
Abstract
Although the Fukushima nuclear accident released a very large number of radionuclides, it is not known exactly how much the people of Fukushima Prefecture were exposed to. Since there are almost no actual measurements of exposure doses, we have to rely on the exposure doses estimated by the UNSCEAR 2020/2021 report. The report concluded that ‘exposure doses at Fukushima are considered to have been very low’, and in response, the Japanese government stated that ‘the effect of exposure on childhood thyroid cancer that occurred at Fukushima is unlikely’. However, as far as I have been able to find out, there are more than 100 problems with that report regarding estimates of thyroid exposure alone, which can be largely summarised in six underestimates.
SUMMARY OF UNDERESTIMATIONS
Thyroid iodine uptake rate was halved
In the UNSCEAR report, the sentence ‘The thyroid equivalent dose coefficient for iodine was set at 1/2 because Japanese people traditionally have a diet rich in iodine and their iodine intake is about two digits higher than the world average’ appears several times. However, in the iodine nutritional status in countries around the world in 2019, iodine intake in Japanese schoolchildren proved to be within the adequate range and not excessive (Iodine Global Network, 2019).
The indoor evacuation effect was halved
According to the report, ‘The reduction factors for dose exposure by inhalation for residents who were indoors during the passage of the plume as reported by Hirouchi et al. ranged from less than 0.1 to about 1 (Hirouchi et al., 2018). Therefore, the Committee used a reduction factor of 0.5 for the assessment of dose owing to inhalation while residents were indoors’, but the rationale for using 0.5 is not stated. In Hirouchi et al.'s experiment, the plume transit time was assumed to be 1 h, and the air concentration in the plume was assumed to be 1.0 Bq m−3, all particulate, which would lead to a large underestimation of the actual long-term high concentration plume.
According to Prof. Hiromi Yamazawa of Nagoya University, when a plume exists for 1 h, the cumulative concentration indoors is reported to be the same as outdoors in a few hours to half a day, regardless of the ventilation rate, when the plume remains closed after its passage (Yamazawa, 2019).
Ignored oral exposure of evacuees
The article by Hirakawa et al. (2017) adopted by the report, which examined only typical evacuation centres operated and managed by local governments, concluded that ‘iodine-131 contaminated food and supplies were generally not consumed in large quantities even before the food restriction order’. In fact, there have been reports of cases where contaminated food was ingested and distributed immediately after the accident. For example, after March 12, when residents of the town of Namie evacuated to Tsushima, they ate at a soup kitchen of local vegetables at their evacuation site (https://www.asahi.com/articles/DA3S14471890.html).
Three households drank milk that had been discarded for 10 days after the accident (https://togetter.com/li/677668).
Raw milk from Kawamata Town on March 16–17 was processed into yogurt and shipped within the prefecture (https://www.mhlw.go.jp/stf/houdou/2r98520000015iif.html).
The report also states that the estimates made from measurements made by the shaded meal method survey reflect only the intake of radioactive caesium (since radioactive iodine was no longer measurable by the time the survey began), ignoring the most important effect of radioactive iodine.
Furthermore, the report states that ‘the estimated doses for Fukushima City are considered to be representative of the doses to residents of Fukushima Prefecture as a whole due to oral intake of food and drinking water’. However, for example, differences of more than one order of magnitude have been observed in air dose rates and soil radioactivity between Fukushima City and Namie Town.
Inhalation exposure estimates are highly uncertain
The UNSCEAR report itself emphasizes the uncertainty of the inhalation estimates, stating that ‘such estimates are subject to considerable uncertainty at any particular location’ and that ‘the ATDM (Atmospheric transport, diffusion and deposition model calculations) direct method significantly underestimated concentrations in the central and western parts of Fukushima Prefecture, sometimes by many orders of magnitude’, and so on.
Professor Emeritus Shinichi Kurokawa states, ‘The ATDM in the Terada paper adopted by the report does not capture the first plume that hit the center of Fukushima City on March 15–16 and underestimates the atmospheric concentration of iodine-131 by a factor of 100’ (Terada et al., 2020; Kurokawa, 2022).
Average estimates do not consider individual exposure at all
The UNSCEAR report fits evacuees into roughly 40 different scenarios, each with an average estimate, but the average estimate does not take into account individual exposure at all.
Fig. 1 shows a histogram of the distribution of thyroid exposure and the number of people in 1 of the 40 scenarios, Scenario 29. It can be found in the attachment to the report. From this graph, the maximum value can be read as 700 mGy.
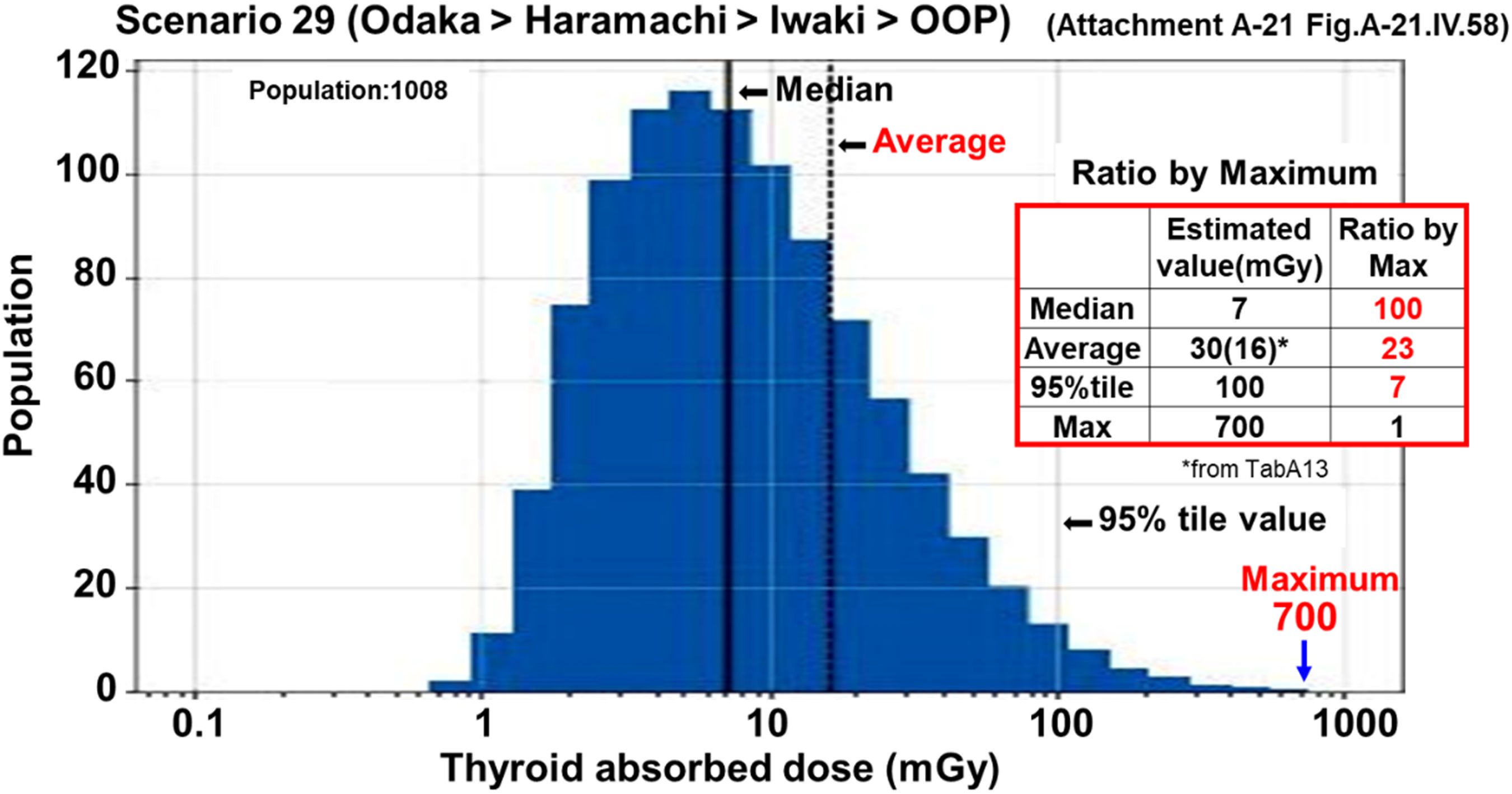
A histogram of the distribution of thyroid exposure and the number of people in 1 of the 40 scenarios, Scenario 29.
As shown in the table on the right of the graph, the maximum value is 100 times the median value, 23 times the mean value, and 7 times the 95% tile value, and it must be considered that even if the median and mean values are low, there is a very high maximum value. This is an extremely serious problem that neglects the health effects on the affected population.
Direct thyroid measurements were performed on 1080 people under the age of 15, but a number of problems have been identified that lead to underestimation.
Problems with the measurement points
It is reported that Kawamata Town, Iitate Village, and Iwaki City were selected for measurement because the area outside the 30-km radius where evacuation and shelter evacuation orders have not been issued was judged to be ‘the area with the highest radiation dose’ and was estimated to be around 100 mSv based on SPEEDI and monitoring data. However, in the contamination screening of evacuees within a 20-km radius, more than 901 people were measured between 13,000 and 100,000 cpm (many people were not recorded), and 102 people were recorded at 100,000 cpm or higher, which is equivalent to 100 mSv for a 1-year-old child at 13,000 and 100,000 cpm at 769 mSv (Sakakibara, 2021). This suggests that the evacuees were exposed to far more radiation than these 1080 non-evacuees.
Problems with the measurement method
There are several problems with the measurement method: the nuclides were not identified because a simple measuring device was used, the measurement started too late (iodine with a short half-life, which has a strong impact, was hardly measured), and the number of measurements was too small (more than 300,000 people were measured in Chernobyl). Furthermore, and more importantly, the measurements around the neck were taken with decontamination, and the measurements of the clothing around the shoulders were taken as background without decontamination. As a result, the net value obtained by subtracting the background from the neck measurement was 0 or negative in more than half of the cases (about 55%). However, with the background value remaining high, the thyroid gland should be considered to have taken in radioactive iodine (Study 2007, 2015).
The UNSCEAR report also reveals its own underestimation when it says, ‘The exposure estimates in the report are in good agreement with the actual measurements of these 1080 people’.
Overly lowered exposure estimates resulted in EAR Gy−1 values 50–100 times higher
As mentioned above, the UNSCEAR 2020/2021 report lowered the exposure estimates as much as possible through a series of underestimations, resulting in the EAR Gy−1 (excess absolute risk Gy−1 coefficient) being at an outrageous value. Kato et al. (2023) compared and analysed graphs obtained from direct thyroid measurements and annual thyroid cancer incidence rates in Chernobyl and graphs obtained from UNSCEAR report estimates and annual thyroid cancer incidence rates in Fukushima. In both cases, there is a dose–response relationship between thyroid exposure (Gy) and annual incidence rate of thyroid cancer, and the slope of the graph for Fukushima is 50 to 100 times higher than that of Chernobyl. Since EAR Gy−1 is generally about the same in different countries, it is natural to interpret this as an underestimation of the UNSCEAR report's estimates as being underestimated by a factor of 50 to 100.
IS ‘FUKUSHIMA AND CHERNOBYL DOSES DIFFER BY MANY ORDERS OF MAGNITUDE’ CORRECT?
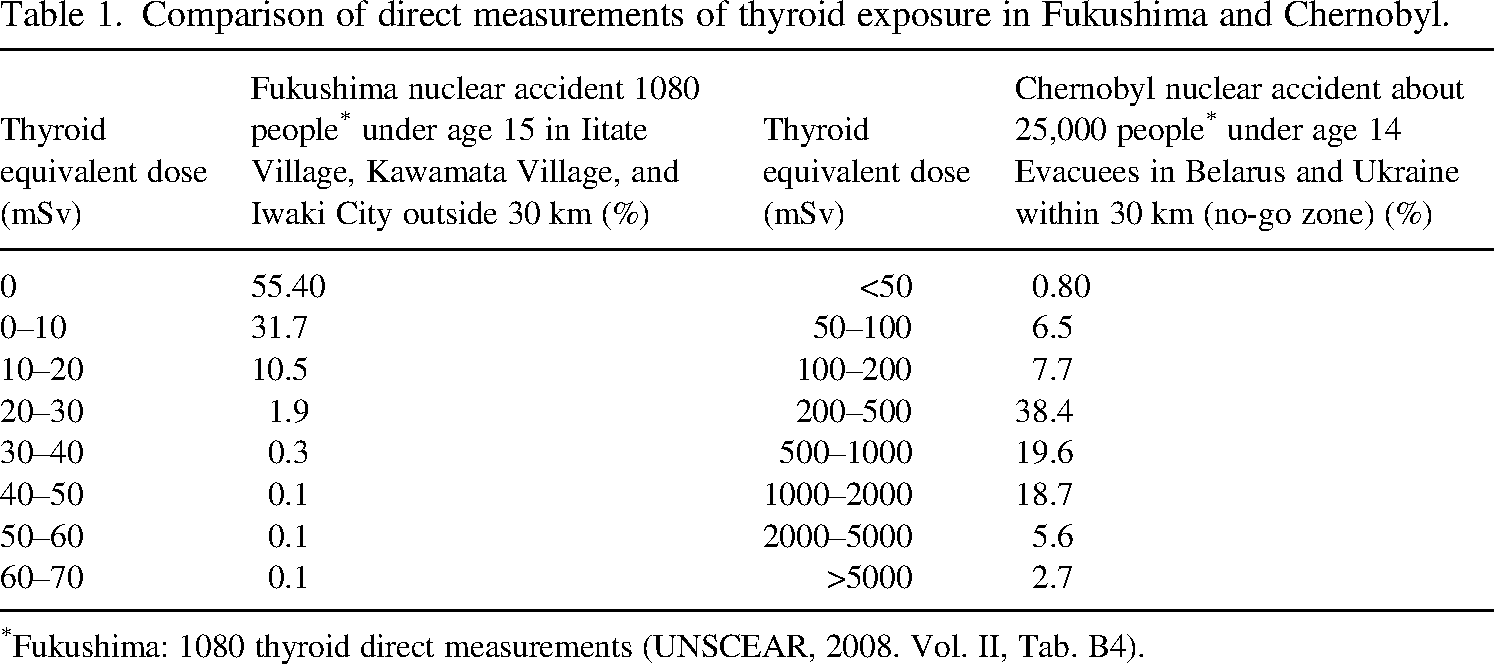
Table 1 is widely used as a decisive factor for the statement, ‘Exposure doses at Fukushima and Chernobyl are many orders of magnitude different’. Although both are measured values, the conditions of people exposed to radiation in Fukushima and Chernobyl are completely different. The table on the left for Fukushima shows inaccurate and inappropriate direct thyroid measurements for 1080 non-evacuees outside the 30-km evacuation zone, with more than half of the measurements being zero or negative and the maximum being 30 mSv, which is an extremely low dose distribution. In contrast, in the case of Chernobyl on the right, the evacuees are within a 30-km radius (no-go zone), so it is not surprising that they are exposed to high doses of radiation.
Comparison of direct measurements of thyroid exposure in Fukushima and Chernobyl.
Comparison of direct measurements of thyroid exposure in Fukushima and Chernobyl.
Fukushima: 1080 thyroid direct measurements (UNSCEAR, 2008. Vol. II, Tab. B4).
It must be said that this is a table that dares to mislead. This table of comparisons is often used in various committees and court cases related to the Fukushima nuclear accident, but it is clearly misleading.
Fig. 2 illustrates the process of transforming Japanese data into an authoritative UNSCEAR report. Japanese data are passed on to the UNSCEAR Japanese working group, and articles that admit radiation exposure effects are rejected, while convenient articles are arbitrarily adopted to produce the UNSCEAR 2020/2021 report. In other words, a thorough conflict of interest has been committed to transform the report into ‘The report of the most prestigious international organisation’.
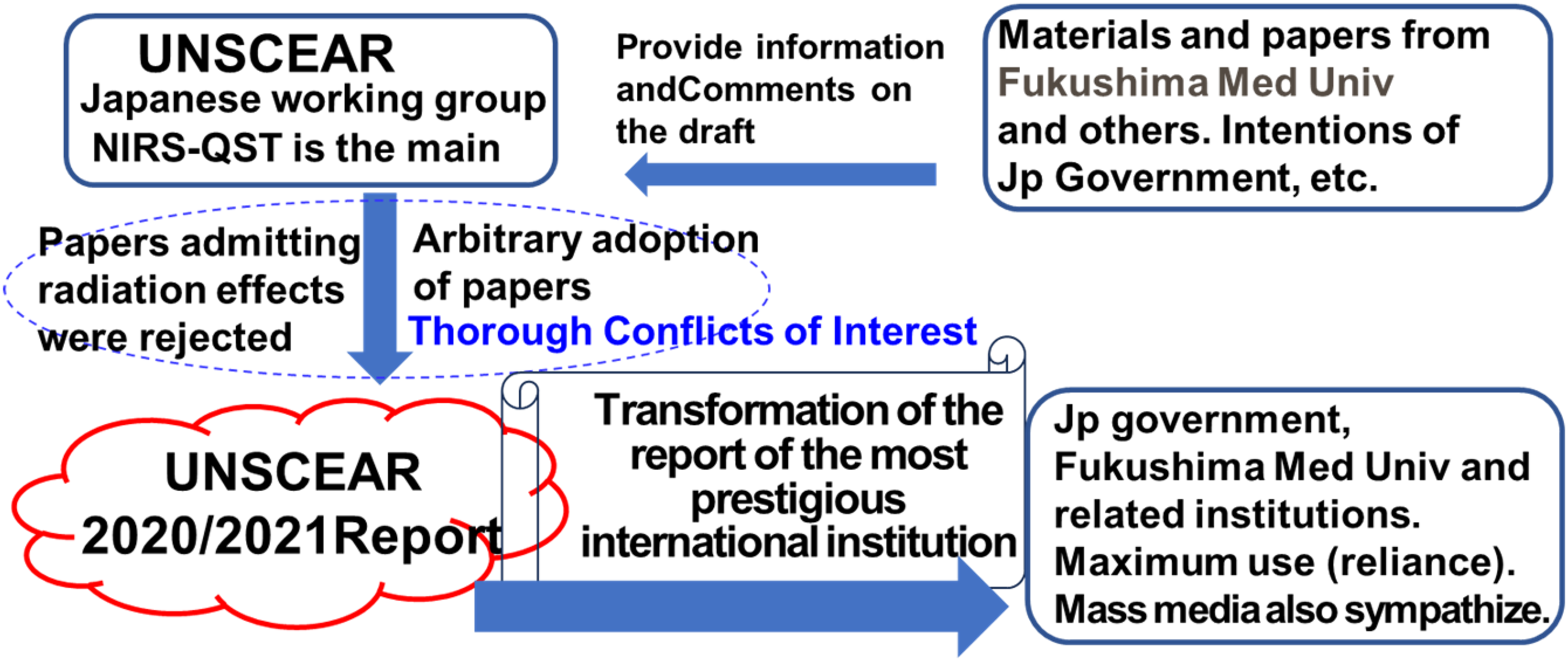
A diagram of the process of transforming Japanese data into an authoritative UNSCEAR report.
The Japanese government, related organisations, Fukushima Medical University, and others are completely relying on this report and making maximum use of it. Most of the mass media also agree. The report concludes that no significant excess of thyroid cancer is expected in the absorbed thyroid doses estimated by this committee.
Since the thyroid exposure estimates in the UNSCEAR report are the most important issue directly related to the thyroid cancer causation theory, we should face too many problems in that report. Furthermore, it should be recognised that as long as we rely on the dose estimates in the UNSCEAR report, it will be difficult to apply the experience of the Fukushima Daiichi nuclear accident to improve radiation protection.
And the best remedy is that the report should be scrapped and a new report prepared by a group of neutral scientists.