
Abstract
While prior research shows that higher-class individuals are perceived as more sensitive to pain than lower-class individuals, little is known about how perceptions of pain are shaped by changes in social class. Across a pilot study and five experiments with Chinese and U.S. participants (N = 1,202), we investigated whether social mobility direction influences judgments of pain sensitivity and treatment, and whether perceived tenacity serves as a mediating mechanism. Results indicated that although Chinese and U.S. participants perceived higher-class individuals as more pain-sensitive, they judged upwardly mobile individuals as less sensitive to pain than downwardly mobile individuals. This effect was driven by the attribution of greater tenacity to upwardly mobile targets, which in turn predicted lower pain sensitivity ratings and fewer pain treatment recommendations. These findings reveal a novel psychological pathway through which dynamic social class information shapes pain perception and treatment decisions, extending the literature beyond static class-based stereotypes.
Introduction
Perceived pain sensitivity—observers’ inferences about the intensity of another person’s subjective pain experience—plays a critical role in interpersonal judgment and decision-making, particularly in domains such as healthcare, social support, and resource allocation (Trawalter et al., 2012). A robust body of research has documented a consistent social class bias in pain perception: Individuals from higher social classes are perceived as more sensitive to pain than those from lower social classes (Bernardes et al., 2021; Brandão et al., 2019; Hollingshead et al., 2016; Summers et al., 2021, 2023). This bias is theorized to stem from lay beliefs about differential life hardship: Higher-class individuals are assumed to have led more sheltered lives, resulting in greater pain sensitivity and stronger reactions to comparable physical injuries (Cheek & Shafir, 2024; Summers et al., 2021).
However, this literature has predominantly treated social class as a static attribute, overlooking a significant and growing segment of the population: class migrants—individuals who have experienced substantial upward or downward social mobility. In both China and the United States, approximately half of the population experiences upward mobility relative to their parents or their own past (Chetty et al., 2017; X. Zhang, 2022). Static class categorizations fail to capture the dynamic trajectories that define these individuals’ lives. When social mobility information is salient, the direction of mobility (upward vs. downward) becomes a primary basis for impression formation (Petsko et al., 2022). The present research addresses this critical gap by investigating how social mobility direction shapes perceptions of pain sensitivity and pain treatment recommendations, and proposes perceived tenacity as a novel mediating mechanism underlying these judgments.
Perceiving Socially Mobile Individuals
Social mobility is not only a widespread societal phenomenon but also a psychologically salient dimension for social categorization. Pervasive cultural narratives, such as the “Chinese Dream” and the “American Dream,” reinforce the ideology that social hierarchies are permeable and that upward mobility is achievable through individual effort and determination (Pena, 2015; Wolak & Peterson, 2020). This salience is reflected in natural language, which possesses a rich lexicon to describe social ascent (e.g., rags to riches, 飞黄腾达) and descent (e.g., downwardly mobile, 一落千丈).
Because people spontaneously categorize others based on mobility direction, they are also likely to form corresponding stereotypes, consistent with theories of social categorization and stereotyping (Allport, 1954; Tajfel et al., 1971). When multiple social categories are available, salient mobility information can serve as a fundamental basis for trait inference (Petsko & Bodenhausen, 2020; Petsko et al., 2022). A growing body of research on perceptions of status change—a concept closely related to social mobility—consistently finds that individuals who ascend in status are perceived as more hardworking and as more determined than those who descend (Davidai & Gilovich, 2015; Klein & O’Brien, 2017; Pettit et al., 2022; Soliman & Buehler, 2018; Xie et al., 2022). This reasoning is grounded in an intuitive theory of social mobility, which posits that upward movement is perceived to require greater tenacity, a volitional facet of agency that captures the disposition to persist in goal-directed striving, to overcome obstacles, whereas downward movement is perceived as reflecting comparatively lower tenacity (Abele et al., 2016; Koch et al., 2024). Building on this intuition, individuals who ascend in social class are evaluated differently from those who do not: the latter are primarily construed through the lens of hardship, whereas the former are defined by their agency in upward mobility (Cheek & Shafir, 2024; Hoffman & Trawalter, 2016).
Importantly, these intuitive trait inferences about the tenacity of upwardly mobile individuals are grounded in the correspondence bias (Gilbert & Malone, 1995). When explicit information rules out dispositional causes of social mobility—for instance, when upward mobility is clearly attributed to external circumstances—observers may no longer infer heightened tenacity in upwardly mobile individuals. By contrast, in the absence of such explicit situational information, observers are more likely to default to dispositional attributions. Accordingly, we predict that, when the causes of mobility are unspecified, upwardly mobile individuals will be stereotyped as more tenacious than their downwardly mobile counterparts.
Perceiving the Pain Sensitivity of Socially Mobile Individuals
The established finding that higher-class individuals are seen as more pain-sensitive presents an intriguing puzzle when considering class migrants. We propose that this static class-based heuristic can be reversed when dynamic mobility information is available, due to a shift in the underlying dimension of judgment.
Judgments of pain sensitivity are not monolithic; they can be influenced by inferences along two distinct dimensions: physical susceptibility (how much pain the body is believed to feel) and psychological tolerance (how much pain the mind is believed to endure; Bourke, 2014; Gray et al., 2007). Research on gender and pain illustrates this distinction. Women are often perceived as physically more susceptible to pain, whereas men are believed to possess greater psychological tolerance (Robinson et al., 2001; L. Zhang et al., 2021). This explains the seemingly contradictory findings that women are believed to feel more pain from the same injury (focus on physical susceptibility), yet men are trusted more when they report pain, as their complaints are seen as more credible indicators of severe suffering (focus on psychological tolerance; Guzikevits et al., 2024; Paganini et al., 2023).
Research on race-based biases in pain perception has primarily focused on the physical susceptibility dimension. For example, Hoffman et al. (2016) showed that lay beliefs about biological differences between racial groups—such as less sensitive nerve endings or thicker skin—lead perceivers to judge Black individuals as less sensitive to pain. In contrast, research on class-based biases in pain perception has largely emphasized the psychological tolerance dimension. According to the toughness hypothesis, lower-class targets are perceived as having endured harsher life conditions and to have overcome greater adversity. This perception, combined with widely held beliefs about toughness—such as that “what doesn’t kill you makes you stronger”—leads perceivers to view lower-class targets as psychologically tougher (Cheek, 2025; Hoffman & Trawalter, 2016). As a result, they are judged to be less sensitive to pain (Summers et al., 2021, 2023).
However, the toughness hypothesis may not fully capture perceptions of upwardly mobile individuals. Although upward mobility is often seen as requiring the overcoming of substantial obstacles—and thus signaling high tenacity—such individuals are also perceived as experiencing improving life conditions, such that their cumulative hardship may not exceed that of downwardly mobile individuals. Under the toughness hypothesis, psychological tolerance attributed to lower-class individuals stems from perceived cumulative hardship and adaptation. In contrast, we propose that the psychological tolerance attributed to upwardly mobile individuals arises from a distinct source: perceived tenacity—an active, goal-directed capacity to overcome challenges that does not depend on chronically harsh conditions.
We ground this account in the dual-dimensional framework of pain perception (Bourke, 2014; Gray et al., 2007). Tenacity reflects the volitional facet of agency (Abele et al., 2016) and is closely linked to the capacity to endure pain in pursuit of valued goals. Cultural narratives across both American and Chinese contexts often portray tenacious individuals as capable of persisting through extreme suffering (e.g., Theodore Roosevelt continuing a speech after being shot; Goujian enduring hardship to achieve revenge). Through social transmission, such narratives may foster an intuitive association between tenacity and reduced pain sensitivity, leading people to infer that those who persist are less susceptible to suffering. Moreover, because tenacity implies sustained goal pursuit despite adversity, individuals high in perceived tenacity may be inferred to be more capable of enduring pain without disengagement. Accordingly, we hypothesize that upwardly mobile individuals will be perceived as less sensitive to pain overall than downwardly mobile individuals (H1), and that this effect will be mediated by perceived tenacity (H2).
Pain Sensitivity and Pain Treatment
Biases in pain perception are not merely academic; they have consequential downstream effects on pain treatment. Extensive research shows a positive relationship between perceived pain sensitivity and the allocation of pain relief. For example, Black and lower-class individuals—who are perceived as less sensitive to pain—receive less analgesic treatment than White and higher-class individuals, even for identical injuries (Hoffman et al., 2016; Summers et al., 2021; Trawalter et al., 2012).
While prior work has primarily linked undertreatment to inferences of physical insensitivity, we argue that a parallel bias can emerge from inferences of high psychological tolerance. When an observer evaluates an objective injury (as opposed to a subjective pain expression), they may reason that an individual perceived as more tenacious requires less intervention, assuming that such individuals are better able to actively manage and cope with the pain on their own. Supporting this, individuals known for high pain tolerance may receive more treatment only when they explicitly express pain, as their complaints are deemed more credible (L. Zhang et al., 2021). However, in the absence of such expressions, or when judging based on the injury itself, high tenacity may signal a lower need for treatment. We therefore hypothesize that upwardly mobile individuals will be recommended less pain treatment for their injuries, and that this effect will be sequentially mediated by perceived tenacity and reduced pain sensitivity (H3).
The Current Work
We present a pilot study and five experiments to test our hypotheses. The pilot study first established the cross-cultural generalizability of the static class-based pain perception bias in a Chinese sample, providing a necessary baseline against which to interpret the effects of dynamic mobility information.
Study 1a employed a between-subjects design to test H1 by manipulating a target’s childhood and current social class, creating clear upward versus downward mobility trajectories. Study 1b examined the cross-cultural robustness of the findings from Study 1a by replicating them with a U.S. sample. Study 2 used an experimental design in which the mediator was manipulated as a moderator to examine whether perceived tenacity mediated the association between social mobility direction and perceived pain sensitivity (H2). Study 3 used a between-subjects design with a lay sample to examine whether perceived tenacity and perceived pain sensitivity sequentially mediated the effect of social mobility direction on pain treatment recommendations (H3). Study 4 employed a within-subjects design with a sample of medical students to investigate whether perceived pain sensitivity mediated the effect of social mobility direction on pain treatment recommendations.
All materials, data, code, and supplementary materials are publicly available on the Open Science Framework https://osf.io/bgydz/overview?view_only=3c7b2dbd5e294700a67d4f43e0bca8d0. Studies 1b (https://aspredicted.org/g5mx2r.pdf), 2 (https://aspredicted.org/s6zu8u.pdf), and 3 (https://aspredicted.org/ct7ew8.pdf) were preregistered through AsPredicted.org.
Pilot Study
The present research examined the cultural generalizability of class-based biases in pain perception. Specifically, we tested whether individuals in a Chinese context—like those in Western contexts—perceive higher-class targets as more pain-sensitive than lower-class targets. We first focused on static social class to rule out potential cultural confounds, ensuring that any effects observed in the main studies on social mobility could not be attributed to culture-specific responses.
To isolate the effects of social class (pilot) and social mobility (main studies), we simplified the design by holding target gender constant: all targets were described as male. This approach minimized potential intersectional confounds (e.g., Gender × Class) and is consistent with prior research on race- and class-based pain perception biases (Bernardes et al., 2021; Mende-Siedlecki et al., 2022; Summers et al., 2021).
Method
Participants
Using G*Power 3.1 (Faul et al., 2007) to estimate the required sample size and referencing the effect size from Study 1a of Summers et al. (2021; d = 0.71), we determined that 66 participants were needed to achieve 80% statistical power at a significance level of .05. We recruited 80 adult participants (46 female; Mage = 33.11, SD = 10.22) through Credamo, a Chinese online platform (www.credamo.com). All participants completed the study by responding to an online questionnaire. There were no participant exclusions.
Procedure
In a between-subjects design (social class: high vs. low), participants were randomly assigned to read a brief description of a target individual. The social class manipulation was adapted from the procedure used in Study 2 of Cheek and Murray (2023). Participants read the following passage: Zhang Wei
1
is a 24-year-old Han Chinese male. He was born into a wealthy (poor) family. His parents have a very high (low) income, and his family never (frequently) worried about basic necessities such as food, housing, or other essentials.
Next, participants evaluated the target individual’s pain sensitivity. The pain sensitivity assessment consisted of 18 scenarios that could potentially cause pain, ranging from minor discomfort (e.g., shampoo in the eyes) to traumatic injuries (e.g., fingers caught in a car door). Participants rated how much pain the target person would feel in each scenario. The average of these 18 items was calculated as the pain sensitivity score (Trawalter et al., 2012; 1 = no pain at all, 4 = extreme pain; M = 2.50, SD = 0.51; α = .92).
Subsequently, participants evaluated the perceived wealth of the target person (“How wealthy do you think Zhang Wei’s life is?” 1 = very poor, 7 = very wealthy), and then rated their own pain sensitivity using the same 18 scenarios (M = 2.31; SD = 0.46; α = .90). Finally, participants provided demographic information, including gender and age.
Results
An independent samples t-test showed that participants perceived the low social class target as significantly less wealthy (M = 1.83, SD = 1.01) than the high social class target (M = 6.38, SD = 0.63), t(78) = 24.20, p < .001, 95% CI [4.18, 4.92], Cohen’s d = 5.41. This indicates that the manipulation of social class was successful.
An analysis of covariance (ANCOVA) was conducted with social class as a fixed factor, self-rated pain sensitivity as a covariate, and target pain sensitivity as the dependent variable. The results revealed a significant main effect of social class, F(1, 77) = 14.12, p < .001, η2 p = .16. Participants rated the pain sensitivity of the low-class target (M = 2.35, SD = 0.50) as significantly lower than that of the high-class target (M = 2.64, SD = 0.48), as shown in Figure 1.
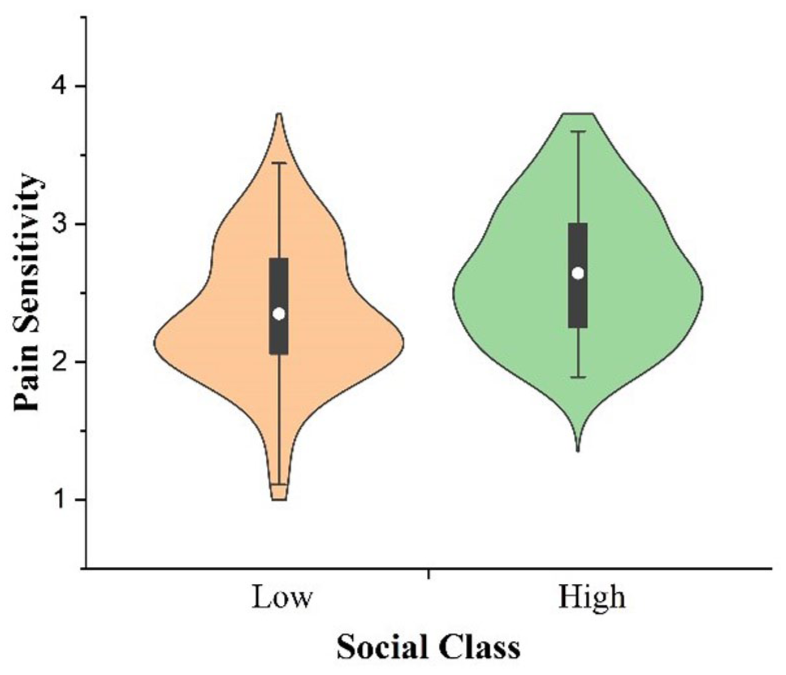
Violin plot of pain sensitivity ratings for high and low social class targets in the pilot study.
Discussion
The pilot study showed that Chinese participants, like those in Western samples (Bernardes et al., 2021; Brandão et al., 2019; Summers et al., 2021), perceived higher-class individuals as more sensitive to pain than lower-class individuals. This pattern holds across cultural contexts (Chinese, American, and Portuguese) and across participant and target gender, suggesting that class-based beliefs about pain sensitivity are culturally generalizable.
Crucially, if upwardly mobile individuals are perceived as less pain-sensitive than downwardly mobile individuals, such judgments cannot be explained by current class alone. Accordingly, Study 1a manipulated social mobility direction to compare perceived pain sensitivity between upwardly and downwardly mobile individuals.
Study 1a
The present study tested H1 by manipulating the target’s childhood and adulthood social class. To control for overall class exposure, the upwardly mobile target’s lower-class childhood was matched to the downwardly mobile target’s lower-class adulthood, with high-class experiences similarly aligned. This design equated exposure to high- and low-class contexts, isolating mobility direction as the only difference.
Method
Participants
Based on the sample size of Study 1b by Summers et al. (2021), the target sample size for Study 1a was set at 200 participants. A total of 200 Chinese adult participants (117 women; Mage = 31.92, SD = 8.32) were recruited via the Credamo platform and took part in the study by completing an online questionnaire. There were no participant exclusions. A sensitivity analysis was conducted using G*Power 3.1 (Faul et al., 2007), which indicated that this sample size would allow for the detection of a small-to-medium effect size (η2 p = .038) with 80% power at a significance level of .05.
Procedure
Using a between-subjects design (social mobility direction: upward vs. downward), participants read a description of the target individual. In the upward (downward) social mobility direction condition, they read: Zhang Wei is a 30-year-old Han Chinese male. He was born into a poor (wealthy) family, and his parents had very low (high) incomes. As a child, his family often (never) struggled to afford food, housing, or other basic necessities. However, he is now wealthy (poor), with a high (low) income, and no longer (often) worries about these necessities.
Using the same measure as in the pilot study, participants next evaluated the target’s pain sensitivity (M = 2.37; SD = 0.46; α = .90). They then indicated their perception of the target’s social mobility direction (1 = from rich to poor, 2 = from poor to rich), followed by a self-assessment of their own pain sensitivity (M = 2.39; SD = 0.41; α = .87). Finally, they provided demographic information, including gender and age.
Results
A chi-square test confirmed the effectiveness of the social mobility manipulation: 100% of participants in the upward condition perceived the change as from poor to rich, and 96% in the downward condition perceived it as from rich to poor, χ2(1) = 184.62, p < .001.
An ANCOVA with social mobility direction as the fixed factor and self-reported pain sensitivity as a covariate revealed a significant main effect of mobility direction on perceived pain sensitivity, F(1, 197) = 25.00, p < .001, η2 p = .11. Upwardly mobile targets were perceived as less pain-sensitive (M = 2.25, SD = 0.43) than downwardly mobile targets (M = 2.49, SD = 0.47; see Figure 2, Study 1a).
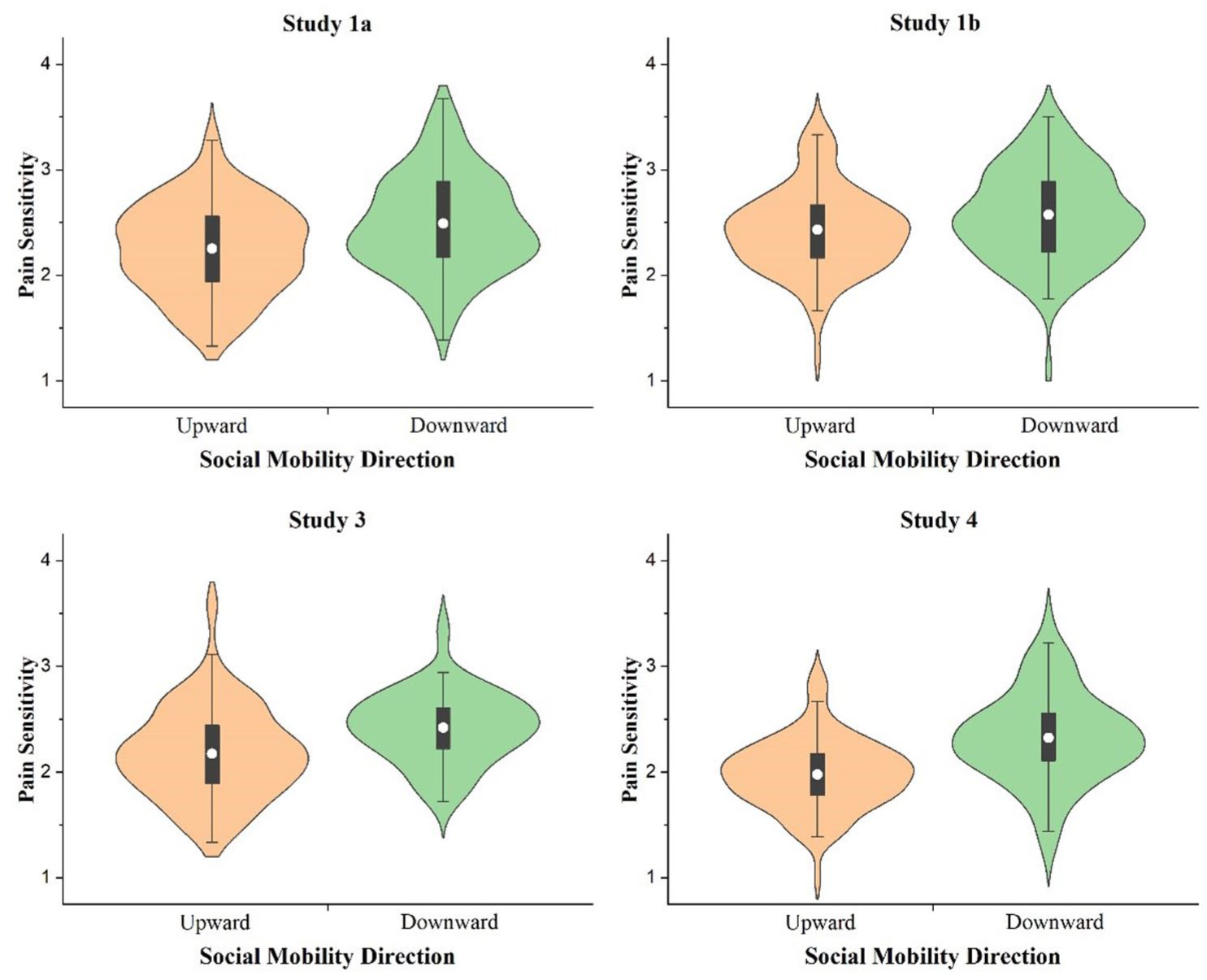
Violin plots of pain sensitivity ratings for targets with upward and downward social mobility directions in Studies 1a, 1b, 3, and 4.
Study 1b
Study 1b replicated Study 1a with American participants to test whether the pattern of findings generalizes across cultural contexts.
Method
Participants
Study 1b was preregistered with a target sample size of 200 participants. A total of 210 U.S. adult participants were recruited via the Prolific platform and completed an online questionnaire. Two participants failed the attention check items and were excluded from the analyses, resulting in a final sample of 208 participants (118 women, 88 men, and 2 prefer not to say; Mage = 46.37, SD = 13.51). The racial/ethnic composition of the sample was as follows: 175 White/Caucasian, 14 Black/African American, 9 Hispanic/Latino, 7 Asian/Pacific Islander, and 3 identifying as other racial/ethnic backgrounds.
Procedure
The procedure was identical to that of Study 1a, except that the target individual was named Jordan.
Results
A chi-square test confirmed the effectiveness of the social mobility manipulation: 99.02% of participants in the upward condition perceived the change as from poor to rich, χ2(1) = 98.04, p < .001, and 96.23% in the downward condition perceived it as from rich to poor, χ2(1) = 90.60, p < .001.
An ANCOVA revealed a significant main effect of mobility direction on perceived pain sensitivity, controlling for self-reported pain sensitivity, F(1, 205) = 18.04, p < .001, η2 p = .08. Upwardly mobile targets were perceived as less pain-sensitive (M = 2.43, SD = 0.40) than downwardly mobile targets (M = 2.57, SD = 0.44; see Figure 2, Study 1b).
Discussion
Study 1a and 1b found that upwardly mobile individuals—though currently occupying a higher social class than their downwardly mobile counterparts—were perceived as less sensitive to pain. This effect was cross-culturally robust and supported H1. A critical question, however, is whether these inferences reflect perceived tenacity or are instead driven by the toughness hypothesis. Study 2 directly adjudicates between these accounts.
Study 2
Study 2 examined whether perceived tenacity mediates the effect of social mobility direction on perceived pain sensitivity using a manipulation-of-mediation-as-moderator (MMM) design (Ge, 2023). Specifically, it examined whether (a) mobility direction shapes perceived tenacity, (b) blocking internal attributions for mobility alters these tenacity inferences, and (c) mobility direction interacts with tenacity manipulation to predict perceived pain sensitivity. Converging evidence across these tests would support H2 by demonstrating a mediating role of perceived tenacity.
The MMM design strengthens causal inferences about mediation, enables us to test whether external attributions attenuate mobility-based biases in pain perception, and provides a foundation for estimating a moderated mediation model. In addition, Study 2 measured perceived life hardship to examine the relationship between tenacity account and the toughness hypothesis in explaining mobility-based biases in pain perception.
Method
Participants
Based on the sample size in Study 1b of Summers et al. (2021), we targeted 100 participants per condition. With four levels of the independent variable, Study 2 required 400 participants. A total of 420 Chinese adults were recruited via Credamo and completed an online questionnaire; 5 failed the attention check, yielding a final sample of 415 participants (264 women; Mage = 31.67, SD = 8.82). Sensitivity analysis using G*Power 3.1 (Faul et al., 2007) indicated that this sample provided 80% power to detect a small effect (η2 p = .019) at a significance level of .05.
Procedure
Following the MMM framework, we employed a 2 (Social Mobility Direction: Upward vs. Downward) × 2 (Tenacity Manipulation: Control vs. Blocking) between-subjects design. Participants first read a description of the target. In the control condition, materials were identical to Study 1a except that the target’s age was described as middle-aged. In the blocking condition, participants were explicitly informed that the target’s social class change was due to external factors. In the upward mobility condition, participants were informed that the target’s transition resulted from a demolition and relocation program, 2 which provided substantial financial compensation and property. In the downward mobility condition, participants were informed that the target’s downward mobility resulted from a fire spreading from a neighbor’s home, leading to the loss of significant financial resources and property.
Participants subsequently evaluated the target’s tenacity. Perceived tenacity was assessed using three items adapted from the volitional facets of the Agency–Communion Inventory and the brief measure of four facets of social evaluation (Abele et al., 2016; Koch et al., 2024): determined, never gives up easily, and stands up well under pressure, which capture persistence in the face of obstacles. Participants rated the target on each item using a 4-point scale ranging from 1 (not at all) to 4 (extremely). The mean of the three items was calculated to form the perceived tenacity index (M = 2.85, SD = 0.86, α = .87).
Next, participants evaluated the target’s life hardship using a two-item scale from Trawalter et al. (2012), which asked, “How hard do you think Zhang Wei’s life has been?” and “How much adversity do you think Zhang Wei has overcome?” Responses were rated on a scale from 1 (not at all) to 4 (extremely). The mean of the two items was computed to form the perceived life hardship index (M = 3.01, SD = 0.64, α = .12).
Then, participants rated the target’s pain sensitivity (M = 2.28, SD = 0.46, α = .90), using the same measures as in the previous studies. Following this, they indicated their perception of the target’s social mobility direction (1 = from rich to poor, 2 = from poor to rich), followed by a self-assessment of their own pain sensitivity (M = 2.31, SD = 0.40, α = .87). Finally, participants provided demographic information, including gender and age.
Results
A chi-square test confirmed the effectiveness of the social mobility manipulation: 100% of participants in the upward condition perceived the change as from poor to rich, and 98.07% in the downward condition perceived it as from rich to poor, χ2(1) = 191.31, p < .001.
A two-way analysis of variance with perceived tenacity as the dependent variable revealed significant main effects of social mobility direction, F(1, 411) = 113.64, p < .001, η2 p = .22, and tenacity manipulation, F(1, 411) = 4.62, p = .03, η2 p = .01. Upwardly mobile targets were rated as more tenacious (M = 3.22, SD = 0.70) than downwardly mobile targets (M = 2.48, SD = 0.85), and targets in the control condition were rated higher (M = 2.93, SD = 0.92) than those in the blocking condition (M = 2.77, SD = 0.79). Critically, the interaction was significant, F(1, 411) = 74.31, p < .001, η2 p = .15: In the control condition, upwardly mobile targets were perceived as more tenacious (M = 3.60, SE = 0.07) than downwardly mobile targets (M = 2.25, SE = 0.07), F(1, 411) = 183.66, p < .001, η2 p = .31, whereas in the blocking condition, no difference was observed, F(1, 411) = 2.11, p = .15, η2 p = .005.
A two-way ANCOVA with self-rated pain sensitivity as a covariate and perceived pain sensitivity as the dependent variable revealed a significant main effect of social mobility direction, F(1, 410) = 52.36, p < .001, η2 p = .12, with upwardly mobile targets perceived as less sensitive to pain (M = 2.17, SD = 0.41) than downwardly mobile targets (M = 2.40, SD = 0.47). The interaction between social mobility direction and tenacity manipulation was also significant, F(1, 410) = 4.09, p = .04, η2 p = .01 (see Figure 3). Specifically, in the control condition, upwardly mobile targets were rated less sensitive (M = 2.12, SE = 0.04) than downwardly mobile targets (M = 2.46, SE = 0.04), F(1, 410) = 42.26, p < .001, η2 p = .09; in the blocking condition, this effect was attenuated (M = 2.18, SE = 0.04 vs. M = 2.38, SE = 0.04), F(1, 410) = 13.88, p < .001, η2 p = .03. The main effect of tenacity manipulation was not significant, F(1, 410) = .11, p = .75, η2 p < .001.
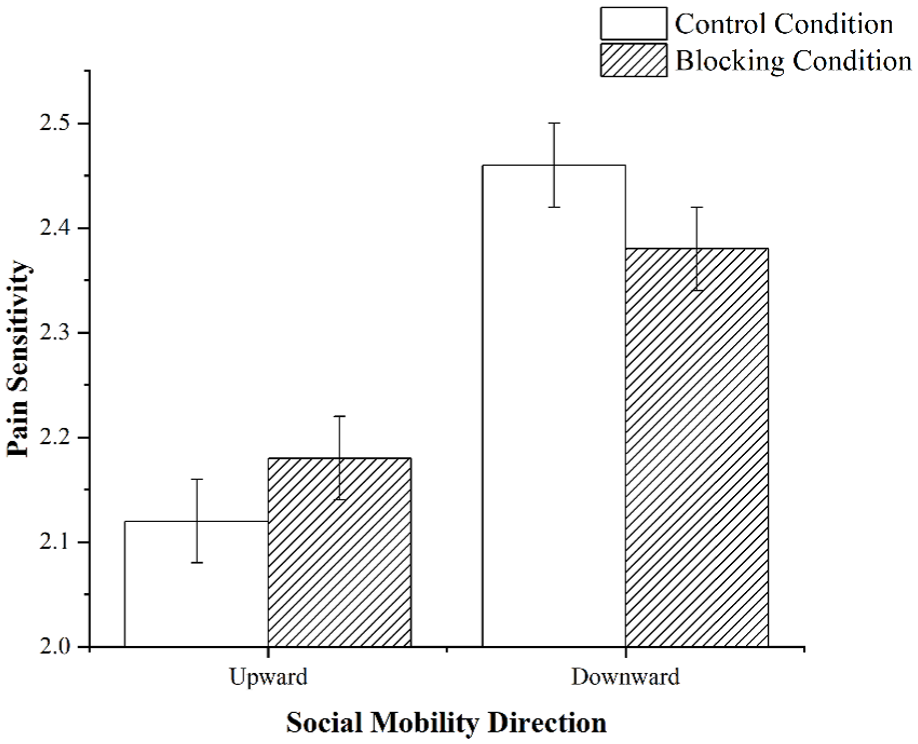
Interactive effect of social mobility direction and tenacity manipulation on perceived pain sensitivity (Study 2).
In the control condition, an independent-samples t-test on perceived life hardship showed a marginal difference, t(203) = 1.97, p = .05, 95% CI [−0.0002, 0.31], Cohen’s d = 0.28 (upward: M = 3.17, SD = 0.55; downward: M = 3.01, SD = 0.58). Due to low internal consistency, the two items were analyzed separately. Upwardly mobile targets were perceived as experiencing less hardship (M = 2.79, SD = 0.87) than downwardly mobile targets (M = 3.38, SD = 0.72), t(203) = −5.34, p < .001 [−0.82, −0.38], Cohen’s d = 0.74, but as having overcome more adversity (M = 3.54, SD = 0.59 vs. 2.64, SD = 0.90), t(203) = 8.54, p < .001 [0.70, 1.11], Cohen’s d = 1.18.
A moderated mediation analysis was conducted using PROCESS Model 8 (Hayes, 2022) with 5,000 bootstrap samples and 95% confidence intervals. Social mobility direction was the independent variable, perceived pain sensitivity the dependent variable, perceived tenacity the mediator, tenacity manipulation the moderator, and self-rated pain sensitivity a covariate. The moderated mediation was statistically significant, Hayes’ index = 0.16, 95% CI [0.10, 0.23] (see Figure 4). The indirect effect was significant in the control condition, [−0.25, −0.11]. Upwardly mobile targets were perceived as more tenacious than downwardly mobile targets, b = 1.34, t(200) = 13.38, p < .001 [1.14, 1.53]. In contrast, the indirect effect was not significant in the blocking condition, [−0.05, 0.01], as social mobility direction did not predict perceived tenacity, b = 0.14, t(205) = 1.41, p = .16 [−0.05, 0.33].
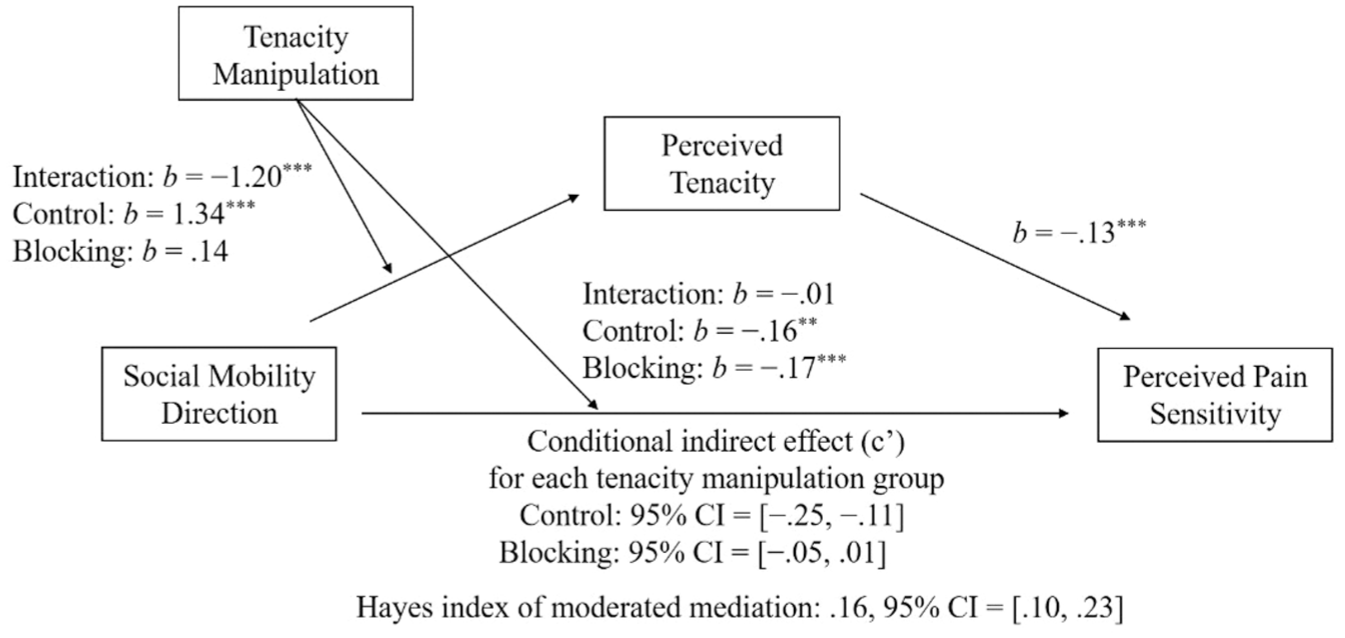
Indirect effects of perceived tenacity on the relationship between social mobility direction and perceived pain sensitivity, controlling for participants’ self-rated pain sensitivity (Study 2).
To examine the relationship between perceived life hardship and perceived tenacity, we first conducted correlational analyses among the two life hardship items, perceived tenacity, and perceived pain sensitivity within each of the two tenacity manipulation conditions (see Table 1). We then additionally included the two life hardship items as covariates in the moderated mediation model. The moderated mediation effect remained significant, Hayes’ index = 0.06, 95% CI [0.02, 0.11]. Although the mediating paths remained significant across both conditions, the effect size in the blocking condition [−0.05, −0.004] was weaker than that in the control condition [−0.14, −0.03]. Notably, R2 for perceived tenacity increased from .32 to .56 with the inclusion of the life-hardship covariates.
Correlations Among Variables by Tenacity Manipulation Condition (Study 2).
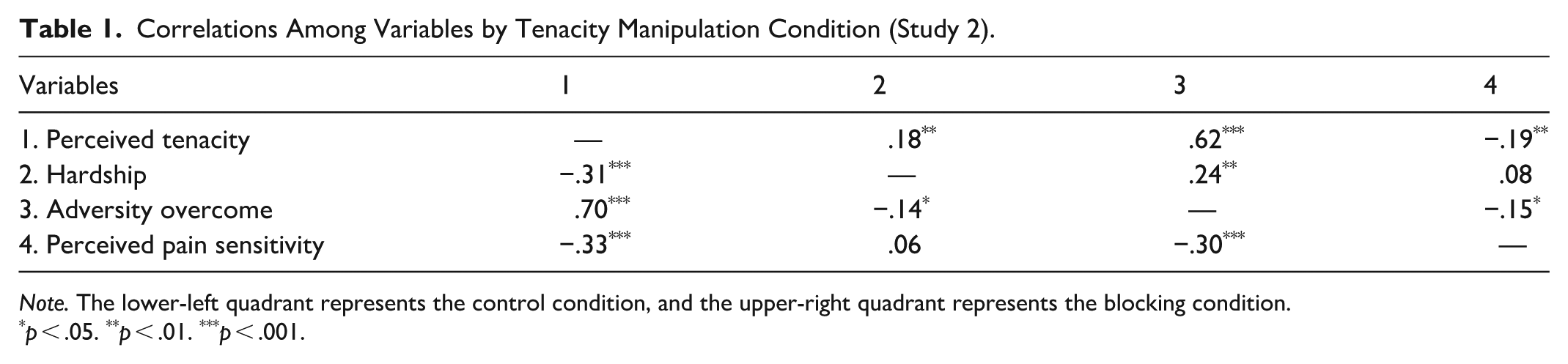
Note. The lower-left quadrant represents the control condition, and the upper-right quadrant represents the blocking condition.
p < .05. **p < .01. ***p < .001.
Discussion
Study 2, using the MMM design, found that social mobility direction influenced perceived tenacity, that blocking internal attributions effectively manipulated tenacity, and that the interaction between mobility and tenacity manipulation affected perceived pain sensitivity. These results, supported by a moderated mediation analysis, indicate that perceived tenacity mediates the effect of social mobility on perceived pain sensitivity.
Analyses of perceived life hardship revealed several noteworthy findings. First, the measure exhibited low internal consistency: upwardly mobile individuals were perceived as having overcome greater adversity, yet as experiencing lower overall hardship. Second, among the two items, overcoming adversity was positively associated with perceived tenacity, suggesting that both the toughness hypothesis and the tenacity account tap into the psychological tolerance dimension of pain perception. Third, after including the two life-hardship items as covariates, the previously non-significant mediation in the blocking condition became significant. This shift may be attributable to the substantial increase in explained variance in perceived tenacity (ΔR2 = .24), which likely reduced residual error and the standard errors of the path coefficients, thereby enhancing statistical sensitivity. These results further suggest that the external attribution manipulation may not fully eliminate the effect of social mobility direction on perceived tenacity. Fourth, after controlling for both life hardship items, the moderated mediation remained significant, and the indirect effect through tenacity in the control condition persisted. This pattern indicates that the tenacity account is not reducible to the toughness hypothesis but instead reflects a distinct form of goal-directed agency.
Study 3
Building on Studies 1a–2, Study 3 tested H3 by examining whether perceived tenacity and perceived pain sensitivity jointly mediate the effect of social mobility direction on treatment recommendations in a serial pathway.
Method
Participants
Study 3 employed a between-subjects design and set a target sample size of 100 participants per condition, resulting in an intended sample size of 200. A total of 210 Chinese adults were recruited via the Credamo platform, and no participant failed the attention check items. The final sample therefore consisted of 210 participants (139 women; Mage = 31.76, SD = 8.65). A sensitivity analysis was conducted using G*Power 3.1 (Faul et al., 2007), which indicated that this sample size would allow for the detection of a small-to-medium effect size (η2 p = .036) with 80% power at a significance level of .05.
Procedure
Study 3 used a between-subjects design, manipulating social mobility direction (upward vs. downward), with target descriptions identical to those in Study 1a except for describing the target as middle-aged.
Participants evaluated the target on perceived tenacity, pain sensitivity, and pain treatment. Perceived tenacity (M = 2.99, SD = 0.87, α = .89) and pain sensitivity (M = 2.30, SD = 0.41, α = .89) were measured in the same way as in Study 2. Pain treatment was assessed based on procedures adapted from Trawalter et al. (2012) and Summers et al. (2021). Participants evaluated which type of treatment should be used to relieve the target’s pain across seven injury scenarios (e.g., “He was in a car accident”; “He sprained his ankle”). Treatment options ranged in analgesic strength (1 = no pain medication, 2 = non-opioid pain medication [e.g., aspirin], 3 = weak opioid [e.g., codeine], 4 = strong opioid [e.g., morphine]). Higher values indicated stronger pain treatment (M = 2.36, SD = 0.54, α = .77).
Afterward, participants indicated their perception of the target’s social mobility direction, then assessed their own pain sensitivity (M = 2.25, SD = 0.39, α = .88) and pain treatment (M = 2.38, SD = 0.58, α = .80). Finally, participants provided demographic information, including gender and age.
Results
A chi-square test confirmed the effectiveness of the social mobility manipulation: 98.10% of participants in the upward condition perceived the change as from poor to rich, χ2(1) = 97.15, p < .001, and 96.19% in the downward condition perceived it as from rich to poor, χ2(1) = 89.61, p < .001.
According to the pre-registered statistical analysis plan, we conducted four analyses. First, an independent-samples t-test showed that upwardly mobile individuals were perceived as more tenacious (M = 3.64, SD = 0.34) than downwardly mobile individuals (M = 2.34, SD = 0.75), t(208) = 16.24, p < .001, 95% CI [1.14, 1.45], Cohen’s d = 2.23.
Next, an ANCOVA was conducted with social mobility direction as the independent variable, perceived pain sensitivity as the dependent variable, and self-rated pain sensitivity as a covariate. The results revealed a significant main effect of social mobility direction, F(1, 207) = 38.67, p < .001, η2 p = .16. Participants perceived the upwardly mobile individual as significantly less sensitive to pain (M = 2.17, SD = 0.44) than the downwardly mobile individual (M = 2.41, SD = 0.34; see Figure 2, Study 3).
Third, an ANCOVA was conducted with social mobility direction as the independent variable, the target’s pain treatment as the dependent variable, and self-rated pain treatment as a covariate. The results revealed a significant main effect of social mobility direction, F(1, 207) = 23.50, p < .001, η2 p = .10. Participants believed that the upwardly mobile individual required significantly less pain treatment (M = 2.24, SD = 0.55) than the downwardly mobile individual (M = 2.47, SD = 0.50).
Fourth, using Model 6 of the PROCESS macro in SPSS (Hayes, 2022), a bootstrap mediation analysis was conducted with 5,000 samples and 95% confidence intervals. Social mobility direction was entered as the independent variable, pain treatment as the dependent variable, perceived tenacity and pain sensitivity as mediators, and self-rated pain sensitivity and self-rated treatment as covariates. The overall regression model was significant, R2 = .42, F(3, 206) = 49.37, p < .001 (see Figure 5). Social mobility direction positively predicted perceived tenacity (b = 1.28, t(206) = 16.06, p < .001, 95% CI [1.12, 1.44]), which in turn had a negative effect on pain sensitivity (b = −0.12, t(205) = −3.00, p = .003 [−0.19, −0.04]). Pain sensitivity positively predicted pain treatment (b = 0.74, t[204] = 10.44, p < .001 [0.60, 0.88]). The direct effect of social mobility direction on pain treatment was not significant (b = 0.07, t[204] = 1.02, p = .31 [−0.06, 0.21]).
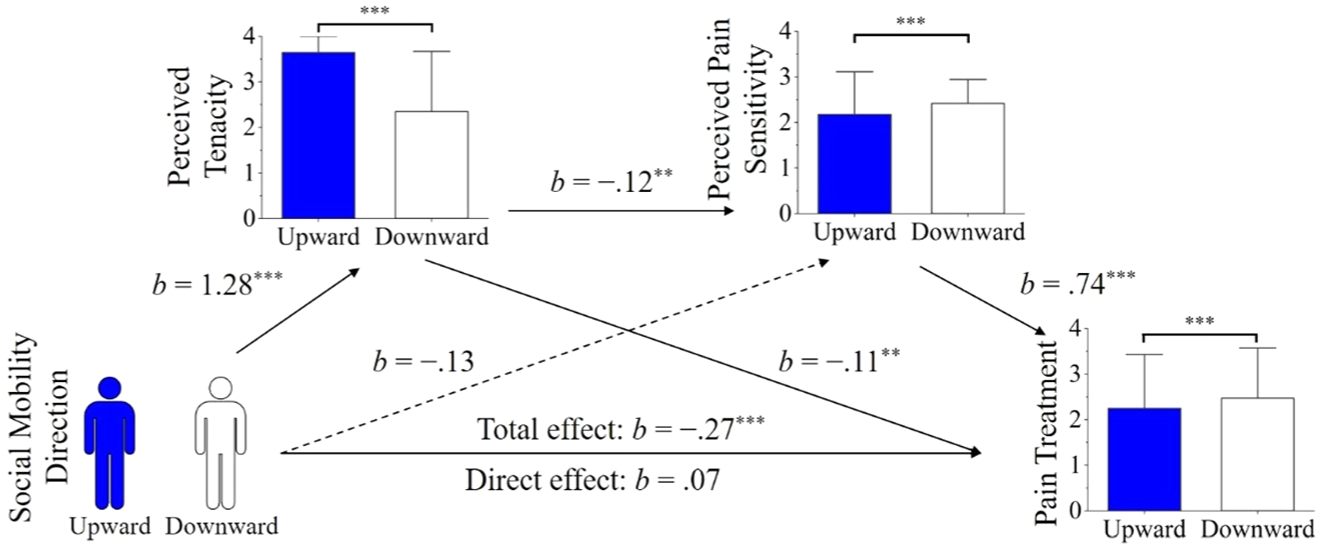
Sequential mediation pathway of perceived tenacity and pain sensitivity in the effect of social mobility direction on pain treatment, controlling for participants’ self-rated pain sensitivity and self-rated pain treatment (Study 3).
Discussion
Study 3 showed that perceived tenacity and perceived pain sensitivity sequentially mediated the effect of social mobility direction on pain treatment recommendations, supporting H3. Replicating Study 2, upwardly mobile individuals were perceived as more tenacious, which was associated with lower perceived pain sensitivity. These perceptions, in turn, reduced recommendations for pain treatment. These findings suggest that people tend to allocate more pain relief to those they perceive as experiencing greater pain, regardless of whether such perceptions are based on physical or psychological attributes.
However, because Study 3 focused on lay judgments, it remains unclear whether similar biases operate in clinical contexts, where pain treatment decisions are made by trained professionals. To address this issue, Study 4 examined whether future healthcare providers (i.e., medical students) similarly perceive upwardly mobile individuals as less pain-sensitive and less in need of pain treatment.
Study 4
Whereas Study 3 demonstrated a sequential mediation among laypeople, Study 4 tested whether perceived pain sensitivity mediates the effect of social mobility direction on pain treatment recommendations among medical students using a within-subjects design.
Methods
Participants
Following Studies 1a–3, the target sample size for Study 4 was set at 100 participants. A total of 89 undergraduate medical students (61 women, Mage = 21.45, SD = 1.33) from a medical university in China participated in the study by completing an online questionnaire. There were no participant exclusions. Among the medical students, there are 0 first-year, 2 second-year, 40 third-year, 23 fourth-year, and 24 fifth-year students. A sensitivity analysis conducted using G*Power 3.1 (Faul et al., 2007) indicated that this sample size would allow for the detection of a small effect size (η2 p = .02) with 80% power at a significance level of .05.
Procedure
Study 4 employed a within-subjects design, with social mobility direction (upward vs. downward) as the independent variable. Participants first read descriptions of two target individuals. Target descriptions were identical to those used in Study 1a, except that the downwardly mobile target’s name was changed to Li Qiang. 3
Participants evaluated both individuals in a counterbalanced order on pain sensitivity and pain treatment recommendations. 4 Perceived pain sensitivity was measured in the same way as in previous studies (α = .91 for upwardly mobile target, α = .86 for downwardly mobile target). Pain treatment recommendations were assessed in the same way as in Study 3 (α = .75 for upwardly mobile target, α = .56 for downwardly mobile target). Afterward, participants evaluated each target’s change in social class, then assessed their own pain sensitivity (M = 2.02, SD = 0.33, α = .85) and pain treatment (M = 2.06, SD = 0.43, α = .64). Finally, participants provided demographic information, including gender and age.
Results
A chi-square test confirmed the effectiveness of the social mobility manipulation: 95.51% of participants in the upward condition perceived the change as from poor to rich, χ2(1) = 73.72, p < .001, and 92.13% in the downward condition perceived it as from rich to poor, χ2(1) = 63.20, p < .001.
A paired-samples t-test on perceived pain sensitivity indicated that upwardly mobile individual (M = 1.98, SD = 0.34) was rated as feeling less pain than downwardly mobile individual (M = 2.33, SD = 0.43), t(88) = 7.20, p < .001, 95% CI [0.25, 0.44], Cohen’s d = 0.76; see Figure 2, Study 4.
A paired-samples t-test on pain treatment recommendations indicated that upwardly mobile individual (M = 1.95, SD = 0.39) was rated as requiring less pain treatment than downwardly mobile individual (M = 2.31, SD = 0.53), t(88) = 7.56, p < .001, 95% CI [0.27, 0.46], Cohen’s d = 0.78.
A mediation analysis was conducted using Model 1 of the MEMORE macro in SPSS (Montoya & Hayes, 2017), with social mobility direction as the independent variable, the pain treatment recommendations as the dependent variable, and perceived pain sensitivity as the mediator. The analysis used 5,000 bootstrap samples with a 95% confidence interval. The overall regression model was significant, R2 = .24, F(2, 86) = 13.75, p < .001. As shown in Figure 6, social mobility direction negatively predicted perceived pain sensitivity, b = −0.35, t(87) = −7.20, p < .001, 95% CI [−0.44, −0.25], which in turn positively predicted pain treatment recommendations, b = 0.43, t(86) = 4.42, p < .001 [0.24, 0.62]. The direct effect of social mobility direction on pain treatment recommendations was significant, b = −0.22, t(86) = −3.99, p < .001 [−0.33, −0.11].
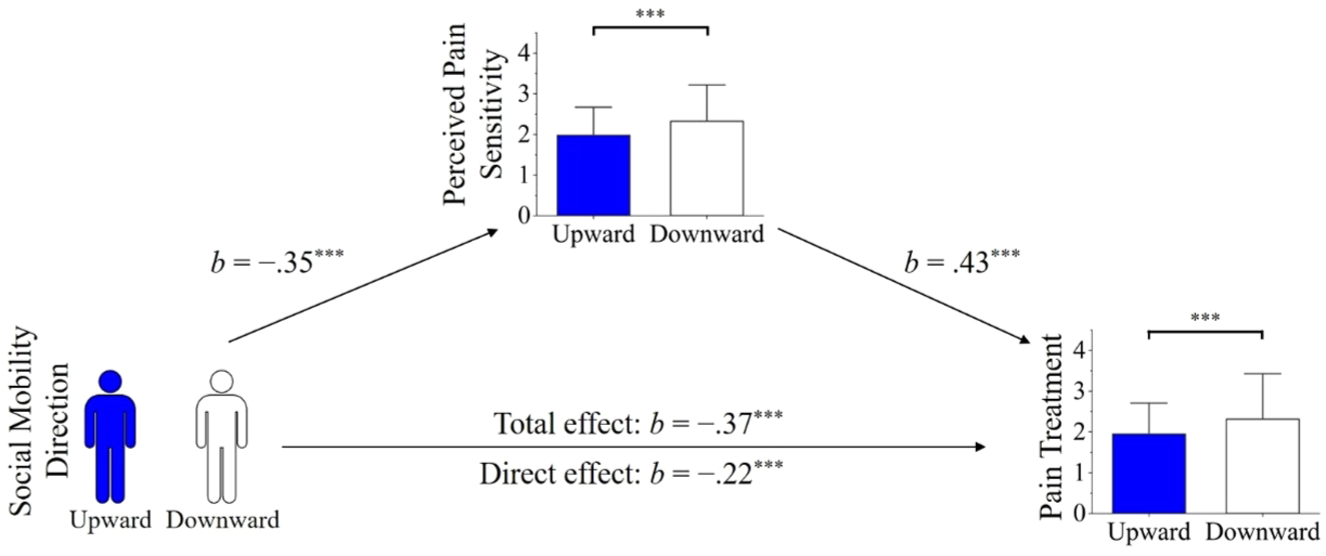
Mediation pathway of perceived pain sensitivity in the effect of social mobility direction on pain treatment (Study 4).
Discussion
Study 4 showed that medical students, like laypeople in Study 3, perceived upwardly mobile individuals as less sensitive to pain and therefore as requiring less pain treatment, providing further support for H3. Notably, these findings suggest that even with extensive medical training, judgments of others’ pain remain shaped by social stereotypes. This pattern aligns with prior research showing similar biases in pain perception based on race (Hoffman et al., 2016; Trawalter et al., 2012) and social class (Summers et al., 2021).
General Discussion
People’s perceptions of others’ pain are shaped not only by where they stand in the social hierarchy but also by the trajectory of their journey. While replicating the established finding that higher social class individuals are perceived as more pain-sensitive (pilot study), our primary experiments demonstrated that upwardly mobile individuals are perceived as less sensitive to pain than downwardly mobile individuals—a reversal driven by inferences of greater tenacity, which in turn led to recommendations for less pain treatment (Studies 1a–4). These effects emerged across China and the United States and among both laypeople and medical students, underscoring the robustness of this bias. This research makes several key contributions: It extends the study of pain perception from static categories to dynamic trajectories, identifies a novel psychological pathway (perceived tenacity) distinct from previously documented physiological attributions, and reveals a consequential bias in treatment judgments that persists among those with clinical training.
The Effect of Static and Dynamic Social Class on Pain Perception
Our findings illuminate how the same individual can be judged differently depending on whether static or dynamic class information is salient. The pilot study confirmed that within a static framework, Chinese participants, like their Western counterparts (Bernardes et al., 2021; Summers et al., 2021), perceive the wealthy as more pain-sensitive than the poor. However, Studies 1a and 1b revealed that introducing mobility information can override this static bias among both Chinese and U.S. participants.
This pattern suggests that people flexibly shift their evaluative perspective based on available social information (Petsko et al., 2022). When only current class is known, observers rely on a heuristic linking wealth to a life free of hardship and thus greater physical vulnerability. However, when information about class trajectory is provided, a different stereotype is activated—one that links upward mobility to tenacity. This perspective-switching underscores the dynamic nature of social cognition (Freeman & Ambady, 2011). Future research could explore how observers integrate or choose between these competing perspectives when evaluating individuals with complex, intersectional identities (e.g., an upwardly mobile Black woman; Crenshaw, 1991).
Physiological and Psychological Pathways in Pain Perception
Our work helps refine the theoretical architecture of pain perception by delineating two distinct inferential pathways: the physiological and the psychological (Bourke, 2014). The physiological pathway concerns beliefs about the body’s sensitivity to nociceptive input—the thickness of skin, the reactivity of nerve endings—and aligns closely with the experience dimension of mind perception, which captures perceived capacity for sensation and feeling (Gray et al., 2007). This pathway explains why Black Americans are stereotyped as feeling less pain than White Americans from the same injury (Hoffman et al., 2016). In contrast, the psychological pathway concerns beliefs about the mind’s capacity to endure suffering and corresponds to the agency dimension of mind perception, particularly its volitional-related facet (Gray et al., 2007). Consistent with this framework, we demonstrate that upwardly mobile individuals are slotted into this pathway: Their perceived tenacity leads to inferences of high pain tolerance, which in turn translate into lower overall pain sensitivity.
This dual-pathway model can resolve apparent contradictions in the literature. For instance, individuals with autism may be perceived as having endured significant life struggles (suggesting physiological toughness via the first pathway) yet also as emotionally vulnerable (suggesting psychological fragility via the second pathway), leading to the complex judgment that they feel more pain (Basargekar et al., 2024).
We propose that social groups can be mapped within a two-dimensional space defined by perceived pain receptivity (how much pain is felt) and pain tolerance (how much pain can be endured). This yields a typology that can parsimoniously categorize diverse stereotypes, see Figure 7. This framework offers a generative foundation for future research on the structure of pain-related stereotypes.
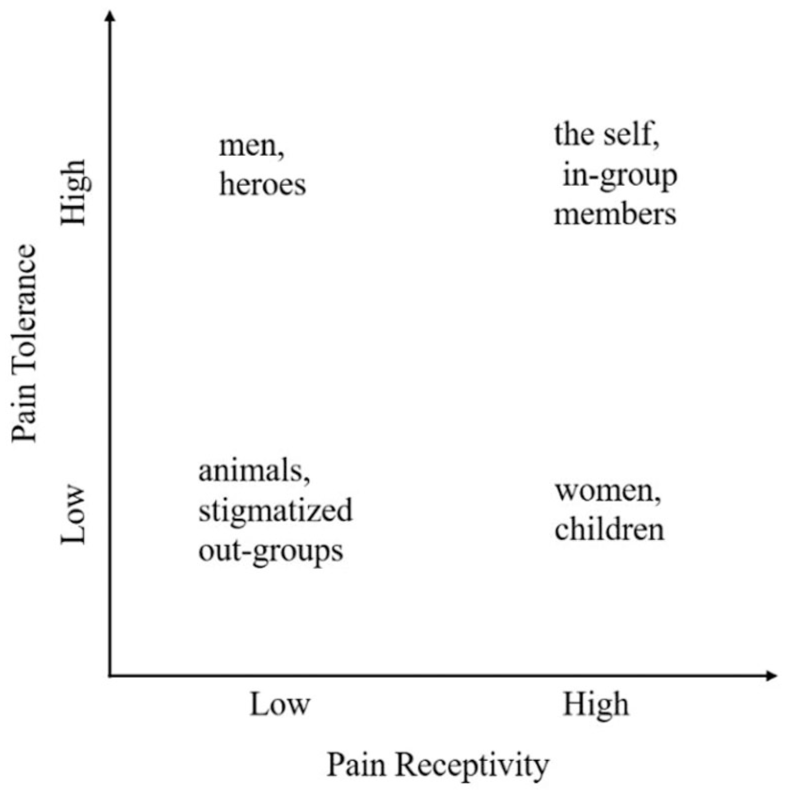
A two-dimensional model of pain perception.
Downstream Consequences of Pain Perception Biases
The biases we identified have direct and troubling implications for equitable care. Studies 3 and 4 found that both laypeople and medical students recommended less pain treatment for upwardly mobile individuals, a decision explained by their perceived lower pain sensitivity. This finding aligns with a basic principle in pain management: Those believed to be suffering less receive less intervention (Trawalter et al., 2012).
However, decisions based on these stereotypes are often empirically inaccurate and ethically problematic. For example, the stereotype that lower-class individuals are pain-insensitive leads to their undertreatment (Joynt et al., 2013), despite evidence that they actually exhibit lower pain tolerance and experience greater pain-related disability (Chou et al., 2016; Dorner et al., 2011). Our findings suggest the possibility of a similar, though psychologically distinct, undertreatment bias affecting upwardly mobile individuals, who are perceived as possessing greater tenacity.
A key question concerns how to reduce the undertreatment bias that healthcare providers may exhibit toward upwardly mobile individuals. We propose two potential intervention strategies to mitigate this bias. First, integrating objective assessments of injury severity with patients’ self-reported pain may help recalibrate treatment decisions. The undertreatment bias identified in the present research is grounded in objective injury information. However, when patients report equivalent levels of pain, healthcare providers may regard upwardly mobile individuals—perceived as more tenacious—as more credible reporters of their pain, and consequently be more inclined to administer adequate analgesic treatment. Thus, incorporating both objective indicators and subjective pain reports may foster more balanced pain perceptions and promote more appropriate pain management.
Second, adopting an individuated approach to patient perception may further reduce this bias. The undertreatment of upwardly mobile individuals appears to stem, at its core, from category-based judgments. When healthcare providers instead attend to richer, person-specific information—such as patients’ narratives (Charon, 2001)—they may be better able to move beyond stereotypes tied to social identity. This shift toward individuated understanding has the potential to disrupt category-based inferences and promote more accurate, compassionate, and equitable treatment decisions.
Limitations and Future Directions
While this research provides novel insights, several limitations should be addressed in future work. First, the scenario-based paradigm, while providing strong internal control, may lack ecological validity. Future research should employ more immersive methods, such as presenting videos of clinical consultations or using standardized patient paradigms, to examine whether these biases persist in more realistic and high-stakes settings. Second, because our studies were conducted in China and the United States, future research is needed to test the generalizability of these effects across other cultural contexts, especially those that vary in beliefs about social mobility and tenacity.
Third, our targets consisted exclusively of male individuals, which leaves open the question of how people perceive the pain sensitivity of women who experience upward social mobility. We propose at least two competing possibilities. On the one hand, men and women are believed to pursue status through distinct strategies, with men more likely to rely on dominance-based strategies and women on prestige-based strategies (Kakkar, 2024). Consequently, perceivers may assume that women attain higher social class primarily through social connections rather than personal tenacity, and thus may be less likely to implicitly associate upwardly mobile women with tenacity. For this reason, the underestimation of pain sensitivity observed for upwardly mobile men may be attenuated for upwardly mobile women. On the other hand, because women are generally perceived as lower in dominance and agency, whereas upward social mobility signals high tenacity, perceivers may view upwardly mobile women as atypical members of their gender category. Prior work has shown that atypical women elicit lower estimates of harm and suffering (Cheek et al., 2023; Goh et al., 2022; Kaiser et al., 2022). Thus, upwardly mobile women may be simultaneously perceived as high in tenacity and as gender-atypical, potentially leading to an even stronger underestimation of their pain sensitivity compared with upwardly mobile men. In summary, target gender may represent an important boundary condition of the present effects and warrants systematic examination in future research.
Fourth, future research should further disentangle tenacity from related constructs. Although our operationalization focused on the volitional facet of assertiveness rather than confidence, a supplementary study found that perceived assertiveness did not mediate the effect of social mobility direction on pain perception (see Supplemental Study). This may be because perceived confidence is unrelated to perceived pain sensitivity, thereby attenuating its mediating role. Moreover, although tenacity conceptually overlaps with overcoming adversity, it remains distinct from hardship. This distinction suggests that the tenacity account and the toughness hypothesis, while related, capture different psychological processes. The fact that both predict pain sensitivity under different conditions further indicates that pain perception is a multifaceted process shaped by multiple pathways. Accordingly, future research could conceptualize pain perception as a multidimensional construct to more comprehensively capture its underlying determinants.
Conclusion
In conclusion, this research demonstrates that perceptions of pain are not merely a reflection of one’s current social station but are profoundly shaped by the narrative of one’s journey through the social hierarchy. We have shown that upwardly mobile individuals are credited with greater tenacity, seen as less sensitive to pain, and ultimately deemed to require less pain treatment. By moving beyond static categories to study dynamic lives, we gain a more complete—and more complex—understanding of how social cognition can perpetuate biases in judgments of human suffering. This work opens a new avenue for research at the intersection of social class, person perception, and health equity, highlighting the power of life trajectories to shape our perceptions of others’ pain.
Footnotes
Acknowledgements
The authors sincerely thank the reviewers and editors for many productive suggestions during the interactive review.
Author Contributions
ZX conceived and designed the experiments, analyzed and interpreted the data, drafted the manuscript, and revised it. FW and CL contributed to manuscript revision. LS and LY contributed to the study design.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the General Project of Humanities and Social Sciences Research for Higher Education Institutions in Henan Province, China (Number 2026-ZZJH-323), and General Program Project of National Natural Science Foundation of China (32271128, 32471125).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.