
Abstract
The 2007 Recommendations of ICRP set out a system of radiological protection that is scientifically based, prudent in its assumptions, and practicable in its application. The system is designed to be straightforward in its use around the world, enabling the control of doses and risks arising from differing exposure situations, but it is not directed at specific individual circumstances. Effective dose is a fundamental concept in the ICRP system. It is a measure of dose that relates to risks of stochastic health effects in the context of a globally averaged population but is often applied, without sufficient thought, to particular exposures experienced by particular individuals. However, using the methodology used to derive risk coefficients for the ICRP 2007 Recommendations, an effective dose can be associated with a risk estimate that results from appropriate adjustments for sex, age-at-exposure, and (broadly speaking) population group. This process is illustrated by considering the risks associated with effective doses for a range of medical diagnostic procedures. In comparison with the aggregated detriment to health set out in the 2007 Recommendations for a population of all ages, enhancement factors of 2–3 are appropriate for exposure of a young boy and of 3–4 for a young girl. The aggregated detriment applies without enhancement to men aged in their mid-20s and women in their mid-30s but steadily reduces for increasing age-at-exposure, reaching a factor of 0.5 for men in their early-50s and women in their early-60s, and so on. It is debatable whether anything beyond such broad-brush adjustments of stochastic risk per effective dose is required for routine protection purposes, but this remains a central question for ICRP as the evolution of the system is considered. It is a question that will be explored by ICRP Task Group 128.
INTRODUCTION
The 2007 Recommendations of ICRP
The 2007 Recommendations of the International Commission on Radiological Protection (ICRP), as set out in ICRP Publication 103 (ICRP, 2007), present a system of radiological protection that is intended for everyday use and can be straightforwardly applied around the world. The 2007 Recommendations are based on (what was then) the latest available scientific evidence on the health effects of exposure to ionising radiation. The system adopted a prudent approach to risk estimation, but was not intended to be overly conservative, and was designed to be practicable in its application by those involved in routine radiological protection. The technical basis of the derivation of estimates of risks and detriment at low doses and low dose rates for the 2007 Recommendations has recently been set out in detail in ICRP Publication 152 (ICRP, 2022), and those wanting further information on this topic should consult this comprehensive report.
The fundamental objectives of the 2007 Recommendations have to be borne in mind when considering the derivation of risk estimates in the context of the ICRP system. In other words, the system is, in general, designed to be operational in every continent and readily applicable to exposures of population groups of both sexes and all ages (or working ages), rather than directed at specific individual circumstances. However, the variation of risk with population, sex, and age is taken into account when constructing the system.
ICRP (2007) recognised the many sources of uncertainty that are present in the derivation of the risk estimates used in its 2007 Recommendations. The intention was for judgements on uncertainties to be made on a prudent basis when adopting various values used in the system, and the risk estimates set out in ICRP Publication 103 must be seen in this light. They are not meant to be exact values with no uncertainty, but were selected as point estimates within the context of a workable programme of radiological protection, as briefly summarised here, and should be viewed as such.
The derivation of nominal risk coefficients
When considering the risk of cancer from low-level radiation exposure, ICRP derived excess relative risk (ERR, the proportional increase in risk over the background risk) and excess absolute risk (EAR, the additional risk over the background risk) models for 10 specific organs/tissues and the group of remaining solid cancers. These 11 pairs of models (ERR and EAR) were based on the Life Span Study (LSS) cancer incidence data for the Japanese atomic bomb survivors, as available at that time. These models did not include skin and bone cancers because of the limitations of the LSS data in deriving models for these cancers, and nominal risk estimates were adopted for these cancers (ICRP, 2022). The 11 pairs of cancer incidence risk models described the variation of the ERR and EAR with organ/tissue dose and allowed for the modification of risk with sex, age-at-exposure, and attained age or time-since-exposure; for solid cancers the dose–response models were linear, non-threshold, while for leukaemia the model was linear-quadratic, non-threshold.
Age-averaged lifetime cancer incidence risks were computed for two composite populations (Euro-American and Asian, representing the global population) and each sex using the ERR and EAR models with a uniform whole-body acute dose of 100 mGy of low-linear energy transfer (LET) radiation. For each sex, weighted averaging of these lifetime risk estimates derived from the 11 pairs of ERR and EAR models was conducted to account for transport of risks between populations with different baseline cancer incidence rates; the weights varied between cancer types but generally were 50%:50%. A dose and dose rate effectiveness factor (DDREF) of 2 was then applied for solid cancers (but not leukaemia); the linear-quadratic model adopted for leukaemia has a similar effect as the application of a DDREF of 2 for solid cancers. Finally, further averaging was carried out over sex and composite population (ICRP, 2022).
This process provided nominal risk coefficients for each cancer type, that is, the average lifetime EAR of cancer incidence per gray of organ/tissue dose of low-LET radiation; ICRP (2007) defined nominal as ‘sex-averaged and age-at-exposure-averaged lifetime risk estimates for a representative population’. Clearly, nominal risk coefficients do not apply to individuals and are not meant to apply to individuals. They are a link in the ICRP system that enables the risk-based control of doses at low levels of exposure.
The next step in the process adopted by ICRP (2007) is the introduction of a hereditary risk estimate so that in combination with cancer incidence risk estimates (including for skin and bone cancers), a full set of 14 nominal risk coefficients for stochastic health effects is obtained. Epidemiological studies have not provided reliable risk estimates for hereditary effects, so hereditary risk coefficients were obtained from laboratory animal experiments and (an incomplete) knowledge of human genetics (Amrenova et al., 2024). These nominal risk coefficients for stochastic health effects are each weighted by factors relating to the severity of the effect upon health, to produce values of detriment for 14 stochastic effects. It is these detriment values that are the basis of tissue weighting factors, wT, used in the calculation of effective dose (see below), which reflect the detriment of each stochastic health effect relative to the aggregated detriment (the sum of the 14 detriment values), as assigned to four broad groupings (i.e. wT takes on one of four values).
Organ/tissue absorbed doses (D, in Gy) are calculated for radiation exposures of reference anatomical models (phantoms) of the human body and are converted to organ/tissue equivalent doses (H, expressed in Sv) by applying radiation weighting factors, wR, appropriate for the absorbed dose of each type of radiation being considered. The wR values are a broad reflection of relative biological effectiveness (RBE) values relevant to stochastic health effects following low-level exposure, as compared to a reference low-LET radiation, and should be seen in the context of the system of radiological protection.
The sets of wR and wT adopted by ICRP (2007) permit the effective dose (E, expressed in Sv) to be calculated for all circumstances of low-level exposure, and effective doses implicitly allow the aggregated detriment values for different exposure circumstances to be compared. However, it must be appreciated that wR, wT, equivalent dose, and effective dose are all quantities defined by the ICRP 2007 Recommendations (ICRP, 2007) for a specific purpose and are not intended for use outside this ICRP system.
Effective dose
Effective dose, the central quantity in the current system of radiological protection, is obtained when the organ/tissue equivalent doses for the whole body are summed, with each organ/tissue equivalent dose weighted by the tissue weighting factor appropriate for the particular organ/tissue. In this way, for any distribution of radiation-type–specific absorbed doses between the various organs/tissues of the body, an effective dose may be calculated. However, it is important to appreciate that this is done with respect to a sex-averaged reference person (as defined in ICRP Publication 103; ICRP, 2007) rather than applying to any particular individual characteristics because the radiological protection system has been deliberately constructed to have general, rather than individual-specific, application. The process of obtaining an effective dose from a radiation exposure is summarised in Fig. 1 (ICRP, 2007), illustrating the sex-averaging of equivalent doses calculated separately using reference male and female phantoms.
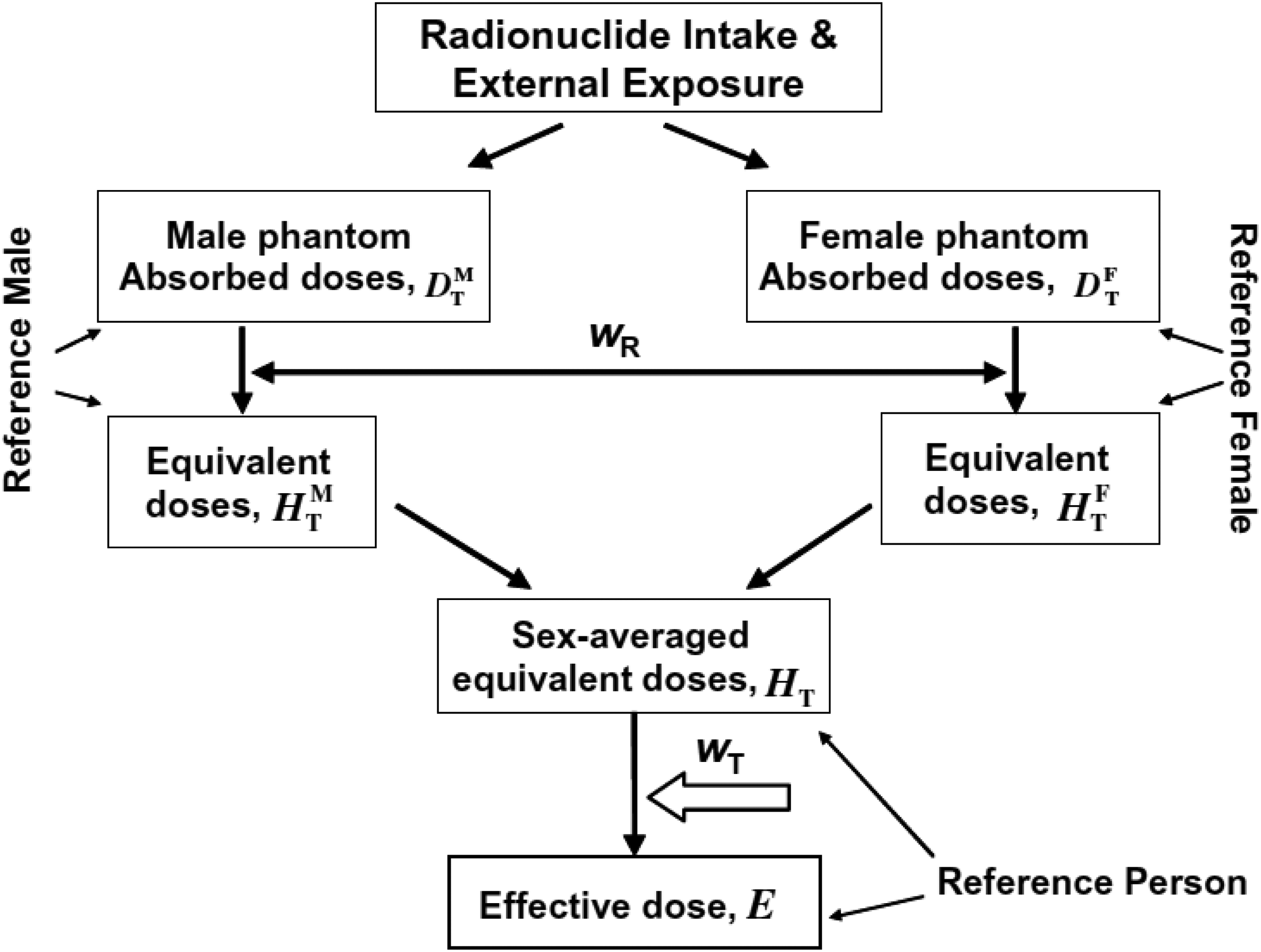
Schematic diagram of the process of obtaining the effective dose from a radiation exposure (ICRP, 2007).
To emphasise the point, the effective dose is a corner-stone of the system of radiological protection established by the ICRP (2007), but it does not apply to an individual as far as the specific risk of radiation exposure for that particular individual is concerned. The organ/tissue absorbed doses are calculated for a reference person using reference male and female phantoms, wR values are prudent radiation-type–specific weightings reflecting relevant RBE values, and wT values are obtained from the broad categorisation of appropriate averages of risk estimates over sex, age, and composite population. The use of effective dose allows all radiation exposures to be related to the ICRP severity–weighted nominal risk coefficients, i.e. the detriments, of 574 × 10−4 Sv−1 for a population of all ages and 422 × 10−4 Sv−1 for a working age population, expressed in terms of effective dose (ICRP, 2007). Effective dose is designed for specific use in the ICRP system of radiological protection and not for determining the risk to a particular individual in specific circumstances of low-level exposure.
However, effective dose can be used to indicate a broadly based risk for exposures experienced by particular categories of people (in terms of sex, age-at-exposure, and composite population) if appropriate adjustments are made, and this will be illustrated with respect to examples of medical diagnostic exposures in what follows. The issue of individualisation and stratification in radiological protection is the subject of deliberations by ICRP Task Group 128 (https://www.icrp.org/icrp_group.asp?id=204, accessed 8 January 2024).
Lifetime attributable risk by sex, age-at-exposure, and composite population
Fig. 2 shows the overall lifetime attributable risk (LAR, the preferred measure of the lifetime EAR) of cancer incidence resulting from a uniform whole-body dose of 10 mGy of low-LET radiation for a population of all ages. Skin and bone cancers are excluded (see Introduction), but otherwise the overall LAR is the summation of the LARs obtained for the 11 separate types of cancer. What is shown is the variation of the aggregated cancer incidence LAR by sex and age-at-exposure and also by composite population (i.e. the Euro-American and Asian composite populations used in ICRP Publication 103; ICRP, 2007). The LAR values are calculated using the sex- and age-at-exposure–specific ERR and EAR models derived by ICRP (2007) as applied to the two composite populations, with the resulting ERR and EAR estimates for each cancer type averaged using the appropriate cancer-type weightings, and a DDREF of 2 applied to all cancer types except leukaemia. Also shown in the figure is the overall nominal risk coefficient appropriate for this grouping of cancers (688 × 10−4 Gy−1), which is obtained from appropriately averaging the sex-, age-at-exposure-, and composite population–specific risks illustrated in the figure, as carried out by ICRP (2007) in constructing the current system of radiological protection, but in this instance excluding skin and bone cancers. Fig. 2 illustrates how the nominal risk coefficient for cancer incidence can be disaggregated into the sex-, age-at-exposure-, and composite population–specific risks, by working through the process conducted by ICRP (2007) prior to averaging these risks. Details can be found in ICRP Publication 147 and associated publications (Harrison et al., 2021, 2023; ICRP, 2021).
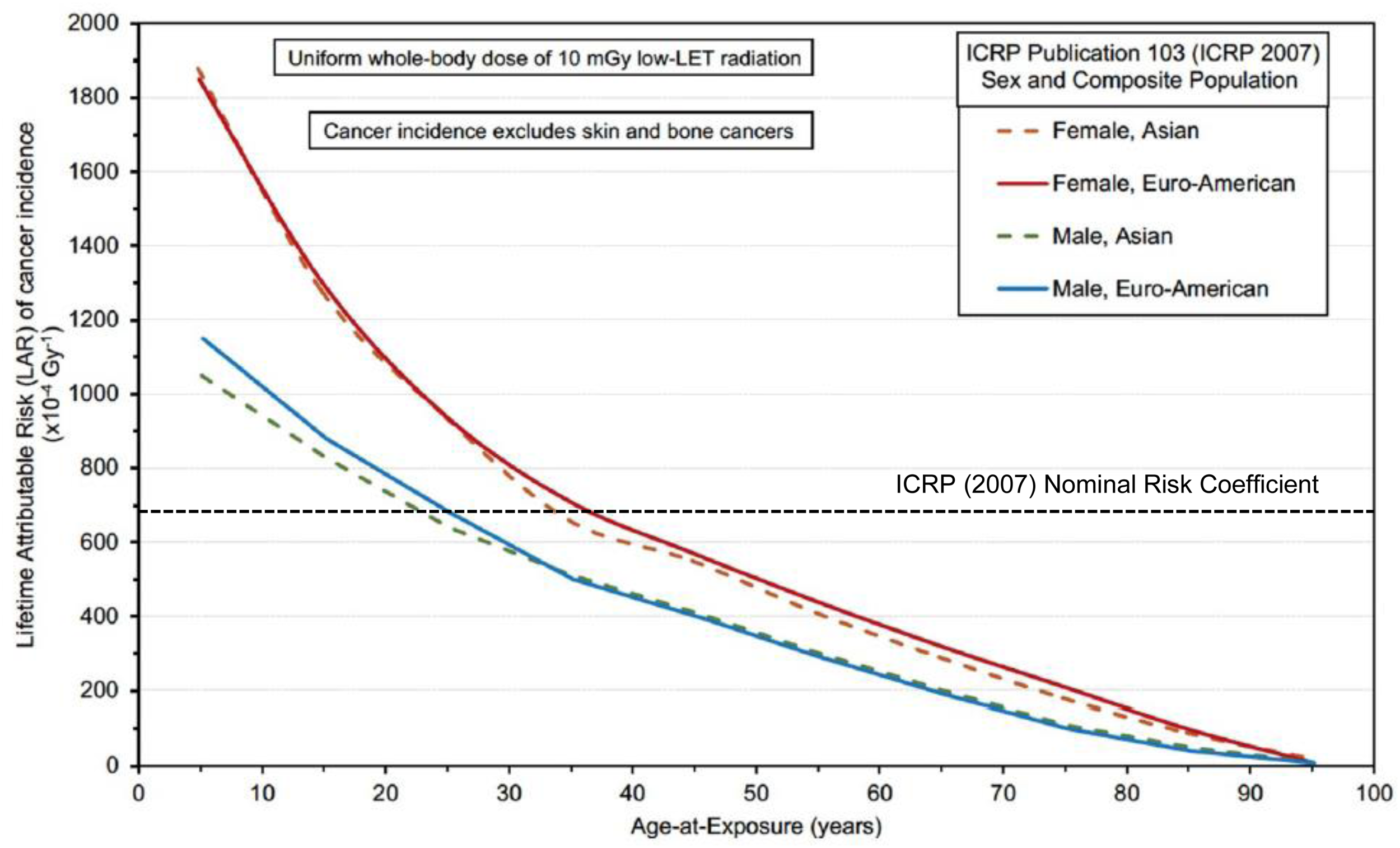
Variation of the LAR of cancer incidence (×10−4 Gy−1) with sex, age-at-exposure, and ICRP (2007) Asian and Euro-American composite population following a uniform absorbed dose of 10 mGy of low-LET radiation received by all organs/tissues of the body. Cancer incidence excludes cancers of the skin and bone (see text). Plots are based upon results presented in ICRP Publication 147 (ICRP, 2021), Tables 2.4 and 2.5, using the risk models and associated assumptions of ICRP Publication 103 (ICRP, 2007). Also shown is the ICRP (2007) nominal risk coefficient for all cancers excluding skin and bone cancers, which is the sex-, age-at-exposure-, and composite population–averaged LAR of cancer incidence.
It is shown in Fig. 2 that the LAR of cancer incidence is, for exposure at the age of 5 years, greater than the nominal risk coefficient, but within a factor of 2 for males and within a factor of 3 for females. The nominal risk coefficient provides an approximate estimate of the LAR for men exposed in their mid-20s and women in their mid-30s, and the LAR becomes half of the nominal risk coefficient for men aged around 50 years and women in their early-60s. The LAR continues to decrease with increasing age-at-exposure.
It is important to appreciate that the overall LAR of cancer incidence shown in Fig. 2 is composed of LAR estimates for 11 types of cancer. Therefore, the overall LAR varies with the doses received by different organs/tissues and how the risk for particular organs/tissues is modified by sex, age-at-exposure, and composite population. To illustrate this point, Fig. 3 shows how the LAR of the incidence of lung and thyroid cancers varies with sex and age-at-exposure for the Euro-American composite population.
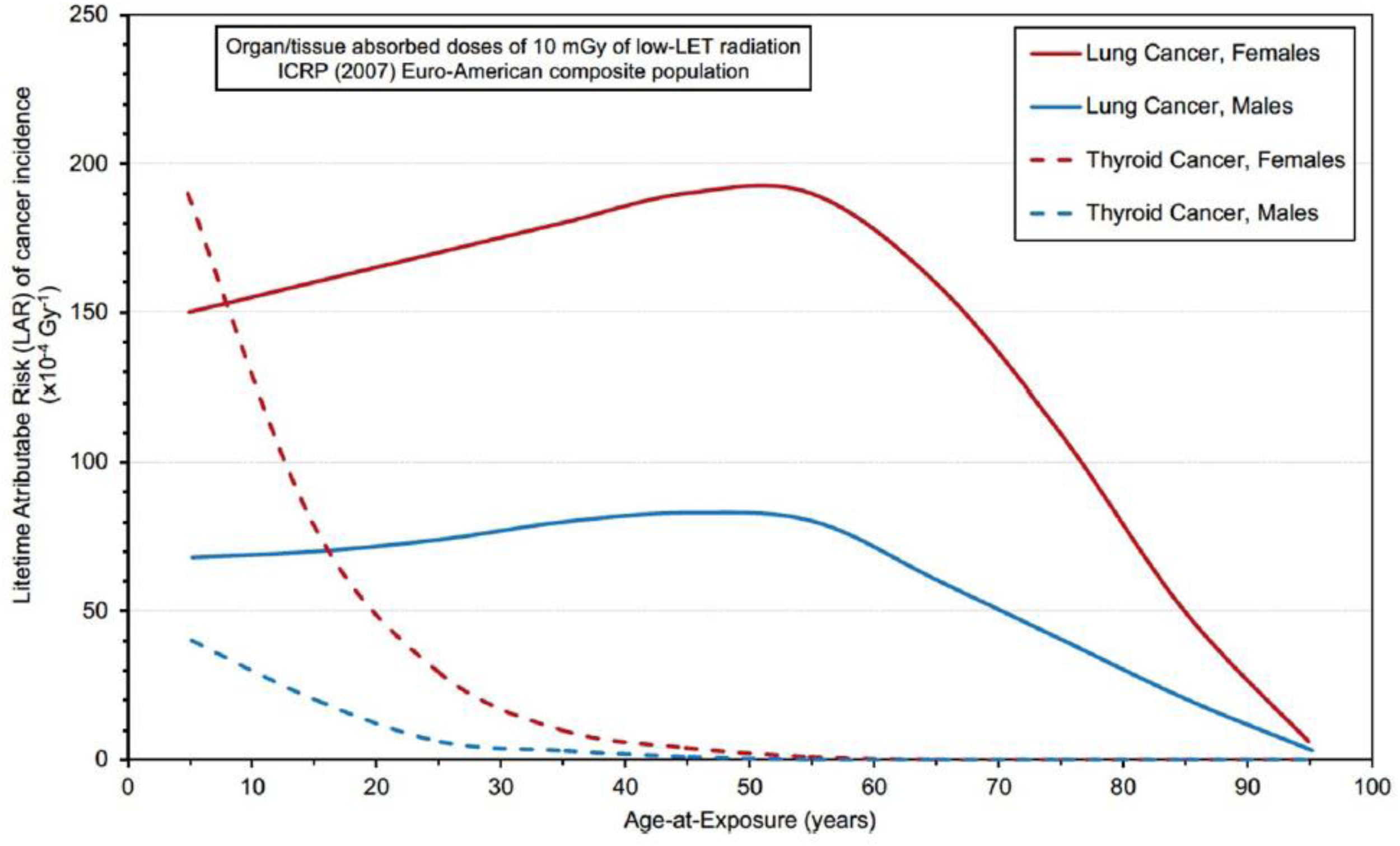
LAR of cancer incidence per organ/tissue absorbed dose (×10−4 Gy−1) from uniform exposure to low-LET radiation for the ICRP (2007) Euro-American composite population for lung and thyroid cancer incidence for females and males by age-at-exposure. Calculations performed with the ICRP (2007) risk models and organ/tissue doses of 10 mGy. Adapted from ICRP Publication 147 (ICRP, 2021), Fig. 2.1.
It is shown in Fig. 3 that the patterns of lifetime incidence risk are quite different for lung and thyroid cancers by sex and age-at-exposure. These differences between organ/tissue-specific risks are important when the distribution of doses between the organs/tissues of the body is heterogeneous because these different patterns of lifetime risks alter, to varying extents, the variations of risks shown in Fig. 2 for all 11 cancer types combined following a uniform whole-body exposure.
Doses from various x-ray examinations
For most medical diagnostic procedures, the organ/tissue doses received vary between organs/tissues, sometimes substantially. The overall LAR of cancer incidence from a particular radiological examination can be computed by applying the organ/tissue-specific risk models derived by ICRP (2007) to the doses received by these organs/tissues during the procedure and summing these cancer-type–specific LARs. It must be appreciated that the LAR estimates vary, not only with the distribution of doses between the various organs/tissues, but also with the sex, age-at-exposure, and (broadly speaking) the composite population from which the patient is drawn.
As noted above, effective dose is the central quantity used in the current protection system for the control of low-level exposures, and it enables the risk-based optimisation of protection. It can be used as a measure of the detriment to health arising from low levels of radiation exposure but applies broadly to population groups of both sexes and ranges of ages rather than as an estimate of risk that applies to a particular exposed individual. This is illustrated in Fig. 2 where the nominal risk coefficient appropriate for the incidence of all cancers except skin and bone cancers may be compared with the variation of the lifetime EAR of cancer incidence with sex, age-at-exposure, and composite population. The separate nominal risk coefficients for each type of cancer, which feed into the effective dose via the tissue weighting factors, are obtained by averaging over sex, age-at-exposure, and composite population, and the aggregated nominal risk coefficient is the sum of these component nominal risk coefficients.
For any particular medical x-ray examination, effective dose may be calculated in the standard way prescribed by ICRP (2007) in the 2007 Recommendations (see Fig. 1). However, the crux of the matter is whether, and if so how, the effective dose may be used to estimate the consequent risk of stochastic health effects under particular exposure circumstances (e.g. a procedure involving a patient of a certain age and sex). As illustrated in Fig. 2, the nominal risk coefficient of 688 × 10−4 Gy−1 for the lifetime EAR of the incidence of cancer (excluding skin and bone cancers) is most directly applicable to a man in his mid-20s or a woman in her mid-30s. Similarly, the use of effective dose with nominal risk coefficients and detriments will underestimate risk at younger ages and overestimate risk at older ages.
However, the LAR of stochastic health effects associated with a given effective dose can be adjusted based on categorisations of the sex, age-at-exposure, and composite population of the exposed person. To do this, an understanding of how the LAR of cancer incidence associated with the effective dose varies with different x-ray examinations needs to be established. Further information may be found in Harrison et al. (2023).
LAR per Sv for typical medical diagnostic procedures
Euro-American composite population
Fig. 4 shows how, for the Euro-American composite population, the LAR of cancer incidence (excluding skin and bone cancers) per effective dose varies with age-at-exposure for each sex, for 18 types of typical x-ray examinations. Here, the effective dose received from a particular procedure is calculated in the standard way set out in the 2007 Recommendations (i.e. it is independent of the sex, age-at-exposure, and composite population of the exposed individual) and compared with the aggregated LAR of cancer incidence calculated for the Euro-American composite population using the sex- and age-at-exposure–specific models for 11 types of cancer and the organ/tissue doses received during the x-ray examination. The variation in the aggregated LAR of cancer incidence per effective dose (LAR/Sv) estimates arises from the different organ/tissue doses received during a procedure and the nature of the risk models for the organs/tissues tending to receive higher doses, particularly in respect of the modification of the risk by sex and age-at-exposure. Also shown is the LAR/Sv variation by age-at-exposure for each sex for a uniform whole-body dose of 10 mGy of gamma radiation, i.e. an effective dose of 10 mSv, which is what is displayed in Fig. 2 for the Euro-American composite population.
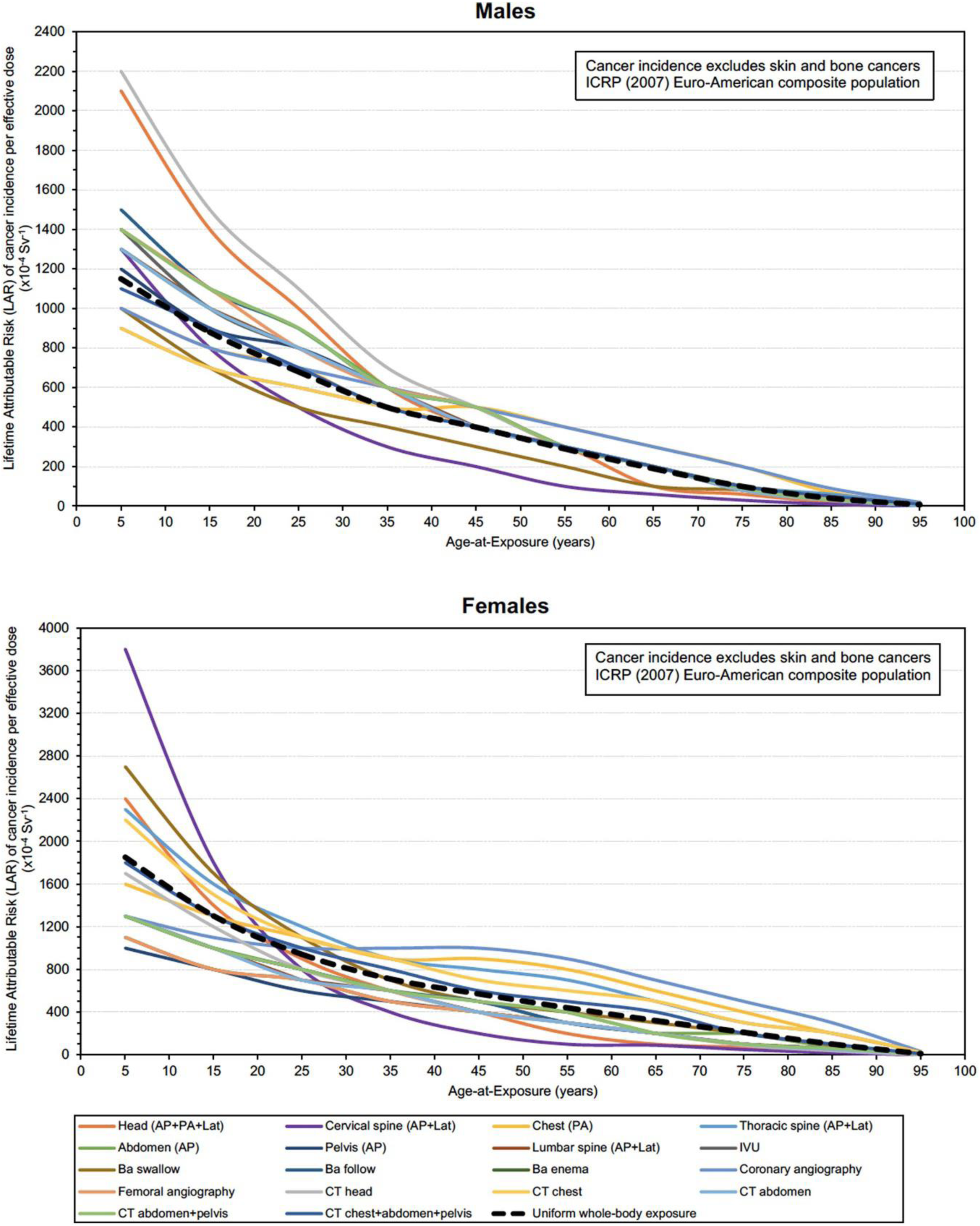
LAR of cancer incidence per effective dose (×10−4 Sv−1) for the ICRP (2007) Euro-American composite population as a function of sex and age-at-exposure for a range of 18 x-ray examinations and for uniform whole-body exposure to gamma radiation, after ICRP Publication 147 (ICRP, 2021), Tables 2.5 and 5.4. Note that the envelope of curves shows the maximum variation in the LAR of cancer incidence resulting from the various combinations of organ/tissue absorbed doses for these different procedures and the application of organ/tissue-specific ICRP (2007) risk models. The black dashed line shows the LAR of cancer incidence corresponding to a uniform whole-body gamma dose of 10 mGy (an effective dose of 10 mSv). Cancer incidence excludes skin and bone cancers (see text). PA, posteroanterior; AP, anteroposterior; Lat, lateral; IVU, intravenous urogram; Ba, barium; CT, computed tomography. Adapted from ICRP Publication 147 (ICRP, 2021), Tables 2.5 and 5.4.
In this way, the range of LAR/Sv estimates for age-at-exposure and sex can be determined, and it is shown that the different distributions of organ/tissue doses for the various x-ray examinations, together with the organ/tissue-specific risk models with sex and age-at-exposure modifications, lead to an envelope of curves that is driven by different procedures at various ages-at-exposure and each sex (Fig. 4).
In Fig. 4, the range of LAR/Sv values for the variety of x-ray examinations considered is generally within ±50% of the LAR/Sv for a uniform whole-body exposure of gamma radiation for the same sex and age-at-exposure, although in a few extreme instances this becomes ±100%.
As would be expected, and as illustrated in Fig. 5, the pattern of variation of LAR/Sv for the 18 types of x-ray examination by sex and age-at-exposure for the Asian composite population is similar to that for the Euro-American composite population. In Fig. 5, rather than presenting the LAR/Sv curves separately for each of the 18 x-ray examinations, the variation of the LAR/Sv by type of diagnostic procedure is shown as an envelope of values bounded by the maximum and minimum LAR/Sv values for the 18 types of examination by age-at-exposure for each sex.
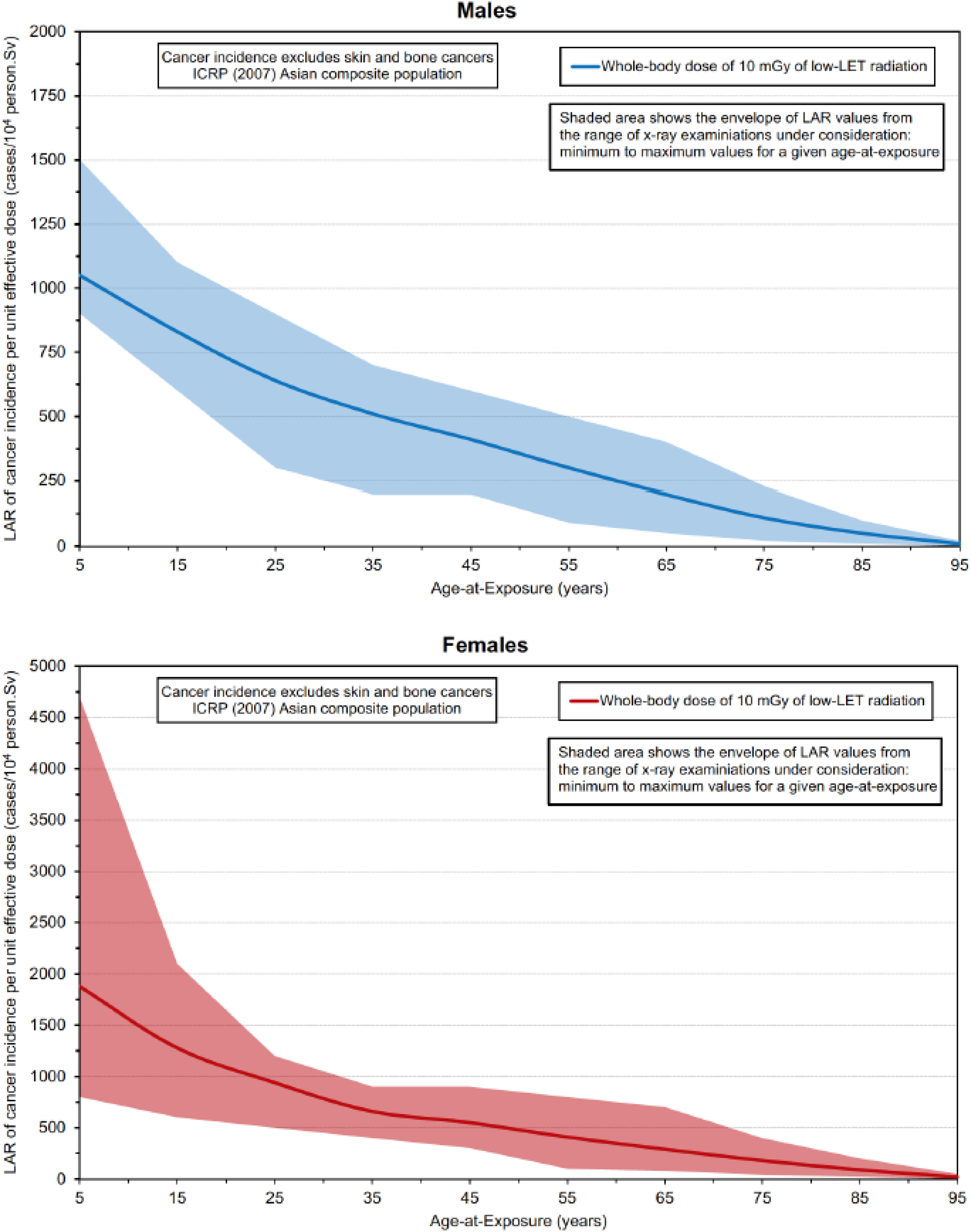
LAR of cancer incidence per effective dose (×10−4 Sv−1) for the ICRP (2007) Asian composite population as a function of sex and age-at-exposure for a range of 18 x-ray examinations and for uniform whole-body exposure to gamma radiation, after ICRP Publication 147 (ICRP, 2021), Tables 2.5 and 5.4. The solid lines show the LAR of cancer incidence corresponding to a uniform whole-body gamma dose of 10 mGy (an effective dose of 10 mSv). The shaded areas show the envelope of curves obtained from the different procedures and indicate the greatest deviation in the LAR of cancer incidence resulting from the various combinations of organ/tissue absorbed doses for these examinations from the LAR obtained from uniform whole-body gamma radiation exposure for each sex at different ages-at-exposure. Organ/tissue-specific risk models are those derived by ICRP (2007). Cancer incidence excludes skin and bone cancers (see text).
In Fig. 5, for males, the LAR/Sv values for the 18 x-ray examinations are within ±50% of the equivalent LAR/Sv values for uniform whole-body exposure to gamma radiation, while for females, there is a single high ERR/Sv value (for a cervical spine (AP + Lat) examination of a 5-year old) that is >100% in excess of the equivalent LAR/Sv for a uniform whole-body gamma ray exposure.
Severity weighting
Having derived 14 nominal risk coefficients, ICRP (2007) weights each of these by severity factors to reflect the impact on health of each of the 13 types of cancer and one category of hereditary disease. For the 11 types of cancer considered in detail in this article, severity weighting reduces the aggregated nominal risk coefficient of 688 × 10−4 Gy−1 to an aggregated detriment of 540 × 10−4 Sv−1, a 22% reduction. In contrast, for all 14 stochastic health effects, the nominal risk coefficient of 1715 × 10−4 Gy−1 reduces to 574 × 10−4 Sv−1, a 67% reduction. It will be noted that the inclusion of the three stochastic effects not considered in detail in this article increases the aggregated nominal risk coefficient by 149%, but the detriment by only 6%. This will be explored in the following subsection.
Skin and bone cancers and hereditary effects
The predominant reason for the 149% increase of the aggregated nominal risk coefficient from 688 × 10 to 1715 × 10−4 Gy−1 when the additional three stochastic effects are included is the nominal risk coefficient for skin cancer of 1000 × 10−4 Gy−1. However, the relatively small increase (6%) in the detriment of the inclusion of the additional three stochastic effects is also due to skin cancer because this is non-melanoma skin cancer, which is comparatively easily treated and so has a very low associated severity in the weighting scheme. Weighting for severity reduces the nominal risk coefficient of 1000 × 10−4 Gy−1 for skin cancer to a detriment of 4 × 10−4 Sv−1. Bone cancer and hereditary effects have comparatively small nominal risk coefficients of 7 × 10 and 20 × 10−4 Gy−1, respectively, and these values are little affected by severity weighting.
In summary, in terms of health detriment, the omission of skin and bone cancers and hereditary effects from explicit consideration in the calculations reported in this article has little impact on the conclusions of the analysis reported.
Calculating risks for individual patients
Should circumstances require the detailed calculation of risks following a particular exposure of a particular individual, the most appropriate organ/tissue-specific risk models (which may not be the models derived by ICRP (2007) for the 2007 Recommendations) may be used in conjunction with the best estimates of organ/tissue doses (if necessary, appropriate RBE values may be used if different types of radiation are involved). In such circumstances, organ/tissue doses may be calculated using anatomical models adjusted to the size and weight of a particular individual; phantom libraries are now available to facilitate such calculations (ICRP, 2020a,b). The overall LAR is the sum of the component LAR values, but these component LARs may not be confined to those obtained using the process adopted by ICRP (2007), since other approaches to cancer risk modelling are available, and may be judged to be more appropriate for the particular circumstances under consideration. However, this level of detail will not be necessary for most occasions when a routine diagnostic procedure is undertaken, so what may be done for everyday x-ray examinations if some sort of measure of risk is thought desirable?
What the analysis of this article has demonstrated is that an estimate of the effective dose associated with an x-ray examination may be used with categories of sex, age-at-exposure, and (in broad terms) composite population to give a reasonable indication of the risk to health from the exposure.
For an aggregated detriment for a population of all ages of 574 × 10−4 Sv−1, which can be taken as the nominal risk of a serious (life-threatening or life-changing) disease developing as a result of a low-level exposure, a factor of 2–3 enhancement for a young boy and 3–4 for a young girl might be in order, depending on the nature of the investigation. These factors will reduce to 1 (±50%, i.e. no or little need for any enhancement) for men in their mid-20s and women in their mid-30s and will continue to reduce with increasing age-at-exposure until a factor of 0.5 is reached for men in their early-50s and women in their early-60s, and so on. Whether anything more than this is required on a routine basis is unclear—the simplicity of such factors applied to everyday situations has to be weighed against the increased complexity of doing anything more detailed. Indeed, given the substantial, and recognised, uncertainties associated with estimates of risk at low doses and low dose rates, greater precision may be spurious and hence misleading.
Other issues
Modifications to the risk of radiation-related cancer are taken to be sex, age-at-exposure, and composite population. However, other risk factors (such as smoking) will likely modify the risk from radiation exposure (perhaps substantially), and such factors have not been accounted for in the risk modelling. Indeed, ICRP (2007) adopts a transport of risk between populations that for most cancers assumes that the background risk of cancer influences the risk from radiation exposure, i.e. there is a component of ERR in the transport of risk for most types of cancer. However, such an assumption is made at the population, not individual, level in the absence of a detailed knowledge of how radiation might interact with these other (largely unknown) risk factors, and for most cancer types, a ‘default’ ERR:EAR of 50:50 is assumed. Therefore, how the background risk of cancer influences the risk of radiation exposure for an individual is largely unclear, except for those with rare genetic conditions known to substantially influence the risk of radiation exposure.
Then there is the matter of how the issues explored in this article have broader ramifications. This article has concentrated on medical diagnostic exposures, but how these issues affect environmental and occupational exposures needs to be considered. For example, questions may arise as to whether certain tasks should be assigned to older male workers rather than younger female workers. These and similar matters arising out of the investigations of this article need to be taken into account.
CONCLUDING REMARKS
An impression is gained from observing the everyday workings of the system of radiological protection that effective dose is being used in a way that was not intended by ICRP (2007) in its 2007 Recommendations, particularly with respect to medical exposures of patients. In particular, the effective dose is being used to calculate stochastic risks arising from specific exposure circumstances by applying the aggregated nominal risk coefficient or aggregated detriment to an effective dose estimate. This procedure ignores recognised differences in risk coefficients between males and females and generally higher lifetime EAR values at younger ages-at-exposure and will underestimate such risks for young children. However, for each sex and category of age-at-exposure (and, to a limited extent, population group as it corresponds to an ICRP composite population), enhancement factors can be derived that may be broadly applied to the nominal risk coefficient or detriment to indicate risk associated with a particular exposure of a particular individual. The accuracy of this process should not be exaggerated, but whether anything further is required for routine exposure circumstances is debatable.