
Abstract
Recent reports indicate a new concept of low-dose ionising radiation cataractogenesis. In 2020, a two-stage aetiology of initiation and maturation was proposed by Richardson and colleagues for posterior subcapsular cataract (PSC) and perhaps cortical cataract development. The mechanisms involve various oxidative stress and biochemical factors, some of which are relevant to A-bomb survivors, such as ocular ion imbalance, inflammation, and maybe oxygen level changes. An example of a known, specific cataractogen is hypoparathyroidism and associated hypocalcaemia. However, a recent report indicated calcium overload in situ is also a cataractogen. In fact, Neriishi and colleagues in 2003 reported a preliminary analysis of the serum in A-bomb survivors, finding persistent inflammation and calcium levels that were statistically significant as indirect systemic effects in the dose response of PSC and cortical cataract. Therefore, the above reports linking cataractogenesis to ‘intermediate variables’ and perhaps insulin resistance strongly support the preliminary results in A-bomb survivors. US astronauts display similar excess cataracts and serum-derived biomarkers. Thus, further analyses of updated datasets from A-bomb survivors and astronauts allowing for these intermediate risk factors and retinal/uveal pathologies are required to test these new concepts in ionising radiation cataractogenesis.
INTRODUCTION
It is well-known that systemic diseases such as diabetes mellitus, hypertension, obesity, and disorders of the immune system increase the risk of cataracts. This article outlines various indirect systemic factors and non-lens eye diseases (called intermediate variables or mediators) to better understand ionising radiation cataractogenesis. This is followed by a framework of the analysis required of updated data sets from A-bomb survivors to confirm or otherwise the significance of these new concepts. In addition, reference is made to the similar characteristics observed in space radiation-induced cataracts in astronauts and their biomarkers.
This new line of enquiry was pursued due to five issues identified whose future study can improve upon the current understanding of excess cataracts promoted by ionising radiation. First, reported animal and in vitro experiments studying radiation-induced cataractogenesis have been mostly at high dose (≥1 Gy) and high dose rates (>0.05 Gy/min) for low-density ionizing radiation (Hamada et al., 2019). It is generally accepted that future experimental and non-experimental research will benefit most from the study of low doses (≤0.1 Gy) and low dose rates (<0.1 mGy min−1). Second, the current trend of experimental and theoretical research is moving away from demonstrating that ionising radiation is a cataractogen encompassing all cataract types and instead considering radiation's role in the distinctive aetiology of specific cataract types. Third, the understanding of the role of radiation in the development of specific cataract types can be advanced by considering the aetiology of other cataractogens (and potential confounding factors) such as diabetes and disruption of calcium homeostasis. Fourth, although the non-vascular whole lens is widely accepted to be the principal ocular target of radiation-induced cataracts, the aetiology of specific cataract types points to the involvement of vascular, extra-lenticular regions such as the uvea and retina. Fifth, the deleterious effects of radiation, especially at moderate (<0.5 Gy) or low doses, do not stand alone but act in combination with oxidative stress and ageing processes, which mature a nascent cataract to cause vision defects.
TWO STAGES: OXIDATIVE STRESS AND OTHER RISK FACTORS
Common senile cataracts are nuclear cataracts, less so cortical cataracts, and less again, PSC (Fig. 1). Astronauts are estimated to receive a chronic dose of ∼1 Sv during a 2-year mission to Mars, which is about four times the mean acute dose to A-bomb survivors (0.27 Gy, limited to doses >0.005 Gy) (Cologne and Preston, 2000). Strongly associated with A-bomb survivors and astronaut studies are PSCs and cortical cataracts and less so nuclear cataracts (Neriishi et al., 2002, 2012; Minamoto et al., 2004; Chylack et al., 2012). A two-stage mechanism, which includes ageing, was proposed for PSCs and likely cortical cataracts (Richardson et al., 2020). Support for a two-stage aetiology for cataracts in A-bomb survivors is demonstrated by late-onset radiation cataracts being preceded by early-onset senile cataracts (Neriishi et al., 2002). Oxidative stress, ionising radiation, and inflammation are risk factors that both initiate and mature cataracts. High-dose radiation can significantly reduce lifespan (≈1 year Gy−1), and hence promote second-stage premature ageing (Richardson, 2009); however, the insignificant ageing associated with moderate- and low-dose exposures may indicate a different form of cataract development.
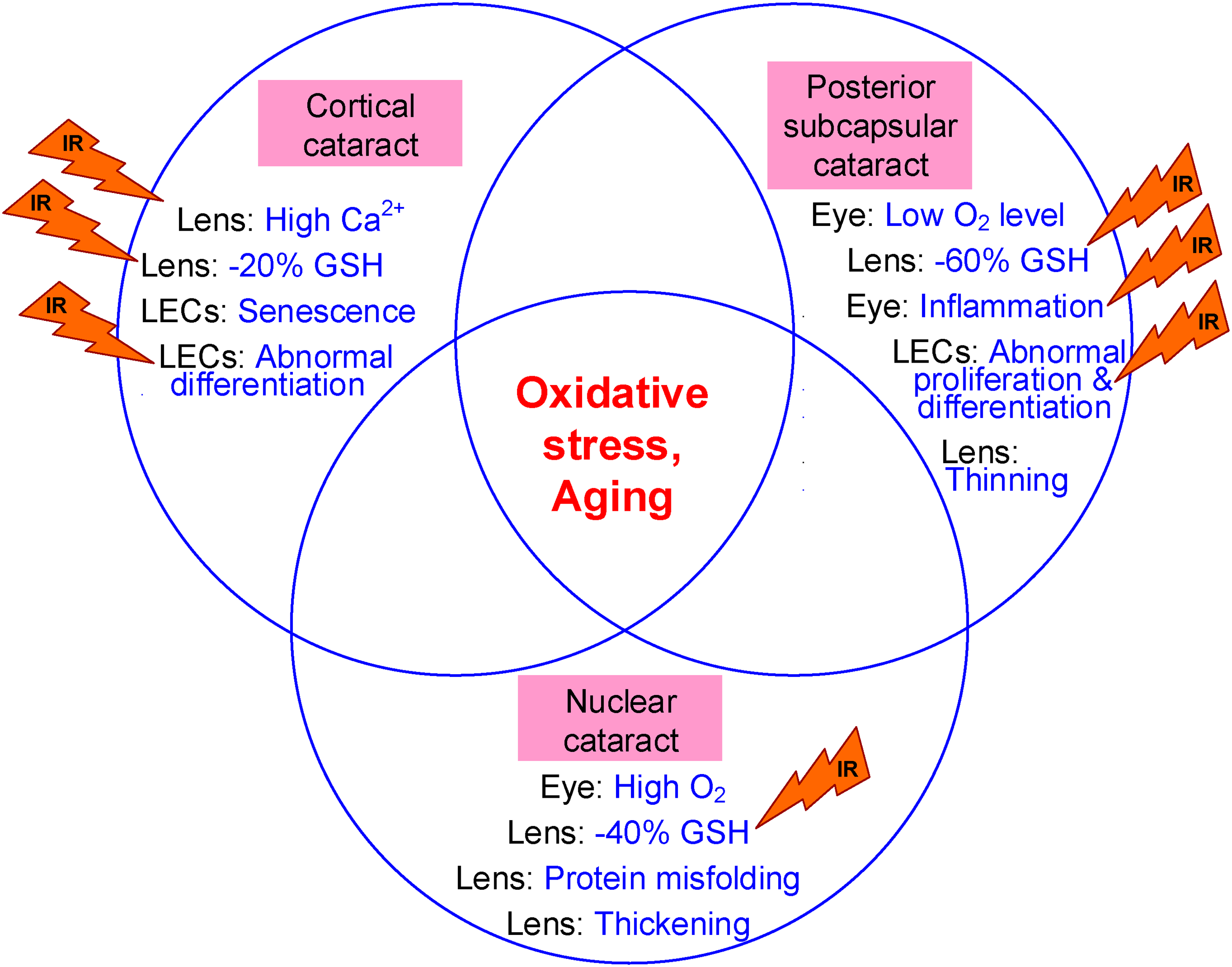
Common characteristics of the three major age-related cataract types and the cataractogenic effects ionising radiation (IR) can modify. Ageing-related changes (not IR ones) are given for the eye, lens, or lens epithelial cells (LEC) and include glutathione (GSH) concentrations, calcium (Ca2+), and oxygen (O2) concentrations (Pau et al., 1990; Beebe et al., 2010).
Oxidative distress, often associated with abnormal oxygen levels, is a dominant detrimental effect of ageing, ionising radiation, and cataract development. Terrestrial and space radiation exposures in general are rarely associated with nuclear cataracts, but when linked to radiation, this cataract type may be due to confounding factors such as the pure oxygen atmospheres of early US spacecraft (Hamada et al., 2019; Richardson, 2022). The lens is the most hypoxic tissue in the body, with 1 mmHg partial pressure of oxygen (∼0.1% O2) in the nucleus and ∼3 mmHg (∼0.4% O2) in lens epithelial cells. The radiosensitivity of all tissues is dependent on the ‘oxygen effect’; hence, hypoxic conditions protect tissues from not only the detrimental effects of radiation but also oxidative stress and premature ageing in general (Fig. 2). Lenticular oxygen levels normally exist in a narrow, hypoxic, ‘Goldilocks’ range. Higher-than-normal oxygen levels in the lens promote nuclear cataracts, while lower oxygen levels have been measured in the eyes of diabetic patients and promote PSC and cortical cataracts (Richardson et al., 2020). Abnormally severe hypoxia can result from arteriolosclerosis due to persistent inflammation inducing blood vessel narrowing. Consequently, non-lens ocular factors associated with lower-than-normal oxygen levels, such as uveitis (ocular inflammation) and retinopathy, are also linked to PSC development.
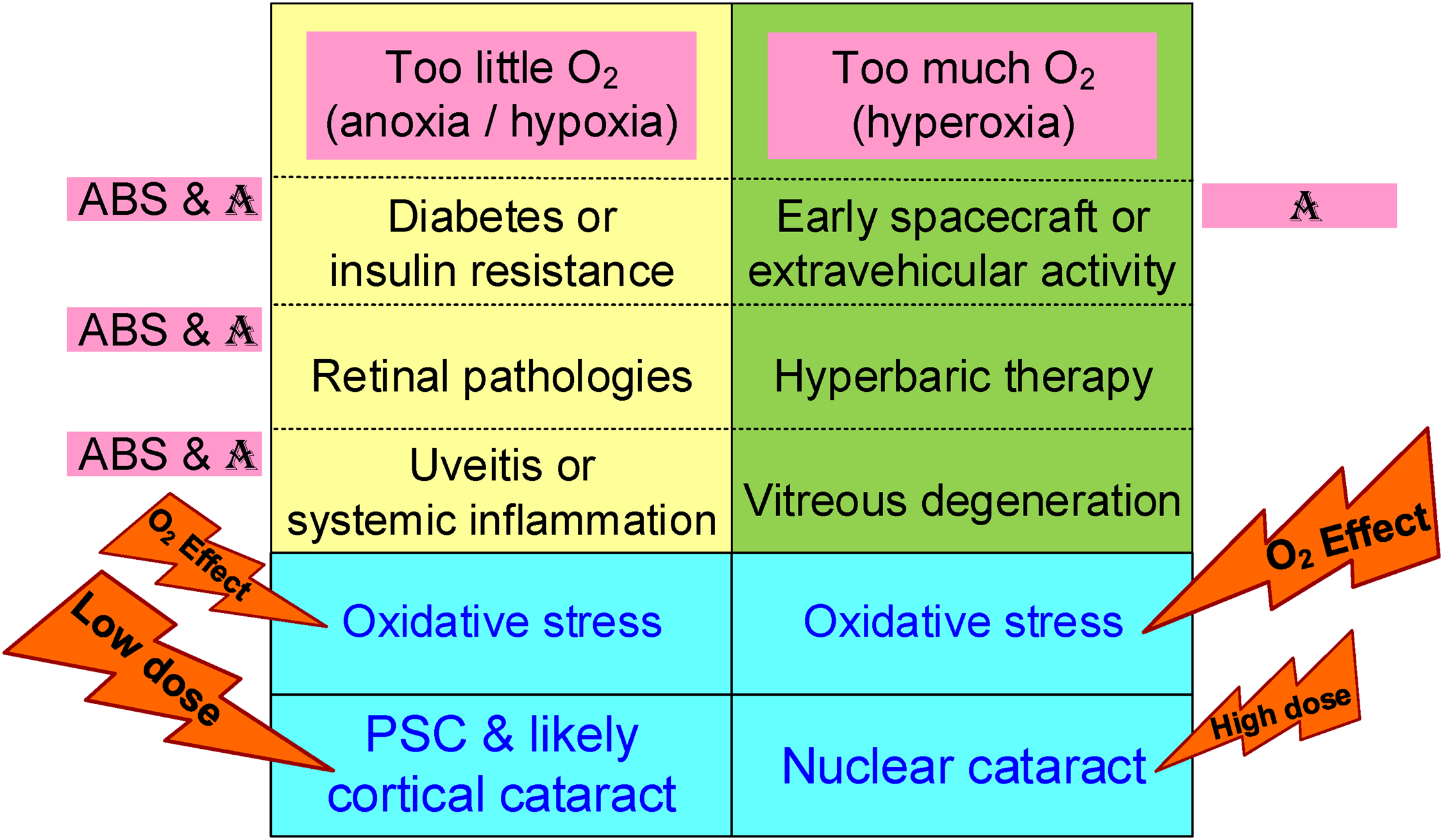
Systemic diseases, eye disorders, and other conditions in A-bomb survivors (ABS) and astronauts (A) related to cataractogenesis and linked to abnormally low and high intraocular oxygen levels (yellow and green cells) outside the normal ‘Goldilocks’ range that result in oxidative stress and cataracts (blue cells).
Other non-lens ocular diseases may also indirectly promote cataracts. Common age-related retinal pathologies such as cataract, glaucoma (the most common form worldwide is primary open-angle glaucoma), diabetic retinopathy, and age-related macular degeneration are accompanied by low-grade, systemic, chronic inflammation (i.e. ‘inflammageing’) and intraocular hypoxia (Grimm and Willmann, 2012). Exposure of the eye to ionising radiation is associated not only with cataracts but also with other ocular diseases such as normal-tension glaucoma and diabetic retinopathy (Hamada et al., 2019). Normal-tension glaucoma was negatively associated with central retinal artery and vein equivalents indicating retinal blood vessel narrowing (Kiuchi et al., 2019). Consequently, there is indirect evidence for eye diseases, including those induced by radiation, altering ocular oxygen levels and promoting cataracts.
We here consider the epidemiological strategies based on the knowledge gained from previous studies of A-bomb survivors. In demonstrating a relationship between ionising radiation dose and cataract promotion, it is important to identify additional potentially significant or confounding factors. Since cataract has multiple risk factors, such as age, sex, city, radiation, inflammation, and calcium, these factors must be accounted for example, a search was conducted for radiation-induced ‘intermediate risk factors’, which cause systemic or ocular changes, which in turn affect the number of lens opacities (Neriishi et al., 2003; Minamoto et al., 2004). Acceleration of age-associated inflammatory biomarkers in blood or plasma samples is one of the most marked health effects in A-bomb survivors (Neriishi et al., 2001; Hayashi et al., 2008). The proportion of the naïve T cells of 723 survivors decreased with age and radiation dose and is an indirect systemic effect, as immune impairment can lead to persistent inflammation (Kusunoki et al., 2002). A preliminary, multiple regression analysis of A-bomb survivors’ data reported that serum calcium and persistent subclinical inflammation were statistically significant in dose responses for PSCs and cortical cataracts (Neriishi et al., 2003).
Hypoparathyroidism and hypocalcaemia are well-known risks for cataract (Richardson et al., 2020), but cataractogenesis may possibly result from calcium disruption in general. Calcium overload and consequent Ca2+-induced proteolysis in vivo and in vitro have been hypothesised as cataractogens, especially of cortical cataracts (Rhodes and Sanderson, 2009). A significant positive dose response was observed for levels of serum calcium (P < 0.001), parathyroid hormone (PTH, P < 0.010), and calcitonin (P < 0.027) from 1459 subjects in Hiroshima and Nagasaki, even after patients with hyperparathyroidism were excluded (Fujiwara et al., 1994). Calcium and calcitonin showed linear dose dependency; similarly, there is a linear increase in PTH at lower doses, levelling off at higher doses.
The incidence of insulin resistance and diabetes are additional cataractogenic factor warranting consideration in view of both PSC and cortical cataracts being associated with both age and ionising radiation (Neriishi et al., 2012; Richardson et al., 2020). Among A-bomb survivors, a significant dose response was observed for the 1417 incidence diabetes cases, but only for Hiroshima and not Nagasaki (Tatsukawa et al., 2022). These inconsistent results could indicate potential confounding of the radiation association with diabetes. Similar to younger diabetes patients, younger survivors at the time of the bombing had a higher hazard ratio for cataracts than those older. Insulin resistance is not only a confounding factor for cataracts in A-bomb survivors but also in US astronauts (Basirun et al., 2021).
Ophthalmologic examinations of A-bomb survivors identified these cataractogenic risk factors including dose effects for diabetic retinopathy and retinal arteriolosclerosis (Fig. 2) (Minamoto et al., 2004). In addition, clinical laboratory blood tests indicated alpha-1 globulin (an indicator of inflammation) was associated with cortical opacities, and white blood cell count, haemoglobin A1C (i.e. glycated haemoglobin, indicating diabetes risk), and serum calcium values were linked to PSC. Inclusion of the significant intermediate risk factors into the analysis did not change the significance of the dose–response relationships of A-bomb survivors but did change the odds ratios of cortical and posterior subcapsular opacities to 1.34 (17% change) and 1.36 (12% change), respectively. In the case of calcium, as shown in Fig. 3, to assess the radiation dose response of cataract alone, it is necessary to account for the variation with and without serum calcium.
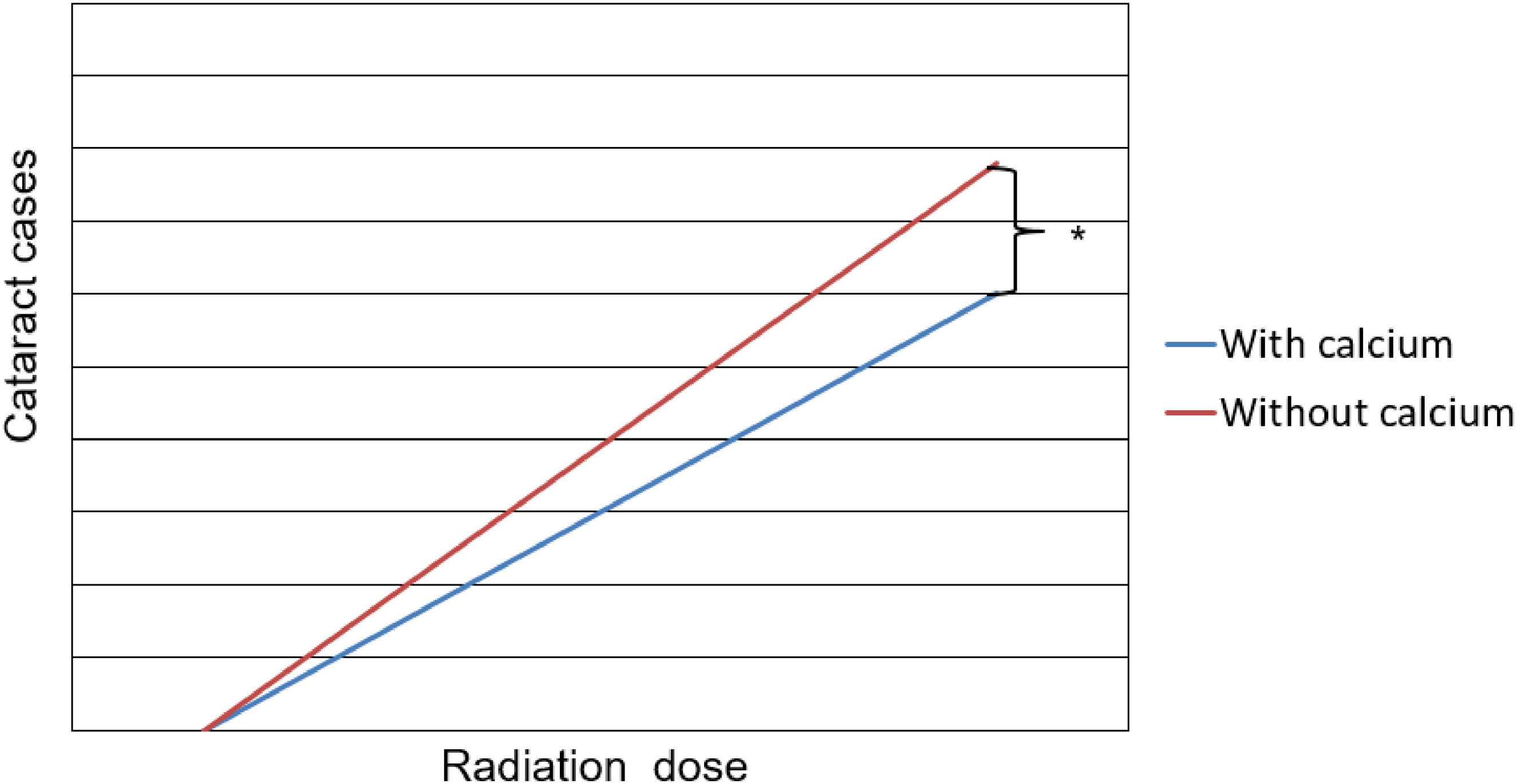
An illustration of how the cortical cataract numbers in A-bomb survivors vary with the radiation dose and how the risk of radiation-induced cataracts is even greater* when removing the calcium variable from the multiple regression analysis (i.e. ‘without calcium’), compared to when included (i.e. ‘with calcium’).
One limitation of a proposed further study of cataracts in A-bomb survivors is that although inference of moderate and even low doses can be made, the nuclear explosion has a high dose rate. Other limitations are non-confirmed factors such as nutritional deficiency and the present age of the A-bomb survivors. The peak age of cataract surgery in Japan is 70 years old or over, which corresponds to postdetonation with the year of 2016 or later. In analyses of previous cataract studies, only the grading of lens opacities was made by ophthalmologists. Data specificity of the cataracts removed or in situ and their type is also important, but is not available. Lenses of study subjects surgically removed during that period did not contribute to the present cataract estimates, resulting in less accuracy in the dose–response relationship of the cataract findings. Instead, inclusion of cataract surgery subjects may better represent the dose–response relationship of cataract in A-bomb survivors even though identification of the types of cataracts is not available. Therefore, any future data analysis has limitations and needs to account for data specificity.
Aberrant systemic inflammation and calcium levels are associated with cataract development; those biomarkers are elevated in A-bomb survivors but also in astronauts exposed to space radiation and microgravity (Basirun et al., 2021). Although a full analysis of indirect effects (systemic and non-lens eye diseases) in A-bomb survivors has not been published, the above preliminary results strongly support non-lens effects in radiation-induced cataractogenesis.
Thus, further analyses with updated data sets from A-bomb survivors are required to test the concept that both intermediate risk factors and confounding risk factors are important in determining the risk of ionising radiation cataractogenesis. If indirect effects are confirmed, cataractogenic risk may need consideration of non-lens, eye tissue doses, such as the dose to the uvea and retina, which can vary considerably compared to the dose to the lens (Ali and Richardson, 2023).
Footnotes
ACKNOWLEDGEMENTS
Dr. Marilyn Vera-Chang of CNL, Chalk River, ON, is thanked for providing helpful comments on this article. RBR has benefited from the library facilities that McGill University makes available to its adjunct professors. The authors declare no conflict of interest.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
This work was supported by Atomic Energy of Canada Limited's Federal Nuclear Science and Technology Work Plan.