
Abstract
Purpose
The purpose of this study was to examine perceived barriers to physical activity among low-income Latina women who were at risk for type 2 diabetes, as well as the demographic factors that influence these perceived barriers.
Methods
Recruited in the waiting room of a community health center in a low-income neighborhood (n = 160), Latina women between the ages of 18 and 49 years completed a survey to assess demographic characteristics and perceived barriers to physical inactivity. Descriptive statistics, chi-square tests, and multivariate regression analyses were conducted to identify barriers to physical activity and the associations between demographic factors and perceived barriers.
Results
The most commonly perceived barriers to physical activity in the study sample were lack of willpower and lack of energy. After adjusting for other characteristics, overweight/obese participants were more likely than women of normal weight to report social influence and fear of injury as important barriers to exercise. In addition, women whose preferred language was Spanish were more likely than women whose preferred language was English to perceive lack of time, and social influence as important barriers.
Conclusions
The effective encouragement of physical activity among Latina women at risk for type 2 diabetes must address the perceived barriers of lack of willpower and lack of energy. Although all women at risk for type 2 diabetes could benefit from counseling and other strategies to encourage physical activity, these efforts should be targeted toward Spanish-speaking overweight/obese women, who are more likely to perceive barriers to exercise.
Low-income populations and racial minorities, especially Latinos, suffer disproportionately from diabetes and prediabetes.1,2 Among Latinos, women have a higher risk for developing diabetes than men, 2 and in a study that compared the lifetime risk of developing diabetes across demographic groups, Latina women had the highest lifetime risk (53%) of all groups. 2 Risk factors associated with the rapidly rising number of patients with prediabetes and type 2 diabetes in the United States include overweight, excess energy intake, and physical inactivity.3,4
Physical activity can improve blood glucose control and prevent or delay the onset of type 2 diabetes.5-10 Studies of adults with elevated blood glucose concentrations demonstrated that regular physical activity reduces type 2 diabetes risk.10-12 In 2 landmark diabetes prevention studies of lifestyle interventions—one that involved 30 minutes of daily moderate physical activity and one that involved 150 minutes of moderate physical activity per week—exercise reduced type 2 diabetes incidence by 58% among American and Finnish adults with impaired glucose tolerance.10,11 Another study demonstrated that even modest changes in exercise alone (20 minutes of moderate exercise, 10 minutes of strenuous exercise, or 5 minutes of very strenuous exercise 1 or 2 times a day) reduced diabetes risk by 46% among Chinese adults with impaired glucose tolerance, as compared with a 42% reduction through diet and exercise in combination and a 31% reduction through diet alone. 12 Although weight loss in these studies was the main predictor of lower diabetes incidence, increased physical activity reduced diabetes risk even when weight loss goals were not achieved.9,13,14
Despite the many health benefits of physical activity, <10% of American adults meet the Physical Activity Guidelines for Americans, which recommend that adults obtain at least 150 minutes/week of moderate-intensity physical activity, 75 minutes/week of vigorous-intensity physical activity, or an equivalent combination of moderate and vigorous physical activity. 15 In addition, previous studies showed that US Latinos have a higher prevalence of inactivity than that of other racial/ethnic groups.16-18 Many studies examined perceived barriers to physical activity among people with type 2 diabetes, which can be grouped into 3 general categories of influences: individual, social, and environmental.19-23 Individual influences include feeling lazy, fear of injury, low priority for health promotion, health problems, and shame or embarrassment.19-23 Social influences include lack of support from friends and family as well as cultural barriers,19-23 and environmental influences include inclement weather and limited access to safe facilities or places for activity.19-23
Although perceived barriers to exercise have been studied extensively among people with type 2 diabetes, research is limited on perceived barriers among people who do not have type 2 diabetes but are at high risk for the disease. A qualitative study of Finnish adults with high risk of type 2 diabetes found that those at risk experienced many individually meaningful motivators for exercise and relatively few barriers. 24 A cross-sectional study of a similar population identified fear of injury, low prioritization of activity, and finding time for activity as the main barriers to exercise. 25 However, more research on the perceived barriers to exercise among people at high risk for type 2 diabetes, particularly among low-income minority populations, is needed to better understand factors that motivate individuals to make lifestyle changes to prevent the disease. 25
Accordingly, this study sought to examine the perceived barriers to physical activity among low-income Latina women in a population at high risk for type 2 diabetes, as well as demographic factors that influence these perceived barriers. Identifying perceived barriers to exercise and factors associated with the perception of these barriers in this understudied population has important implications for strategies to promote physical activity, as well as for context-specific diabetes prevention efforts.
Methods
Research Design and Participants
A convenience sample of women aged 18 to 49 years (N = 256) at the Fair Haven Community Health Center (FHCHC) participated in this cross-sectional study. The FHCHC is located in Fair Haven, a neighborhood in New Haven, Connecticut, that is 72% Hispanic/Latino and has a multigenerational prevalence of obesity and type 2 diabetes. 26 The health center offers a diabetes prevention program for individuals with prediabetes, which includes a weekly lifestyle class and structured exercise classes 3 times per week tailored to a low-income majority-Latino and Spanish-speaking population. 27
Data Collection Procedures
Women who visited the FHCHC, as either patients or companions, were recruited for the study in the clinic’s waiting room from June to August 2017. Participants completed a written survey in English or Spanish, according to their language preference, and received a $10 coupon to a local farmers’ market upon its completion. This study focuses on Latina women at risk for type 2 diabetes, so participants who did not identify as Latina (n = 74) and/or had type 2 diabetes (n = 30) were excluded from analyses. After these participants were excluded, the resulting sample size for the subsequent analyses was 160. The Human Subjects Review Boards of Yale University and the FHCHC approved the study.
Survey Instrument
The study’s survey included a section on demographic information and a previously validated questionnaire designed to measure perceived barriers to physical activity. The authors translated the survey to Spanish and back translated it to English. A bilingual nurse familiar with the literacy levels of the FHCHC’s patient population reviewed the survey, which was then pretested in the patient population (n = 15) for comprehension and flow.
Measures
Demographic data collected on the survey included age, marital status, ethnicity, country of origin, employment status, education level, number of children, and self-reported height and weight. The survey also included questions about previous diagnoses of type 2 diabetes and prediabetes, as well as whether participants had recently made lifestyle changes to reduce their risk for type 2 diabetes. Body mass index (BMI) values were calculated from participants’ self-reported height and weight. Food security status was measured with the US Department of Agriculture’s validated 6-item Household Food Security Module.28,29 The module asks participants to respond “yes” or “no” to questions such as “In the last 12 months, did you or others in your household ever cut the size of your meals or skip meals because there wasn’t enough money for food?” as well as to indicate whether statements such as “(I/we) couldn’t afford to eat balanced meals” were “often true,” “sometimes true,” or “never true” for them or members of their household. According to the department’s scoring guidelines for the 6-item module, “yes,” “often true,” and “sometimes true” were considered affirmative responses; participants with 1 to 4 affirmative responses were classified as “food secure,” and participants with 5 or 6 affirmative responses were classified as “food insecure.”
Outcome Measures
Perceived barriers to physical activity were measured with the validated Barriers to Being Active Quiz (BBAQ). 30 The BBAQ asks participants to indicate whether they are “very unlikely,” “somewhat unlikely,” “somewhat likely,” or “very likely” (scored 0-3) to express individual statements such as “I am embarrassed about how I will look when I exercise with others” and “My free times during the day are too short to include exercise.” The BBAQ contains 21 statements in total, and according to the survey’s scoring system, groups of 3 statements constitute perceived barrier categories: lack of time, social influence, lack of energy, lack of willpower, fear of injury, lack of skill, and lack of resources. 30 The purpose of the BBAQ is not to determine a participant’s total score for all 21 statements, but rather to determine which barriers an individual experiences as “important.” 30 A barrier category is considered important if the participant’s scores for the statements in that category sum to an overall likelihood score ≥5. 30
To determine reliability of the BBAQ in this patient population, Cronbach alpha, a measure of internal consistency, was calculated for each barrier category before use in analyses. Alpha values for 6 of the 7 barrier categories ranged from 0.63 to 0.72, and the authors considered these values acceptable for this exploratory research. The seventh barrier category, lack of resources, had an alpha value of 0.56, which fell below the acceptable range. As a result, it was not included as a category in further analyses.
Statistical Analyses
Descriptive statistics were used to summarize the demographic characteristics of the sample and to determine the mean scores for each barrier category as well as the percentage of participants for whom each barrier category was important.
Next, the authors examined unadjusted associations between demographic characteristics (age, marital status, BMI, food security status, employment status, education level, children, birth in the United States, prediabetes diagnoses, and preferred language) and the perceived importance of each barrier category with chi-square tests. A dichotomous variable for perceived importance, based on likelihood scores ≥5 or <5 as previously described, was used for each barrier category.
Finally, the authors performed multivariable logistic regression analyses to identify independent demographic correlates of perceived barriers to physical activity. The outcome variable in these multivariable logistic regressions was the dichotomous variable for perceived importance, and the predictor variables were the demographic characteristics that were significantly associated with each barrier at the level of P < .1 in bivariate analyses. The authors used the enter method for the regressions, and significance was determined per a P value <.05 or a 95% CI for an odds ratio (OR) that was exclusive of the value of 1.0. All analyses were completed in SPSS 22.0 (IBM, Chicago, Illinois).
Results
Characteristics of the Study Population
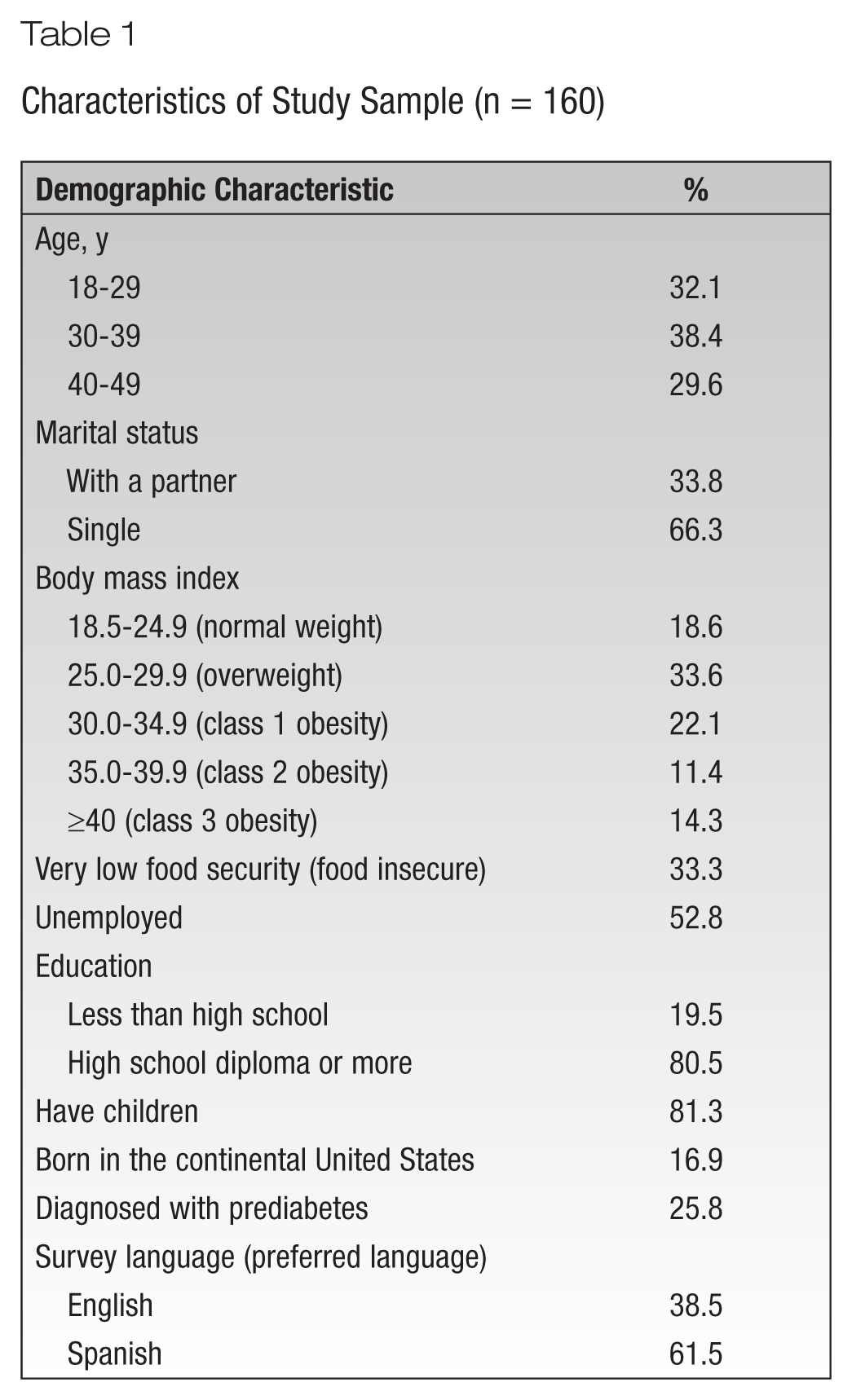
Table 1 presents the characteristics of women in the study population. The mean age was 33.7 years (SD = 8.58); BMI, 31.56 (SD = 7.15); and years of education received, 10.99 (SD = 3.99). Of the study population, 25.8% had received diagnoses of prediabetes, and 81.5% of women were overweight or obese based on BMI calculated from self-reported height and weight. Most women were not born in the continental United States, and the mean number of years lived in the continental United States was 15.6 (SD = 10.32). Reported countries of origin included Puerto Rico, Mexico, Ecuador, Columbia, and Peru. The preferred language of the majority of women (61.5%) was Spanish.
Characteristics of Study Sample (n = 160)
Perceived Barriers to Physical Activity
The most commonly perceived barriers to physical activity in the study population were lack of willpower and lack of energy, which were important barriers for 61.9% and 53.6% of study participants, respectively. The mean likelihood scores for these barriers were 5.08 (SD = 2.5) for lack of willpower and 4.52 (SD = 2.63) for lack of energy (Table 2).
Perceived Barriers to Physical Activity in the Study Sample
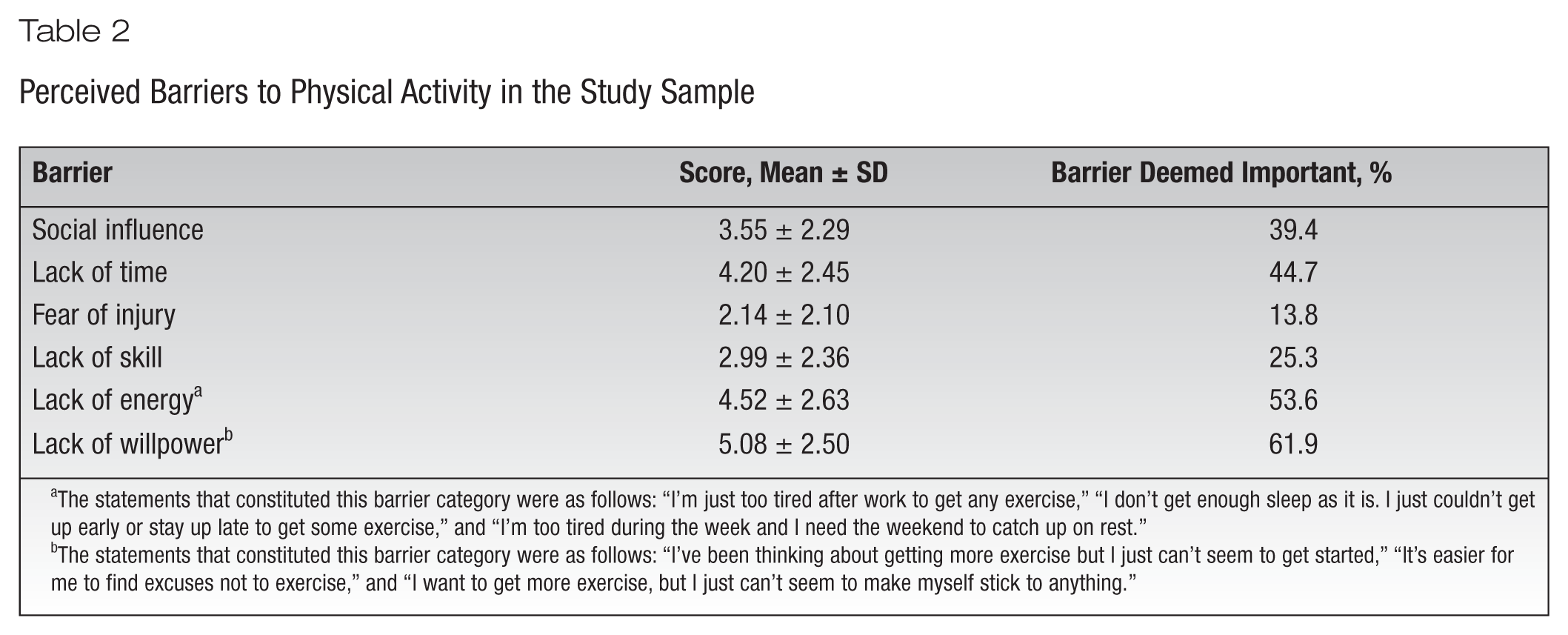
The statements that constituted this barrier category were as follows: “I’m just too tired after work to get any exercise,” “I don’t get enough sleep as it is. I just couldn’t get up early or stay up late to get some exercise,” and “I’m too tired during the week and I need the weekend to catch up on rest.”
The statements that constituted this barrier category were as follows: “I’ve been thinking about getting more exercise but I just can’t seem to get started,” “It’s easier for me to find excuses not to exercise,” and “I want to get more exercise, but I just can’t seem to make myself stick to anything.”
Factors Associated With Perceived Barriers to Physical Activity
Bivariate analyses (Table 3) indicated that older women (40-49 years) were more likely than younger women (18-39 years) to perceive fear of injury (P = .01) as an important barrier to physical activity. Overweight/obese women were more likely than women of normal weight to perceive social influence (P = .04) and lack of skill (P = .05) as important barriers, and unemployed women were more likely than women who were employed to perceive fear of injury as an important barrier (P = .03). Women who were not born in the continental United States were more likely than women born in the United States to perceive lack of time as an important barrier (P = .03), and women whose preferred language was Spanish were more likely than women whose preferred language was English to perceive lack of time (P < .01), social influence (P < .01), and lack of skill (P = .01) as barriers.
Unadjusted Associations Between Sample Characteristics and Perceived Barriers to Physical Activity a
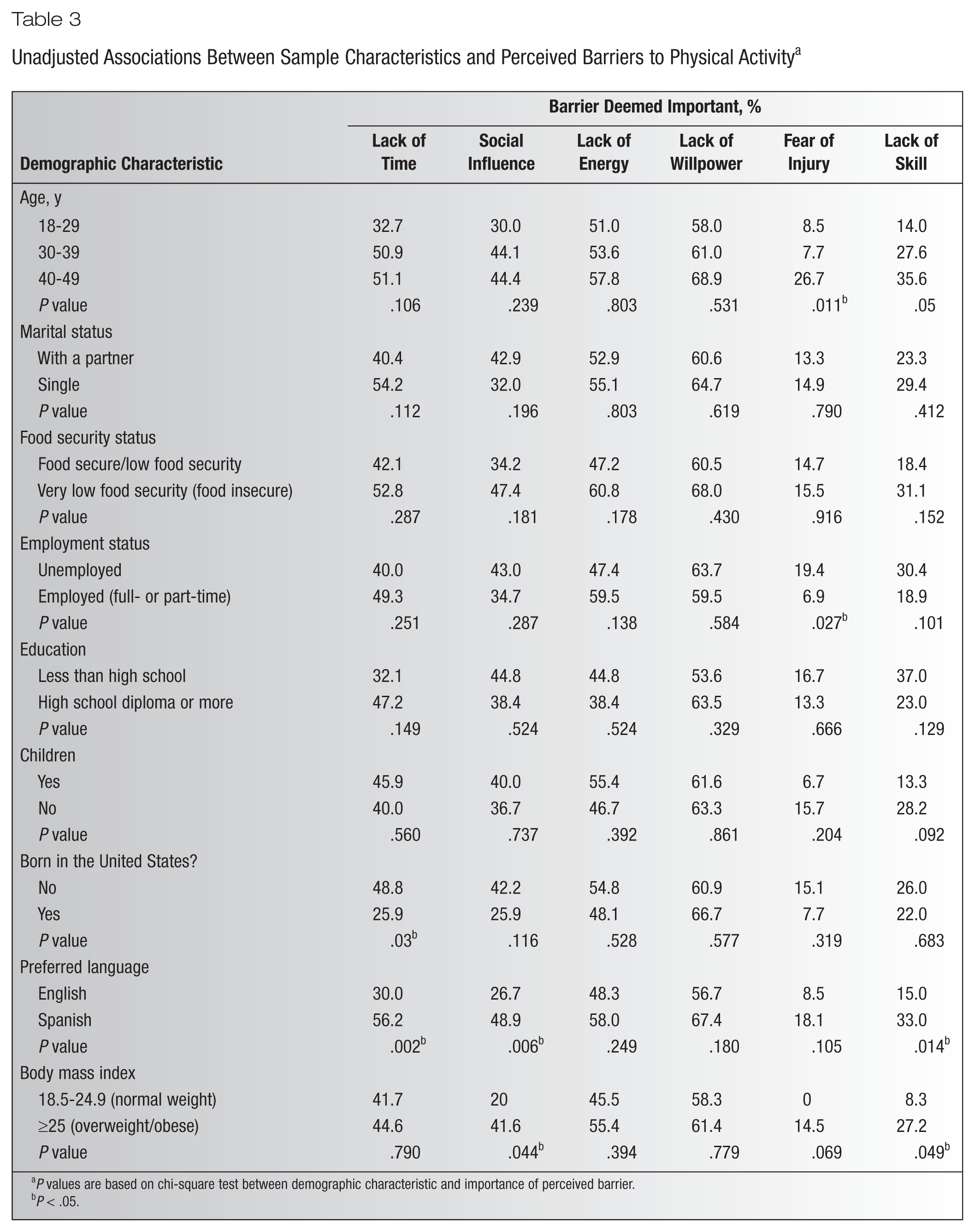
P values are based on chi-square test between demographic characteristic and importance of perceived barrier.
P < .05.
Multivariable Regression for Factors Associated With Perceived Barriers to Physical Activity
The authors carried forward any characteristic with an unadjusted association with the perceived barriers at a significance level of P < .1 into the multivariable models reported in Tables 4 to 7.
Regression for Social Influence
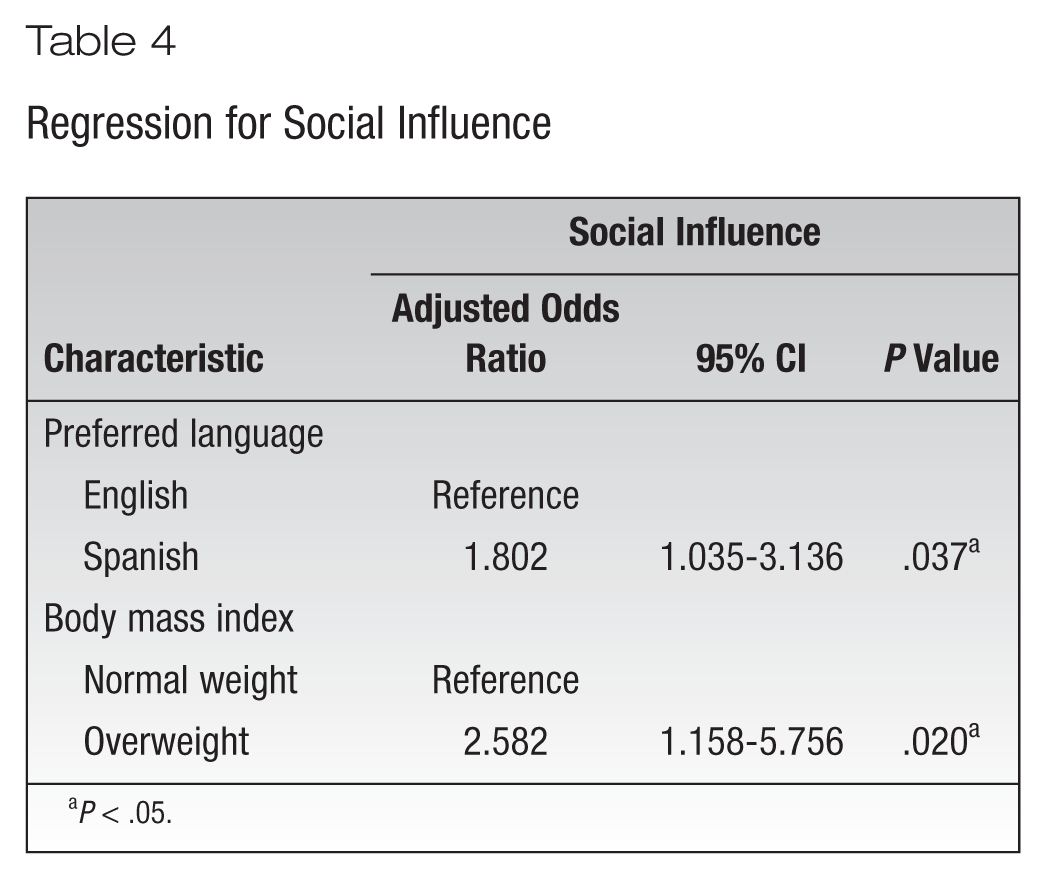
P < .05.
Regression for Lack of Time
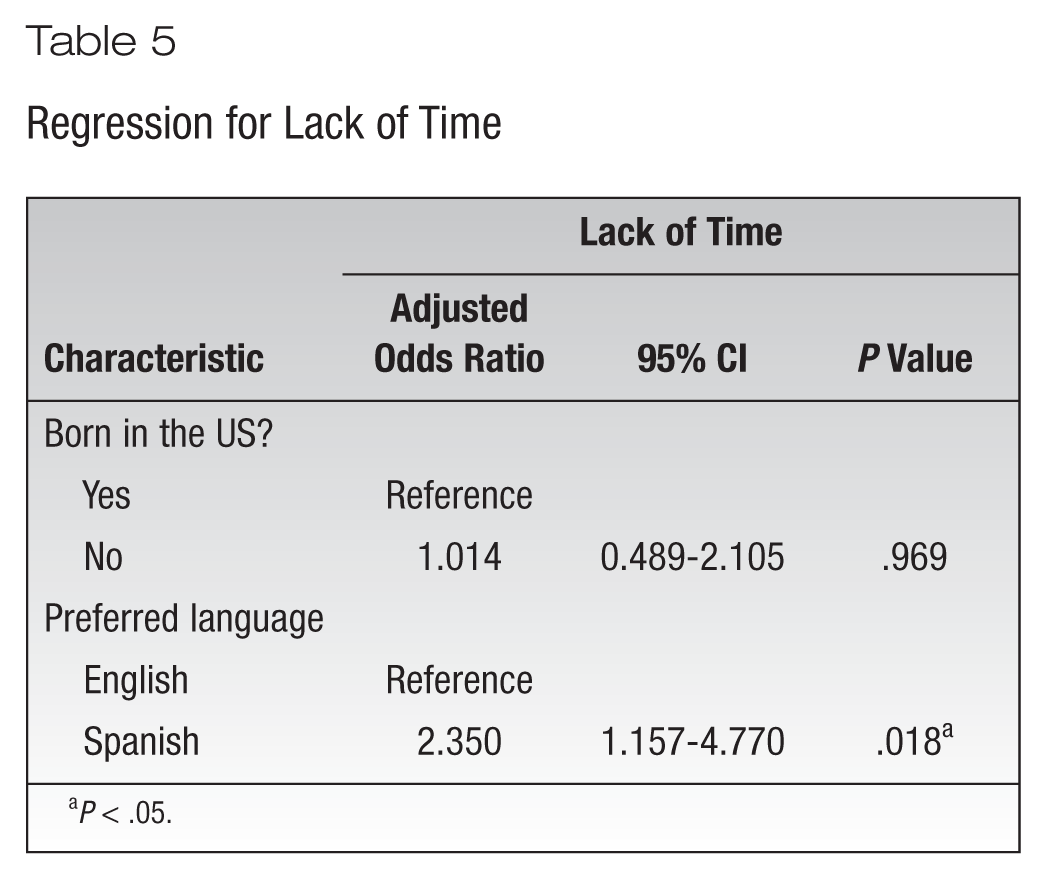
P < .05.
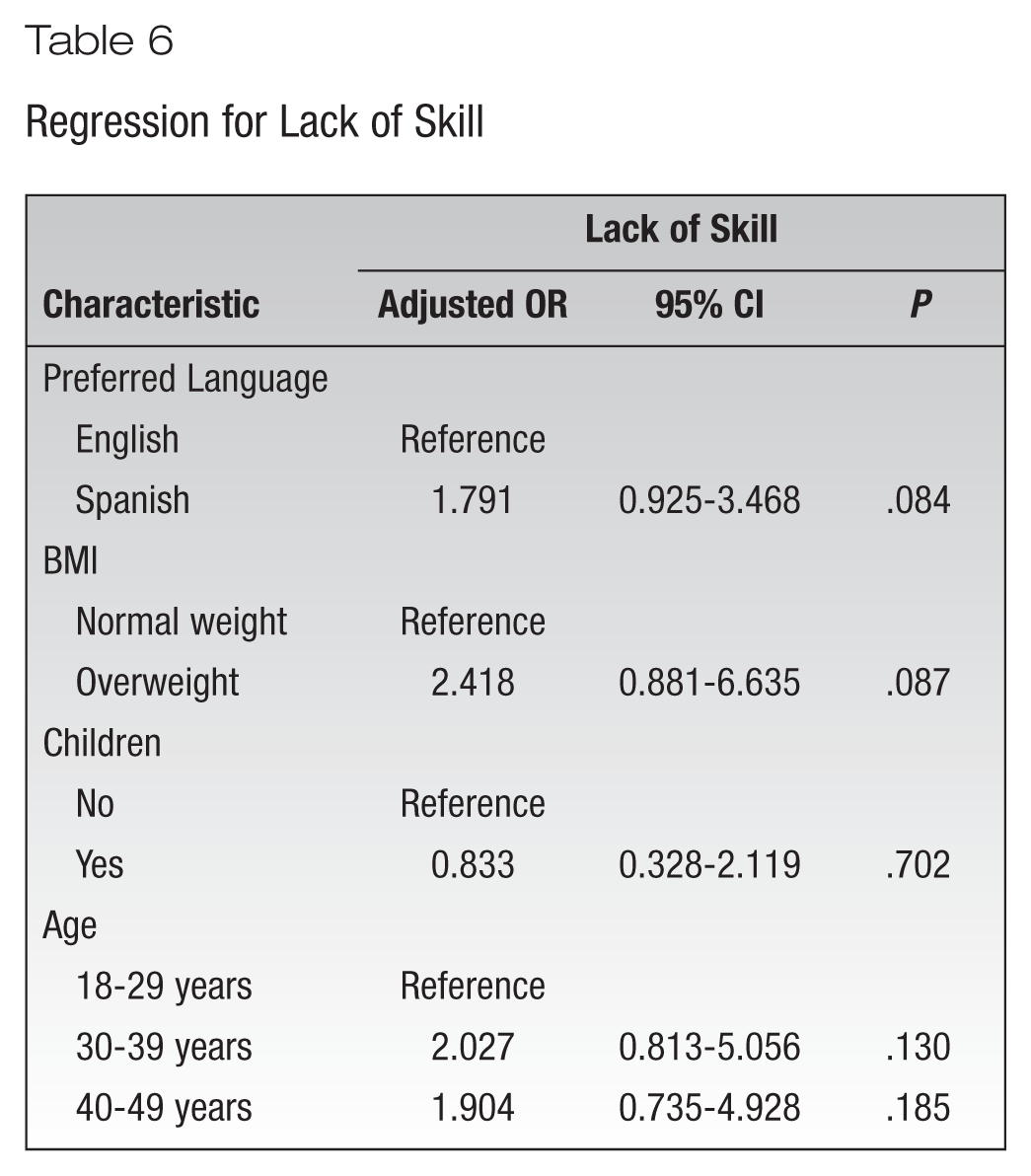
Regression for Lack of Skill
Regression for Fear of Injury a
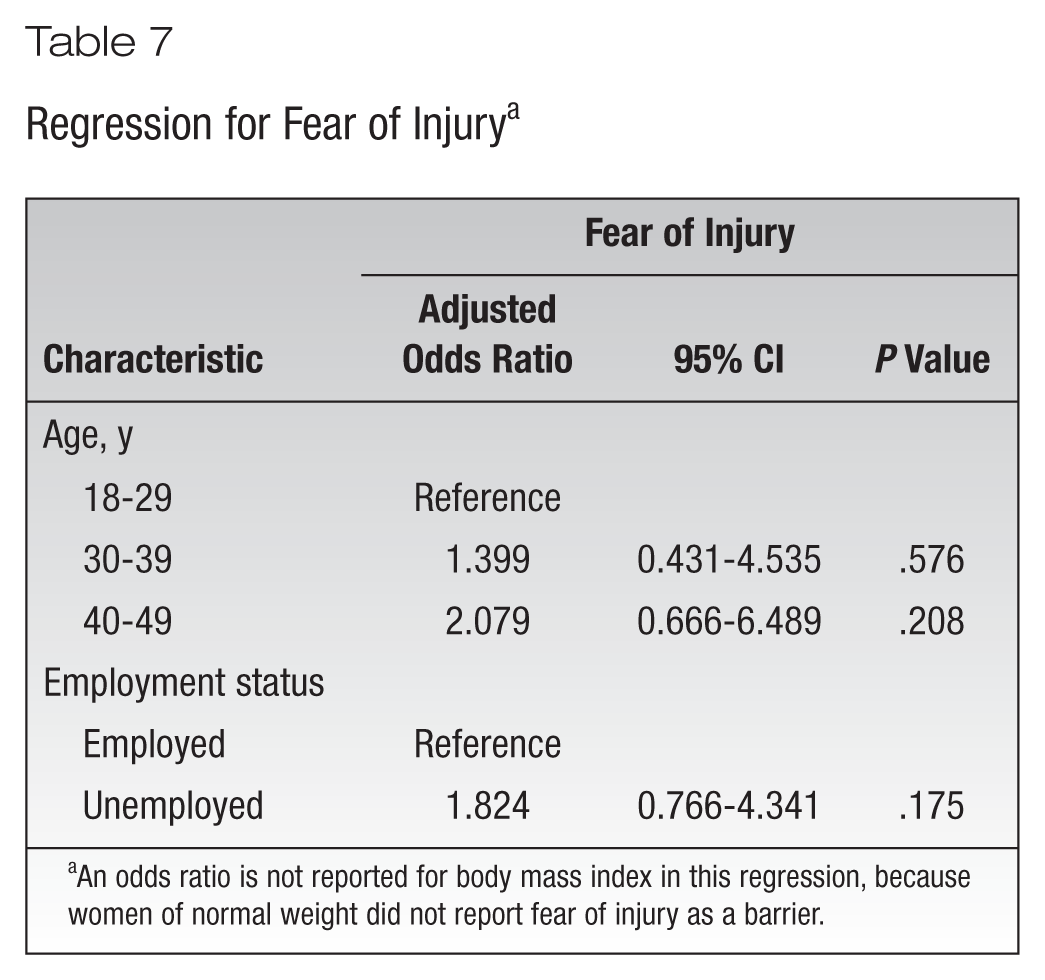
An odds ratio is not reported for body mass index in this regression, because women of normal weight did not report fear of injury as a barrier.
After adjusting for other characteristics, overweight/obese women were 2.58 times more likely than women of normal weight to report social influence (OR, 2.582; 95% CI, 1.158-5.756; P = .04) as an important barrier to exercise. Overweight/obese women were also more likely than women of normal weight to report fear of injury. In addition, when compared with women whose preferred language was English, women whose preferred language was Spanish were 1.80 times more likely to perceive social influence (OR, 1.802; 95% CI, 1.035-3.136; P = .04) and 2.35 times more likely to perceive lack of time (OR, 2.350; 95% CI, 1.157-4.770; P = .02) as important barriers. The authors did not report an OR for the association between BMI and perceived fear of injury, because no women of normal weight perceived fear of injury as an important barrier. However, to control for the variable, BMI was included as a predictor variable in the regression for fear of injury.
After adjusting for other characteristics, associations between age and perceived fear of injury and lack of skill became insignificant, as did the association between employment status and perceived fear of injury.
Discussion
The most commonly perceived barriers to physical activity among a sample of low-income Latina women at risk for type 2 diabetes were lack of willpower and lack of energy. Overweight/obese women and women whose preferred language was Spanish were more likely to perceive barriers to physical activity than were women of normal weight and women whose preferred language was English. While all women at risk for type 2 diabetes would benefit from physical activity counseling and interventions, these results suggest that efforts should target overweight/obese Spanish-speaking women in particular.
The main perceived barriers to physical activity experienced in this study’s population—lack of willpower and lack of energy—are consistent with those identified in previous research. However, most studies that identified these barriers to physical activity were conducted among adults with type 2 diabetes rather than among adults at risk for the disease.19,20,31,32 The findings of this study suggest that adults at risk for type 2 diabetes experience many of the same barriers related to lack of willpower and lack of energy that adults with type 2 diabetes experience, such as “laziness,” “tiredness,” “fatigue,” “stress,” and “low prioritization of exercise.”19,20,31,32 Among the current studies of adults at risk for type 2 diabetes, time constraints were frequently reported as a primary barrier to physical activity.24,25,33,34 In contrast, for women in this study, lack of time was secondary to the barrier categories related to internal motivation. These findings emphasize the need to address barriers related to lack of willpower and lack of energy, in addition to lack of time, to encourage physical activity among women at risk for type 2 diabetes.
Overcoming these barriers to physical activity may require the promotion of self-efficacy, defined as “people’s beliefs about their capabilities to exercise control over their own level of functioning and over events that affect their lives.” 35 One way of promoting self-efficacy may be to help individuals focus on factors that motivate, rather than impede, exercise. Examples of motivators to exercise identified among adults at risk for diabetes include an improved sense of well-being and the desire to serve as a positive example for their children.24,36
Other studies found that overweight and obese adults tend to perceive more barriers to physical activity and exercise less than do adults of normal weight.37,38 These prior studies support this study’s finding that overweight/obese women were more likely than women of normal weight to perceive social influence and fear of injury as important barriers to physical activity. The “social influence” and “fear of injury” barrier categories in this study included statements such as “I’m embarrassed about how I will look when I exercise with others” and “I’m afraid I might injury myself or have a heart attack.” Identification with these statements among overweight/obese women in this study is consistent with the fact that feeling “too fat” to exercise is a common barrier among overweight adults 37 and that negative self-image is often highly ranked as a barrier to activity among inactive adults. 39 However, this study’s finding that overweight/obese Latina women were more likely than women of normal weight to perceive social influence as a barrier is striking, as Latina women are more likely than other demographic groups to underestimate their weight and less likely to desire to lose weight.40,41
Previous studies have not examined the association between preferred language and perceived barriers to physical activity, so the findings of this study represent a new contribution to the literature. Although a study of urban-dwelling Latinas in the Midwest did not find any associations between language spoken at home (Spanish, Spanish and English, or English) and physical activity levels, 42 this study’s finding that women whose preferred language was Spanish were much more likely to perceive lack of time, and social influence as barriers to physical activity suggests that among inactive women, language may influence their ability to increase their physical activity levels through lifestyle changes. Previous studies of the influence of acculturation on physical activity levels among Latinos came to mixed conclusions, although higher levels of acculturation are often associated with lower levels of occupational activity and higher levels of leisure time activity.16,43,44 In this study, only preferred language—not years lived in the continental United States—was associated with the perception of barriers to physical activity. This finding is consistent with a study of first-generation Latino women living in North Carolina, which found that the likelihood of meeting physical activity recommendations was associated with higher English acculturation and arriving in the United States before age 25 but not with time lived in the United States. 45
This study has several limitations. As a result of this study’s cross-sectional design, causality cannot be inferred. However, the associations between demographic factors and perceived barriers to physical activity do indicate that in situations where time and resources for physical activity counseling are limited, overweight/obese and Spanish-speaking patients may benefit the most. Another limitation is the self-reporting of height and weight to determine BMI. Because recruitment for and completion of the study surveys took place in a clinic, however, most participants had their height and weight measured by a health care provider before they submitted the survey to the research team. In addition, this study did not include lack of resources as a barrier category in analyses, because the survey item’s low Cronbach’s alpha (which measures how closely related items in a group are) indicated low reliability of this particular measure. Previous studies found that external factors, such as community safety, transportation, and cost of fitness facilities, are important barriers to physical activity among Latino/a adults,34,46 and these barriers would have been encompassed in this study’s “lack of resources” barrier category. Still, this study’s findings that the population’s main perceived barriers were related to a lack of internal motivation emphasize the need for counseling and other strategies that promote self-efficacy. Finally, it is possible that the translation of the survey from English to Spanish contributed to some of the differences between English- and Spanish-speaking groups. However, a provider fluent in Spanish and familiar with the study population checked the translation, and the survey was piloted for comprehension and flow; thus, the effects of translation on the results were minimized.
Implications and Recommendations
The perceived barriers to physical activity identified in this study may be best addressed through promotion of self-efficacy. Self-efficacy is one of the most consistent predictors of greater levels of physical activity.46-48 The primary barriers to physical activity that women in this study perceived were lack of willpower and lack of energy, so helping women identify and act on motivators to engage in regular exercise is crucial to promoting lifestyle change. Adults at risk for and with type 2 diabetes identified the sense of well-being derived from exercise, weight loss, social relationships related to exercise, and encouragement from others as factors that motivate regular physical activity.24,33,36 Incorporating these motivators into counseling and other strategies to promote self-efficacy among sedentary low-income Latina women may help them overcome lack of willpower and lack of energy as barriers to physical activity.
Counseling for physical activity is effective in promoting increased physical activity among previously sedentary patients,49-53 and findings of this study suggest that Latina women at risk for type 2 diabetes would benefit from physical activity counseling. However, since limited time with patients often prevents physicians and other healthcare providers from providing adequate counseling, 54 counseling should be targeted toward those individuals who would benefit from it most. This study suggests that overweight/obese women and women whose preferred language is Spanish may benefit the most from counseling that helps them overcome the barriers to physical activity that they perceive. For overweight/obese women who are more likely to perceive social influence and fear of injury as barriers, effective counseling methods may entail helping them determine which forms of exercise and in which settings alleviate their concerns about appearance or their fears about hurting themselves. For women whose preferred language is Spanish, providing physical activity counseling in Spanish and offering culturally appropriate exercise options may help them overcome the barriers to exercise that they perceive.45,55,56
In conclusion, the main barriers to physical activity perceived by low-income Latina women at risk for type 2 diabetes were lack of willpower and lack of energy, and overweight/obese women whose preferred language was Spanish were more likely to perceive barriers to exercise. Thus, strategies to increase physical activity for this population should focus on promoting self-efficacy and should target overweight/obese Spanish-speaking women. Future development of and research on culturally specific exercise counseling and promotion programs are needed.
Footnotes
Funding sources:
Yale Global Health Field Award, Yale Global Health Seed Funding, Yale College Fellowship for Research in Health Studies, and Yale Collaborative Action Project.