
Abstract
At low dose and low dose rate, the system of radiological protection developed by ICRP is based on the linear non-threshold (LNT) relationship between dose and risk. In ICRP Publication 9, the Commission stated ‘As the existence of a threshold dose in unknown, it has been assumed that even the smallest doses involve a proportionately small risk of malignancies […]. The Commission is aware that the assumptions of no threshold and of complete additivity of all doses may be incorrect but is satisfied that they are unlikely to lead to the underestimation of risks’. ICRP Publication 26 laid down the basis of the current system of radiological protection and established a clear rationale between radiological risk assessment and radiological risk management. The effective dose concept was introduced in ICRP Publication 26 along with wT based on the relative contribution of organs to radiological detriment. Dose limits values were directly supported by quantitative risk criteria. This rationale is less apparent in ICRP Publication 60, which introduced a somehow less quantitative approach for radiological risk management, based on detriment, tolerability of risk, reasonableness of the optimisation process and acceptable level of risk. Over the last two decades, several scientific results have raised questions related to radiological risk assessment and consequences for risk management. This article investigates some of these questions and potential consequences to be considered for the future of the system of radiological protection.
Keywords
INTRODUCTION
The system of radiological protection aims at protecting humans and the environment against deleterious effects associated with ionising radiation exposure. With regard to human health, the objective of the system is to prevent tissue reactions and to maintain the probability of stochastic effects to an acceptable level, considering characteristics of the exposure situation. The first objective can be achieved by setting adequate dose limits, and the second objective relies on the implementation of the optimisation of radiological protection. Assessing radiological risk at low dose and low dose rate thus provides useful information not only to guide the implementation of the system but also to support the rationale behind dose criteria (dose limit, dose constraint, or reference level).
This article is about radiological risk at low dose and low dose rate, detriment, and the system of radiological protection. It is mostly based on a review of several ICRP Publications, which aims at highlighting important questions with regard to the preparation of the next set of general recommendations of ICRP.
RADIOLOGICAL RISK AND THE SYSTEM OF RADIOLOGICAL PROTECTION
LNT and the system of radiological protection
At low dose and low dose rate, the system of radiological protection is based on the prudent hypothesis of a linear non-threshold (LNT) relationship between dose and risk. In 1966, ICRP Publication 9 (ICRP, 1966) provided the following statement: ‘The mechanism of induction by radiation of leukaemia and other types of malignancy is not known. Such induction has so far been clearly established after doses of more than 100 rads, but it is unknown whether a threshold dose exists below which no malignancy is produced. […] The Commission sees no practical alternative, for the purposes of radiological protection, to assuming a linear relationship between dose and effect, and that doses act cumulatively. The Commission is aware that the assumptions of no threshold and of complete additivity of all doses may be incorrect but is satisfied that they are unlikely to lead to the underestimation of risks’. It is clear, from this statement, that the system of radiological protection is not only based on science but also on values such as prudence.
There has been, and there is still, a continuous debate about the scientific rationale of the LNT. It is the view of the author that since ICRP Publication 9, science has nothing but confirmed the rightfulness of the LNT relationship (Simon et al., 2022; Laurier et al., 2023) as the most adequate approach for radiological risk management. It should be kept in mind that LNT was not introduced as a scientifically established fact, but to support a practical approach for the management of radiological risk at low dose and low dose rate.
ICRP Publication 26
In ICRP Publication 26 (ICRP, 1977), the Commission introduces in its general recommendations the concept of detriment to quantify deleterious effects of exposure to ionising radiation: ‘the detriment in a population is defined as the mathematical expectation of harm incurred from an exposure to radiation, taking into account not only the probability of each type of deleterious effect, but also the severity of the effect’.
The Commission estimates that the mortality risk factor for radiation-induced cancer is about 10−2 Sv−1 as an average for both sexes and all ages and that the average risk factor for hereditary effects is about 4 × 10−3 Sv−1. These numbers are used to define the value of the dose limits for workers and for the public by making direct and quantitative comparison with other occupations: ‘the Commission […] believes it appropriate to assess the levels of risk that are associated with its dose-equivalent limits. The Commission believes that for the foreseeable future a valid method for judging the acceptability of the level of risk in radiation work is by comparing this risk with that for other occupations recognized as having high standards of safety, which are generally considered to be those in which the average annual mortality due to occupational hazards does not exceed 10−4’.
A risk of 10−4 year−1 can be associated with a dose in the range of 5 mSv year−1 (bearing in mind a detriment of 1.4 × 10−2 Sv−1). Considering (from practical experience) that the annual average dose over a worker population is not greater than 1/10th of the annual dose limit, the Commission recommends a dose limit for uniform irradiation of the whole body of 50 mSv year−1. For the public, the Commission indicates that ‘a risk in the range of 10−6 to 10−5 per year would be likely to be acceptable to any individual member of the public […] The assumption of a total risk of the order of 10−2 Sv−1 would imply the restriction of the lifetime dose to the individual member of the public to a value that would correspond to 1 mSv per year of life-long whole body exposure. For the reasons given in the following paragraphs, the Commission’s recommended whole-body dose-equivalent limit of 5 mSv in a year […]’. It is clear from this approach that radiological protection in practice does not aim at simply respecting the dose limit but is really aiming at reducing exposures far below the limit. The protection objective is around 1/10th of the limit.
In ICRP Publication 26, the values of dose limits for both workers and the public are directly related to the value of detriment and based on the level of risks which are judged to be acceptable. Optimisation of radiological protection (already) appears as the corner-stone of the system of radiological protection.
ICRP Publication 60
The rationale behind the selection of the dose limits evolved with ICRP Publication 60 (ICRP, 1991). ICRP Publication 60 confirmed the objective of the system of radiological protection ‘The Commission’s basic framework is intended to prevent the occurrence of deterministic effects, by keeping doses below the relevant threshold, and to ensure that all reasonable steps are taken to reduce the induction of stochastic effects’.
The Commission introduced an update value of detriment (mostly) based on the latest results from the LSS cohort follow-up, together with the concept of the dose and dose rate effectiveness factor (DDREF). The update value of detriment is significantly higher than the one in Publication 26 and led to a decrease of the proposed dose limits from 50 to 20 mSv year−1 for workers and 5 to 1 mSv year−1 for the public.
With regard to dose limitation, the Commission outlined that ‘It is the Commission’s intention to choose the values of dose limits so that any continued exposure just above the dose limits would result in additional risks from the defined practices that could reasonably be described as “unacceptable” in normal circumstances. Thus, the definition and choice of dose limits involve social judgements’.
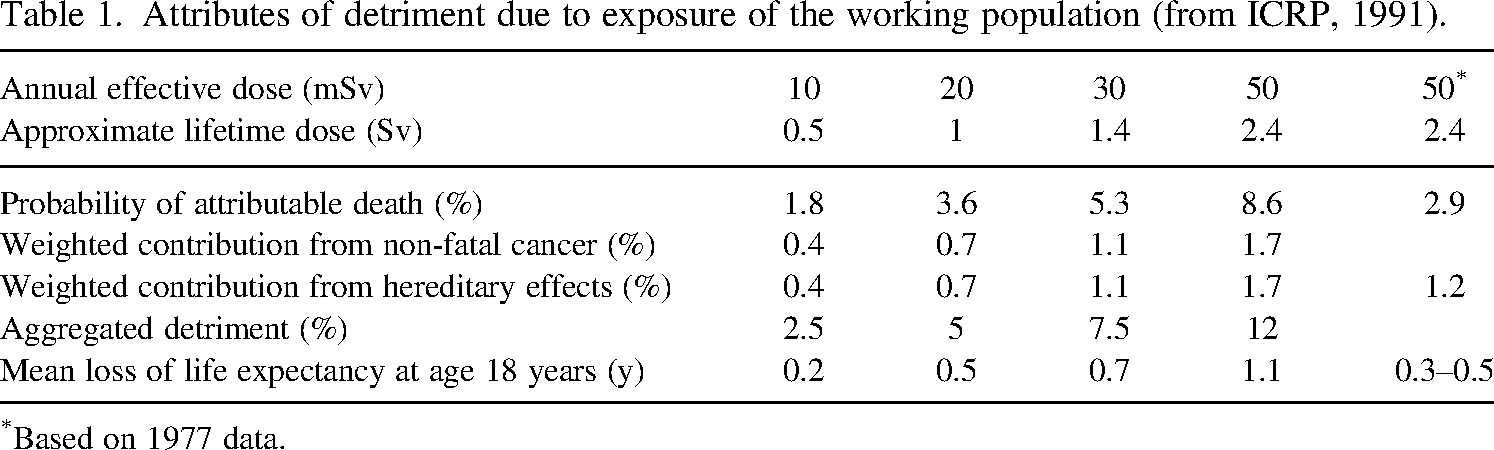
The Commission tested various values of annual effective dose as a basis for the dose limit for occupational exposure: 10, 20, 30, and 50 mSv per year. The results are shown in Table 1. It is worth outlining that the numbers shown in Table 1 include a DDREF of 2. The DDREF is the ratio between the risk or radiation detriment per unit effective dose for high doses and/or dose rates and that for low doses and dose rates. Such a factor was not considered in ICRP Publication 26.
Attributes of detriment due to exposure of the working population (from ICRP, 1991).
Attributes of detriment due to exposure of the working population (from ICRP, 1991).
*Based on 1977 data.
The Commission provided a judgement on what value gives rise to a combination of consequences that is judged to be just short of unacceptable, i.e. just tolerable, and this value was selected as the dose limit. The Commission recommended a limit of 20 mSv per year, averaged over 5 years (100 mSv in 5 years). In addition, the effective dose should not exceed 50 mSv in any single year.
The probability of attributable death associated with 20 mSv year−1 over the working lifetime appears to be higher than the probability of attributable death based on 1977 data and associated with the former 50 mSv year−1 dose limit. But the rationale behind the dose limit evolved, moving from a quantitative comparison of risks to a judgement of what is tolerable.
Optimisation of radiological protection (keeping exposures as low as reasonably achievable) appears as the most important aspect of radiological risk management, a key question being what should be considered as an acceptable level of risk with regard to the characteristics of an exposure situation (often referred to as prevailing circumstances). This is discussed in several ICRP publications. Among others, ICRP Publication 60 refers to a publication published in 1983 (Royal Society, 1983). This publication provides useful insights to guide the process of optimisation ‘The background spectrum of risks has often been canvassed as a possible source of information about the acceptability of risks. It has become abundantly clear from these attempts that there is no simple relationship between the acceptance of a risk and its detriment […]. There is not, and cannot be, a single acceptable level of risk’. Still, the publication provides some numerical criteria aiming at providing a structure to guide risk management. It considered several zones of risks as well as quantitative guidance:
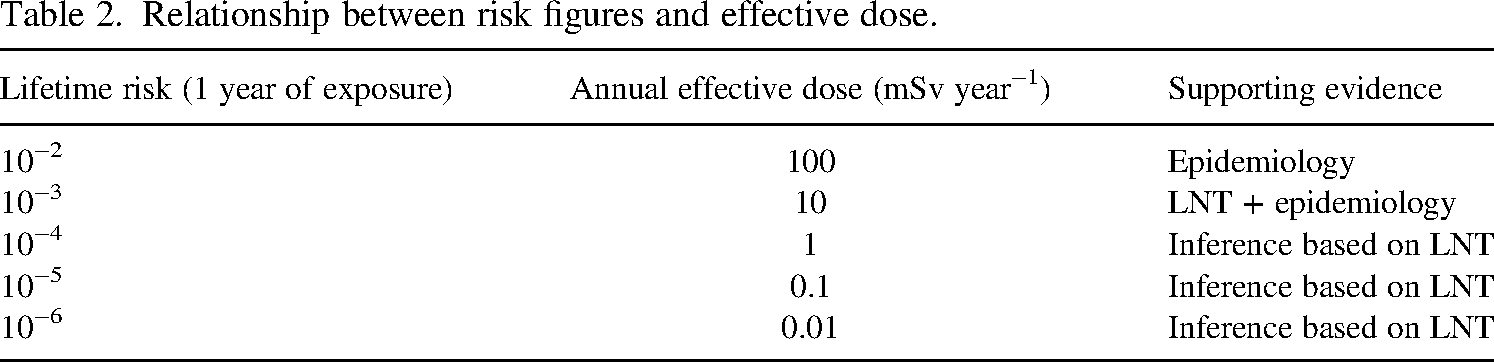
A continuing annual risk of death of 1 in 100, in addition to the risks from all other sources, should be described as unacceptable. An imposed risk of 1 in 1000 could hardly be called totally unacceptable provided the individual at risk knew of the situation, judged he had some commensurate benefit as a result, and understood that everything reasonable had already been done to reduce it. The current levels of fatal accidents averaged over broad areas of industry traditionally considered dangerous are mainly between 1 and 3 in 10,000 annually; For manufacturing industry as a whole the level is roughly 0.3 in 10,000. Few people would commit their own resources to reduce an annual risk of death that was already as low as 10−5 and that even fewer would take action at an annual level of 10−6.
ICRP Publication 147 (ICRP, 2021) provides effective dose values which can be associated with these numbers. These figures are provided in Table 2.
Relationship between risk figures and effective dose.
Relationship between risk figures and effective dose.
Considering these elements, the articulation between the principle of dose limitation and optimisation of radiological protection is summarised in Fig. 1. The choice of the dose constraint, as well as the acceptable level of dose, is related to the considered exposure situation.
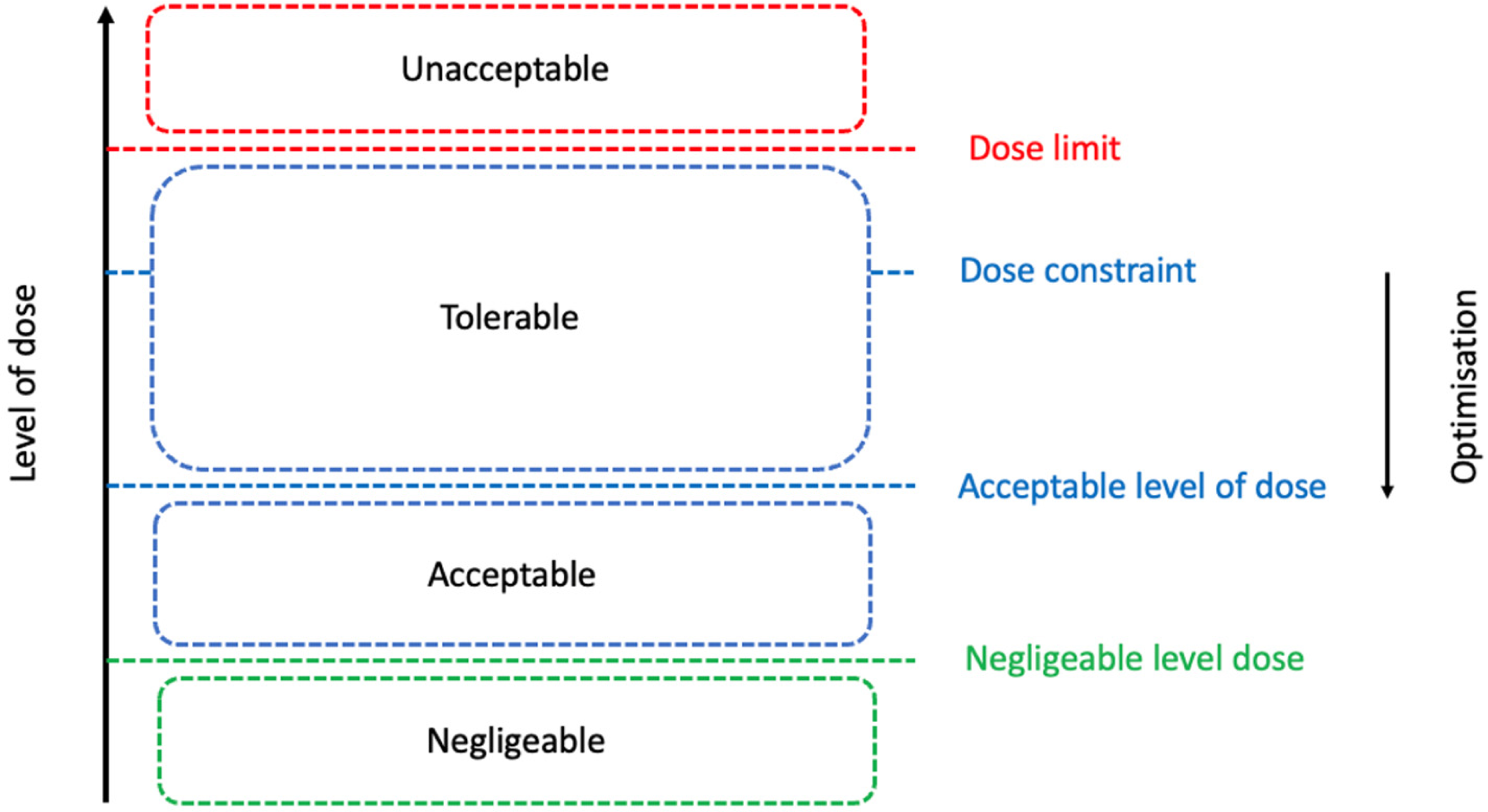
Articulation between the principles of dose limitation and optimisation of radiological protection.
The Commission updated its general recommendations in 2007 (ICRP, 2007). While the value of detriment was updated, the values of the dose limits remained unchanged and based on the same approach: ‘The Commission has concluded that the existing dose limits that it recommended in Publication 60 continue to provide an appropriate level of protection. The nominal detriment coefficients for both the workforce and the general public are consistent with, although numerically somewhat lower than, those given in 1990 […] On the basis of current data, the Commission judges that the occupational and public dose limits, including the limits on equivalent dose for the skin, hands/feet and eyes, given in Publication 60, remain applicable for preventing the occurrence of deterministic effects (tissue reactions)’.
ICRP Publication 118
In 2012, the Commission published a publication providing updated threshold doses for tissue reactions in a radiation protection context (ICRP, 2012). The threshold dose for a specified tissue reaction is the dose estimated to result in only 1% incidence of this tissue reaction. The relationship between dose, frequency, and severity of a tissue reaction is outlined in Fig. 2 (taken from ICRP Publication 118).
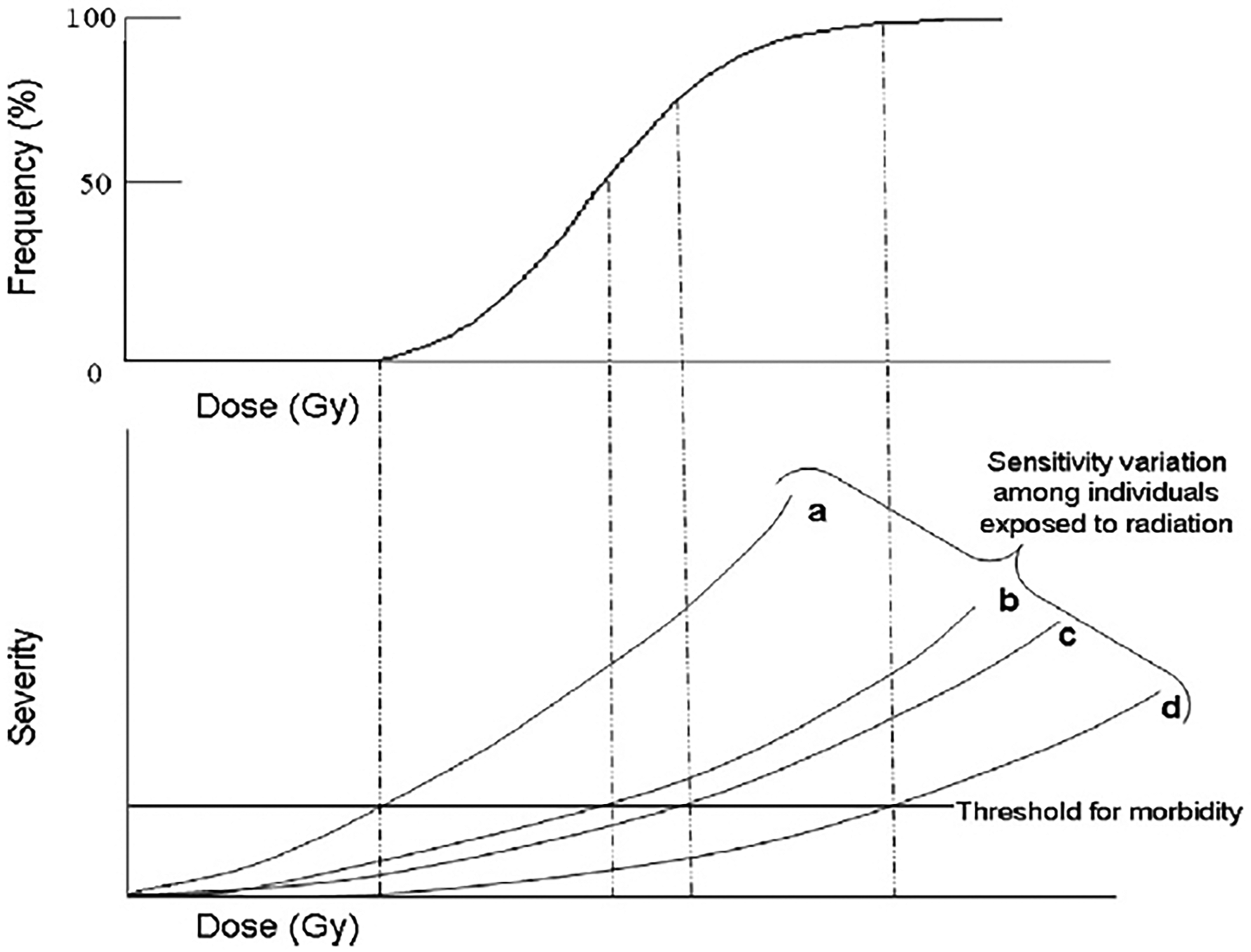
Relationship between dose, frequency, and severity of a tissue reaction.
This publication introduces significant changes for cataract and circulatory diseases. With regard to the latest, the commission indicates ‘From current evidence, a judgement can be made of a threshold acute dose of approximately 0.5 Gy (or 500 mSv, see note about units below) for both cardiovascular disease and cerebrovascular disease. On that basis, 0.5 Gy may lead to approximately 1% of exposed individuals developing the disease in question >10 years after exposure’.
The definition of the 0.5 Gy dose threshold for disease of the circulatory system is based on epidemiological results and detailed in the publication (it is based on an excess relative risk of 0.08 Gy−1 and an incidence rate of 30 to 50%). The numerical value nevertheless raises question with regard to the effective dose limit, as it cannot be stated that dose limitation allows for preventing tissue reactions, which questions the robustness of the system of radiological protection. Therefore, it reinforces the importance of optimisation of radiological protection, as indicated in the publication: ‘With the recent evidence, the Commission further emphasizes that protection should be optimized not only for whole-body exposures, but also for exposures to specific tissues, particularly the lens of the eye, the heart, and the cerebrovascular system’.
The system of radiological protection is based on scientific knowledge, values, and practical experience. With regard to values, ICRP Publication 138 (ICRP, 2018) clarifies the ethical foundations underlying the system. The Commission defines prudence as ‘making informed and carefully considered choices without full knowledge of the scope and consequences of an action. Prudence is reflected, for example, in the consideration of uncertainty of radiation risks for both humans and the environment’.
ICRP has launched the revision of its general recommendations, and several aspects must be carefully considered to ensure the system is robust and meets its objectives with regard to the protection of human health and the environment (Clement et al., 2021). Several ongoing task groups related to radiological risk assessment at low dose have already started to work: inference of risk at low dose and low dose rate (DDREF), update of detriment calculations for cancer, consideration of heritable effects, and disease of the circulatory system (DCS).
Among other topics, consideration of DCS within the system of radiological protection is a key challenge. Recent publications (Little et al., 2023; Peters et al., 2023) highlight questions regarding DCS incidence at low doses and their potential inclusion (or not) in the calculation of detriment. Scientific evidence is carefully considered, together with expert judgements, and the ethical values underlying the system of radiological protection. This work is achieved by ICRP Task Group 119 1 , in association with ICRP Task Group 123 1 .
Another important aspect to be considered with regard to detriment is the inference of risk at low dose and low dose rate. While LNT remains the basis for the current system of radiological protection at low dose, a judgement should be made on the use and value of the DDREF in the near future, considering both the low dose effectiveness factor (LDEF) and dose rate effectiveness factor (DREF). Outcomes of this work could have an important impact on the detriment value and, potentially, the choice of dose criteria which guide the implementation of the system.
While it was not discussed in detail within this article, detriment quantification has always included a component related to hereditary effects. In ICRP Publication 60, it represented around 15% of the detriment and only a few % in ICRP Publication 103. Epidemiology has not demonstrated, so far, an excess of risk of heritable effects at low doses. The methodological framework used in ICRP Publication 103 to estimate the hereditary risks of radiation exposure is described in a study by Amrenova et al. (2024), which indicates ‘the justification of including both in one single indicator of detriment, and consequently in the construction of the effective dose, may be debatable’. While there may be room for improvement of the current approach, the question of hereditary effects risk at low dose is a sensitive one, not only from a scientific perspective, and should be, also, carefully examined in the near future.
Defining dose criteria which are used to guide the implementation of the system of radiological protection is a multi-attribute process, which partly relies on the value of detriment and expert judgements. This is clearly illustrated in ICRP Publication 60 when defining the occupational dose limit, considering not only radiological risk quantification but also discussing tolerability and acceptability of risk, which are related to the characteristics of the exposure situation.
A revision of detriment, and its potential consequences on the system of radiological protection, including the selection of dose criteria, should be carefully considered, adopting a prudent attitude, keeping in mind the objectives of protection for human health, the need for practicality, and the history of the system.