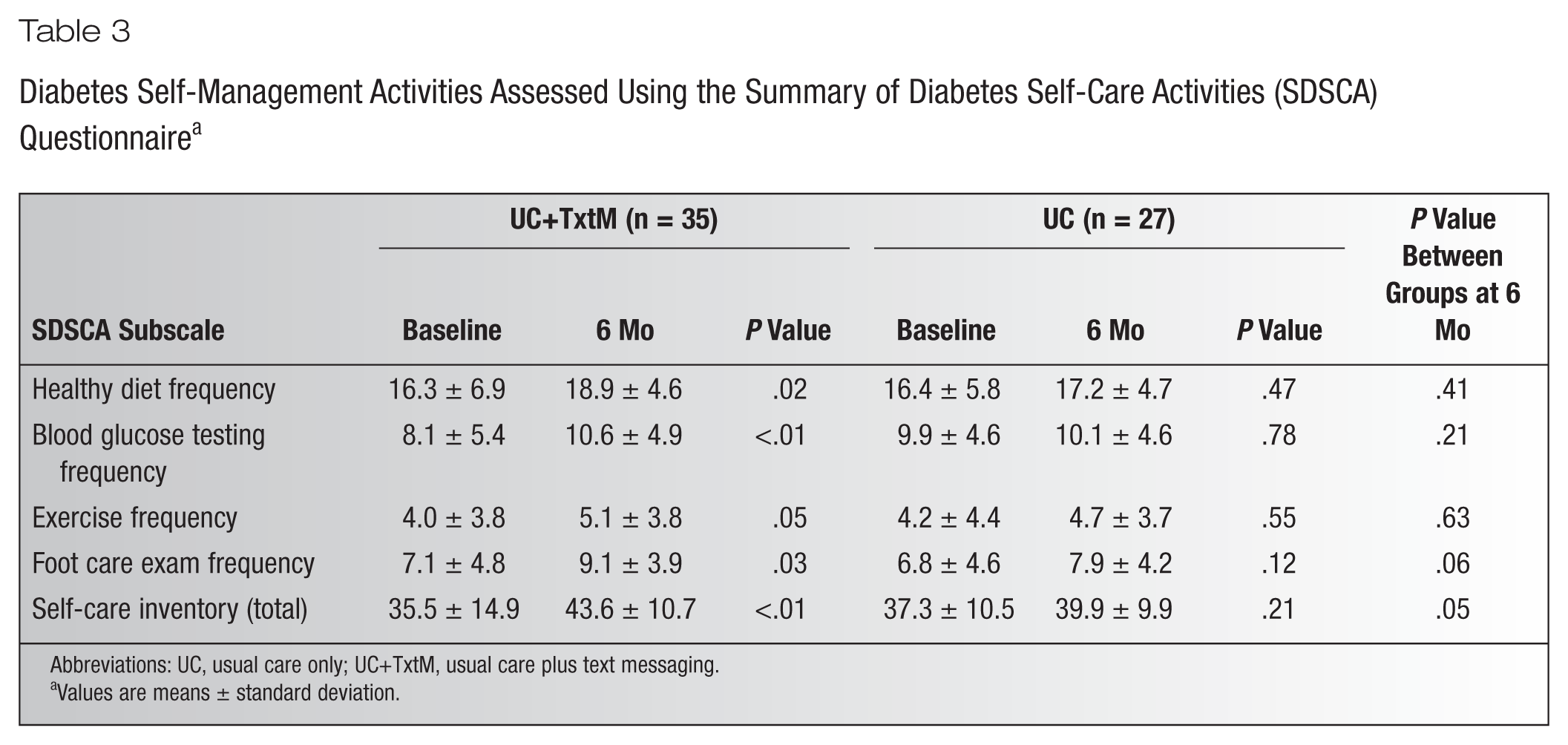
The scores of all SDSCA subscales as well as the total score showed that the frequency of performing diabetes self-management activities at the 6-month timepoint significantly increased relative to baseline in the UC+TxtM group (Table 3). The largest proportional increases were for blood glucose testing (30.9%), followed by foot care exam (28.2%) and exercise (27.5%). Among the UC group, none of the reported increases in frequency from baseline were statistically significant. Proportional increases ranged from 2.0% (blood glucose testing) to 16.2% (foot care exam). While improvements in self-management were numerically greater in the UC+TxtM group relative to UC, only the difference in total score at 6 months approached significance (P = .05).
Diabetes Self-Management Activities Assessed Using the Summary of Diabetes Self-Care Activities (SDSCA) Questionnaire a
Abbreviations: UC, usual care only; UC+TxtM, usual care plus text messaging.
Values are means ± standard deviation.
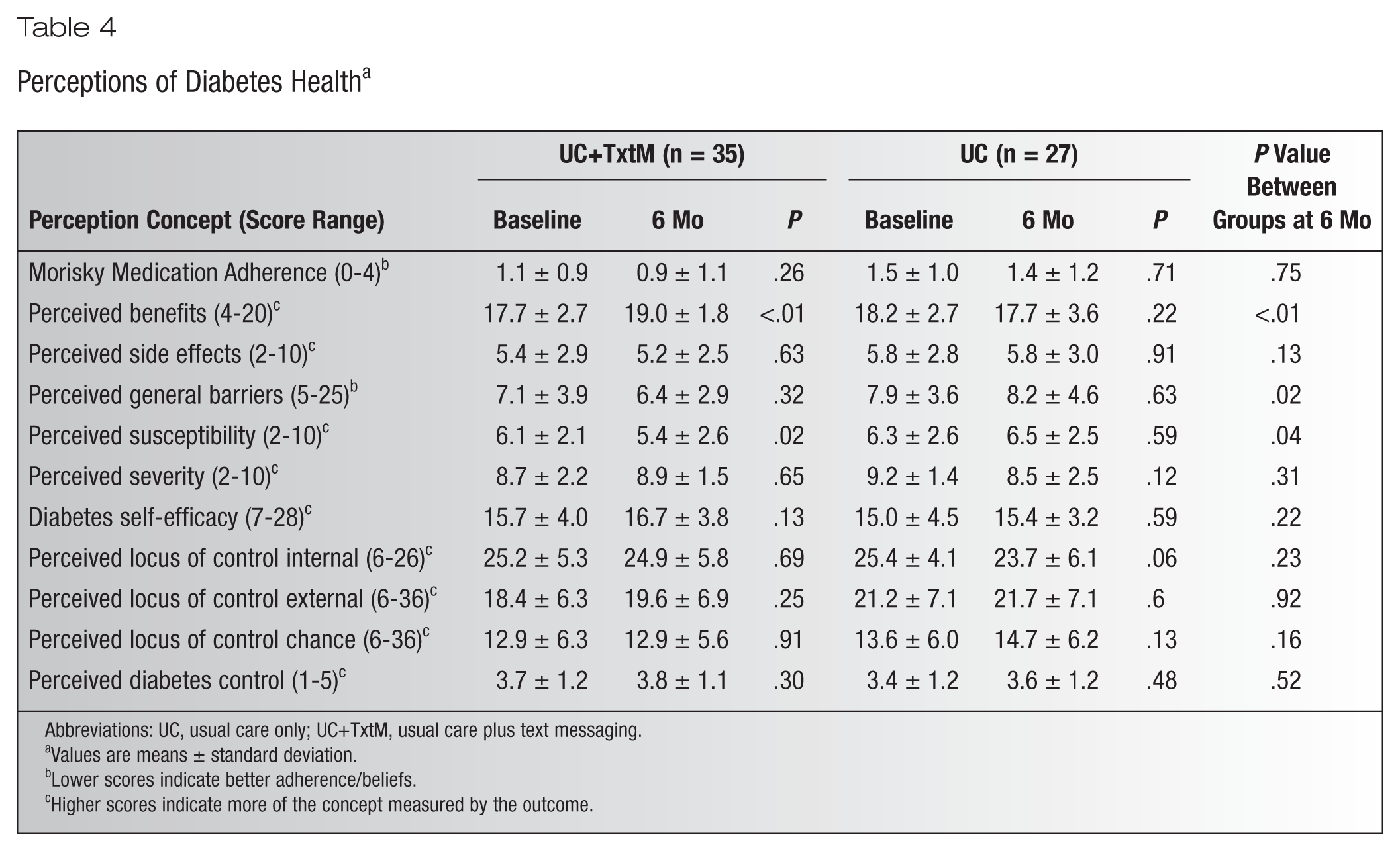
With regard to diabetes health benefit questions, patients in the UC+TxtM reported significant improvements in perceived benefits and perceived susceptibility (Table 4). In contrast, patients in the UC group did not report significant benefits. In fact, perceptions of diabetes health at 6 months were numerically poorer compared with baseline on most of the concepts. As a result, significant differences at 6 months favored UC+TxtM for the concepts of perceived benefits, perceived general barriers, and perceived susceptibility (Table 4).
Perceptions of Diabetes Health a
Abbreviations: UC, usual care only; UC+TxtM, usual care plus text messaging.
Values are means ± standard deviation.
Lower scores indicate better adherence/beliefs.
Higher scores indicate more of the concept measured by the outcome.
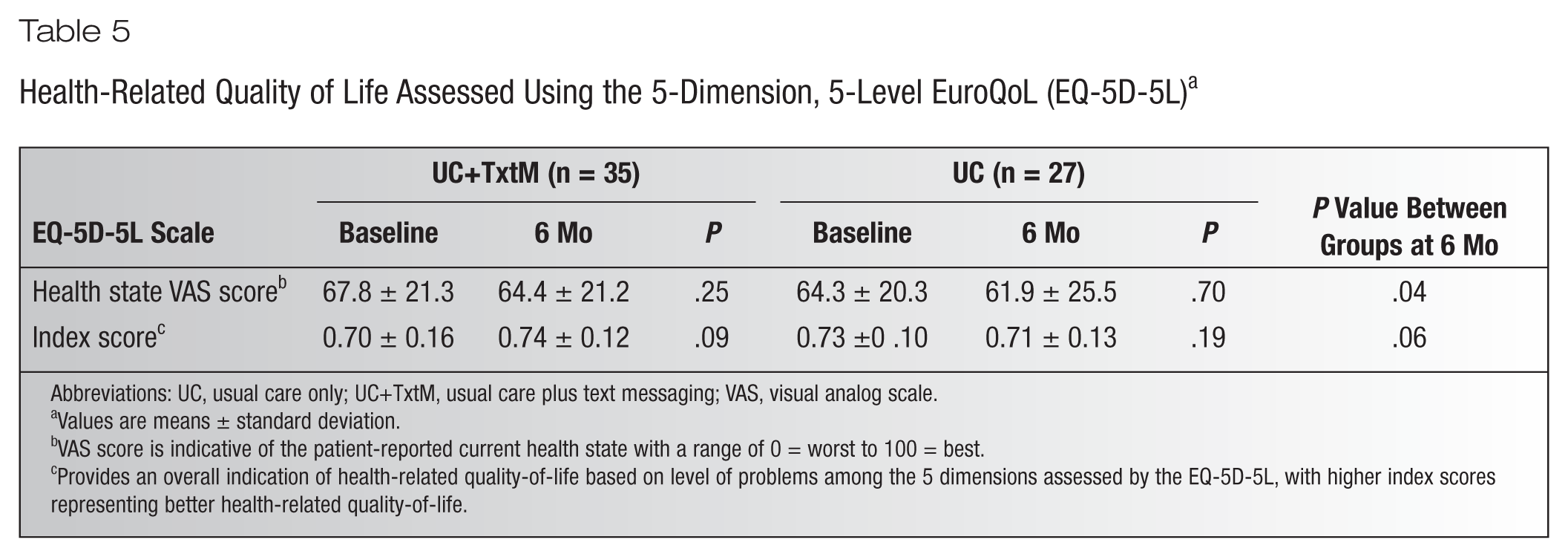
On the EQ-5D-5L VAS, patients in both treatment groups reported their health state at the 6-month timepoint as being worse on average than at baseline (Table 5), although the mean changes were not significant. At the 6-month timepoint, patients in the UC+TxtM reported a decremental change in health state that was numerically greater than the UC group (3.4 points vs 2.4 points). However, after adjustment for baseline differences between treatment groups, the mean VAS score at 6 months in the UC+TxtM group was statistically higher than the UC group (P = .04). A similar trend was noted with the EQ-5D-5L index score (Table 5).
Health-Related Quality of Life Assessed Using the 5-Dimension, 5-Level EuroQoL (EQ-5D-5L) a
Abbreviations: UC, usual care only; UC+TxtM, usual care plus text messaging; VAS, visual analog scale.
Values are means ± standard deviation.
VAS score is indicative of the patient-reported current health state with a range of 0 = worst to 100 = best.
Provides an overall indication of health-related quality-of-life based on level of problems among the 5 dimensions assessed by the EQ-5D-5L, with higher index scores representing better health-related quality-of-life.
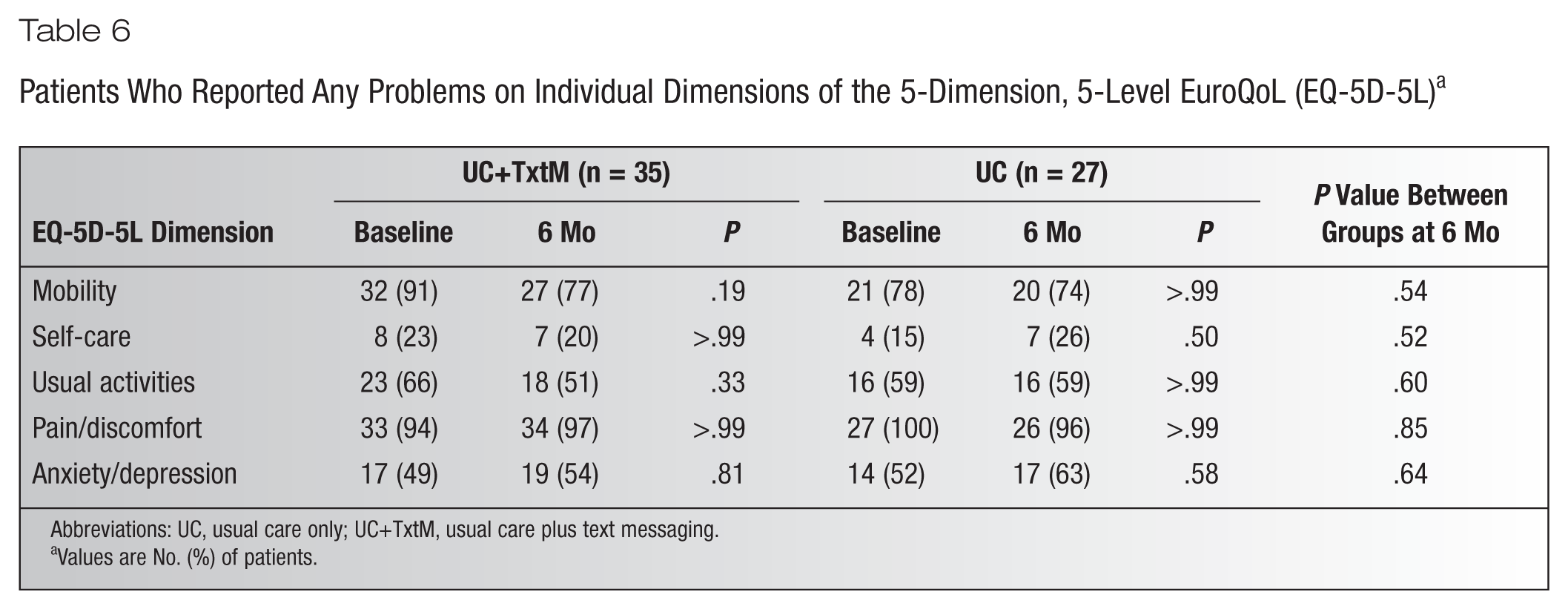
The percentage of patients who reported any problems on each of the EQ-5D-5L dimensions is shown in Table 6, and there were no significant differences between groups at 6 months. While within-group changes from baseline in either group were not significant, decremental changes from baseline to 6 months were observed for UC+TxtM for the proportions of patients who reported problems on mobility (from 91% to 77%) and usual activities (from 66% to 51%). In the UC group, the proportions remained essentially the same at both timepoints.
Patients Who Reported Any Problems on Individual Dimensions of the 5-Dimension, 5-Level EuroQoL (EQ-5D-5L) a
Abbreviations: UC, usual care only; UC+TxtM, usual care plus text messaging.
Values are No. (%) of patients.
Small changes were observed in glucose control that were neither statistically significant with regard to baseline nor significant between interventions at 6 months. In the UC+TxtM group, A1C was reduced from a mean (±SD) of 7.96% ± 2.35% (63.5 ± 2.2 mmol/mol) to 7.67% ± 1.93% (60.3 ± 2.4 mmol/mol; P = .11) and in UC from 7.95% ± 2.25% (63.4 ± 1.1 mmol/mol) to 7.46% ± 2.26% (58.0 ± 1.2 mmol/mol; P = .39), with no difference between the groups at 6 months (P = .74).
Discussion
This study expands on the potential utility and benefits of text messaging that have been reported in patients with diabetes20,45,46 by showing that text messaging improved self-care management and health beliefs in patients with pDPN. Although the study did not meet the primary endpoint based on differences in pain relief between the 2 interventions, patients in the UC+TxtM group reported significantly lower pain at 6 months relative to baseline, whereas the reduction in the UC group was not significant. Neuropathic pain management is especially challenging in patients with pDPN,47,48 and any impact of text messaging on pain management was likely indirect as the intervention relied on patients discussing foot pain and its treatment with their physicians. In addition, although perceived benefits of medication adherence improved in the group receiving text messages, this study did not assess adherence to specific medications. As a result, enhanced self-care and health beliefs may have contributed as much to pain improvement as adherence to particular medications for diabetes or pain control.
Significant improvements from baseline in the UC+TxtM group but not the UC group were reported for the frequency of all evaluated self-care management activities. These included self-care activities generally related to diabetes such as healthy diet and blood glucose monitoring as well as foot exams that are of special relevance to patients with pDPN. Furthermore, for foot exams, the results suggested a trend for a greater increase in this self-care activity in the UC+TxtM group relative to UC. The consistent improvements with the UC+TxtM intervention on all SDSCA subscales resulted in an overall benefit in self-management that was of greater magnitude relative to UC. Also, UC+TxtM appeared to have a more positive effect relative to UC on patients with regard to diabetes health beliefs, including improvements in perceptions of benefits, barriers, and susceptibility that were significant relative to UC. However, baseline scores on diabetes health belief questions were nearly at the bounds of the subscales, suggesting not only that patients already had good perceptions and few barriers but also implying that there may be a ceiling/floor effect limiting assessment of further improvements.
These results are consistent with an observational study that also reported an association between text messaging and improved self-care and health beliefs. 20 Use of a randomized trial design in the current study further supports the proposal that mobile-based health interventions such as text messaging can positively impact pathways associated with disease-related behavior. While self-care and health beliefs are central components of disease management, it is important to consider whether these behavioral outcomes translate into clinical outcomes. Although changes in A1C were not significant in either group, the observed changes were consistent with a 0.5% reduction found over 6 months in a meta-analysis of mobile phone interventions. 12 One of the main considerations in reducing A1C to optimal target levels is that management needs to be individualized based on patient characteristics. Thus, the observed changes may not necessarily reflect the clinical conditions or goals of the patients, especially since inclusion criteria did not include an A1C threshold as in other studies that evaluated text messaging to enhance glycemic control.20,45
On the EQ-5D-5L, patients in both treatment groups reported a slight decrease in health state (VAS) at the 6-month timepoint relative to baseline, although the score in the UC+TxtM group showed significantly better HRQoL than UC after adjusting for baseline values. The UC+TxtM group was characterized by overall improvements in HRQoL (index score) that trended toward significance both with regard to baseline as well as compared with the UC group, which showed a small decrease in HRQoL. This improvement in index score in the UC+TxtM group despite patient report of small decreases in health state likely results from the shift to fewer patients with problems in specific functional dimensions of the EQ-5D-5L, such as mobility and usual activities, with mobility in particular showing an almost 3-fold increase from 8.6% to 22.9%. Of note, baseline index scores were generally comparable to the 0.75 that has been reported for patients with diabetes, 49 although the fact that they were slightly lower may relate to the presence of diabetes complications such as pDPN.
Strengths and Limitations
Strengths of this study are its pragmatic approach using a community-based population and randomized design. Study limitations include the potential for selection bias since patients who agreed to participate may have characteristics and perspectives different from those who declined.
Additionally, as with all studies reliant on ICD codes for population identification, it is possible that there were errors in coding. In this regard, it should also be noted that patient use of medications associated with chronic pain was an identification criterion because many patients with pDPN do not have ICD-9 codes reflecting peripheral neuropathy. Since these medications may be used for several conditions and the reasons for medication use were not determined, misidentification of patients for inclusion was possible. However, such misidentification should be minimized by the requirement of a positive neurologic foot exam.
While duration was similar to other studies that evaluated text messaging as an intervention,28-35 long-term follow-up of diabetes and pDPN management was lacking, thus limiting the longitudinal generalizability of the study. In addition, 1-way texting such as used in the current study limits feedback and interaction, which may potentially result in some subjects becoming less engaged.
It should also be noted that a larger sample size may have resulted in statistical and clinical benefits of greater magnitude in pain and other outcomes. Because of the small sample, the results and conclusions of this study should be considered exploratory. Finally, the management strategies recommended by clinicians and used by the patients were not captured. It is therefore difficult to determine whether differences in outcomes were due solely to text messages or a combination of text messages and differences in management strategies that may have been triggered by increased patient-physician communication.
Summary and Implications
Text messaging improved self-management activities and resulted in benefits related to diabetes health beliefs and total self-care. These effects may have contributed to the significant reduction from baseline in pain scores in the text messaging group. Although the between-group pain scores trended to favor the text message group, the difference was not statistically significant. With the increased availability of mobile devices, text messaging may represent a low-cost strategy for disease-related behavioral modification that can be incorporated into a multimodal approach for reducing the risk and impact of pDPN in patients with diabetes. Additional studies are needed to confirm these results and determine the long-term benefits of text messaging on patient perceptions and clinical outcomes.
Footnotes
Funding:
This study was sponsored by NorthShore University HealthSystem and Pfizer Inc. Victoria Bauer, Nancy Goodman, and Ed Wang are employees of NorthShore University HealthSystem. Terri L. Craig, Scott E. Glosner, Mark S. Juhn, Joseph C. Cappelleri, and Alesia B. Sadosky are employees and shareholders of Pfizer. Brittany Lapin was an employee of NorthShore University HealthSystem when this study was initiated but is now an employee of Cleveland Clinic. Christopher Masi was an employee of NorthShore University HealthSystem during the study but is now an employee of Emory University School of Medicine. Camille Cooley was an employee of NorthShore University HealthSystem during the study and remains affiliated with Northwestern University. Editorial support was provided by E. Jay Bienen and was funded by Pfizer.