
Abstract
Purpose
The purpose of this qualitative study is to explore familial patterns that may be related to type 2 diabetes (T2DM) and to patients’ ways of coping with the illness.
Methods
A purposive sample of 32 Israeli Jewish (n = 12) and Arab (n = 20) individuals with T2DM were recruited from a community population and interviewed about their familial experiences and their illness. Interview data were analyzed using Colaizzi’s phenomenological method.
Results
Many participants, particularly from the Arab society, reported familial patterns that suggest fused relationships and emotional cutoff. They described highly close and positive family relationships, on one hand, but demonstrated unwillingness to share their difficulties with their family members, on the other hand. Precipitating stressful or traumatic events and day-to-day stress appeared as leading perceived causes of the illness. Maintaining an appropriate lifestyle, stress reduction, and family support were the main coping strategies with the illness.
Conclusions
The findings suggest a possible avenue in which fusion with family members and inability to attenuate emotional distress by sharing difficulties with others may contribute to the development of T2DM. Assessment of such family dynamics and ways of coping with stress could lead to more appropriately nuanced treatment for individuals with T2DM and prediabetes.
Diabetes mellitus type 2 (T2DM), characterized by the body’s resistance to insulin, 1 is considered a universal epidemic, with the number of patients with diabetes steadily increasing. 2 Cumulative findings suggest that psychological and sociopsychological factors, particularly those associated with heightened stress response, contribute to the onset and progression of T2DM. 3 In particular, increased risk for T2DM was found in individuals exposed to major adverse experiences, such as trauma, business failure, or family crisis, 1 as well as stressful environments, anxiety, 4 and depression.5,6 Moreover, among patients with T2DM, depressive symptoms are associated with poor psychological adjustment to diabetes and poor metabolic control. 7
The mediatory pathways between adverse psychosocial factors and T2DM are not fully understood but may involve greater engagement in known behavioral risk factors for T2DM (eg, poor diet, smoking) 8 and/or the overactivation of the major physiological stress mechanisms: the hypothalamus-pituitary-adrenal (HPA) axis and the sympathetic nervous system. Specifically, overactivation of the HPA axis and the sympathetic system, which is associated with anxiety 9 and depression, 10 may lead to suppression of the insulin receptors in the body, which could result in insulin resistance and the development of T2DM. 11 Thus, psychological factors that may influence the individual’s tendency to experience events as stressful and to manage stress-inducing situations may influence the risk of developing T2DM. These may include personality traits and coping styles. 12 Indeed, risk for T2DM is higher in individuals with personality traits that put them in conflict with others, 3 such as trait anger.13,14 Another important potential factor is social support, which may include instrumental support as well as emotional support and companionship. 15 A meta-analytic review of longitudinal studies concluded that low social support (resulting from unstable partnership, poor family contact, loneliness, etc) was more strongly associated with poorer diabetes control than were stressful events and stress-prone personality or coping style. 12
As the individual’s family is a major source of support, patterns of familial relationships may particularly affect the risk for developing T2DM. Moreover, from a developmental perspective, familial patterns develop early in life and continue to shape basic attitudes toward the self and one’s relation to significant others throughout the life span and thus may influence the individual’s ability to cope with stressful situations. 11 Consistent with this view, a recent study has found an association between dysfunctional family patterns in childhood and adverse psychosomatic symptoms in adulthood, with levels of depression mediating this association. 16
Familial patterns may also be highly important for the ability to cope with T2DM following diagnosis. Indeed, patients with T2DM report that family members were very important in providing support and improving the ability to cope. 17 Yet, the effectiveness of family support may depend on the nature of the relationships in the family, as evident by data suggesting that patients with T2DM who engage in an open and collaborative form of spousal involvement in their coping with the disease demonstrate better adherence to a healthy diet and lower diabetic distress.18-20 Although family patterns, to which the individual was exposed to as a child, have a long-term impact, 21 both on his or her interpersonal interactions 22 and on physical 23 and mental health in adulthood,24,25 the specific familial patterns (in the current family and in the original family of the individual) that may be associated with the development of T2DM and with coping with the disease remain largely unknown.
Finally, familial patterns may differ between people of different cultural and social backgrounds. For example, collectivist societies, such as that of the Arab minority in Israel, are characterized by close family relationships 26 and a traditional patriarchal structure. In the Arab society in Israel (21.09% of the population), considerable emphasis is put on nuclear and extended family ties, and much effort is devoted to preserving and strengthening the family as a major source of emotional, social, and economic support.27,28 It was reported, however, that individuals of Arab origin, especially Arab men, rarely share their feelings with significant others.24,28 It is important to note that members of the Arab minority in Israel have significantly higher rates of T2DM than the Jewish majority. 26 As observed with other minority groups, such as Latinos and African Americans in the United States, 23 these higher rates of T2DM could partially result from differences in lifestyles (eg, smoking, diet), socioeconomic status, and exposure to stressors. However, it is also possible that familial patterns 24 play an important role in their heightened risk of T2DM.
Research Questions and Aims
Given that the role of psychological and familial antecedents in the etiology of T2DM has scarcely been investigated, and given the complex and rich nature of familial relationships, this research explored family experiences of Jewish and Arab individuals with diabetes with the aim of beginning to identify and describe familial patterns that may be related to the development of T2DM, ways of coping with stress in general, and coping with the disease.
The goals of the current study were addressed using a phenomenological qualitative methodology 29 intended to explore the subjective experiences of the participants. The research questions were 5-fold: (1) What is the meaning of family to participants? (2) What characterizes relationships in their family? (3) How do participants cope with daily difficulties? (4) What does it mean for participants to have diabetes? (5) Is there an association between having diabetes and the experiences in the family? Research questions 1 and 2 were formulated to address family relationships, question 3 to explore participants’ ways of coping with stress not necessarily related to the illness or to family relationships, question 4 to specifically address their experiences with the illness, and question 5 to explore possible connections between the illness and family relationships.
Methods
Participants
Purposeful sampling was used with the inclusion criterion of being an adult diagnosed with diabetes. The study was advertised through word of mouth in local communities in northern Israel, and via the snowball method, participants referred us to other individuals they knew who had diabetes. Thirty-two individuals who were interviewed (12 Jews and 20 Arabs; see Table 1) were diagnosed with T2DM (with blood glucose levels of 125 mg/dL and over among the major diagnostic criteria) and resided in northern Israel. The Jewish sample included 6 men and 6 women with a mean (SD) age of 57.8 (8.78) years. Most (9) were married, while the rest (3) were widowed. The mean (SD) years of education was 10.9 (1.80). The Arab sample included 10 men and 10 women with a mean age of 54.1 years (5.83). Sixteen were Sunni Muslim and 4 were Catholic. All but 1 were married. The mean (SD) years of education was 13 (1.80). Participants of both samples belonged to the middle socioeconomic class with the exception of 1 participant from each sample reporting low income. The complete study protocol was approved by the College Institutional Review Board.
Demographics of Participants a
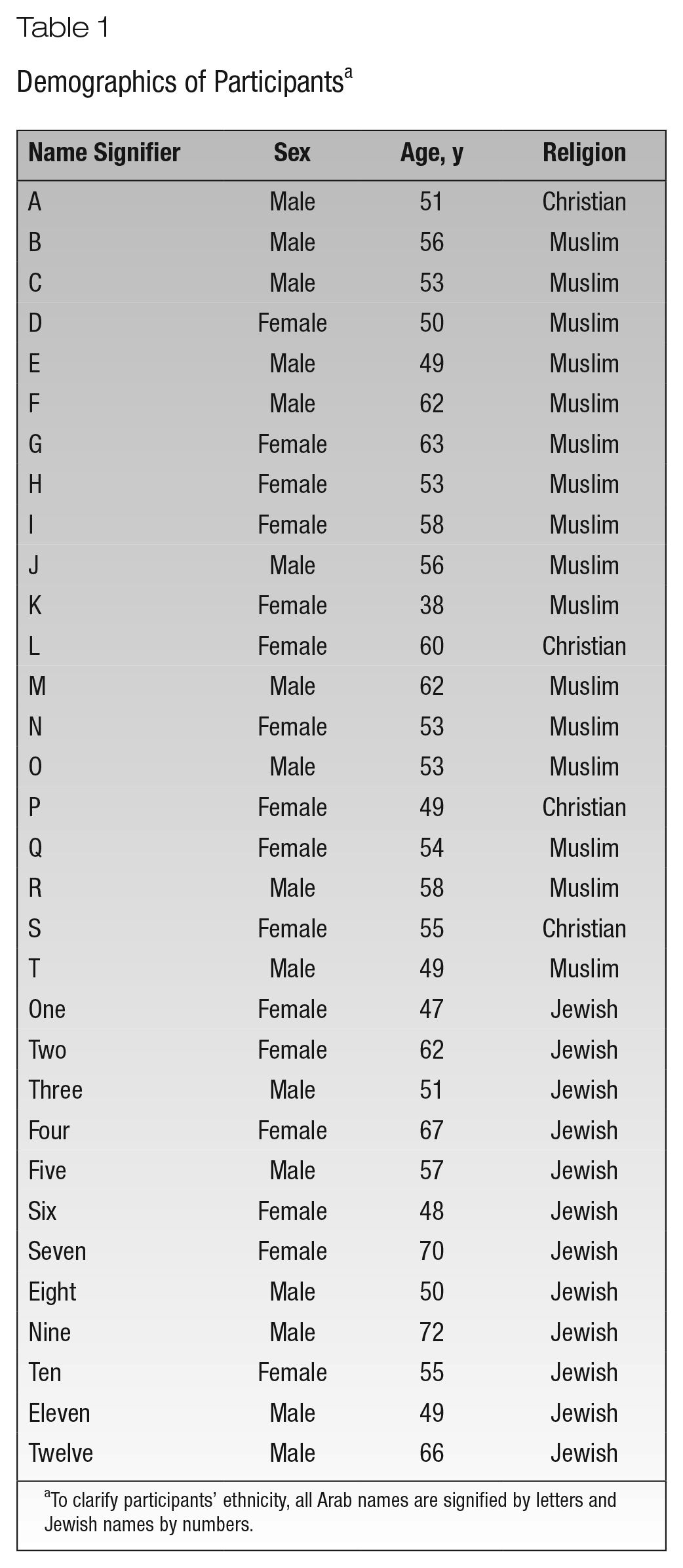
To clarify participants’ ethnicity, all Arab names are signified by letters and Jewish names by numbers.
Measures
The measures consisted of a demographic questionnaire, which included questions regarding age, number of children, marital status, and so on, and a semistructured interview guide based on the research questions. The interview was composed of a series of general questions that allowed for more detailed follow-up questions based on how each interview developed. Interview questions were as follows:
What is a family to you?
What is your experience in your family?
How was it like growing up in your family for you? (research question 1)
What characterizes the relationships in your family?
How do you feel about your relationship with your family members? (research question 2)
How do you deal with day-to-day difficulties?
When you are stressed, what do you do? (research question 3)
What does it mean for you to have diabetes?
What difficulties arise? What makes it easier?
Please tell me about your lifestyle. Is your lifestyle affected by the diabetes in any way? If yes, how? (research question 4)
Do you think the development of your diabetes is related to anything?
Do you think there is a connection between your family experience and your illness? If yes, what? (research question 5)
Procedure
Data were collected by 3 female research assistants, 2 Arabs and 1 Jewish, who were graduate students in school counseling, trained specifically for this study by the second author, who has substantial experience conducting qualitative research. The first step of the study involved bracketing 30 by the interviewers and the second author—a process of self-reflection aimed at becoming aware of one’s expectations, biases, stereotypes, and prejudices regarding the phenomenon studied, in order to put these aside (“in brackets”) so they will influence data collection and analysis as little as possible. The bracketing process continued and was documented throughout the study. Next, participants were given information about the study, including their right to discontinue participation at any time and assurances of anonymity. They then filled out an informed consent form and the demographic questionnaire. Finally, they were interviewed in private, and the interviews were audiotaped and transcribed verbatim.
Data Analysis
Analysis was based on the phenomenological method by Colaizzi. 31 It included 6 steps (see also Demir and Ercan 32 ): (1) reading the interview protocols to get a sense of what was said; (2) extracting meaningful statements from each protocol; (3) giving meaning to each statement; (4) identifying clusters of themes from shared meanings among protocols (themes were usually deemed significant when they were common to at least half the participants or half of each ethnic group), and at this stage, themes were also compared to the interview transcripts to check for interpretation accuracy; (5) writing a rich description based on the clusters of themes; and (6) describing the essence of the phenomenon by identifying its most basic elements.
Trustworthiness
Several verification steps31,33,34 were taken to increase the study’s rigor and strength by enhancing its quality of validity and reliability. For example, (1) bracketing was employed before and throughout the data collection, analysis, and interpretation; (2) interviews and analyses were performed by research assistants from the same cultural background as the participants to enhance understanding and rapport; (3) summary of the bracketing journal and all stages of analysis were documented in writing and reviewed by the principal investigators; (4) the second author read all transcripts, reviewed all analyses, and performed an independent analysis of the entire data, and where there were discrepancies in interpretation or understanding, these were clarified, worked through, and mutually agreed upon; (5) because the study is exploratory, due to the complex nature and limited knowledge about family experiences of individuals with diabetes, extra care was taken to identify and describe only the strongest and most evident themes that emerged; and (6) many quotes from the actual interviews are presented in the Results section to demonstrate and verify the identified themes. Overall, the composition of the research team, which was diverse in terms of religion, ethnicity, sex, age, and expertise, allowed for multiple lens and ways of understanding and can be viewed as a strength of the current study.
Results
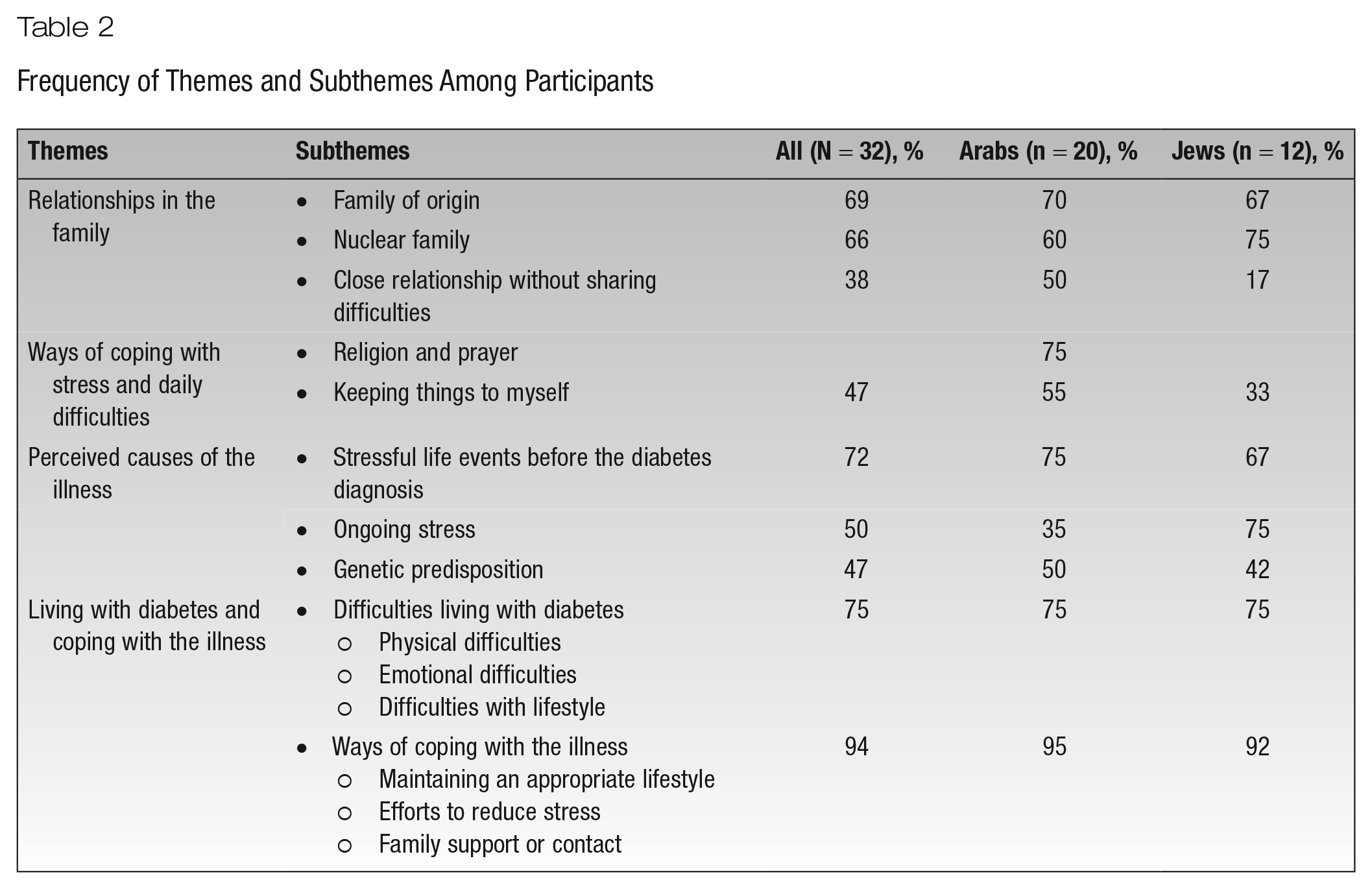
Results are presented according to 4 main themes identified from participants’ interviews: (1) relationships in the family, (2) ways of coping with stress and daily difficulties, (3) perceived causes of the illness, and (4) living with diabetes and coping with the illness. Table 2 details the identified themes and subthemes and their frequency among participants. Quotes were translated from Hebrew and Arabic. Where meaningful, results were presented separately for Jews and Arabs. To assist with identifying the ethnicity of the participant quoted, names with letters signify Arabs while names with numbers signify Jews.
Frequency of Themes and Subthemes Among Participants
Relationships in the Family
The participants discussed their relationships in the family of origin and in their nuclear family. Three subthemes were identified across participants: (1) family of origin, (2) nuclear family, and (3) close relationship but without sharing difficulties.
Family of origin
Overall, descriptions of relations in the family of origin tended to be very positive, and participants reported they had very close and meaningful contact with family members. Most interviewees (14 Arabs and 8 Jews) described relationships with parents and siblings as very warm, close, and based on love and caring. Mr C said, Family is the essence of life. . . . [My] family of origin is a very warm family, supportive. It’s a family that simply provided a very, very good atmosphere. Egalitarian, with a lot of love, with a lot of drive for success.
Seven participants (6 Arabs and 1 Jew) described distant and cold, or more complex, relationships with individuals in their family of origin. Mr R said, The truth is that there were no emotions in our relationships. I don’t remember, even when I was little, that I came and told my father or my siblings things that bothered or hurt me. I don’t know why, but that’s the way it was. Yes, you could say there were cold relationships between us.
Of note is that, among the Arab participants, half stated they grew up in a large family with low socioeconomic status and financial problems.
Nuclear family
Similar to the descriptions of relationships in the family of origin, most participants (12 Arabs and 9 Jews) described close and strong relationships in the family they created. Ms D said, “In our family I feel there are very good and strong relationships. There’s compassion, love, concern, and caring about each other, and that’s something that I don’t experience or see anywhere else.” More than half the participants (10 Arabs and 7 Jews) reported that their nuclear family is highly important and central to their lives. Some of their statements also suggest some lack of psychological differentiation. In Ms Six’s words, “My kids, they are the air I breathe. I dedicated my whole life to them.” Speaking about her family members, Ms Seven said, “I care about them and I love them and they are my life. I don’t think about anything but them.” Ms K similarly stated, I come back from work and long to see them again every day. They are the air I breathe . . . I love them to death, they are life. For me, let God give me life so I can motivate them and give them independence, and after that I don’t care if I die or my life ends. I go to work and in the morning think only of them.
Close relationship without sharing difficulties
Half of the Arab participants and 2 of the Jewish participants exhibited a pattern in which they described highly close and positive family relationships but, when asked how they deal with stress or difficulties, said they tend to cope alone and avoid discussing these topics with others or do so very rarely or with few people. This pattern may suggest idealization of family relationships, when in reality there is more emotional distance than one would wish to acknowledge. For example, Mr M described his very close relationship with his siblings: It’s a type of love. We can’t get far from each other. Our relationship is strong. I have to see them every day. The eldest, who retired, comes through my grocery store every morning, drinks his coffee here, goes to the center of town and sits with friends, prays in the mosque, buys things for the house and then comes back. Sometimes even on his way back he drops in to say hello.
Nonetheless, when asked how he deals with daily difficulties, Mr M answered, “With every difficulty I had, the first thing, I would keep it to myself and not tell [anyone]. So if something happened with my children, only my wife and I would take care of it.” When the interviewer mentioned that he had said that he has a good relationship with his siblings and asked if he does not share the difficulties with them, Mr M replied, No way. We are used to sharing happiness together, but with difficulties at each home, [it’s only] for [that] home. Like our father made sure that things would stay within the walls of the house and not go beyond it. That’s the way I do it and my siblings [do it] in their home. I love my siblings, but what would they care if I’m in a fight with my wife or if one of my children has a problem?
For some participants, it seems that closeness meant spending time together but not necessarily sharing private emotional experiences or issues. For example, Ms Q also described her family in a highly positive manner: Family is everybody together, family is closeness, love, respect for one another, how you speak with each other, how you visit each other, how you help, support, and contain in moments of distress. Family is the backbone in the life of each of us. It’s the wall we lean on when we’re weak, broken or hurt. The family is also our base in moments of happiness, on happy occasions, weddings, and so on. Family is simply everything.
When asked how she deals with daily conflicts and stress, she nonetheless replied, When I’m in distress or a situation that stresses me, I tend to isolate myself. I pray because that really helps me calm myself down. Usually I don’t like to share with others when it’s something that depends on me and I can solve myself. Only my sister is very close to me and if I, for some reason, want to share with someone, I turn to her.
Ways of Coping With Stress and Daily Difficulties
Participants mentioned varied coping strategies to deal with stress, such as walking, smoking, and seeking help from mental health professionals. But only 2 means of coping emerged as common themes: (1) religion and prayer and (2) keeping things to myself.
Religion and prayer
Most Arabs (15) mentioned that faith in God and prayer are an important and helpful means of dealing with difficulties. Praying helped them calm down and gave them strength and hope for a better future. Mr B explained, Since I was little, every conflict that I’m in, I turn to God and to prayer. I’m a person who really believes in God, and it’s something that really gives [me] strength. . . . If I feel tired or stressed or anything else, I go and pray and then I calm down.
Keeping things to myself
Similar to the pattern mentioned earlier, almost half the participants (11 Arabs and 4 Jews) reported that they do not share their feelings and inner experiences with others or do so very rarely. Mr R related his tendency to withhold his feelings to the pattern he learned in his family of origin: In our home there wasn’t sharing of sadness or grief. [If I have] stress or a personal problem, I take care of it by myself . . . I always share with my wife. Not everything . . . I’m used to dealing with stress and difficulties alone . . . I never had a partner to help with the challenges and to cope with experiences in my life . . . I don’t express emotions with my children. That’s how I grew up and what I got used to.
Five Arabs saw sharing difficulties with others as a sign of weakness, and some reported efforts to conceal their emotions from others. Ms G said, First, as much as the difficulty is great, I make an effort for no one to know and always show the opposite [feeling] outwardly. Because I don’t want to be [the] poor [person] or get pity from others. I prefer being alone. I do a deep self-examination and get to the bottom of it.
Perceived Causes of the Illness
Participants mentioned several causes they believed to be related to their illness, and 3 main causes emerged as themes: (1) stressful life events before the diabetes diagnosis, (2) ongoing stress, and (3) genetic predisposition.
Stressful life events before the diabetes diagnosis
Most participants (23) reported that they had experienced a traumatic or very stressful event shortly before they were diagnosed with the illness (usually up to a year beforehand). They believed these stressors led to the onset of the disease. The negative situations they mentioned were mostly related to family members and included events such as death of a relative, family conflict, divorce, or a difficult financial situation. Mr Five connected the death of his daughter to the onset of his illness: We lost our daughter 6 years ago when she was in the military. An only daughter. She was 19 [deep breath]. Even today [drinks water], it’s not something that goes away. The more time passes, the more you think of her . . . yes, after what happened with my child . . . you have to be strong for your wife and kids, but who has strength anymore? My body collapsed.
When asked whether he discovered he had diabetes after what happened to his daughter, he replied, “Yes. Exactly that. I believe it’s connected. There’s no remedy for stress.” Ms S described how family conflict brought about her illness: And then [my son] told me about the girl he met. And at that time I got diabetes because it was a very difficult time. I was very nervous, the girl was very rude, treated us badly and I didn’t want her for my son, especially when I understood that he stopped his studies because of her. That’s why I really struggled with him and it was a really stressful time until he agreed to give up this relationship.
Ongoing stress
In addition to stressful or traumatic events, half the participants also described a pattern of ongoing stress throughout periods in their lives that they believed contributed to the onset of their illness. These stressors mainly included everyday burdens, overload or worries, and family problems and conflicts. Mr C described his daily stress: I think that everyday stress, tension, and those sorts of things can make things worse and affect the onset of the illness. And these are things that I generally experience in my day-to-day life, but I try as much as possible not to get into stressful situations, and with all the obligations and my crazy schedule and all those things, I try to be a more relaxed person.
Genetic predisposition
Half the Arabs (10) and almost half the Jews (5) mentioned that they have at least 1 close family member with diabetes and that they believe there is a genetic predisposition for their illness. Ms P said, “I think the basis for the diabetes is hereditary, because both my parents and another brother are type 2 diabetes patients.” Some participants believed it is possible there is an interaction between the genetic component and stress or lifestyle that caused the illness. Mr Five said, My older brothers have problems with sugar too, because they didn’t stick to [an appropriate lifestyle]. They ate sweets, didn’t go for checkups, didn’t exercise. In the end their body collapsed. I have a sister who goes to the hospital every week because her sugar goes up. But she doesn’t stick to [an appropriate lifestyle]. Doesn’t listen to what she’s told. . . . We probably got it from dad. In his family there were also people with sugar problems.
Living With Diabetes and Coping With the Illness
Two subthemes emerged regarding the way participants experienced and dealt with their illness: (1) difficulties living with diabetes and (2) ways of coping with the illness.
Difficulties living with diabetes
Most participants (24) reported difficulties related to their illness. Three types of difficulties were mentioned: (1) physical, (2) emotional, and (3) lifestyle.
Physical difficulties
Most participants (21) reported experiencing pain in various body parts, fatigue and the need for rest or sleep, difficulty walking for long periods of time, lack of energy, and medical problems. Mr Eleven said, First of all, by definition, you become a sick person. You can’t do anything about it. You can’t do everything you want. Suddenly things you did in the past that seemed obvious, now seem really hard. . . . Like simple activities, like walking, eating without taking a pill. It’s not a feeling of freedom like in the past.
Emotional difficulties
More than half of the participants (17) reported emotional difficulties, such as stress, disturbing thoughts about the illness and its complications, fear of death, changing moods, and worries about the family. Mr B said, “It’s also very difficult mentally, because I feel [the illness] is taking over my body and affecting other aspects. That’s why I’m worried about it and that the end is near.”
Difficulties with lifestyle
Seventeen participants (11 Arabs, 6 Jews) mentioned having problems with their daily routines. These included sleep issues, difficulty maintaining a diet and refraining from eating foods they like, and difficulty taking medication on a regular basis. Ms S described how hard it is to maintain a healthy lifestyle, also mentioning emotional and physical difficulties in the process: Emotionally, it really affects my mood when I’m in pain, taking medication, and having tests and checkups all the time. When I stick to the right diet—but I can’t always restrain myself. I try, but I don’t always succeed. Giving up things I like is difficult.
Ways of coping with the illness
Almost all participants (30) mentioned ways they deal with their illness. Three strategies emerged as subthemes across participants: (1) maintaining an appropriate lifestyle, (2) efforts to reduce stress, and (3) family support or contact.
Maintaining an appropriate lifestyle
Most participants (25) felt it was important to maintain a healthy lifestyle to deal with their diabetes. This mainly included an appropriate diet, taking medication, and exercising. Most described a change in their lifestyle after they were diagnosed and a need to learn new habits. Ms P said, I really make sure that I don’t eat [foods] with sugar or any food that raises the blood sugar. I take medication responsibly, and as for exercise, my husband and I go out walking once or twice a week in the village.
Efforts to reduce stress
More than half the participants (17) reported that they make an effort to relax and remain calm as much as possible as a way of dealing with their illness. Some of the strategies mentioned were thinking positively about their situation, seeking solace in faith, and avoiding thoughts about their illness. Ms Ten described how she deals with her stress: I breathe and count to ten. . . . It’s advisable, if you suffer from diabetes, that you don’t get stressed. It simply exhausts you . . . so it’s really important not to be stressed. It’s hard to put into practice but it’s true. It’s things you have to learn. A lot of self-work.
Family support or contact
Fifteen participants (10 Arabs and 5 Jews) stated that their family members are a source of support and provide caring, emotional containment and help with daily needs. Ms S noted, “My family really helped me with the coping process with the illness and to this day they help and make sure I don’t eat unhealthy food.”
Discussion
The current study examined family relationships of Jewish and Arab individuals with T2DM and their ways of coping in general and with the illness. The results suggest several possible links between family patterns and ways of coping with stress that may contribute to the participants’ vulnerability to the illness. Overall, findings depict similarities but also some important differences between the Arab and Jewish participants.
Many of the participants emphasized the family as an important source of support. However, an in-depth analysis of the interviews revealed a complex picture regarding the extent to which the participants actually turn to their family members when troubled or emotionally distressed. Most participants viewed their family of origin and their current nuclear family as fundamental parts of their lives and as sources of their sense of identity and well-being. Consistently, many of them reported having close, warm, and supportive relationships with their family members in the past and present. Nevertheless, half of the Arab participants (but only 2 of the Jewish participants) exhibited a pattern in which they described highly close and positive family relationships, on one hand, but unwillingness to share their difficulties with their family members, on the other hand.
This apparent discrepancy may be interpreted in 2 nonexclusive ways. First, it may reflect a tendency to idealize family relationships, when in reality there is more emotional distance than one wishes to acknowledge. Second, it may reflect a sociocultural expectation that individuals deal with their negative feelings and difficulties on their own, without bothering others. Indeed, these participants attested to having close ties to other family members but did not necessarily use these ties as a means of sharing their personal issues and receiving advice or support. Moreover, some participants overtly stated that revealing one’s difficulties is a sign of weakness that should be avoided. It is also of interest that some of the participants described their feelings toward their family members, particularly their children, through statements that imply high dependency and fusion.
These tendencies expressed by the participants correspond well with the concept of differentiation of self in the family therapy theory of Kerr and Bowen. 25 The result of relationship experiences within the family in early life, differentiation of self is defined as the degree to which one is able to balance emotional and intellectual functioning as well as intimacy and autonomy in relationships. 25 Importantly, unwillingness to involve family members in one’s emotions and distress (termed “emotional cutoff” by Kerr and Bowen 25 ) and fusion with others are considered 2 key factors related to the individual’s level of differentiation of self.
According to the theoretical assumptions by Kerr and Bowen, 25 emotional cutoff deprives a person of resources by isolating him or her from those who might render valuable help, leading to greater anxiety and emotional distress. 21 As for fusion with others, the creation of significant relationships with unclear boundaries increases difficulties because it produces considerable dependence, which in turn negatively influences the regulation of anxiety and stress. 22 Indeed, previous studies found high levels of emotional cutoff and fusion with others to be associated with trait anxiety, 22 depression, 35 heightened emotional distress, 36 and physical symptoms associated with stress, such as fibromyalgia. 37 Thus, it is possible that fusion with family members and emotional cutoff may contribute to the development of T2DM in these participants by increasing their vulnerability to experience emotional distress.
As mentioned, the Arab minority in Israel has significantly higher rates of T2DM than the Jewish majority. 26 Consistent with previous studies on the perceptions of the family in Arab society in Israel as a major source of emotional, social, and economic support,27,28 most of the Arab participants in the current sample emphasized the family as an important source of support. However, as mentioned above, half of the Arab participants exhibited unwillingness to share their difficulties with their family members (ie, “emotional cutoff”). This is consistent with previous studies that found emotional cutoff to be more common among Arabs than Jews and to be associated with higher levels of stress and anxiety (eg, Peleg and Zoabi 24 ). Certainly, other factors are also likely to contribute to the higher T2DM rates among Arabs in Israel, such as dissimilarities in diet and socioeconomic status. Yet, as emotional distress has been implicated in the etiology of T2DM, the current findings may suggest a possible avenue in which familial patterns that reduce the individual’s ability to attenuate his or her emotional distress by sharing difficulties with others may contribute to the higher tendency of Arabs in Israel to develop T2DM.
With regard to causes of the illness, most participants believed that, in addition to genetic predisposition, emotional distress contributed to the development and progression of T2DM, and most of them related the onset of their disease to traumatic events and stressful periods that were mostly related to family members. Thus, it is possible that the tendency to fuse with family members, taken together with stressful events related to family members, contributed to increasing the participants’ vulnerability to experience emotional distress, which in turn may be related to the development of T2DM. This inference, however, requires confirmation in future studies.
With regard to ways of coping with the illness, it seems that most participants, while reporting multiple difficulties, were actively managing their condition and addressing physical symptoms as well as trying to reduce their level of stress. Help of family members in treating the illness was mentioned by less than half the participants, which is surprising given the close and positive relationships described and the collectivist nature of the Arab society.
Limitations and Contributions
The findings of this study should be viewed in light of certain limitations. First, participants not having T2DM were not included. Thus, the extent to which the observed patterns are unique to individuals with T2DM is unclear. Second, the sample was small and included individuals from 1 region in Israel, and thus the generalizability of the findings is limited. Third, family relationships are naturally highly complex and multidimensional, and the current study likely did not capture all family patterns that may characterize patients with T2DM. Fourth, conclusions regarding relationships between familial patterns and the development of T2DM should be taken with considerable caution. It is conceivable, for example, that the tendency for fusion with others increased in some participants as a result of the diagnosis with T2DM and/or that the diagnosis and ensuing experiences influenced participants’ perceptions regarding relationships in their family of origin.
Nevertheless, the current study sheds light into how patients with T2DM experience their illness and their familial patterns and suggests directions for future studies on possible psychological and social factors that may contribute to the development of T2DM. Understanding the personal and family factors that increase the risk of the disease and affect how people cope with it may be a basis for developing more specific emotional therapy and treatment for individuals with diabetes or prediabetes. These treatments can focus, for example, on learning more effective stress management and coping skills, enhancing abilities to express one’s emotional needs, and communication with individuals who can provide support.