
Abstract
When do people experience versus regulate responses to compassion-evoking stimuli? We hypothesized that compassionate responding is composed of two factors—empathic concern and the desire to help—and that these would be differentially affected by perspective taking and self-affirmation. Exploratory (Study 1) and confirmatory (Study 2) factor analyses indicated that a compassion measure consisted of two factors corresponding to empathic concern and the desire to help. In Study 1 (N = 237), participants with high emotion regulation ability reported less empathic concern for multiple children than for one, but perspective taking prevented this effect. In Study 2 (N = 155), participants reported less desire to help multiple children, but only in the presence of self-affirmation. In both the studies, empathic concern predicted greater distress while the desire to help predicted greater chances of donating. Compassionate responding may consist of two separable facets that collapse under distinct conditions and that predict distinct outcomes.
Witnessing the suffering of others, particularly when those others are valued, frequently gives rise to compassion (Goetz, Keltner, & Simon-Thomas, 2010). Compassion may elicit helping behavior; however, compassion alone does not always lead to helping (Batson & Shaw, 1991; Goetz et al., 2010; Haidt, 2003). Part of the reason for compassion’s variable effects on helping behavior is that people are motivated to avoid feeling it when they can and even to stop feeling it once they have already begun to do so—a phenomenon referred to as the “collapse of compassion” (Cameron & Payne, 2011, 2012; Shaw, Batson, & Todd, 1994). This appears particularly to be the case when people anticipate that helping will be costly, such as when faced with multiple needy victims versus one needy victim, and when people have sufficient emotion regulation ability to manage their compassionate feelings.
Although prior research (Cameron & Payne, 2011, 2012) demonstrates when compassion will or will not collapse, what remains less clear is exactly what collapses. Compassion is defined as “the feeling that arises in witnessing another’s suffering and that motivates a subsequent desire to help” (Goetz et al., 2010). This conceptualization suggests that compassion, like many other emotions, consists of both a subjective feeling state and a related motivational state or desire to act (Lazarus, 1991; Nussbaum, 2001). It is possible that these conceptually distinct parts of compassionate responding are empirically distinct as well, and as such collapse or resist collapse under different conditions. That is, while a particular compassion-evoking situation may lead empathic concern to flourish, it may simultaneously lead one’s desire to help to collapse or vice versa. Considering these facets of compassionate responding individually may clarify how compassion functions, ultimately allowing for more accurate predictions about behavior.
It is important to note that, in distinguishing between two potentially distinct facets of compassion, we are further differentiating a construct that other researchers have worked to differentiate from empathy. For example, Singer and Klimecki (2014) distinguish between “feeling for” (compassion) versus “feeling with” (empathy) another. Similarly, Jordan and colleagues (Jordan, Amir, & Bloom, 2016) find that empathy, defined as feeling what others feel, is conceptually and empirically quite distinct from having an emotional reaction to others’ suffering. The latter is a phenomenon called concern (Jordan et al., 2016) or empathic concern (Batson, 2011; Davis, 1980) and is part of the broader construct of compassion (Goetz et al., 2010). Whether or not a person experiences empathy, defined either as mentalizing about another’s feeling states or as taking those states upon oneself, is subject to a variety of motivational and situational factors (Zaki, 2014) and is an important research topic in its own right.
Compassionate Responding as a Subjective Feeling State: Empathic Concern
A subjective feeling state that closely resembles compassion is empathic concern (Goetz et al., 2010), defined as “an other-oriented emotion elicited by and congruent with the perceived welfare of someone in need,” encompassing feelings of tenderness, warmth, and sympathy (Batson, Early, & Salvarani, 1997, p. 752). Empathic concern can spontaneously arise when perceiving another’s need, but is also commonly promoted by perspective taking, defined as thinking about how a suffering person feels in their situation (for a review, see Batson, 2011). Thus, while compassionate responding in the form of empathic concern may collapse in the face of multiple victims, perspective taking may inoculate against this collapse.
Although empathic concern can predict a variety of helping behaviors, such as donating one’s time or money (Coke, Batson, & McDavis, 1978) or volunteering to receive painful electric shocks in place of another “participant” (Cialdini, Brown, Lewis, Luce, & Neuberg, 1997), it does so only to the extent that it leads to a desire to help. What is empathic concern without a desire to help? Batson considered this point, warning that his hypothesis that perspective taking leads to altruism “makes no claim that empathic concern per se influences helping; it claims that empathy evokes altruistic motivation” (Batson, 1997, p. 520). That is, if empathic concern and the desire to help frequently co-occur, this may be because empathic concern can evoke this subsequent desire, which ultimately predicts helping. Similarly, others have found that the relationship between empathy and helping is completely mediated by a felt moral imperative to care about others’ well-being (Wilhelm & Bekkers, 2010). However, factors that evoke empathic concern, including perspective taking, can also induce feelings of distress and anxiety, which have been found to hinder the provision of help (Batson, Duncan, Ackerman, Buckley, & Birch, 1981; Cialdini et al., 1997). Together, this evidence suggests that the relationship between empathic concern and helping is neither certain nor direct and linear since empathic concern impacts helping by eliciting a desire to help alongside emotions that can inhibit acting on this desire. Thus, a collapse of empathic concern on its own could have relatively little impact on helping but have more of a role in predicting feelings of distress.
Compassionate Responding as a Motivational State: The Desire to Help
Witnessing the suffering of others may lead to the desire to help them, but it also leads to conflicting desires, such as the desire to protect oneself and one’s resources and to avoid distress (Batson et al., 1981). Therefore, it is important to consider which factors lead people to prioritize helping others over pursuing other salient goals. The desire to help specific others might emerge from the higher order goal of maintaining the belief that one is a good, moral person—that is, one’s moral identity (Aquino & Reed, 2002; Reed, Kay, Finnel, Aquino, & Levy, 2016). Specifically, such a desire may stem from general moral principles. For example, it has been theorized that people have an internalized value that helping others in need is important and necessary and that the strength of this value varies from person to person. Wilhelm and Bekkers (2010) refer to this as “the principle of care.”
As important as people may perceive the principle of care to be, there may be circumstances under which people disengage from it in favor of other concerns, especially if the costs of helping are perceived to be high. This would constitute a collapse of the desire to help. One factor that might promote this type of a collapse via goal disengagement is self-affirmation. Self-affirmation allows people to acknowledge and accept their own weaknesses. Although some research indicates that doing so can lead people to strive to become more morally virtuous (Sherman & Cohen, 2006), other research points out that self-affirmation promotes disengagement from goals in the face of failure or difficulty (Vohs, Park, & Schmeichel, 2013). Specifically, self-affirmation can lead people to internalize, rather than downplay, the likelihood of failure when goal pursuit is difficult, thus leading to goal disengagement. In the context of helping goals, several factors could increase difficulty and decrease the chances of complete success. One such factor is victim number: As the number of victims increase, so do the resources necessary to alleviate their suffering. Accordingly, in the face of larger numbers of victims, self-affirmation could lead individuals to acknowledge the possibility that helping is futile and to disengage from helping goals.
The Present Work
Although other researchers similarly suggest that compassionate responding is multidimensional, they do not describe the same components of compassionate responding that we describe in the present work. Our investigation of empathic concern, as well as motivation and intentionality, above and beyond emotion, makes this work a unique contribution. The overarching goal of the present research was to test the possibility that compassionate responding comprised two components, empathic concern and a desire to help, that can be measured separately and that may function independently in situations in which helping is possible. In particular, we wanted to follow up on research on the collapse of compassion (Cameron & Payne, 2011, 2012) and test whether these two components of compassionate responding might collapse under different conditions, with differing respective implications for distress and for helping behavior.
To examine the distinctiveness of the two proposed facets of compassionate responding, we decided to use the measure of compassion developed and used by Cameron and Payne (2011). This scale includes items that on their face tap both empathic concern and a desire to help, but these have previously been combined into a single index of compassion. In fact, the first four items of the compassion scale contain words that Batson and colleagues have long used to measure empathic concern (Batson, 1997, 2011), asking, “How sympathetic do you feel” toward the targets of compassion, “How warm . . .,” “How compassionate . . .,” and “How touched . . .” We hypothesized that these items would load on to one empathic concern factor because they map directly on to the emotion words described by Batson. Other items (five through nine) broadly map onto the desire to help, that is, desiring that the targets of compassion experience general well-being and decreased suffering, and perceiving the targets as worthy of help.
In addition, we wanted to examine different predictors for the two proposed facets of compassionate responding. We expected that perspective taking would protect empathic concern against collapse among people with sufficient emotion regulation ability for collapse to occur. We also expected that promoting a sense of moral identity or self-integrity more broadly would promote collapse of the desire to help. In particular, we expected that asking people to affirm an important value, or engaging in self-affirmation, should function in this manner.
For the sake of clarity in our predictions, it is important to note why we made asymmetrical predictions across dependent variables such that we expected emotion regulation ability to influence whether or not empathic concern collapsed, but we did not necessarily expect it to influence whether or not desire to help collapsed. First, we were trying to replicate a specific effect (the collapse of compassion) that is known to be dependent on emotion regulation ability, as measured by the Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004). We suspected that the component of compassionate responding that can be downregulated as a function of emotion regulation ability is likely empathic concern because, as we have pointed out, empathic concern is a suite of per se emotions associated with the experience of compassion. By contrast, we view the desire to help as a set of goals tied to more general moral principles such as one’s moral identity or the principle of care. Although goal disengagement certainly can be a form of emotion regulation—arguably, that is why self-affirmation might prompt helping goal disengagement—it is unclear whether emotion regulation ability, as operationalized by the DERS, would capture this capacity. Of the six dimensions of emotion regulation (in)ability captured by the DERS, two directly address the interplay of goals and emotions: difficulties engaging in goal-directed behavior and impulse control difficulties. The others are nonacceptance of emotions, lack of emotional awareness, lack of emotion regulation strategies, and lack of emotional clarity. Notably, the two dimensions that do address goals or goal-driven behavior focus on the impact of emotions on goals, rather than vice versa. For these reasons, we hypothesized that emotion regulation ability would be likely to impact emotional responses, but we were uncertain whether such ability would also impact compassionate desires. Nevertheless, we tested the effect of emotion regulation in models predicting both empathic concern and the desire to help.
Finally, this research examined the associations between the two proposed facets of compassionate responding and important outcomes for the self and for the targets of compassionate responding: distress for the self and helping behavior toward the targets. To examine this and all our research questions, we conducted two studies that tested the following hypotheses:
Study 1 uniquely tested Hypothesis 2a, while Study 2 uniquely tested Hypothesis 2b; both studies addressed Hypothesis 3.
Study 1
Method
Participants
To determine sample size for this study, an a priori power analysis was conducted using G*Power software for a six group (2 Target Number × 3 Perspective Taking) design with one continuous moderator (self-regulatory ability) and a small effect size (Cohen’s f = 0.25) for power of 0.80. This analysis indicated an ideal sample size of N = 237. We were successfully able to recruit 236 male and female participants from the Introductory Psychology participant pool at the University at Buffalo (61% European American, 17% African American, 14% Asian, 6% Latino/a, 1% other, 56% female). Students received partial course credit for their participation in the study.
Design
The independent variables that were manipulated in this study were perspective-taking instructions (imagine-self perspective taking [ISPT] vs. imagine-other perspective taking [IOPT] vs. none) and number of target persons (one vs. eight). We examined the effects of both ISPT and IOPT to explore any important differences between the two methods. For example, Batson (2011) has suggested that IOPT may be a more pure elicitation of empathic concern than ISPT, which also brings to mind self-relevant concerns. The measured participant variables in the study were how much participants reported explicit feelings of empathy and distress as well as trait-level difficulties in emotion regulation and how much participants were willing to donate to the person(s) whom they saw and read about.
Materials
Materials used in this study included PCs running MediaLab and DirectRT stimulus presentation software as well as several questionnaires presented via PC. These included a brief demographics questionnaire, Batson’s Empathy and Distress scale (Batson, 1997), a compassion scale developed by Cameron and Payne (2011), and the Difficulties in Emotion Regulation scale (DERS; Gratz & Roemer, 2004). The donation procedure also required the use of folders and paper donation forms created to resemble those that the American Red Cross might use.
Measures
Emotion regulation (in)ability
The DERS (α = .93; Gratz & Roemer, 2004) contains 36 items that measure how much people are unable to control their own feelings. Each item was scored on a 1 (almost never) to 5 (almost always) scale. Items include “I am confused about how I feel,” and “When I am upset, it takes me a long time to feel better,” among others.
Compassion
Cameron and Payne’s (2011) compassion scale (α = .95) includes nine items phrased as questions about compassionate feelings toward the child(ren). Responses were rated on a scale from 1 (not at all) to 7 (extremely). These items measured feelings of sympathy, warmth, and compassion but also included more specific questions regarding perceived appropriateness of donating money to help the child(ren), perceived urgency of helping, and how much one feels that it is important that the child(ren) be happy and not suffer.. All items are listed in Table 1. Empathic concern (α = .94, Items 1-4) and the desire to help (α = .93, Items 6-9) were measured as subsets of the compassion items described above.
Factor Structure, Two-Factor Exploratory Factor Analysis (N = 236).
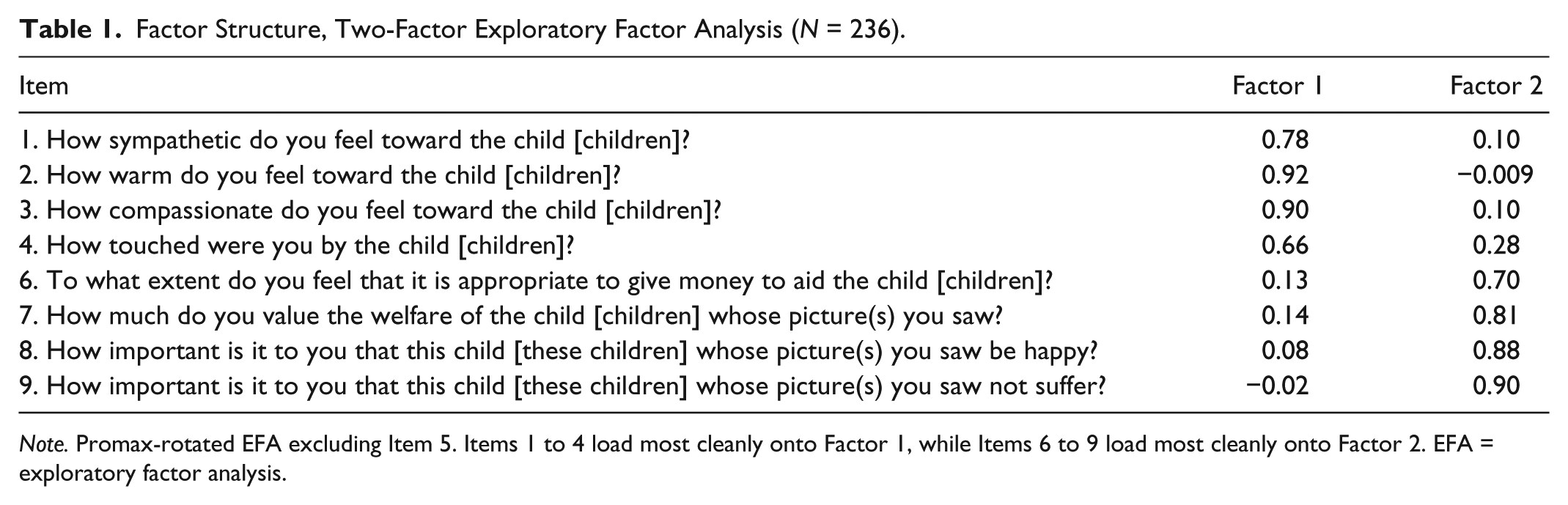
Note. Promax-rotated EFA excluding Item 5. Items 1 to 4 load most cleanly onto Factor 1, while Items 6 to 9 load most cleanly onto Factor 2. EFA = exploratory factor analysis.
Distress
Distress was measured by averaging self-reported scores indicating personal relevance of the words previously used by Batson and colleagues (Batson, Fultz, & Schoenrade, 1987) to measure personal distress. Participants reported how much a series of words reflected their current experience on a scale of 1 (not at all) to 7 (extremely). These include alarmed, grieved, troubled, distressed, upset, disturbed, worried, and perturbed (α = .93).
Donations
Paper donation forms created to resemble those used by the Red Cross asked participants to indicate the amount that they wished to pledge and to provide their contact information (name, street address, phone number, and e-mail address) so that the Project Darfur Donation Coordinator could reach them to collect their pledges. The forms also indicated that any money pledged would go directly to the specific person(s) whom they learned about during the session.
Procedure
Participants were told that they were participating in a study of “Individual Differences in Emotional Responses” and that we were interested in emotional responses to stimuli. After consenting to the study’s procedures, participants began by completing some measures on the computer including the DERS (Gratz & Roemer, 2004). Next, participants continued on to a task in which they were told that they would be viewing and responding to some visual and written stimuli. Participants read one of two versions of perspective-taking instructions, or they received no-perspective-taking instructions, serving as a replication of Cameron and Payne’s (2011) findings. They were randomly assigned to such conditions prior to their arrival to the lab. Those in the perspective-taking conditions were told via on-screen instructions that these instructions are necessary, as we were specifically interested in the effects of people’s mind-sets on their emotional responses. The perspective-taking instructions used were adapted from prior work by Batson and colleagues (Batson et al., 1988).
Those in the IOPT condition received the following instructions: While you are reading the information that follows, and viewing the image(s), try to think about how the person [people] whom you are presented with feels. Try to imagine how he or she [they] feels about the situation described and how it has affected his or her life [their lives]. Try not to concern yourself with attending to all of the information presented. Just concentrate on trying to imagine how the person feels.
Those in the ISPT condition received the following instructions: While you are reading about the information that will follow, and viewing the image[s], try to think about how you feel. Try not to concern yourself with attending to all of the information presented. Just concentrate on trying to think about your own feelings.
Following this, participants either viewed an image of one or eight children from the Darfur region of Sudan (conditions were determined by random assignment prior to participants’ arrival in the lab). The image(s) were accompanied by a description of the conditions in the area, mentioning violence, poverty, and the spread of deadly diseases. The images as well as the descriptive text were taken from Cameron and Payne’s (2011) earlier work. The exact description was presented as follows: In the West Darfur region of Sudan, there has been a civil war raging for the past four years. The Sudanese government and allied militias have been in intense conflict with various rebel groups. This conflict has resulted in unchecked violence against civilians, who have been killed, abducted, or driven from their homes. These civilians suffer from malnutrition, unsanitary living conditions, and are at risk for a variety of deadly diseases such as malaria, dysentery, and cholera.
After viewing the stimuli, participants responded to a compassion scale developed by Cameron and Payne (2011) as well as Batson’s (1997) Empathy and Distress Scale. For the last part of the study, instructions on the computer informed people that they would have the opportunity to help the person or people whom they read about. Once the participant read these instructions, they were asked to ring a bell to alert the experimenter, who brought them an envelope and a form that was ostensibly from the Red Cross as part of their Project Darfur Relief Fund. Participants were given the opportunity to pledge however much they wished to the Red Cross to help those in the images that they viewed. They were also asked to provide their contact information as they were led to believe that the Project Darfur Coordinator would receive the form and would be contacting them soon to collect their pledge. Written instructions directed them to write the amount that they wish to pledge on the form, and they were instructed to place the form back into the folder and ring the bell on their desktop so that the experimenter could collect it from them.
Finally, people completed a short demographics questionnaire so that we could gather some basic information about their backgrounds for statistical purposes. After this, the research assistant asked them a few probing questions to ensure that they had not guessed our hypotheses. They were then told the specific hypotheses of the study and that the donation procedure was not real. They were thoroughly debriefed and allowed to ask questions. Participants were also asked whether or not they wished to have their data discarded. If they wished for their data to be discarded, we did so immediately. At this time, we also asked participants about their emotional state after the experimental procedures. Before any participant was dismissed, we made sure that participants were not distressed as a result of having read about and seen images of people in need or as a result of their decision to donate or not.
Results
All analyses were conducted using Mplus 7 and Stata 14 software. No participants were excluded from data analysis, and there was no missing data within the variables of interest that were used for analysis.
Exploratory factor analysis (EFA): Compassion
The factor structure of the compassion scale was first examined by conducting an EFA. Maximum likelihood (ML) estimation was the preferred method of factor analysis as it allows for the computation of fit indices and significance tests for model comparison. As skewness and kurtosis were slight, 1 the assumption of multivariate normality was not violated, and ML estimation was appropriate for this dataset. (Curran, West, & Finch, 1996). For all models, factors were scaled using the first marker indicator as is the default in Mplus. Analyses were conducted using the full information as all original data were available for use.
Although the items that make up the compassion scale (Cameron & Payne, 2011) were internally consistent in the Study 1 data (α = .95), a high value of Cronbach’s alpha does not imply anything about scale dimensionality. To examine the underlying factor structure, and begin exploring competing hypotheses that compassion is either unitary or multidimensional, we conducted an EFA. In doing so, we allowed for a range of anywhere between one and three factors to arise. This allowed us to compare Cameron and Payne’s (2011) original usage of a one-factor structure with the current hypothesis regarding a two-factor structure while still allowing an additional factor to emerge if present in the data. Furthermore, as this scale was recently developed and is not yet well-validated, it was appropriate to conduct an EFA that allows for the suggestion of multiple solutions before conducting a confirmatory factor analysis (CFA). The data were rotated using a promax oblique rotation, as the items in the scale are highly intercorrelated (α = .95). A scree plot showed a clear bend at the second eigenvalue, 2 indicating that it was appropriate to extract two factors (see Figure 1).
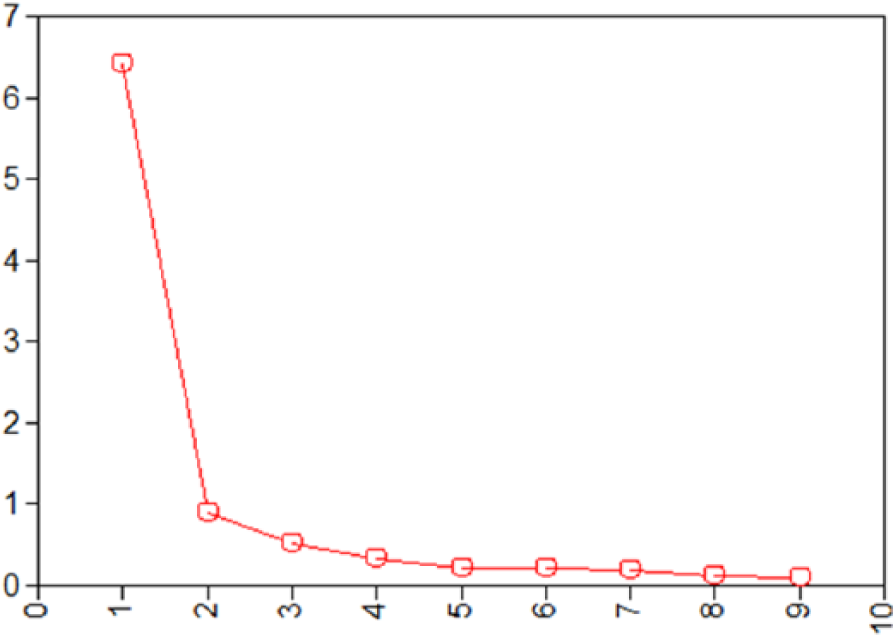
Scree plot for EFA.
The one-factor solution provided a poor fit to the data, with a high, statistically significant chi-square value and an RMSEA (root mean square error of approximation) value that indicated poor fit based on Hu and Bentler’s (1999) rules of thumb—χ2(27) = 401.28, p = .00; RMSEA = 0.24. The two-factor solution (see Table 1) indicated better fit—χ2(19) = 65.70, p = .00; RMSEA = 0.10—as demonstrated by a decrease in the chi-square value as well as the estimate for the RMSEA. In addition, a chi-square difference test indicated significantly better fit when moving from a one to a two-factor model—
Factor Structure, Three-Factor Exploratory Factor Analysis (N = 236).
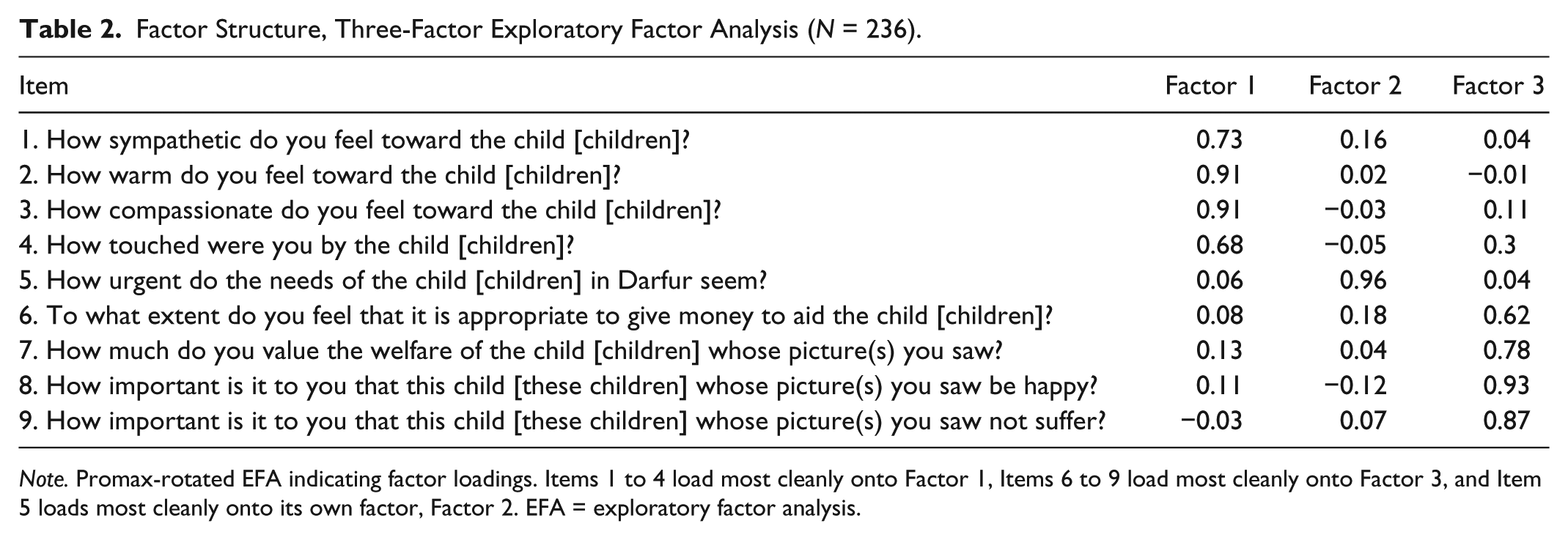
Note. Promax-rotated EFA indicating factor loadings. Items 1 to 4 load most cleanly onto Factor 1, Items 6 to 9 load most cleanly onto Factor 3, and Item 5 loads most cleanly onto its own factor, Factor 2. EFA = exploratory factor analysis.
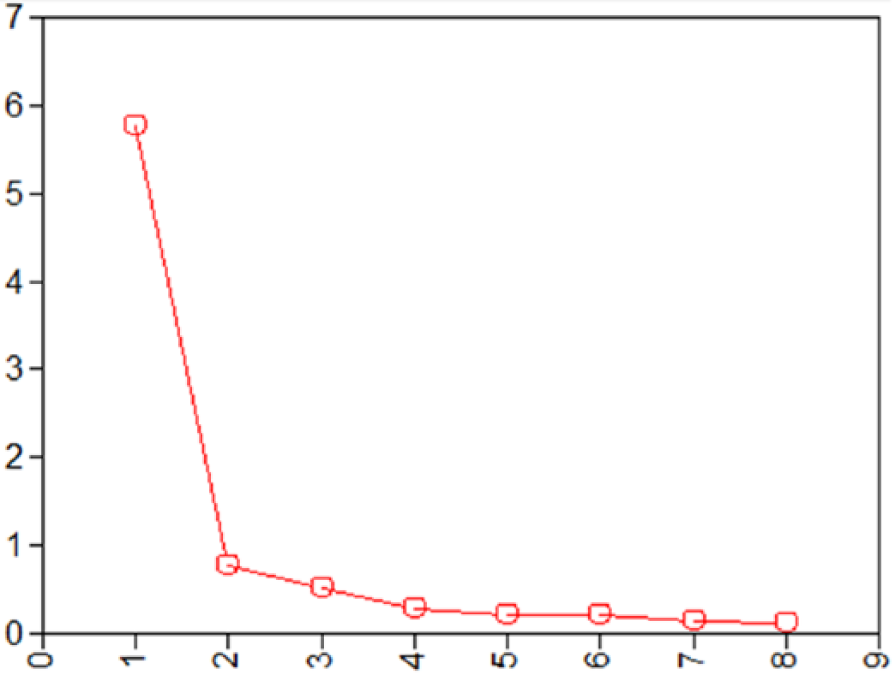
Scree plot for EFA, excluding Item 5.
Perspective taking, empathic concern, and the desire to help
To test the hypothesis that empathic concern would be affected by perspective taking, we examined whether perspective taking would moderate the effects of victim number (dichotomously coded as single victim = 0, multiple victims = 1) on empathic concern—an effect itself moderated by emotion regulation. That is, we examined whether the three-way interaction of perspective taking, emotion regulation, and number of victims would predict each dimension of compassion: empathic concern and the desire to help. We predicted that this three-way interaction would be significant for empathic concern. That is, we expected that empathic concern would decrease with increasing victim number among those high in emotion regulation. However, we specifically expected to find this effect among participants who did not engage in perspective taking, and we expected to find that this effect would not occur among participants who did engage in perspective taking.
We included both IOPT and ISPT to explore whether there were any meaningful differences between these two methods of perspective taking; however, their separate effects were not significant, consistent with the diminished power of these analyses, so they were combined for analysis. 3 To test our hypotheses, two multiple regression models—one with empathic concern as the dependent variable and one with the desire to help as the dependent variable—examined perspective taking (coded as perspective taking = 1, no-perspective taking = 0), emotion regulation, number of victims, all two-way interactions among those variables, and the three-way interaction as predictors.
Empathic concern
Examining the model for empathic concern revealed that the three-way interaction was significant (B = −1.14, 95% confidence interval [CI] = [–1.94, –0.34],p = .006, f2 = .04). To evaluate the simple two-way interaction between emotion regulation and number of victims in the presence or absence of perspective taking, we reexamined the model predicting empathic concern separately with either perspective taking or no-perspective taking set as equal to 0.
Empathic concern with perspective-taking
In the presence of perspective taking (B = −0.17, 95% CI = [–0.63, 0.30], p = .48, f2 < .01), there was no two-way interaction between emotion regulation and number of victims. Therefore, we examined the simple effect of number of victims on empathic concern for those in the perspective-taking condition. In this group, empathic concern increased with number of victims (B = 0.88, 95% CI = [0.42, 1.33],p < .001, f2 = .06).
Empathic concern without perspective taking
In the absence of perspective taking, there was a significant emotion regulation by number of victims interaction (B = 0.97, 95% CI = [0.32, 1.62], p = .004, f2 = .04). To understand this interaction, we examined this model with emotion regulation recentered at a low (M – 1 SD) or high (M + 1 SD) value to evaluate the simple slope for number of victims for those high or low in emotion regulation. These analyses revealed that for those high in emotion regulation (those low in difficulties with emotion regulation), a greater number of victims decreased empathic concern (B = −1.06, 95% CI = [–2.01, –0.11], p = .03, f2 = .02), while for those low in emotion regulation (those high in difficulties with emotion regulation), a greater number of victims marginally increased empathic concern (B = 0.88, 95% CI = [–0.03, 1.79], p = .06, f2 = .02). This pattern suggests that, in the absence of perspective taking, those high in emotion regulation showed especially high levels of empathic concern in response to single versus multiple victims (a pattern consistent with Cameron & Payne, 2011, Experiment 2) but that perspective taking reverses this. This pattern is displayed in Figure 3.
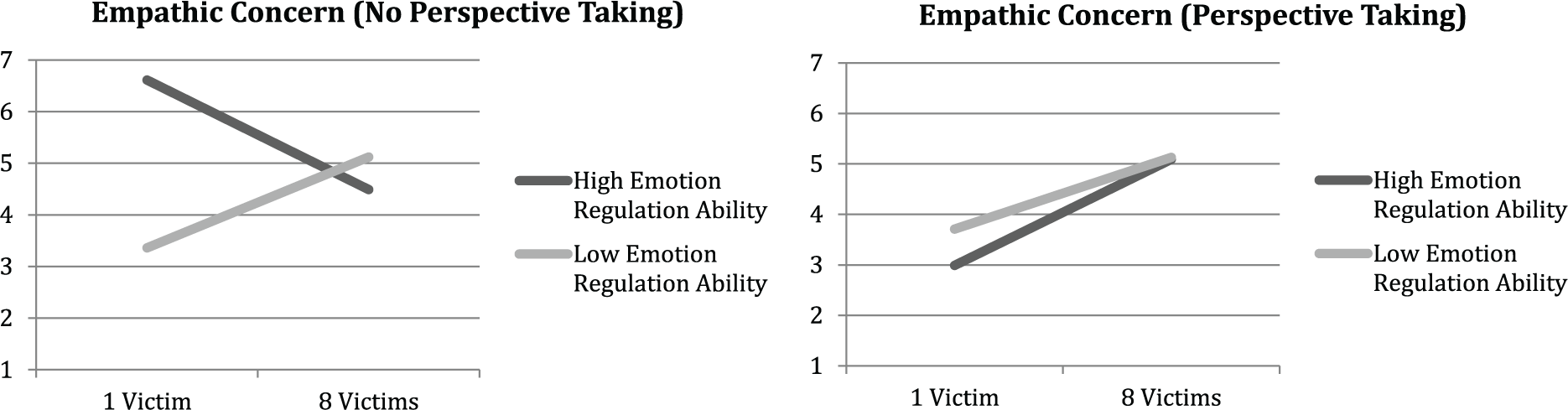
Study 1: Associations between number of victims and empathic concern, by emotion regulation ability and perspective-taking condition.
The desire to help
There was no three- way interaction among perspective-taking, emotion regulation, and victim number for the desire to help (B = −0.85, 95% CI = [–2.51, 0.80], p = .31, f2 < .01). Given that, a follow-up analysis examined whether the two-way interaction of just emotion regulation and number of victims would predict this DV. Results indicated that there was also no such two-way interaction (B = 0.02, 95% CI = [–0.75, 0.80], p = .95, f2 < .01). However, there was a main effect of victim number on the desire to help, such that greater numbers of victims led to a stronger desire to help (B = 0.84, 95% CI = [0.06, 1.62],p = .03, f2 = .02).
In sum, empathic concern collapsed in the presence of multiple victims (people felt less empathic concern for eight victims than for one) when participants had high emotion regulation ability, but only in the absence of perspective taking. By contrast, the desire to help did not collapse in the presence of multiple victims, and perspective taking did not affect the collapse of the desire to help, which increased with the number of victims, irrespective of emotion regulation.
Distress and helping
We examined the possibility that empathic concern and desire to help would differentially predict distress and helping behavior, respectively. To do so, both predictor variables were entered simultaneously in a multiple regression for each outcome. Examining descriptive statistics revealed that helping behavior in the form of donations was highly skewed, with 46% of participants donating nothing. To manage this, we used zero-inflated Poisson regression, which allows for simultaneous prediction of the amount of a variable and the likelihood of a zero value, somewhat akin to simultaneous logistic and Poisson regression (Cameron & Trivedi, 2009). For this analysis, both empathic concern and desire to help were used as predictors of amount of donation and zero values. These predictor variables were standardized to facilitate interpretation of all our analyses. Results indicated that empathic concern marginally predicted higher levels of distress (B = 0.24, 95% CI = [–0.02, 0.51], p = .07, f2 = .01), while the desire to help did not (B = 0.17, 95% CI = [–0.10, 0.43], p = .22, f2 < .01); see the first panel of Figure 4. By contrast, the desire to help predicted higher levels of donations (B = 0.74, 95% CI = [0.68, 0.80], p < .001, φ = 1.68), while empathic concern actually did the opposite (B = −0.38, 95% CI = [–0.42, –0.33], p < .001, φ < 1.05). The desire to help also predicted greater likelihood of donating (i.e., lower likelihood of a zero value; B = −0.60, 95% CI = [–0.99, –0.20], p < .001), while empathic concern did not (B = −0.13, 95% CI = [–0.51, 0.25], p = .50); see the first panel of Figure 5.
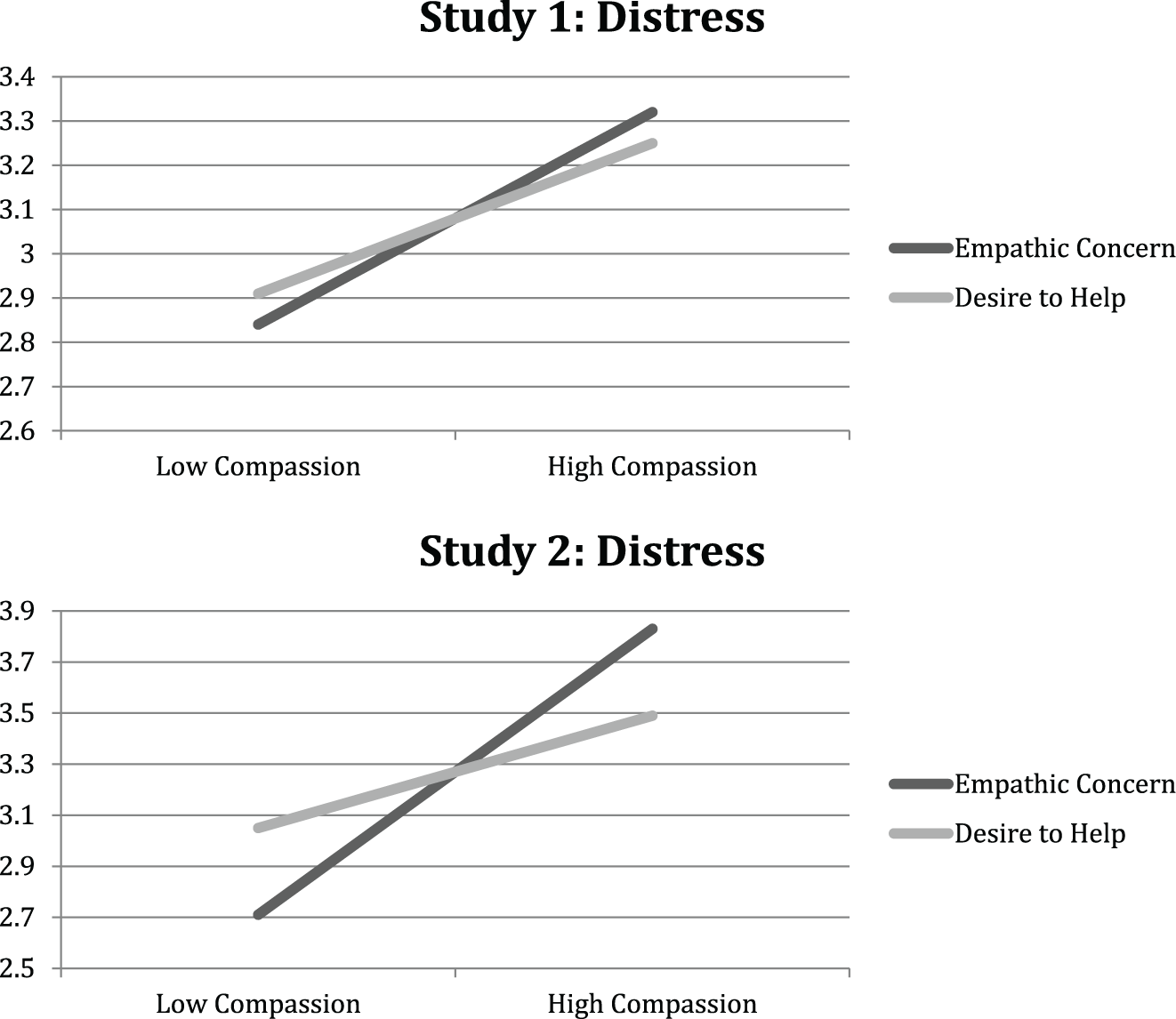
Associations between both elements of compassion and distress in Studies 1 and 2.
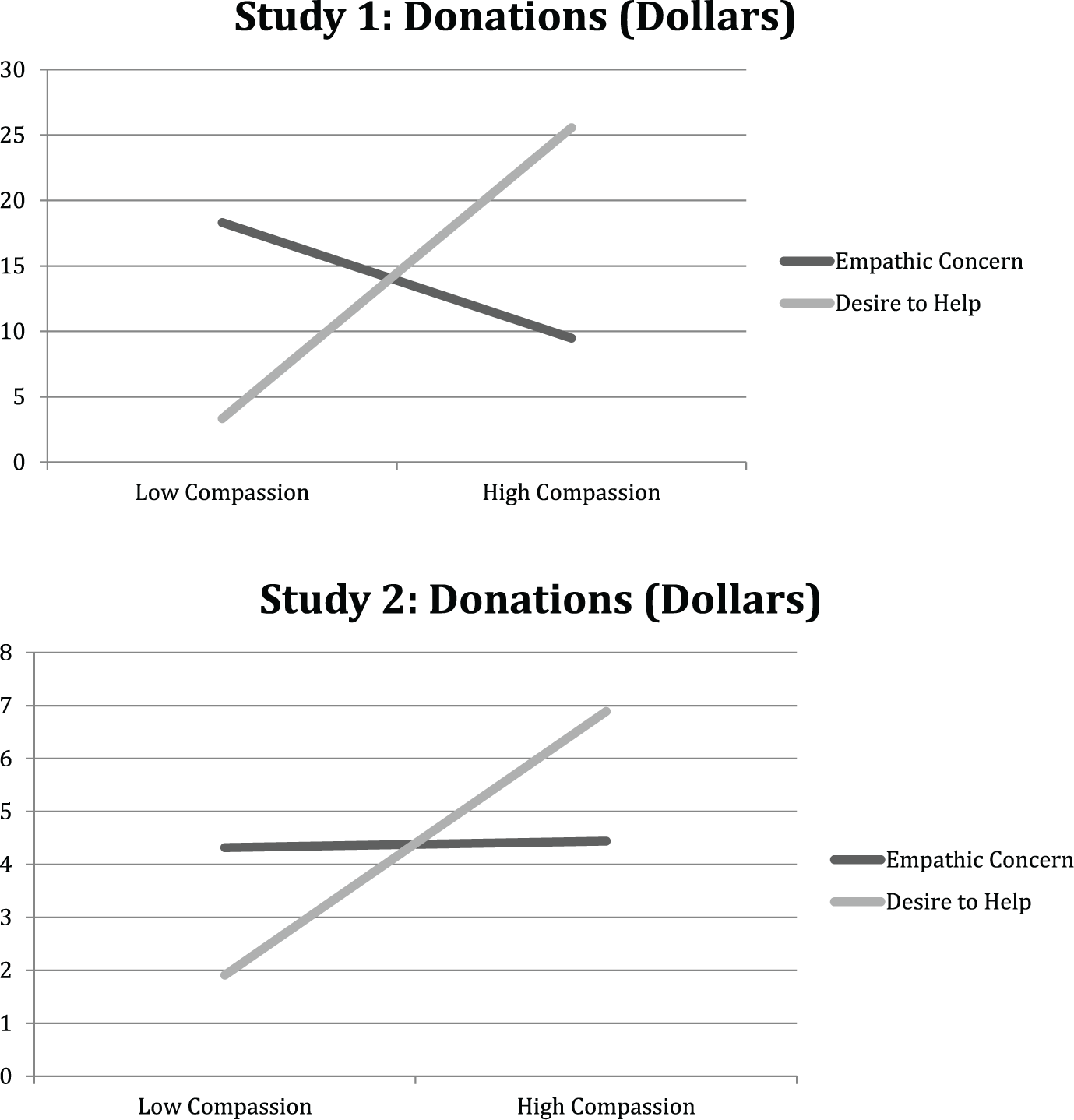
Associations between both elements of compassion and donations in Studies 1 and 2.
Discussion
The results of Study 1 supported our hypothesis that compassion is made up of two facets: empathic concern and the desire to help. As predicted, we found that empathic concern collapsed in the presence of multiple victims among those who had high emotion regulation ability, and our findings supported our hypothesis that perspective taking would eliminate this effect. This pattern of results was not found for the desire to help, which did not collapse but increased with the number of victims. In addition, we found that only empathic concern was marginally associated with distress.
Although our hypotheses that the desire to help would predict higher levels and likelihood of donations were confirmed, we were surprised to find that empathic concern actually had the opposite effect—that is, empathic concern predicted lower levels of donations. Study 2 provided an opportunity to potentially replicate this unpredicted finding. Study 2 also provided an additional test of the factor structure that emerged in Study 1 with an independent sample, as well as replications of analyses predicting distress and helping from each facet of compassion. Furthermore, Study 2 enabled us to test whether self-affirmation interacts with number of victims predicting compassion.
Study 2
Method
Participants
Again, an a priori power analysis was conducted using G*Power software for a six group (2 target number × 2 perspective taking × 2 self affirmation) design with one continuous moderator (self-regulatory ability) and a small effect size (Cohen’s f = 0.25) for power of 0.80. This analysis indicated an ideal sample size of N = 236 for Study 2 as well; however, due to semester deadlines, we were only able to recruit 155 participants. In addition, due to a programming error, the design of this study was not fully crossed (the perspective-taking manipulation was not present in all conditions). For this reason, the perspective-taking findings from Study 1 could not be replicated in this dataset, and we limited our analyses of self-affirmation effects to only those in the no-perspective-taking condition (n = 101). 4 However, the full sample was used to test the factor structure of the compassion scale and its correlations with distress and helping. Participants were again ethnically diverse male and female participants from the Introductory Psychology participant pool at the University at Buffalo (63% European American, 16% African American, 10% Asian, 8% Latino/a, 3% other, 65% female). Students received partial course credit for their participation in the study.
Design
The independent variables that were manipulated in this study were perspective-taking instructions (IOPT vs. none), number of target persons (one vs. eight), and self affirmation (affirmation vs. control). The measured participant variables in the study were how much participants reported explicit feelings of empathy and distress, as well as trait-level difficulties in emotion regulation, and how much participants were willing to donate to the person(s) whom they saw and read about.
Materials
Materials used in Study 2 were identical to those used in Study 1 aside from the inclusion of a self-affirmation manipulation (Steele, 1988). All measures were internally consistent (DERS: α = .94; compassion: α = .92; empathic concern: α = .90; the desire to help: α = .87 distress: α = .94).
Procedure
The procedure was the same as Study 1 with the addition of random assignment to a self-affirmation or control task prior to the perspective-taking (vs. no-perspective-taking) manipulation and the use of only one perspective-taking manipulation (IOPT). To administer the self affirmation manipulation, all participants were asked to rank a list of given values from most to least personally important. Values included theoretical, economic, aesthetic, social, political, and religious. Following this, those in the self-affirmation condition were asked to write a short essay about why their highest ranked value was important to them. Those in the control condition were asked to write a short essay about why their lowest ranked value might be important to the average student, as is typical in self-affirmation manipulations (Steele, 1988). Content of essays indicated that all participants followed directions.
Results
All analyses were conducted using Mplus 7 and Stata 14 software. No participants were excluded from data analysis, and there was no missing data within the variables of interest that were used for analysis.
CFA: Empathic concern and desire to help
We used data from the compassion scale presented in an independent sample (Study 2, N = 155) to determine whether the fit of a two-factor solution was adequate. ML estimation was appropriate as skewness of the measured variables did not exceed 0.10 and kurtosis did not exceed 0.96 (Curran et al., 1996; Finney & DiStefano, 2006; Muthen & Kaplan, 1985). As in Study 1, factors in all models were scaled using the first marker indicator, and analyses were conducted using the full information, as all original data were available for use.
As in Study 1, the compassion scale had high internal consistency (α = .92). Here, we conducted a CFA, excluding Item 5 (as described above) and specifying that any error associated with the two factors should be correlated with one another, as the factors themselves were correlated (α = .68). The chi-square test of model fit was significant, indicating poor fit—χ2(19) = 43.50, p = .001—however, the alternate fit indices looked promising (RMSEA = 0.09, comparative fit index [CFI] = 0.97, Tucker–Lewis index [TLI] = 0.96, standardized root mean square residual [SRMR] = 0.06; Hu & Bentler, 1999). There were several suggested modification indices related to covarying items with similar wording. For example, the beginning of both Items 8 and 9 is “How important is it to you that this child [these children] whose picture(s) you saw . . .” A modified model was generated to determine whether or not this change significantly improved model fit. Examining the two-factor CFA model, still without Item 5, allowing Items 8 and 9 to covary, the fit improved significantly—
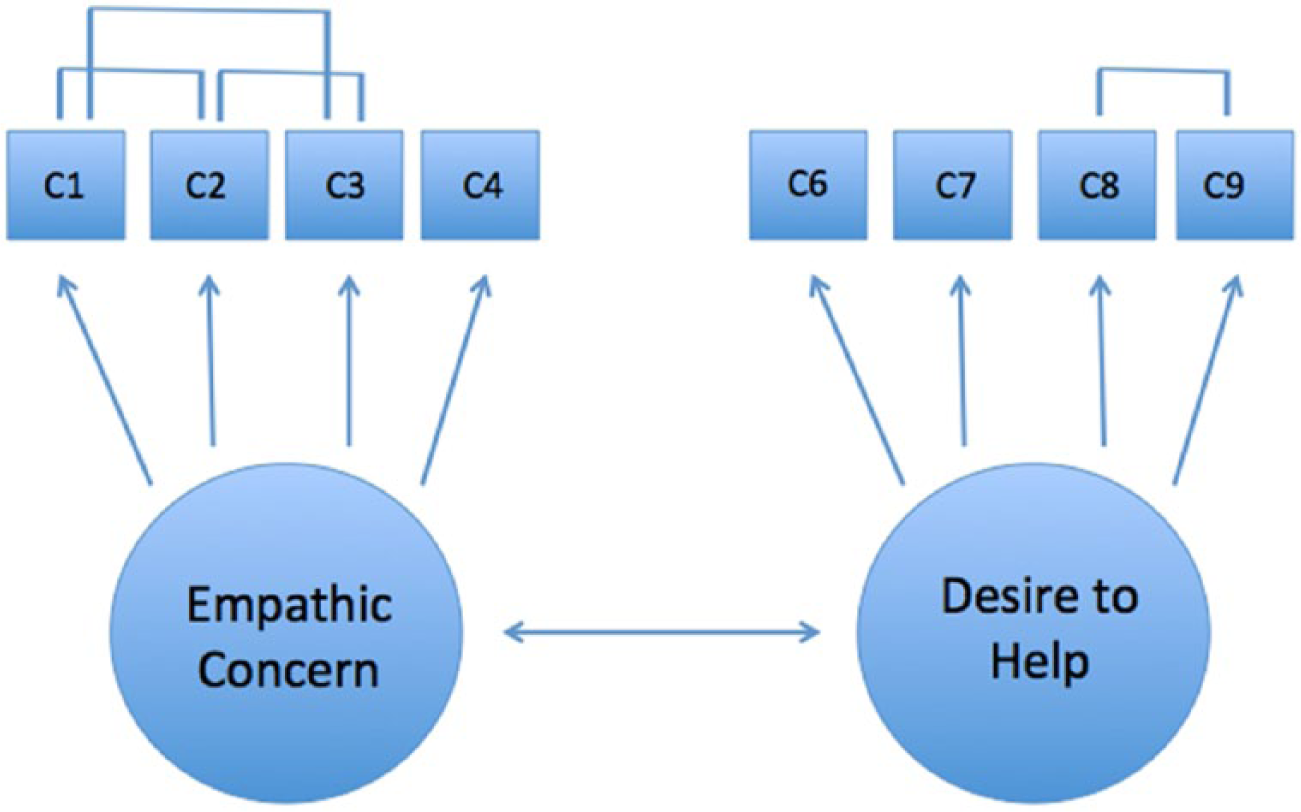
Best-fitting measurement model, changes made according to modification indices and theoretical rationale.
Correlation Matrix, Final CFA Model (N = 155).
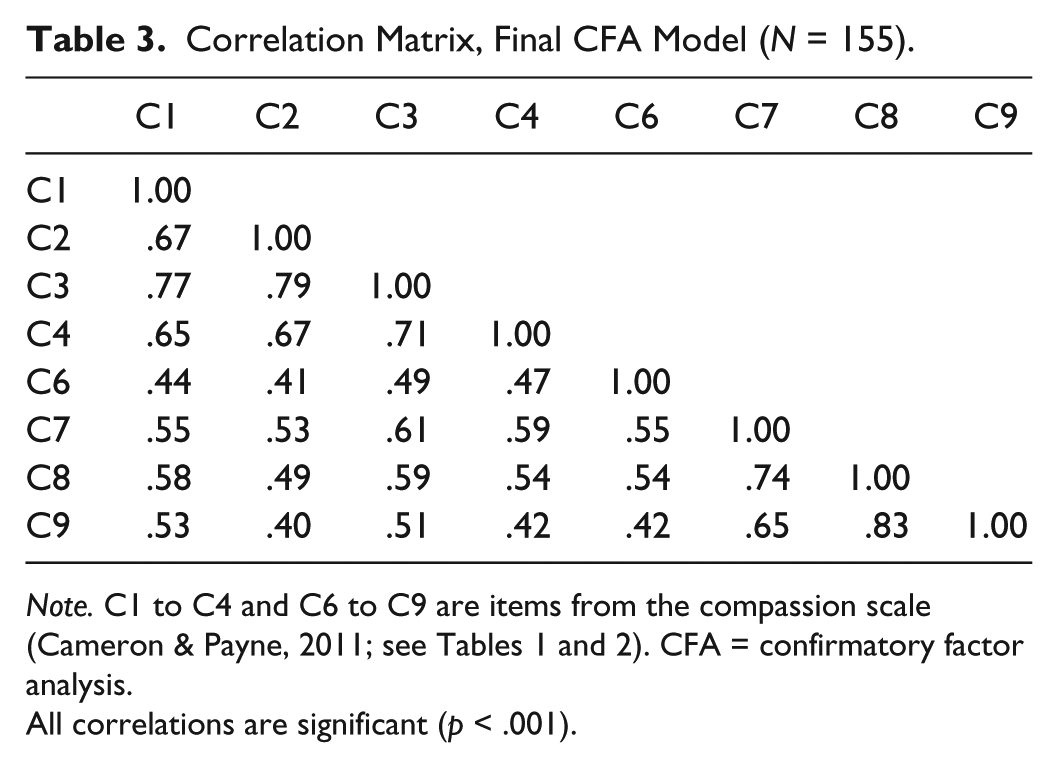
Note. C1 to C4 and C6 to C9 are items from the compassion scale (Cameron & Payne, 2011; see Tables 1 and 2). CFA = confirmatory factor analysis.
All correlations are significant (p < .001).
R2, Final CFA Model.
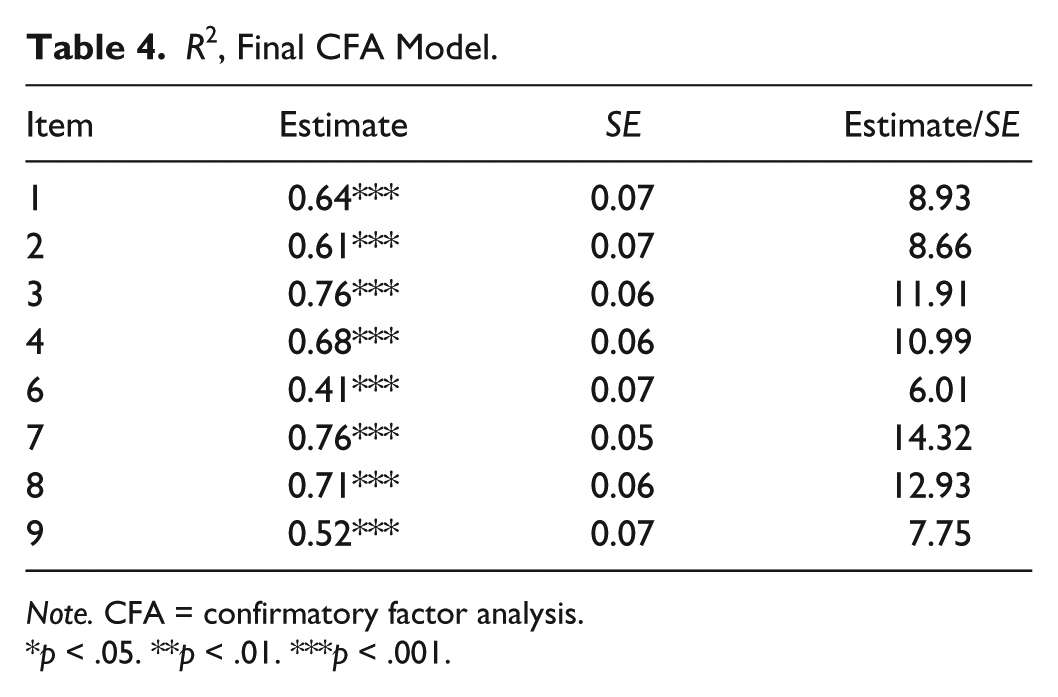
Note. CFA = confirmatory factor analysis.
p < .05. **p < .01. ***p < .001.
Study 1 had an N of 236, while study 2 had an N of 155. To meaningfully derive information about a scale’s factor structure, it is advisable to examine a sample of no less than 200 independent observations (Boomsma, 1982; Kline, 2011). However, we present a model based on a short (nine items) measure, in which the parameter to participant ratio is reasonable. As such, we chose to feature the replicability of our findings over parameter estimate precision but also recognize the importance of such precision. We do not have reason to believe that the data from Studies 1 and 2 differ in any systematic way as all data were collected from the same population using parallel experimental designs. Therefore, we also tested our model using a combined N of 392, combining the data from Studies 1 and 2. Whether examined individually or combined, both samples reflected the same pattern of results. 5
Self-affirmation and desire to help
To test the hypothesis that the desire to help would be affected by self-affirmation, we examined whether self-affirmation would moderate the effects of victim number (as in Study 1, dichotomously coded as single victim = 0, multiple victims = 1) predicting compassion. That is, we examined whether the two-way interaction of self-affirmation and number of victims would predict each dimension of compassion: empathic concern and the desire to help. We predicted that this two-way interaction would be significant for desire to help and that desire to help would decrease with increasing victim number when self-affirmation was present but not in the absence of self-affirmation. 6
To test our hypotheses, two multiple regression models—one with empathic concern as the DV and one with the desire to help as the DV—examined self-affirmation (coded as self-affirmation = 1, no self-affirmation = 0), number of victims, and their two-way interaction as predictors. Examining these models revealed that the two-way interaction was significant for the desire to help (B = −0.77, 95% CI = [–1.31, –0.24],p = .005, f2 = .08) but much less or not at all for empathic concern (B = −0.55, 95% CI = [–1.12, 0.01], p = .054, f2 = .03).
Next, to evaluate the simple effect of victim number in the presence or absence of self-affirmation, we reexamined the model predicting desire to help separately with either self-affirmation or no self-affirmation set as equal to 0. These models showed that in the presence of self-affirmation, a greater number of victims decreased the desire to help (B = −0.40, 95% CI = [–0.78, –0.03], p = .04, f2 = .05), but this was not the case in the absence of self-affirmation (B = 0.37, 95% CI = [–0.01, 0.76], p = .06, f2 = .04). This pattern is illustrated in Figure 7.
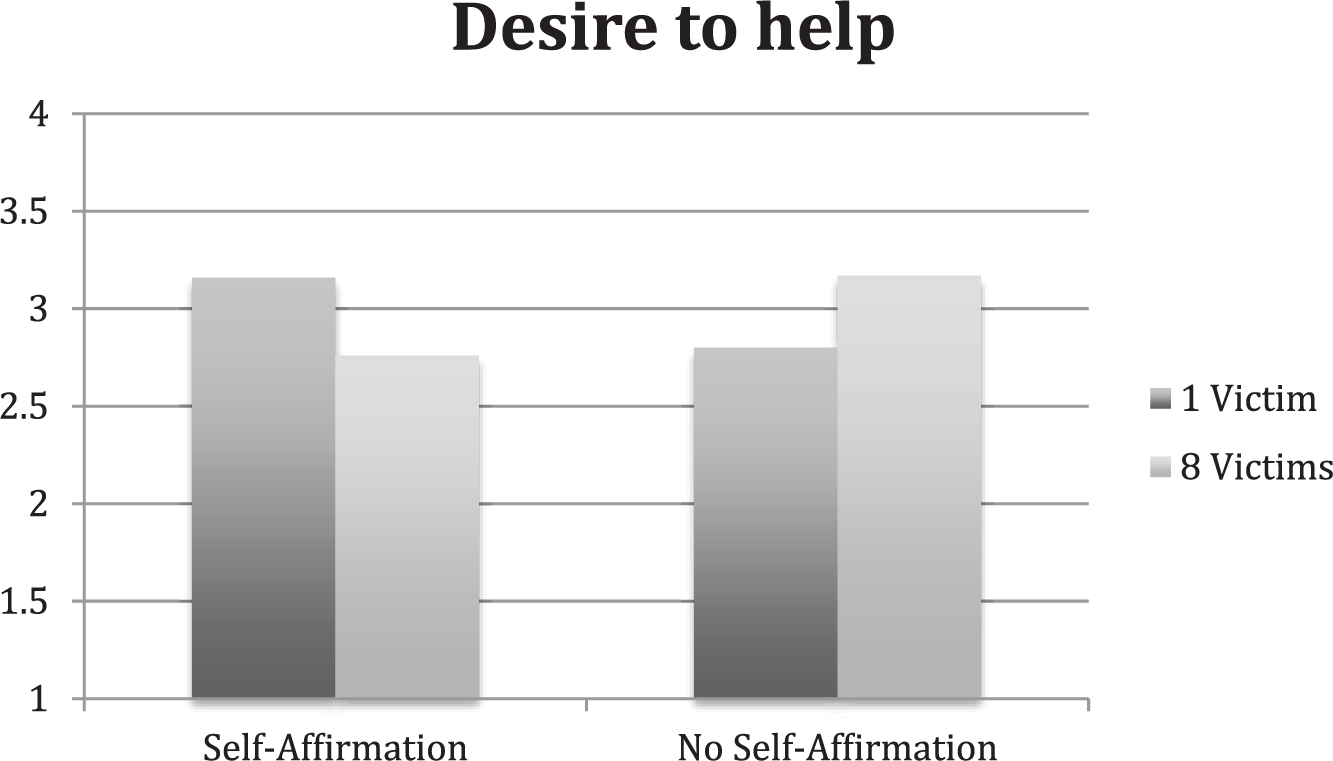
Study 2: Associations between number of victims and the desire to help, by self-affirmation condition.
In sum, the desire to help collapsed in the presence of multiple victims, but only in the presence of self-affirmation. By contrast, self-affirmation did not affect the collapse of empathic concern.
Distress and helping
The Study 2 analyses of distress and helping were conducted exactly the same as the Study 1 analyses of the same variables. Results indicated that empathic concern predicted higher levels of distress (B = 0.56, 95% CI = [0.27, 0.86], p < .001, f2 = .08), while the desire to help did not (B = 0.22, 95% CI = [–0.06, 0.51], p = .13, f2 = .01); see the second panel of Figure 4. By contrast, the desire to help predicted higher levels of donations (B = 0.36, 95% CI = [0.22, 0.49], p < .001, φ = .42), while empathic concern did not (B = 0.04, 95% CI = [–0.10, 0.17], p = .60, φ < .01). The desire to help also marginally predicted greater likelihood of donating (i.e., lower likelihood of a zero value; B = −0.45, 95% CI = [–0.93, 0.03], p = .07), while empathic concern did not (B = 0.04, 95% CI = [–0.43, 0.51], p = .87); see the second panel of Figure 5.
Discussion
The results supported our hypothesis that the desire to help would collapse in the presence of multiple victims, but only in the presence of self-affirmation. Self-affirmation did not affect the collapse of empathic concern. Furthermore, findings from Study 1 were largely replicated with respect to distress and donations. Specifically, empathic concern uniquely predicted increased distress, and the desire to help uniquely predicted higher levels and greater likelihood of donations. However, unlike in Study 1, empathic concern did not predict decreased likelihood of donations, which suggests that this unexpected effect is not reliable.
General Discussion
We hypothesized that compassionate responding may be best treated as multiple separable experiences that frequently occur together and identified empathic concern and the desire to help as two such experiences. Data from two studies supported this hypothesis. Moreover, we predicted that different factors would cause empathic concern or the desire to help to either collapse or not. These hypotheses were supported such that perspective taking prevented the collapse of empathic concern, which would otherwise occur in the face of multiple victims among those with high emotion regulation ability. Conversely, self-affirmation facilitated the collapse of the desire to help multiple victims. In addition, we hypothesized and found that empathic concern and the desire to help predicted different outcomes such that empathic concern was associated with distress, while the desire to help predicted likelihood of pledging to help via donation as well as donation amount. These findings have implications for understanding the nature of compassionate responding as well as interpreting effects previously reported in the literature. In light of recent research on the collapse of compassion (Cameron & Payne, 2011, 2012), the present work may help to determine exactly what is collapsing, or being downregulated, due to situational constraints. The present work may also help us to better understand when and why compassionate responding affects individual well-being and prosocial behavior.
Defining Compassion
Compassion has been defined as a mixture of compassionate emotions as well as the motivation to act in benevolent, goal-directed ways (Goetz et al., 2010). We built on this characterization by empirically isolating the basic conceptual components of compassionate responding. Our analyses suggest that empathic concern and the desire to help are statistically distinct from one another. These findings advance an interesting alternative to existing (if tacit) assumptions that compassionate responding is a one-dimensional experience. Currently, accepted measures of compassion and related constructs do not reflect these two factors, instead focusing singularly on emotional responses (Batson, Early, & Salvarani, 1997), the tendency to engage in perspective taking (Lawrence, Shaw, Baker, Baron-Cohen, & David, 2004), or both (Davis, 1983). Such measures do not directly address the motivational component of compassionate responding, which we refer to as the desire to help. Our findings suggest the value of creating new measures of compassionate responding that cleanly assess both facets.
In addition, if compassionate responding consists of two separable factors, it may be important for researchers to design experimental manipulations that specifically target each facet. Doing so could reveal how these factors relate to one another. It is unclear when and how frequently these factors co-occur and whether there is a causal relationship between them. Evoking either factor may activate the other, such that manipulating any part of compassionate responding will ultimately elicit both empathic concern and the desire to help. Conversely, the desire to help may reliably predict empathic concern, but empathic concern may not reliably predict the desire to help or vice versa. This could be a generative area of future research.
When Does Compassion Collapse?
Given that compassionate responding may consist of two separable factors, we were interested in the notion that different parts of compassionate responding would collapse in the face of multiple victims (vs. one) under different circumstances. Specifically, we hypothesized and found that perspective taking would eliminate the collapse of empathic concern. That is, in the absence of perspective taking, empathic concern was lower for multiple versus single victims among people with high emotion regulation ability, meaning that, when they were able to downregulate their emotional responses, they did so. However, in the presence of perspective taking, empathic concern increased with victim number among these individuals, a result consistent with prior work in which participants reported feeling more empathic concern for those who needed greater amounts of instrumental help (Cialdini et al., 1997). In other words, even among people who had the ability to downregulate their emotional responses, perspective taking prompted them not to do so. Perspective taking may attenuate the impact of emotion regulation, allowing individuals to be more emotionally responsive to actual severity of need.
By contrast, we predicted and found that the desire to help would only collapse in the face of multiple victims if one were to affirm an important value. We believe that this effect occurred because self-affirming prior to a demanding helping situation should predict disengagement from difficult-to-attain goals (Vohs et al., 2013). In essence, affirming makes people more likely to accept that they may not have the necessary resources to meet situational demands or that their efforts will not ultimately make a difference, resulting in decreased motivation to help. We suggest that the situation presented in these studies (one or more suffering children in the Darfur region of Sudan) is especially demanding such that it is a high-need situation and that reevaluating the likelihood of successfully helping should reduce self-efficacy and curb helping motivation. In our data, after self-affirming, people disengaged from the goal to help others, potentially choosing instead to protect the self and one’s own resources in the face of a demanding situation. This finding suggests that the collapse of the desire to help, unlike the collapse of empathic concern, may not be about emotion regulation but instead about avoidance of spending unnecessary resources when one no longer feels efficacious and disengagement is possible.
Correlates of Compassionate Responding
Finally, we hypothesized that empathic concern and the desire to help would have different implications in potential helping situations. First, we predicted and found that empathic concern, separate from the desire to help, would be uniquely associated with distress but not with donation behavior. These findings suggest that, on its own, empathic concern could be largely unhelpful for both victims and potential helpers. They may also help to explain why empathic concern collapses, at least in the absence of perspective taking: Specifically, it may be the anticipated emotional state included in compassion that one avoids, more than the goal to help or the actual act of helping. Research has long shown that empathic concern is associated with distress (Batson, Early, & Salvarani, 1997; Batson et al., 1987), and individuals may be explicitly or implicitly aware of the connections between these emotional states. It is becoming increasingly apparent that empathic concern is not enough to reliably elicit helping behavior. In fact, it may evoke behaviors that are more closely related to risk aversion and self-protection, including ineffective forms of “helping” (Cameron, Spring, & Todd, 2017), a possibility that warrants further study.
We also predicted and found that the desire to help, separate from empathic concern, uniquely predicted higher levels of donations and a greater likelihood of donating but not distress. Previous research supports the idea that valuing the welfare of specific individuals is associated with prosocial behavior (Batson, Turk, Shaw, & Klein, 1995). We expect that almost all participants possessed the desire to help the suffering victims to some degree, though those desires coexisted with participants’ desires to protect themselves and their resources. In this context, strongly endorsing statements about desiring to help others, as some participants did, may have been more indicative of goal commitment than goal salience. That is, endorsement of such statements may indicate the presence of an implemental mind-set with respect to helping goals. According to the mind-set model of goal pursuit (Gollwitzer, 1990; Gollwitzer & Bayer, 1999; Gollwitzer et al., 2004), the process of goal pursuit involves two distinct mind-sets associated with differences in cognition, affect, and action. Although an implemental mind-set involves committing to a goal and planning means by which to achieve it, a deliberative mind-set involves considering multiple courses of possible action (in this case, helping vs. retaining resources). A reduction of competing goals (e.g., self-protection) and a heightened focus on the goal to help once one is in an implemental mind-set, thus could lead to increases in enacted prosocial behavior without accompanying increases in distress. This potential explanation for our findings suggests the value of exploring connections between compassion and the goals literature (e.g., Poulin, 2017).
The possibility that the desire to help and empathic concern differentially predict helping behavior and distress, respectively, has broad implications for studying the effects of compassion. Empathic concern and the desire to help are highly correlated, but our results strongly suggest they are not the same thing. As a result, their respective effects may be conflated if both are not measured and controlled for in the analyses. Previous work citing the effects of empathic concern on helping behavior may have unknowingly capitalized on variance more closely related to the desire to help. Our findings may inspire others to reanalyze existing data to further test this hypothesis. In addition, our findings suggest that researchers interested in helping behavior may benefit from specifically measuring desire to help in addition to empathic concern. Conversely, researchers who are interested in examining emotional reactions in response to others’ need may benefit from focusing specifically on empathic concern. Both facets of compassion are associated with important outcome variables. Regardless of one’s interests, the present work suggests the value of specificity in the study of prosocial emotions and behaviors. Differentiating between the desire to help and empathic concern could allow researchers to focus more precisely on their topics of interest and the outcomes of each facet.
Limitations and Future Directions
We acknowledge what we consider the primary limitation of the studies presented in this work: only one scale was used to examine facets of compassionate responding, the compassion scale used to demonstrate the collapse of compassion effect (Cameron & Payne, 2011). Using this scale made practical sense in that a major goal of our research was to explore when and why compassion may or may not collapse. Other measures of compassion may or may not yield the same results, though this scale is representative of broader conceptions of compassionate responding that exist in the literature, thus making it plausible that the results that we have presented will apply to other operationalizations of compassion as well.
Another limitation of the present research is that both studies presented used a specific compassion-evoking scenario used in prior collapse-of-compassion research (Cameron & Payne, 2011). This scenario specifically focused on compassionate feelings toward and willingness to help distant strangers. Thus, our results are silent about the nature and function of compassionate responding for more familiar or close others (cf. Cialdini et al., 1997). Future research should investigate compassionate responding in these contexts. Furthermore, future research replicating these findings with additional out-group targets would be beneficial, as the targets in both studies that we present were Sudanese children. For some, helping members of this particular group may have a unique sociopolitical meaning.
In addition, while the factor structure that we present was replicable across the two studies presented, both samples were drawn from the same population (University at Buffalo students). We cannot say for certain that these effects would replicate in other contexts. Further research testing the tenability of the proposed factor structure and effects within a sample drawn from a different population is needed to increase confidence in the generalizability of these findings.
Finally, we would like to acknowledge potential limitations inherent in using a donation pledge as a dependent variable. Despite the fact that privacy was maintained between participants, and each was assured that their responses would not be shared with anyone outside of the research team, participants may have felt pressured to donate given the socially desirable nature of donation behavior. Furthermore, we collected contact information to make our cover story more convincing, (e.g., that the Project Darfur Coordinator would contact them at a later time to collect their donation) for pledges to represent a stronger commitment. This may have heightened concerns with social desirability.
Research in the future should address exactly when empathic concern and the desire to help will and will not diverge. For example, seeing poverty-stricken strangers may evoke empathic concern, but without context, one may not have the desire to help those who are both different and far away. Conversely, one might desire to help another person but feel nothing for them in the instance of an instrumental relationship. For example, one may desire to help a coworker because their well-being and presence at one’s workplace ensure that one’s job runs smoothly. There are undoubtedly many other scenarios in which facets of compassion may behave independently rather than as one; we hope our research can serve as a starting point for the discovery of these scenarios and the processes that define them.
Conclusion
Compassionate responding can be conceptualized as an umbrella term referring to prosocial responses to others’ suffering. We identified two facets of compassionate responding that are theoretically meaningful: empathic concern and the desire to help. We provide evidence that these facets may function independently, as they are affected by different outside forces and differentially affect behavior. Despite the preponderance of published work associating empathic concern and prosociality, in our studies, empathic concern did not predict helping behavior, but having the desire to help did.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.