
Abstract
Exposure settings should vary with patients to have an acceptable quality image with an appropriate patient dose. To manage medical exposure from computed tomography (CT), the size-specific dose estimates (SSDE) have been recommended to replace the volume computed tomography dose index because it considers patient size. However, organ dose is deemed more appropriate in the radiation protection field due to its correlation with radiation risk. In this presentation, the difference in medical radiation exposure in CT based on age and body mass index (BMI) by using the web-based CT dose calculator WAZA-ARIv2 and dosimetry system of radiophotoluminescence dosimeters (RGDs) and anthropomorphic phantoms will be introduced. In addition, the feasibility of BMI-based and age-based correction methods for organ dose estimation will also be investigated. For both BMI-based and age-based correction methods, the SSDE-associated correction factors showed consistency with the experimental results. Implementation of the SSDE-associated correction factors to the CT dosimetry systems is feasible, and organ dose estimation accuracy can be improved by applying these two correction methods.
INTRODUCTION
The awareness of risk from radiation causes people to be concerned about the effect of additional radiation received through medical imaging procedures. An indicator of risk from imaging procedures for the individual person is favourable while the current radiation protection system is mainly approached from a population average. Therefore, the International Commission on Radiological Protection (ICRP) Task Group 128 aims to clarify the situation and the approach of radiation protection for individualisation and stratification, including in the field of medical exposure.
Medical exposure is the largest source of radiation exposure in populations other than natural radiation (UNSCEAR, 2022). Medical exposure in developed countries is significantly higher than the worldwide average because of their adequate medical equipment and long-life expectancy. Nevertheless, the implementation of dose reference levels and the improvement of medical equipment help decrease medical exposure. For example, the annual effective dose per caput from medical exposure is 2.6 mSv in Japan which has decreased by 30% compared to 2011[Environmental Radiation in Daily Life (Estimation of the National Doses) ver. 3, 2020].
The variations in risk to different organs lead to the necessity of evaluating organ doses for the individual patient. However, currently implemented computed tomography (CT) dosimetry matrices, such as the CT dose index (CTDI), dose–length product (DLP), and size-specific dose estimates (SSDE), only provide dose information related to the scan condition and whole body. Moore et al. (2014) investigated the correlation of the geometric-based SSDEs with organ doses and developed a simple methodology for estimating patient organ doses in a paediatric population. They found that the average agreement between the SSDE and the absolute organ dose was within ±10% for organs fully covered by the scan volume. However, the organ dose for partially irradiated organs and tissues had a poor correlation with SSDE, resulting in the underestimation of organ doses.
This proceeding briefly reviews the current situation of medical exposure from CT, CT dosimetry matrices, and calculation-based CT dosimetry. Then, differences in medical radiation exposure in CT based on age and body mass index (BMI) are determined using the web-based CT dose calculator WAZA-ARIv2, radiophotoluminescence dosimeters (RGDs), and anthropomorphic phantoms.
CALCULATION-BASED CT DOSIMETRY
Monte Carlo (MC)–based methods are substantially used to estimate patient dose from CT examinations. Estimating organ doses via MC methods requires (1) a model of the x-ray source, including energy spectra and filtration, and (2) patients’ anatomy information, a description of the scan parameters, and the mechanism used to transport photons through the geometry and tally dose to the organs of interest. However, the development of such models is time-consuming.
WAZA-ARIv2 is a free web-based CT dose calculator (Takahashi et al., 2011; Kamei et al., 2015). It contains an organ dose data set assessed by the Monte Carlo code Particle and Heavy Ion Transport Code System (PHITS) and adult and child voxel phantoms. The adult voxel phantoms were developed by the Japan Atomic Energy Agency based on the average Japanese (Sato et al., 2007), and the child phantoms were developed by the University of Florida (Lee et al., 2010). WAZA-ARIv2 also provides organ dose data sets for adults with body shapes classified as obese (+5 SD), fat (+2 SD), and thin (−2 SD) in addition to the standard body shape. Fig. 1 shows a comparison of organ doses calculated using WAZA-ARIv2 between different body shapes under the same irradiation conditions. The absorbed dose for each organ varied with the body shape under the same irradiation conditions. This indicated the necessity of considering body shape when calculating organ doses. In 2021, the BMI-based organ dose calculation function was released in WAZA-ARIv2.

Comparison of organ dose between different body shapes.
In addition to organ dose calculation, WAZA-ARIv2 enables calculation result registration; users can compare the dose level from their institutions and the dose levels of the registered data in WAZA-ARIv2 and use the comparison result to optimise CT scanning conditions in a manner that prevents overexposure (QST, 2019).
This proceeding discusses the individual differences in CT exposure based on age and BMI. Previous studies suggest that organ doses between different ages and BMIs (similar to the SSDE, a size-corrected CTDIvol) can be corrected using a function of the effective diameter of the human body (Boone et al., 2011; O’Neill et al., 2018). These two correction methods (age- and BMI-based correction) were evaluated in this work using RGDs and the anthropomorphic phantom (ATOM series, CIRS, Inc., USA) and the MC-based dose calculator WAZA-ARIv2 (Chang and Koba, 2021). The RGD dosimetry system used in this study was the Dose Ace GD-300 series (Asahi Techno Glass, Japan). All experimental measurements in this work were performed using the SOMATOM Definition Flash (Siemens AG, Florsheim, Germany), and the scanning range covered the neck to the pelvic bone. To reflect the real situation, the results by WAZA-ARIv2 were corrected using the actual CTDIair values obtained using a diode electrometer (Piranha 657, RTI Electronics, Sweden).
Age-based individual difference
Given the relationship between the effective diameter Φeff and patient age derived by the AAPM as follows:

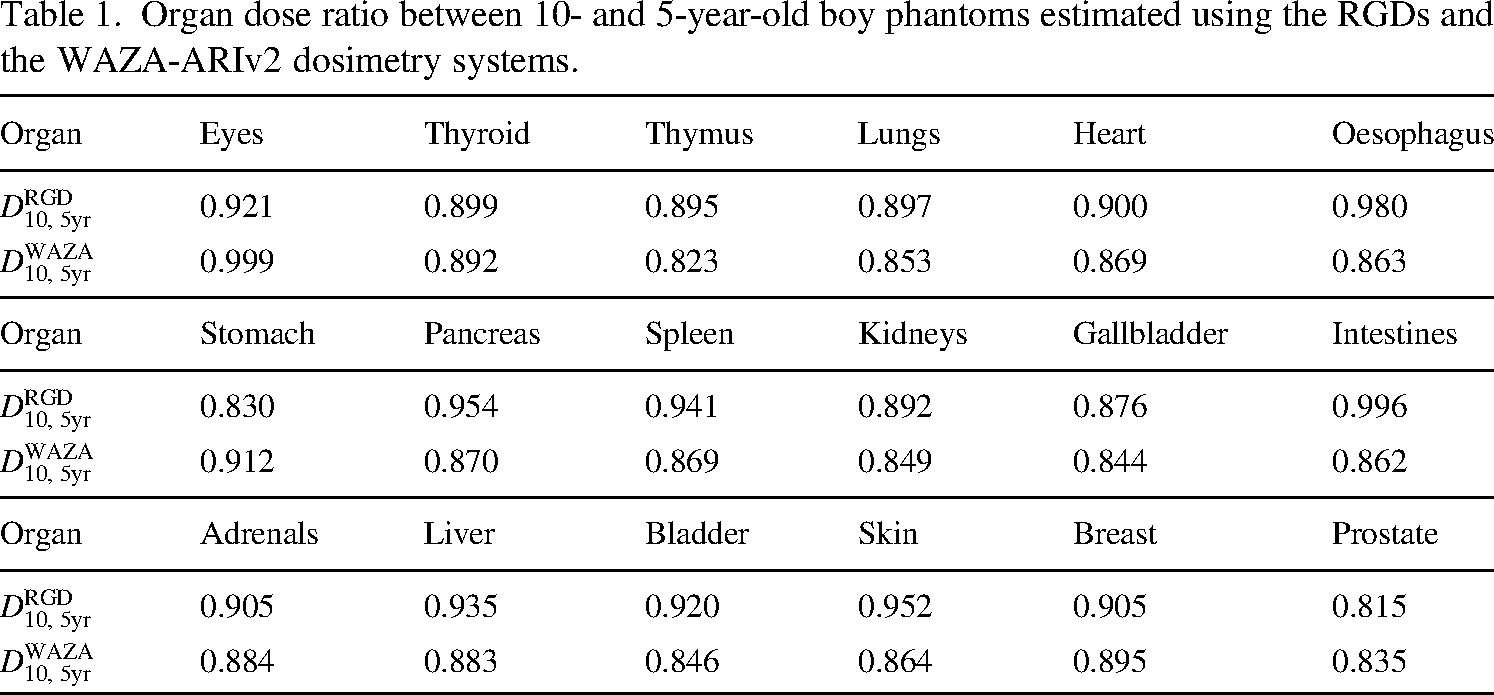
Table 1 shows the organ dose ratio between 10- and 5-year-old boy phantoms obtained using the RGD dosimetry system
Organ dose ratio between 10- and 5-year-old boy phantoms estimated using the RGDs and the WAZA-ARIv2 dosimetry systems.
According to O’Neill et al. (2018), Φeff can be estimated using the following equation:
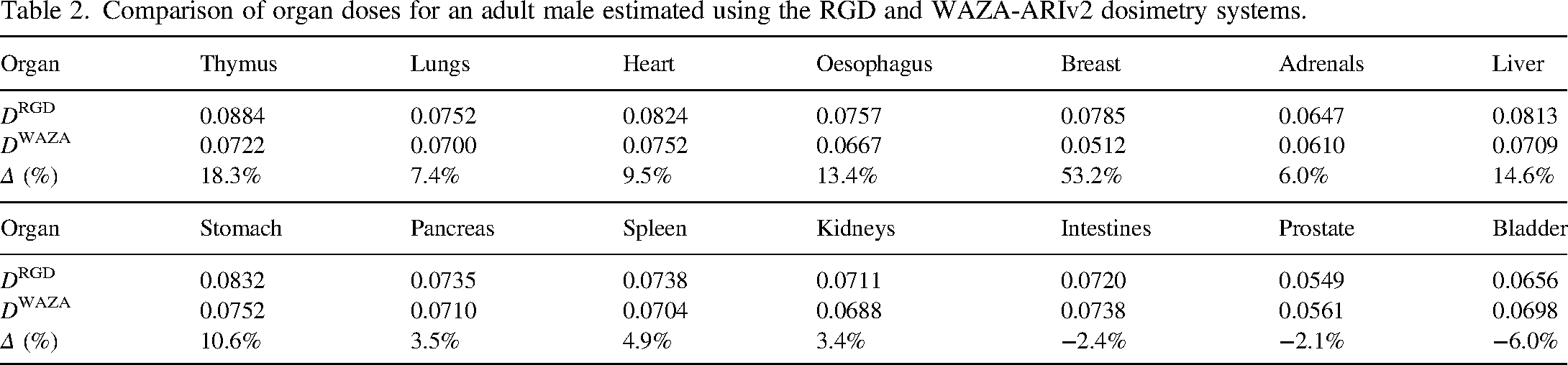
Table 2 shows a comparison of the organ doses for an adult male (BMI = 24.4) estimated using the RGD and WAZA-ARIv2 dosimetry systems. The dose differences Δ for most organs were less than 10%. This indicated that the BMI-based correction method could improve the accuracy of organ dose estimated using WAZA-ARIv2. However, the Δ for some organs, such as the thymus and breast, exceeded 10%. These organs were similar in location: the peripheral region of the human body. In fact, Δ increased with the distance between the organ centre and the central axis of the body. The RGDs used in this study have a high energy response in low-kilovoltage x-rays. Using the μen:ρ ratio corresponding to the energy in the centre axis region may overestimate doses to organs in the peripheral region. This explains the phenomenon observed in our results: The calculated breast dose was smaller than the measured breast dose.
Comparison of organ doses for an adult male estimated using the RGD and WAZA-ARIv2 dosimetry systems.
This proceeding provides an overview of the current situation of medical exposure from CT and the CT-related dosimetric matrices. The feasibility of age- and BMI-based correction methods was investigated using the RGD and WAZA-ARIv2 dosimetry systems. The accuracy of organ dose estimation can be improved by applying these correction methods.