
Abstract
Breast cancer remains a significant health concern for women worldwide. Ultrasound imaging is widely adopted for screening due to its non-invasive and radiation-free nature. However, challenges such as low image contrast, blurred tumor boundaries, and diverse tumor morphologies severely hinder accurate segmentation. To address these issues, we propose LKCAU-Net, a novel hybrid multi-scale network that integrates Large Kernel Coordinate Attention (LKCA) and Atrous Spatial Pyramid Pooling (ASPP). The LKCA module enhances the model’s ability to capture spatial details and global contextual information, while the ASPP module enhances multi-scale contextual representation. Embedded within a deep U-Net architecture, these components enable effective global-local feature fusion, significantly improving the robustness and accuracy of breast tumor segmentation in complex ultrasound images. We conducted experiments on four widely used public datasets: BUSI, Dataset B, BUSBRA and QAMEBI. For Dataset B, our proposed LKCAU-Net attained a Dice score of 0.8215, a Jaccard index of 0.7167, a precision of 0.8797, a recall of 0.7937, and a specificity of 0.9949. On the BUSI dataset, it reached a Dice score of 0.7973, Jaccard index of 0.6899, precision of 0.8320, recall of 0.7886, and specificity of 0.9825. When evaluated on the BUSBRA dataset, the model achieved a Dice score of 0.9085, Jaccard index of 0.8402, precision of 0.9206, recall of 0.9057, and specificity of 0.9964. On the QAMEBI, it reached a Dice score of 0.8815, Jaccard index of 0.8770, precision of 0.8993, recall of 0.8937, and specificity of 0.9949. Experimental results demonstrate that LKCAU-Net outperforms current state-of-the-art segmentation approaches, providing enhanced accuracy and robustness in breast cancer segmentation from ultrasound images.
Introduction
Breast cancer remains one of the most prevalent malignancies threatening women’s health worldwide. A large-scale analysis published in Nature Medicine by the International Agency for Research on Cancer (IARC) on February 24, 2025, projects that the annual incidence of new breast cancer cases will rise to 3.2 million by 2050, resulting in more than 1.1 million related deaths each year. 1 Early detection is crucial for improving patient survival rates,2,3 and among the available diagnostic tools, ultrasound imaging plays an increasingly vital role due to its accessibility and effectiveness in identifying breast lesions at an early stage.
Ultrasound has become a cornerstone in breast cancer screening, offering a non-ionizing, real-time, and cost-effective imaging solution. In the field of computer-aided diagnosis (CAD), the segmentation of breast ultrasound (BUS) images is particularly critical for the accurate localization and characterization of tumors,4 -6 which in turn supports timely and reliable early diagnosis. However, achieving precise segmentation is still challenging due to inherent limitations of BUS images, including low contrast, indistinct tumor boundaries, and significant morphological variability—factors that often lead to false positives and missed detections.7,8 Representative BUS images illustrating these challenges are presented in Figure 1.
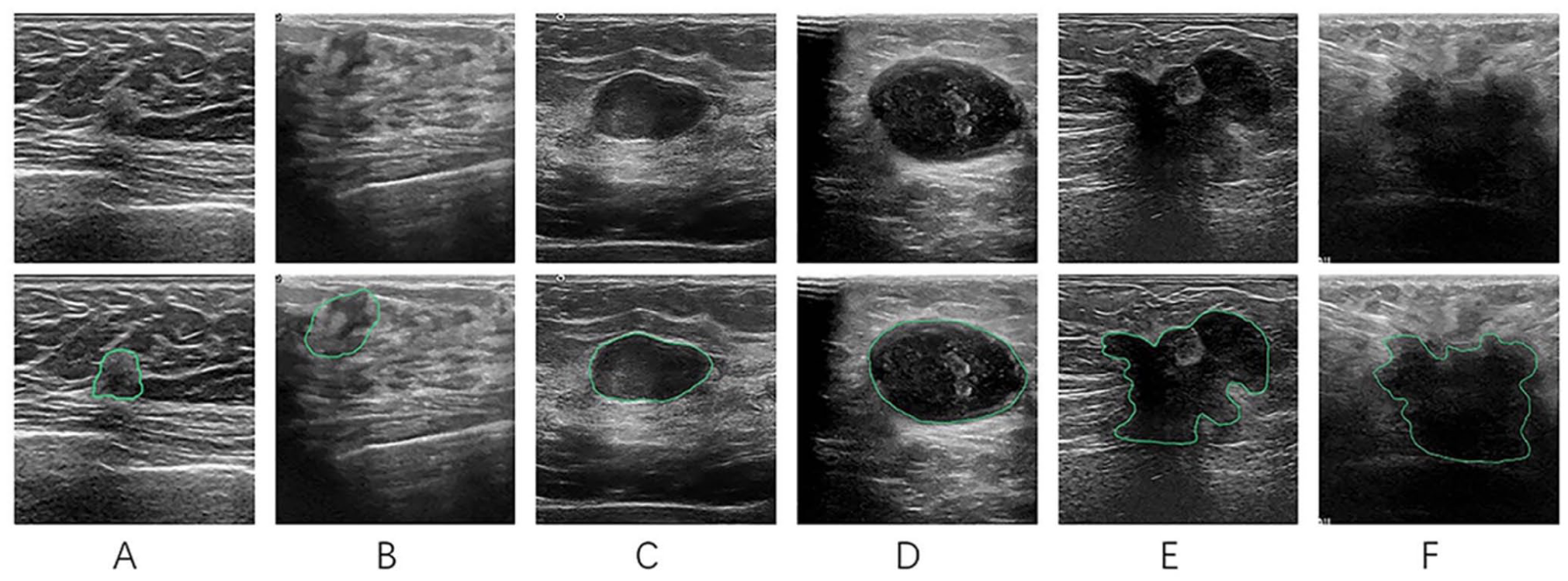
Representative BUS images illustrating key segmentation challenges. The green contours indicate ground truth annotations. (A and B) Tumors with low image contrast. (C and D) Tumors with ambiguous boundaries. (E and F) Tumors with significant morphological variability. Images (B, D and F) are from the BUSI dataset, 9 while the others are from Dataset B. 7
With the rise of deep learning, many segmentation frameworks have been proposed to automate BUS image analysis.10 -12 The U-Net architecture has become particularly prominent due to its encoder-decoder structure and strong performance in medical image segmentation. 13 Variants such as U-Net++, 14 U-Net 3D, 15 and nnU-Net 16 have further enhanced performance by improving feature fusion, network depth, and adaptability.
In recent years, medical image segmentation has made significant progress through multi-scale feature extraction technology, exhibiting a clear developmental trajectory.17 -19 Beginning with the U-Net encoder-decoder architecture that supports hierarchical feature learning, researchers identified limitations in simple symmetric structures for feature transfer. To address this, DenseNet introduced dense connections to enhance feature reuse, 20 NU-Net improved expressive capabilities by increasing network depth, 21 and SegNet optimized the feature restoration process using pooling indices in the decoder. 22 These advancements effectively improved the extraction of high-level semantic features, but robust low-level feature expression remained a challenge. To mitigate this issue, DeepLabV3 proposed the ASPP module, 23 which fuses receptive fields of different scales by constructing multiple parallel atrous convolution branches, achieving dynamic integration of cross-scale features for the first time. Concurrently, models like D-DDPM 24 and EMCAD 25 explored alternative approaches, integrating deep convolution strategies with nested structure design to enhance the model’s robustness and boundary perception in complex backgrounds, further expanding the expressiveness of multi-scale modeling technology. Recently, HCMU-Net introduced a hybrid attention fusion module that effectively integrates multi-scale semantic information, 26 further improving segmentation performance. However, multi-scale features alone are insufficient to fully address challenges posed by surrounding tissue interference and blurred tumor boundaries.
In parallel, various attention mechanisms have been developed to refine feature representations in segmentation networks.27 -29 For instance, SENet enhances feature selection by modeling inter-channel dependencies through channel attention. 30 Hou et al. proposed CA, which embeds positional information into channel attention, 31 enabling the capture of long-range dependencies and improving object localization. CBAM sequentially applies channel and spatial attention to extract more informative and discriminative features. 32 Building on these methods, AAU-Net employs a hybrid adaptive attention mechanism to fuse multi-scale features across diverse receptive fields, 33 resulting in more robust segmentation of complex breast lesions. More recently, ESKNet introduced an enhanced selective kernel convolution module that adaptively selects features from multiple receptive field scales by jointly leveraging channel and spatial information, 34 while also reinforcing long-range feature dependencies. This enhances the network’s ability to represent intricate anatomical structures. Collectively, these attention mechanisms help reduce noise interference and improve sensitivity to clinically relevant regions.35,36 Nevertheless, segmentation models still face challenges such as false detections and missed detections, particularly in cases with ambiguous boundaries and heterogeneous lesion appearances.37,38
In summary, the existing multi-scale feature fusion strategy and attention mechanisms each have distinct advantages in enhancing segmentation performance: the former captures contextual information at different scales, bolstering the model’s capacity to express complex structures, while the latter effectively reduces interference and improves focus on key areas. Drawing on the successful practices of these two methods, we propose a new fusion segmentation architecture, LKCAU-Net, to synergistically integrate multi-scale contextual information with the attention mechanism.
Our main contributions are summarized as follows:
Design a new LKCA module that integrates large-core spatial attention and coordinate attention to effectively improve the ability to model long-range dependencies and express location information.
Introduce the ASPP module in the deepest feature extraction layer of the network to enhance the aggregation ability of multi-scale contextual features.
Construct a deeper architecture to strengthen feature learning capabilities.
We implemented experiments on four public datasets. Results show that our network outperforms the state-of-the-art methods for tumor segmentation on BUS images.
The rest of this paper is organized as follows: Section 2 describes the proposed segmentation network. Section 3 provides details on the public ultrasound datasets, experimental setup, and evaluation metrics. Section 4 presents the experimental results. The discussion and conclusions are offered in Sections 5 and 6, respectively.
Methodology
In this section, we introduce the overall architecture of LKCAU-Net, followed by detailed descriptions of its key components: the LKCA module, the ASPP module, 23 the deeper U-Net structure, and the loss function.
Overall Architecture
Figure 2 illustrates the overall architecture of LKCAU-Net. The network is built on a deep U-Net framework, where the standard convolutional layers in the decoder are replaced by the proposed LKCA modules to enhance spatial and channel-wise feature representation. To further improve multi-scale feature extraction, an ASPP module is embedded at the deepest feature extraction layer of the network. This combination of components allows LKCAU-Net to capture richer contextual information and more accurate boundary features. The following subsections provide a detailed explanation of each component.
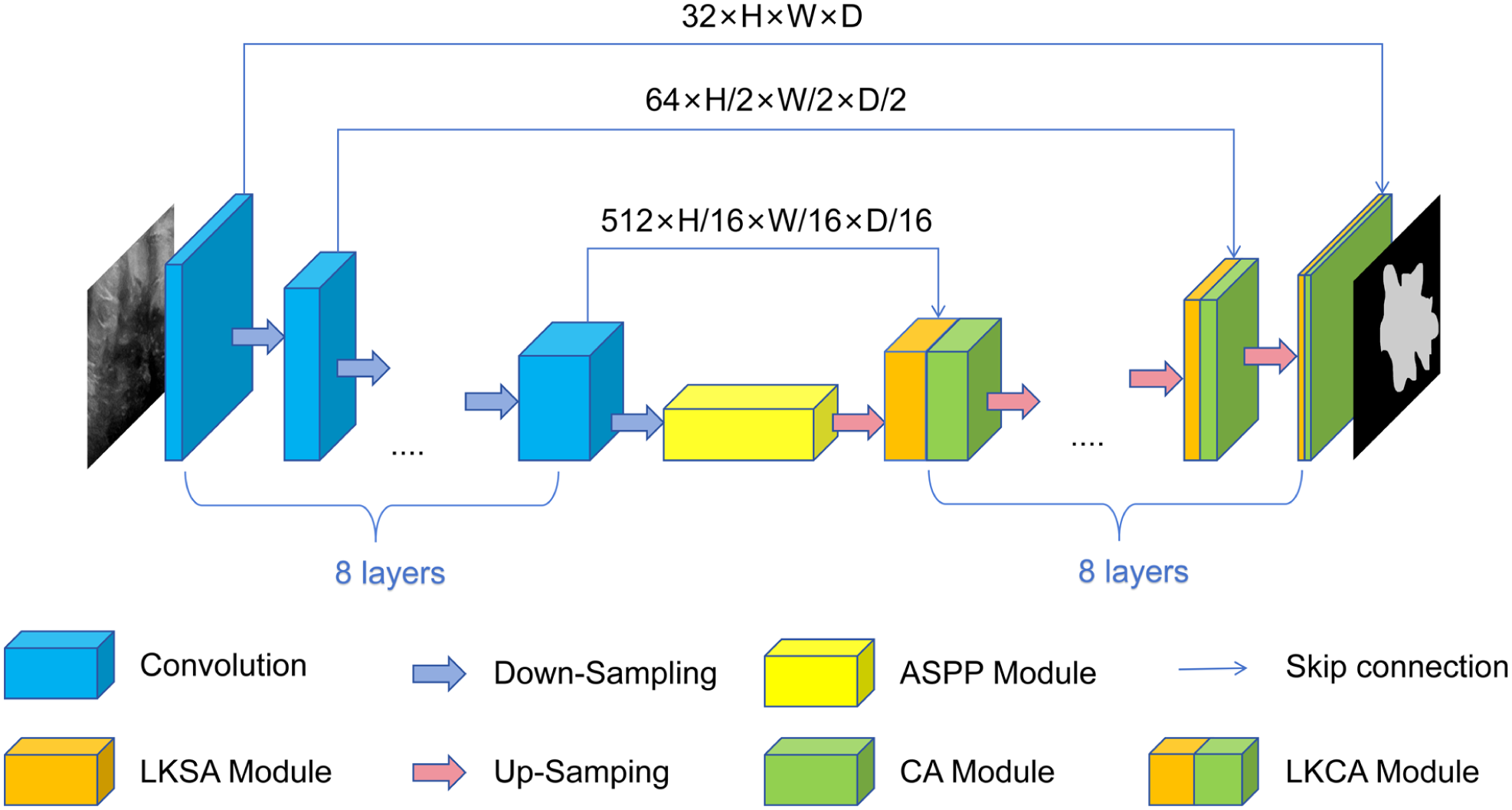
The overall architecture of LKCA-UNet, which adopts an eight-layer encoder-decoder structure with channel dimensions of 32, 64, 128, 256, 512, 512, 512, and 512 at each successive layer. In the decoder, each stage incorporates an LKCA module that integrates the Large Kernel Spatial Attention (LKSA) module and the Channel Attention (CA) module. Furthermore, an Atrous Spatial Pyramid Pooling (ASPP) module is embedded at the deepest feature extraction layer to enhance multi-scale feature representation.
Large Kernel Coordinate Attention(LKCA)
The LKCA module is designed to model long-range spatial dependencies and precise positional information by combining two attention mechanisms: Large-Kernel Spatial Attention (LKSA) and Coordinate Attention (CA). 31 In the following sections, we will elaborate on the design and functionality of each attention submodule.
Large-kernel spatial attention (LKSA)
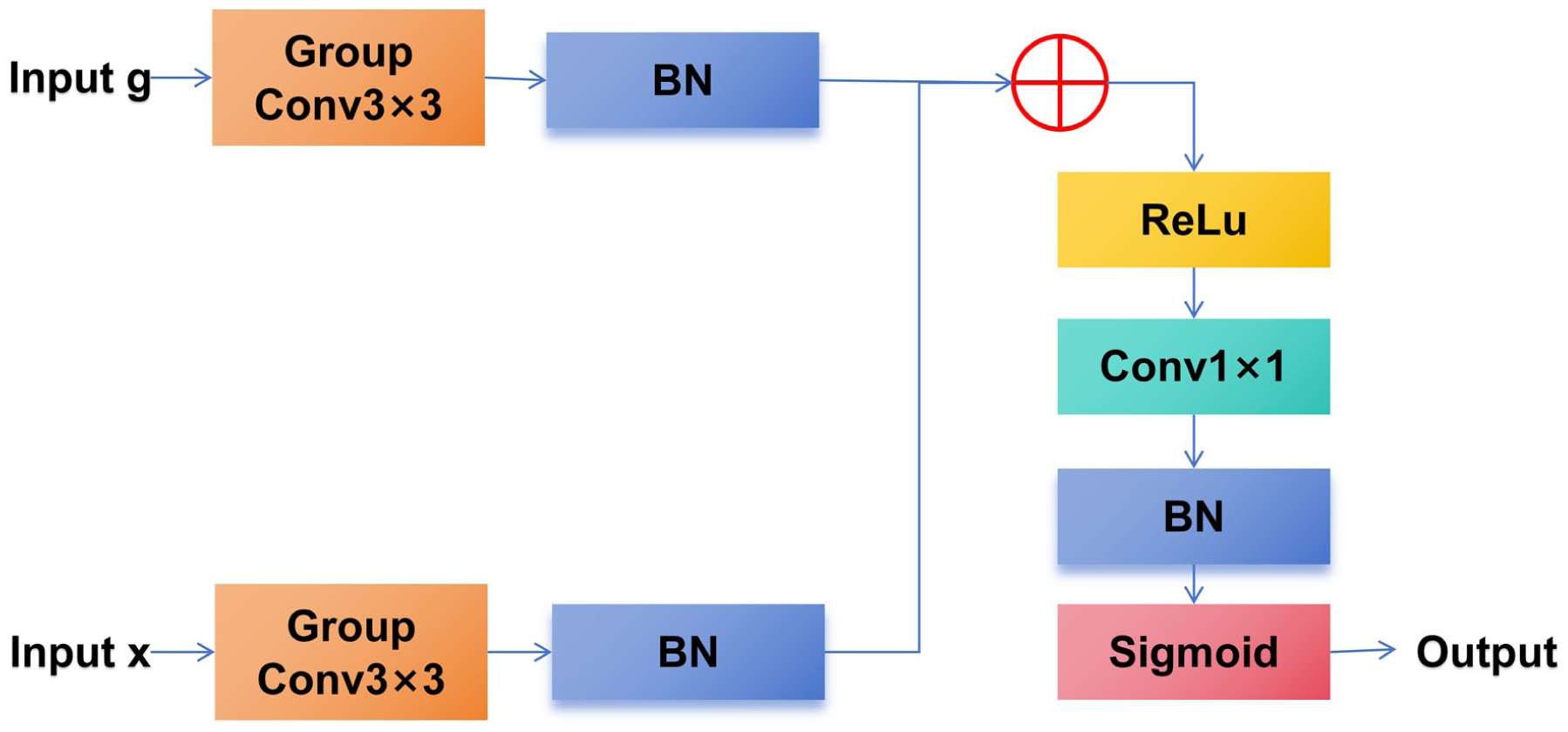
To enhance the feature selection process during segmentation, we propose the LKSA module (as illustrated in Figure 3), which progressively fuses feature maps with attention weights that are adaptively learned by the network to emphasize relevant features and suppress irrelevant ones. Specifically, a gating mechanism is employed, where high-level features act as gating signals to selectively control the flow of information from current-layer features, improving segmentation accuracy in medical imaging tasks.
The architecture of the Large-Kernel Spatial Attention module (LKSA).
The attention function is originally defined in Attention U-Net, 39 where both the gating signal g (from skip connections) and the input feature map x (from the decoder) are processed using 1 × 1 convolutions. Building upon this, we propose an improved attention function qatt(·) by replacing the original 1 × 1 convolutions with separate 3 × 3 group convolutions, denoted as GCg(·) for the gating input g and GCx(·) for the feature input x. The outputs of these convolutions are independently normalized by batch normalization (BN(·)), 40 then combined via element-wise addition. The combined feature undergoes a ReLU activation (ReLU(·)), 41 followed by a 1 × 1 convolution (ConV(·)) and another batch normalization layer. Finally, a Sigmoid activation (S(·)) generates the single-channel attention weight map. These attention weights are then applied to modulate the input feature map b through element-wise multiplication, resulting in the attention-enhanced output LKSA(g, x). The complete formulation of LKSA is detailed in equations (1) and (2):


By incorporating 3 × 3 group convolutions within the qatt(·) function, our design captures broader spatial dependencies while maintaining computational efficiency.
Coordinate attention mechanism (CA)
To enhance the model’s ability to capture both long-range dependencies and precise spatial information, especially critical for the structural characteristics of BUS images, we incorporate the CA mechanism (as shown in Figure 4). 31 Unlike traditional channel attention mechanisms that typically perform global average pooling across spatial dimensions. thus discarding positional information, Coordinate Attention encodes both channel-wise dependencies and precise positional context by decoupling spatial information into two one-dimensional feature encodings.
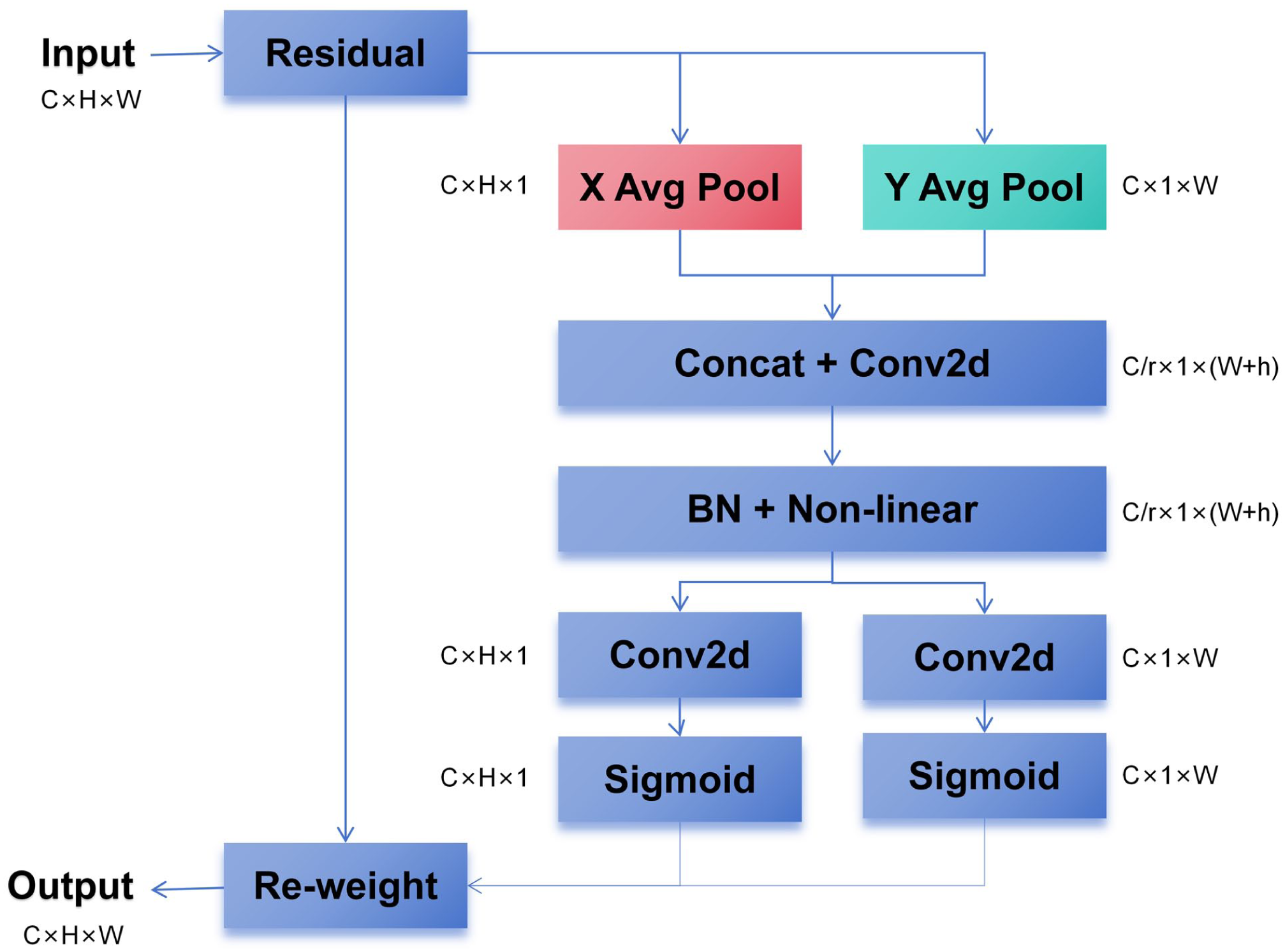
The architecture of the Coordinate attention mechanism (CA).
Given an input feature map
Horizontal pooling along the height axis to produce
Vertical pooling along the width axis, followed by a transpose, to yield
These two representations are then concatenated along the spatial (height) dimension to form a unified tensor
Each of the split tensors is processed by separate

In equation (3), the operator (e.g.,

In equation (4), the operator (e.g., ⊙) represents element-wise multiplication, and the spatial alignment is ensured through appropriate reshaping and permutation operations.
This mechanism allows the network to model long-range dependencies in one spatial direction while preserving precise location information in the other. By embedding positional information into channel attention, the CA module enhances the model’s spatial awareness with minimal additional computational overhead. In our framework, the integration of Coordinate Attention effectively improves the delineation of tumor boundaries, which are often ambiguous in BUS images, and contributes to more accurate and robust segmentation performance. Specifically, by enabling the network to focus on spatially relevant regions while maintaining a strong response to critical features along both horizontal and vertical axes, the CA module helps to suppress background noise and highlight lesion contours. This leads to improved segmentation consistency across varying tumor sizes and shapes, ultimately enhancing the network’s generalization capability.
Atrous Spatial Pyramid Pooling (ASPP)
To enrich multi-scale contextual information, we incorporate the Atrous Spatial Pyramid Pooling (ASPP) module at the deepest feature extraction layer of the network. Initially proposed in DeepLab V2, 43 ASPP leverages parallel atrous convolutions with different dilation rates to capture features at multiple receptive fields. DeepLab V323 further enhances this design by introducing image-level global average pooling and expanding the number of parallel branches, enabling more effective integration of both local details and global context. In our work, we adopt the improved ASPP module from DeepLab V3 to better capture semantic information across diverse scales and enhance segmentation performance.
The ASPP module consists of five parallel branches. The first branch applies a 1 × 1 convolution, capturing fine-grained local features while preserving detailed spatial information. The second, third, and fourth branches employ 3 × 3 atrous convolutions with dilation rates of 6, 12, and 18, respectively. These branches are designed to extract contextual features at multiple scales, with atrous convolutions enlarging the receptive field by inserting spaces within the convolution kernel, thereby maintaining the spatial resolution of the feature map. The fifth branch performs global average pooling, compressing the input into a 1 × 1 global representation, followed by a 1 × 1 convolution to extract channel-wise features. This global feature is then upsampled via bilinear interpolation to match the spatial dimensions of the other branches, providing a rich global context.
Finally, the outputs from all five branches are concatenated along the channel dimension and fused using a 1 × 1 convolution layer. This design effectively integrates both local detail and global semantic information, enhancing the model’s ability to perceive object boundaries and small-scale structures. In this study, high-level semantic feature maps are input to the ASPP module prior to the upsampling stage, enabling the network to capture and fuse features at multiple scales and thereby improve segmentation performance. The structure of the ASPP module is illustrated in Figure 5.
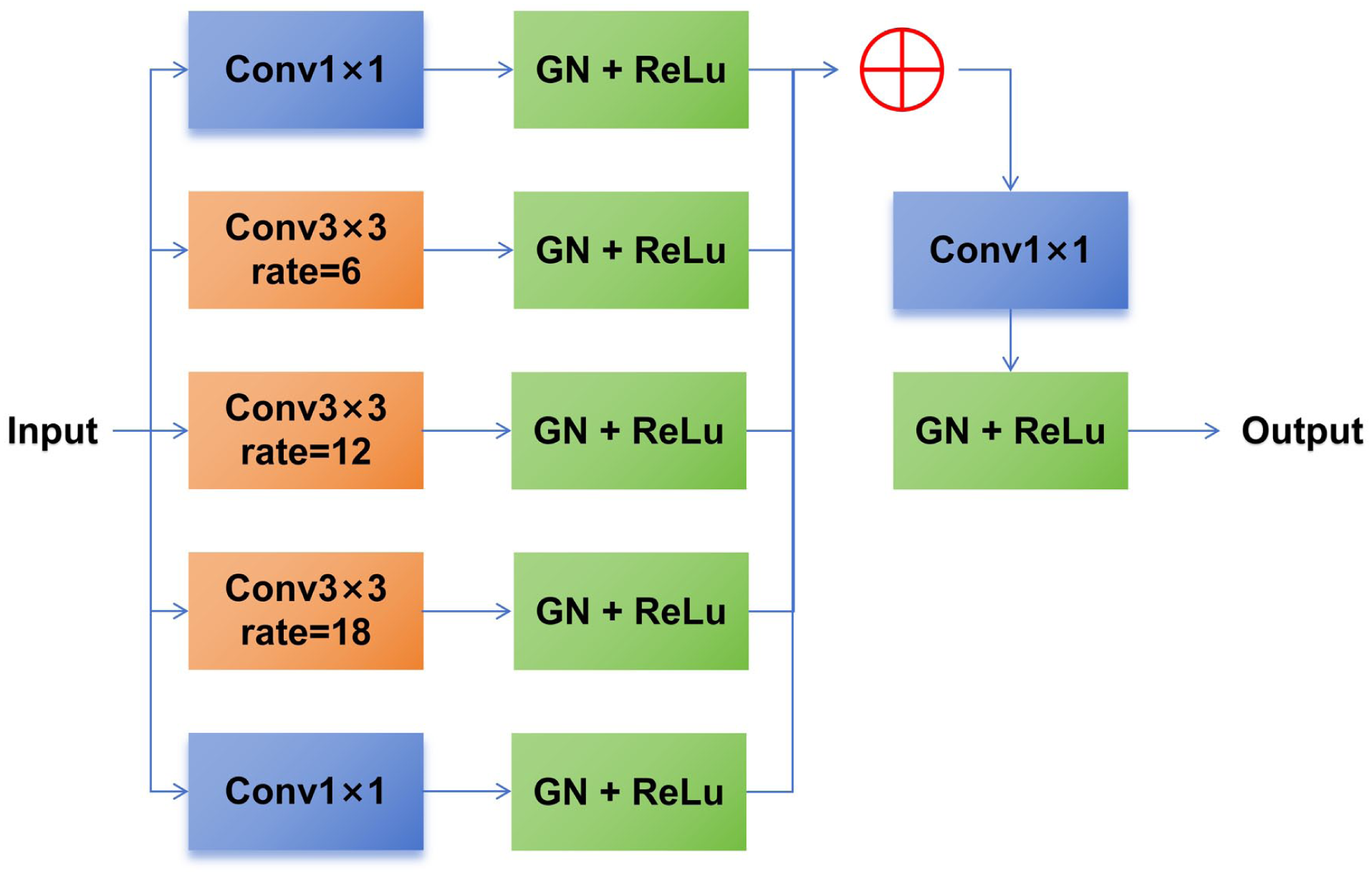
The architecture of the atrous spatial pyramid pooling module (ASPP).
Deeper U-Net
U-Net and its variants have been widely adopted for breast lesion segmentation in ultrasound images. Despite their proven effectiveness, most existing models are relatively shallow, typically consisting of only five layers. 14 Such shallow architectures often struggle to adequately capture the spatial and locational characteristics of breast tumors, particularly in ultrasound images that are inherently challenging due to their low quality, diverse morphological patterns, homogeneous surrounding tissues, and blurred lesion boundaries.
To overcome these limitations, recent studies have highlighted the benefits of deeper network architectures, which offer improved generalization and enhanced representational capacity, thereby leading to better segmentation performance. 44 Motivated by this observation, we propose a deeper U-Net-based architecture that extends the network depth to eight layers. This design enables the model to more effectively capture hierarchical features, as illustrated in Figure 2.
In our implementation, the number of feature channels progressively increases across layers as follows: 32, 64, 128, 256, 512, 512, 512, and 512. In the encoder, the number of standard convolutional modules per layer is set to 1, 3, 4, 6, 6, 6, 6, and 6, respectively. Each module consists of a 3 × 3 convolution followed by batch normalization and a ReLU activation. In the decoder, standard convolutional modules are replaced by LKCA modules, while the number of modules per layer remains unchanged. Additionally, a CA module is applied after multiple LKCA modules. This design ensures a consistent and efficient feature extraction pipeline throughout the network.
Loss Function
In this study, we adopt a composite loss function, DC_and_CE_loss, which combines Cross Entropy (CE) loss and Soft Dice loss to enhance the segmentation performance of BUS images. This loss function leverages the pixel-level classification strength of CE loss and the shape-awareness of Dice loss, making it particularly suitable for medical image segmentation tasks characterized by severe class imbalance. Specifically, the Soft Dice loss measures the overlap between the predicted segmentation and the ground truth, and is defined as:

where

where

Furthermore, the loss function supports settings, allowing the model to skip gradient updates for irrelevant regions in the label map and thus focus on regions of interest. By jointly optimizing for both region overlap and classification accuracy, this loss function effectively improves segmentation robustness and precision, particularly in scenarios with boundary ambiguity and class imbalance.
Datasets and Experimental Settings
BUS Datasets
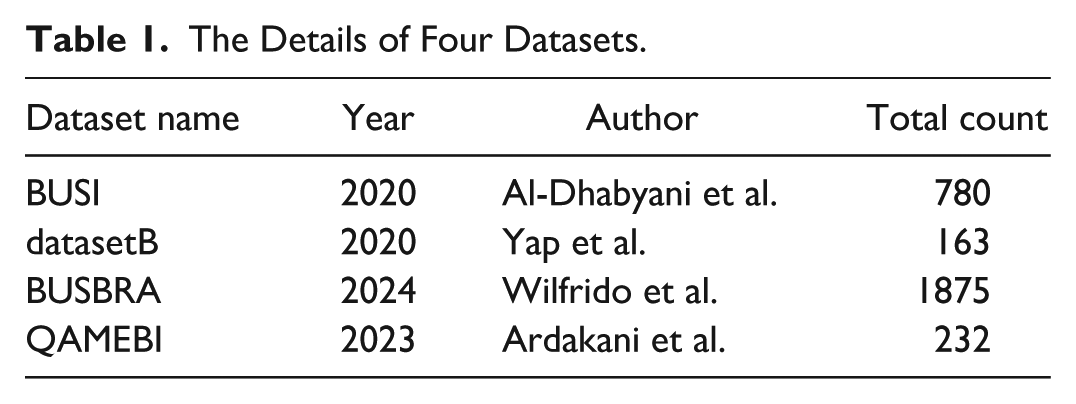
As shown in Table 1, we evaluate the segmentation network’s performance in this research using four publicly accessible breast ultrasound (BUS) datasets of various scales. The first dataset, BUSI, 9 was developed by Al-Dhabyani et al. and comprises 780 images obtained from two ultrasound devices, including LOGIQ E9 and LOGIQ E9 Agile, at Baheya Hospital. The images have an average resolution of 500 × 500 pixels. The second dataset, Dataset B, 7 was curated by Yap et al. It includes 163 ultrasound images, each with an average resolution of 760 × 570 pixels, captured using the Siemens ACUSON Sequoia C512 scanner. The third dataset, BUS-BRA, 45 was introduced by Gómez-Flores et al. and consists of 1875 ultrasound images of breast lesions, sourced from 1064 female patients. These images were collected using four different ultrasound machines at the National Institute of Cancer in Rio de Janeiro, Brazil. The fourth dataset, QAMEBI, 46 was introduced by Abbasian Ardakani et al. and comprises 232 ultrasound images of histologically confirmed breast lesions. The dataset was collected from female patients aged over 18 years without a history of breast cancer in either the ipsilateral or contralateral breast. All images were acquired using an AirPlorer Ultimate ultrasound machine in accordance with the guidelines of the American College of Radiology.
The Details of Four Datasets.
Experimental Settings
To rigorously evaluate the performance and robustness of the proposed network, we conducted a series of carefully designed experiments. This section details the implementation environment, training configuration, and data augmentation strategies used during model development. These settings are crucial for ensuring fair comparison, reproducibility, and optimal generalization in the breast tumor segmentation task.
The network was implemented using PyTorch 1.11.0 on Ubuntu 20.04 and trained from scratch for 100 epochs on a single NVIDIA RTX 4090 GPU with a batch size of 13. ReLU activation functions and Batch Normalization (BN) were employed throughout the model. Training utilized the Adam optimizer with an initial learning rate of 1 × 10−2.
To enhance the model’s generalization capability in breast tumor segmentation tasks on ultrasound images, we developed a comprehensive data augmentation pipeline. This pipeline introduces a variety of random transformations to the input images and their corresponding labels during the training phase. By simulating diverse real-world imaging conditions, this approach improves the model’s robustness and adaptability to clinical variations.
The data augmentation strategy includes spatial transformations such as random rotations, scaling, and mirror flipping, which introduce geometric variability. Additionally, intensity-based transformations are employed, including Gaussian noise injection, Gaussian blurring, brightness and contrast adjustments, pseudo-resolution simulation, and gamma correction. These operations mimic different acquisition qualities and lighting conditions. To further enhance the model’s resistance to noisy annotations, label refinement techniques are applied to improve label consistency and reduce the impact of outliers.
All augmentation operations are performed probabilistically during each training iteration, ensuring that the model is exposed to a wide range of potential perturbations throughout training. This strategy effectively enhances both the robustness and generalization performance of the segmentation network.
Evaluation Metrics
To objectively assess the effectiveness of various segmentation methods on breast ultrasound lesion images, we adopt five widely accepted performance indicators: Dice Similarity Coefficient, Jaccard Index, Precision, Recall, and Specificity. These metrics collectively offer a multidimensional evaluation of segmentation accuracy.
The Jaccard Index, or Intersection over Union (IoU), quantifies the similarity between the predicted lesion area and the ground truth by calculating their overlap ratio. Precision measures the accuracy of positive predictions, indicating the proportion of correctly identified lesion pixels among all pixels predicted as lesions, thereby reflecting the model’s ability to avoid false positives. Recall—also known as Sensitivity or the True Positive Rate—captures the model’s capacity to detect all true lesion pixels, representing its effectiveness in minimizing false negatives. Specificity, on the other hand, represents the proportion of correctly classified background pixels out of all true background pixels, and thus assesses the model’s reliability in distinguishing non-lesion areas. The Dice coefficient integrates both Precision and Recall, providing a balanced assessment of segmentation performance and serving as a robust metric in the context of medical image analysis. In addition, we incorporate the 95th percentile Hausdorff Distance (HD95) to evaluate boundary accuracy. HD95 measures the distance between the predicted and ground-truth contours by computing the 95th percentile of the Hausdorff Distance(HD), which reduces sensitivity to outliers compared to the maximum Hausdorff Distance. Lower HD95 values indicate closer alignment between the predicted and true boundaries, making it particularly suitable for assessing fine-grained contour delineation in medical image segmentation tasks.
These metrics are crucial for evaluating segmentation performance, especially in clinical scenarios where both lesion detection accuracy and control of false positives are essential. 47 The mathematical definitions of these five indicators are as follows:






Here, TP (true positives) refers to the count of lesion pixels accurately identified by the model, FP (false positives) indicates the number of background pixels mistakenly classified as lesions, FN (false negatives) represents the lesion pixels that the model failed to detect, and TN (true negatives) corresponds to the background pixels correctly classified as non-lesions.
Experimental Results
This section provides a comprehensive evaluation of the proposed LKCAU-Net model through both quantitative and qualitative experiments. We aim to assess its segmentation performance, compare it to state-of-the-art methods, and analyze the contributions of its key architectural components. First, we conduct benchmark comparisons with several leading segmentation models using four public BUS datasets to demonstrate the overall effectiveness and generalizability of our method. Next, we perform detailed ablation studies to explore the impact of individual modules and network depth on model performance. These experiments offer critical insights into the strengths and potential limitations of our design choices, guiding future improvements.
Comparison With State-of-the-Art Methods
To evaluate the overall effectiveness and generalizability of our method, we first compare it with state-of-the-art deep learning techniques for BUS images and medical image segmentation. The comparative methods include U-Net, 13 SegNet, 22 Att U-Net, 39 U-Net++, 14 AAU-Net, 33 LKMU-Net, 48 and nnU-Net. 16 To ensure a fair comparison, we perform five-fold cross-validation on the BUSI, 9 BUSBRA, 45 Dataset B 7 and QAMEBI. 46 All comparative methods are adequately retrained on the same training data. In the comparison experiments, the segmentation results of all methods do not undergo any post-processing.
The quantitative results are summarized in Tables 2 to 5, which report the performance of all models on the BUSI, Dataset B, BUSBRA and QAMEBI, respectively.
Quantitative Analysis Results of Our Network (LKCAU-net) Compared to State-of-the-Art Methods on BUSI With Five Evaluation Metrics.
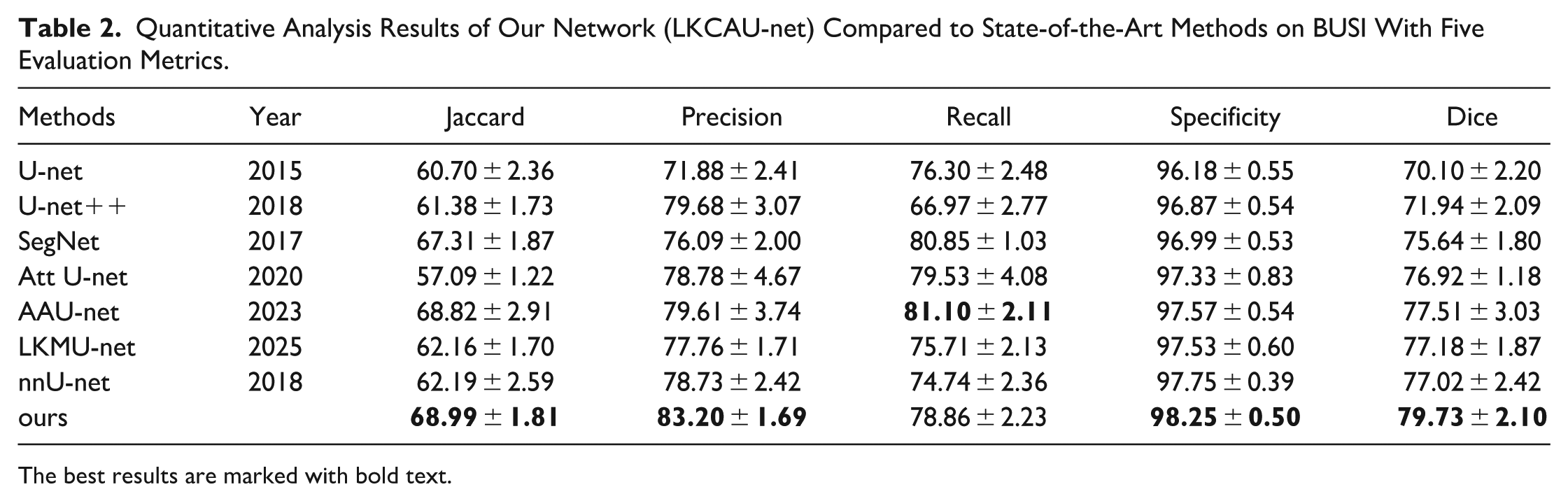
The best results are marked with bold text.
Quantitative Analysis Results of Our Network (LKCAU-net) Compared to State-of-the-Art Methods on DatasetB With Five Evaluation Metrics.
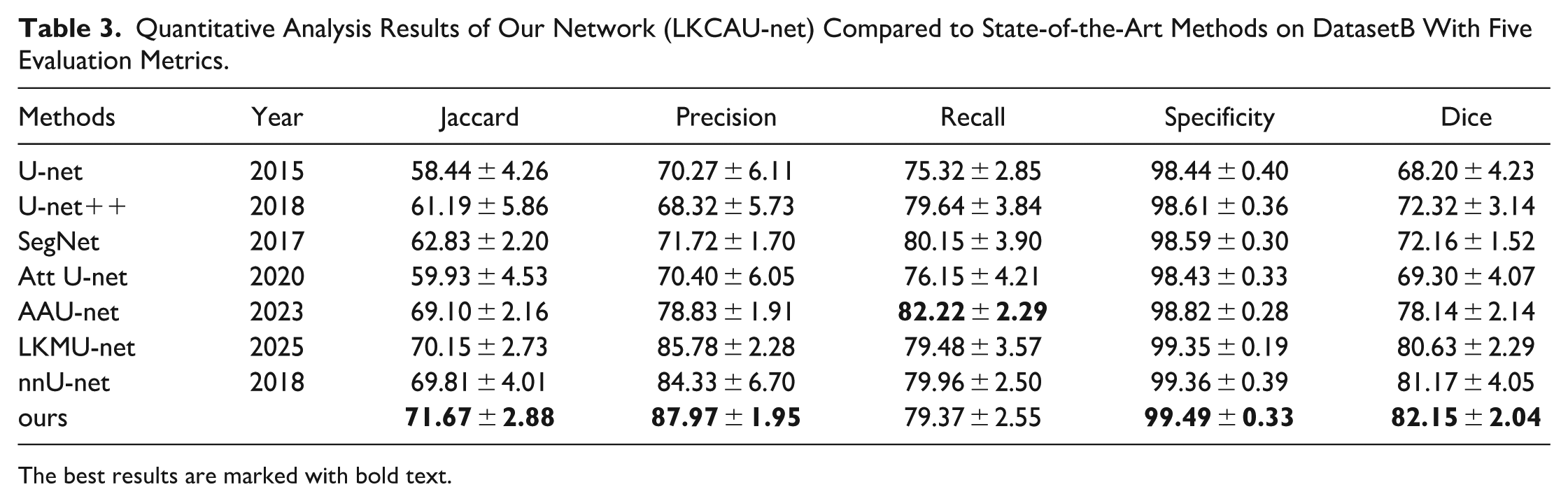
The best results are marked with bold text.
Quantitative Analysis Results of Our Network (LKCAU-net) Compared to State-of-the-Art Methods on BUSBRA With Five Evaluation Metrics.
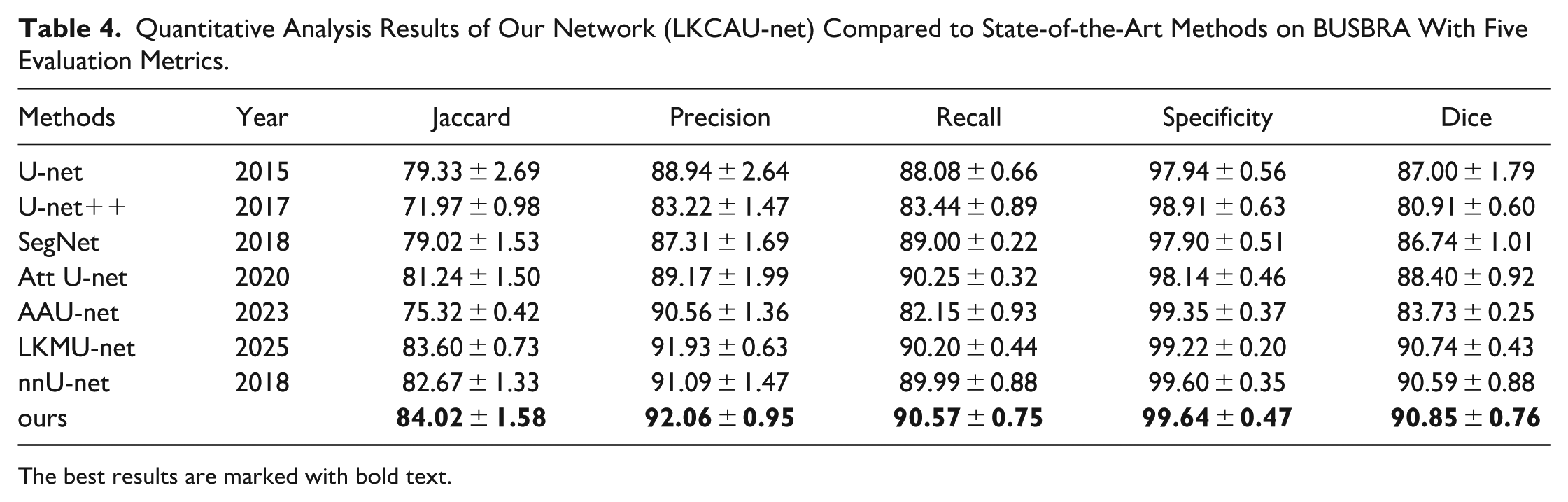
The best results are marked with bold text.
Quantitative Analysis Results of Our Network (LKCAU-net) Compared to State-of-the-Art Methods on QAMEBI with Five Evaluation Metrics.
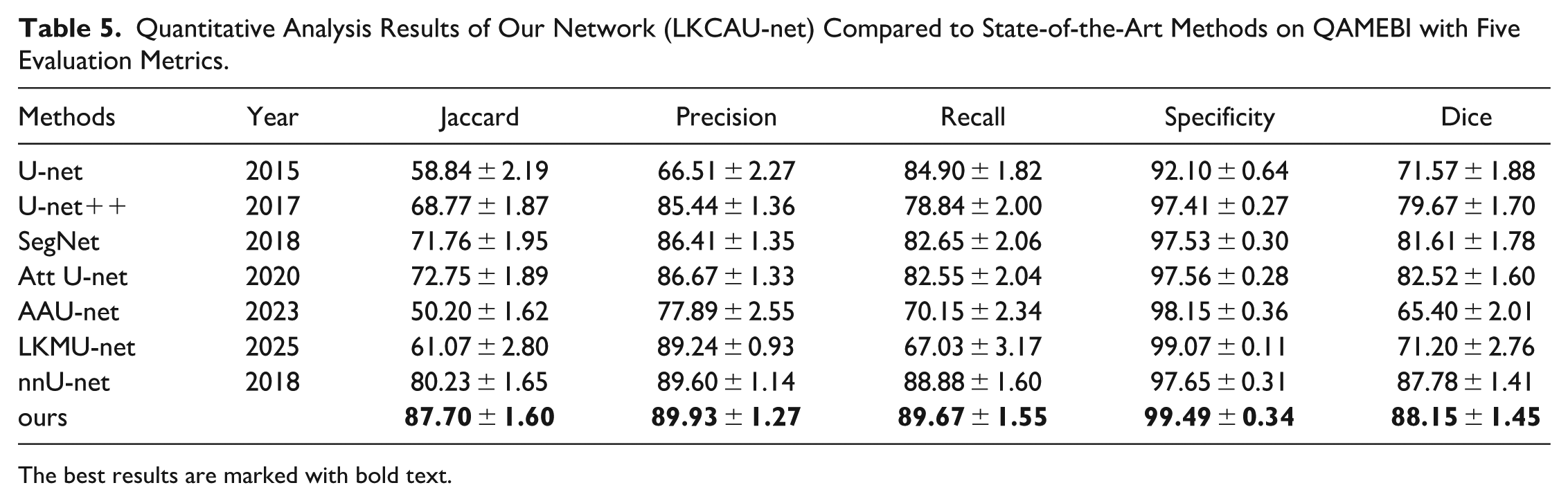
The best results are marked with bold text.
Tables 2 and 3 present the quantitative results on the BUSI and Dataset B datasets. On the BUSI dataset, our method achieves the best performance across four evaluation metrics, with Jaccard of 68.99, Precision of 83.20, Specificity of 98.25, and Dice of 79.73. Compared to the baseline nnU-Net, 16 these results correspond to improvements of 9.3%, 5.6%, 0.5%, and 3.5%, respectively. Similarly, on Dataset B, our method achieves Jaccard of 71.67, Precision of 87.97, Specificity of 99.49, and Dice of 82.15, yielding improvements of 2.6%, 4.3%, 0.1%, and 1.2%, respectively.
Table 4 presents the quantitative results on the BUSBRA dataset. Our method achieves the best performance across five evaluation metrics, with Jaccard of 84.02, Precision of 92.06, Recall of 90.57, Specificity of 99.64, and Dice of 90.85. Compared to the baseline nnU-Net, 16 these results correspond to improvements of 1.6%, 1.0%, 0.6%, 0.04%, and 0.2%, respectively.
Table 5 presents the quantitative results on the QAMEBI dataset. Our method achieves the best performance across five evaluation metrics, with Jaccard of 87.70, Precision of 89.93, Recall of 89.67, Specificity of 99.49, and Dice of 88.15. Compared to the baseline nnU-Net, 16 these results correspond to improvements of 9.3%, 0.3%, 0.9%, 1.9%, and 0.4%, respectively.
Figure 6 presents a visual comparison of tumor segmentation results generated by our proposed method and several state-of-the-art approaches. The first three examples are from the DatasetB, the fourth to sixth examples are from the BUSI, the seventh and eighth examples are from the BUS-BRA and the ninth example is from the QAMEBI. These representative samples are carefully selected to illustrate the strengths of our model in addressing three critical challenges commonly encountered in breast ultrasound image segmentation.
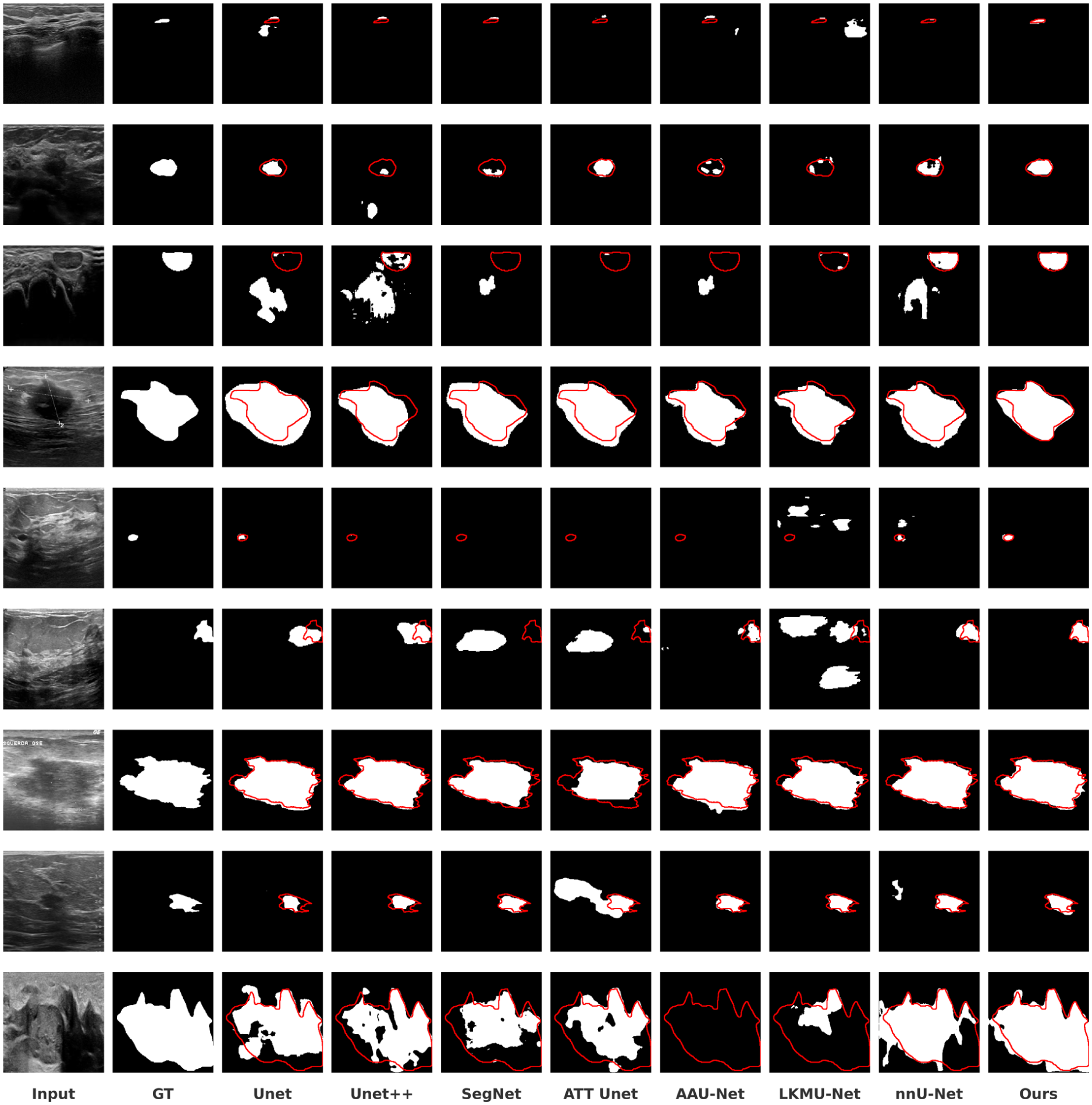
Visual comparison of our network (LKCAU-Net) against state-of-the-art methods, including UNet, UNet++, SegNet, AttUNet, AAU-Net, LKMU-Net, and nnU-Net. The first three examples are selected from the DatasetB, the fourth to sixth examples are from the BUSI, the seventh and eighth examples are from the BUS-BRA and the ninth example is from the QAMEBI.
The first challenge is low image contrast, a typical feature of breast ultrasound images that often hinders accurate tumor delineation. While most models perform reasonably well on large, clearly defined tumors, their accuracy often declines in low-contrast scenarios, where normal tissue may be misclassified as tumor regions. As shown in the third and sixth examples, several compared methods tend to over-segment, whereas our model achieves more precise and reliable boundary detection.
The second challenge is the morphological variability of tumors, particularly in cases involving very small lesions, such as in the first, fifth and ninth examples. In the fifth example, models like UNet++, SegNet, Att-UNet, and AAU-Net fail to detect the tumor entirely. In contrast, our method successfully identifies the lesion and produces segmentation results that closely align with the ground truth, demonstrating superior sensitivity to subtle abnormalities.
The third challenge involves blurred tumor boundaries, which further complicate the segmentation task. As observed in the second, fourth, seventh, and eighth examples, most baseline methods can roughly locate the tumor region, but struggle to capture precise contours. Our model, however, excels at delineating fine-grained details, resulting in more accurate and refined segmentation outputs.
This advantage is further supported by the quantitative results in Table 6. Specifically, our method achieves the lowest HD95 across all four datasets, with values of 45.31 on QAMEBI, 12.61 on BUSBRA, 70.89 on BUSI, and 43.70 on DatasetB, outperforming all competing methods by a clear margin. Since HD95 measures the boundary distance between the predicted segmentation and the ground truth, lower values indicate more accurate boundary delineation. Therefore, the superior HD95 performance demonstrates that our model is more effective in capturing fine-grained boundary details, especially in challenging cases with blurred tumor edges.
HD95 Results of Different Methods on Four Ultrasound Datasets.
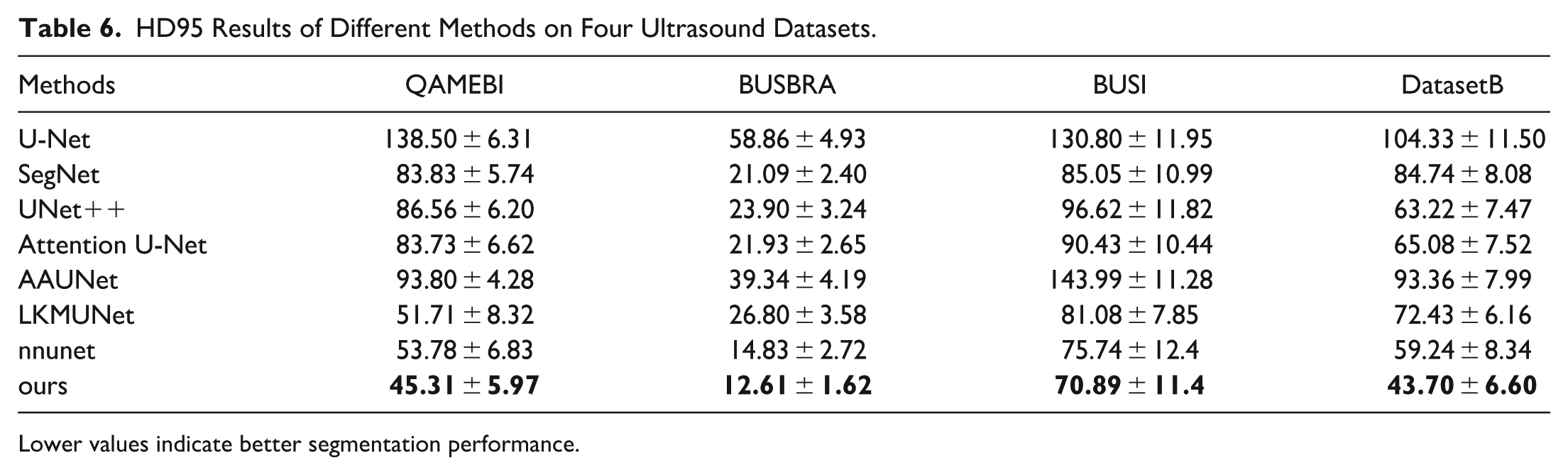
Lower values indicate better segmentation performance.
The aforementioned results provide strong evidence of the superior segmentation capability of our model. The performance improvements are primarily attributed to the LKCA module, which captures long-range dependencies through a large kernel spatial attention mechanism, while the coordinate attention mechanism encodes precise location information, enhancing the discrimination of tumor boundaries and reducing the risk of misclassifying non-tumor areas as tumors. Additionally, the ASPP module aggregates multi-scale contextual information, enabling the model to effectively perceive tumors of varying sizes and shapes, thereby avoiding local noise or structural abnormalities that could mislead the segmentation results.
Architecture Ablation
In this section, we conduct both module ablation and depth ablation experiments to evaluate the individual contributions of each proposed component and the impact of network depth on segmentation performance. The Dice coefficient, which directly measures the overlap between the predicted segmentation and the ground truth, provides an intuitive and clinically meaningful assessment of segmentation accuracy. Accordingly, we primarily report the Dice score in this section to ensure consistent, reliable, and interpretable comparisons across different methods.
Module ablation
To thoroughly evaluate the effectiveness of each component within the proposed architecture, we conduct ablation studies on the BUSI dataset 9 using nnU-Net 16 as the baseline framework. All experiments are carried out using five-fold cross-validation, and the results are summarized in Table 7.
Ablation Study of Different Network Components.
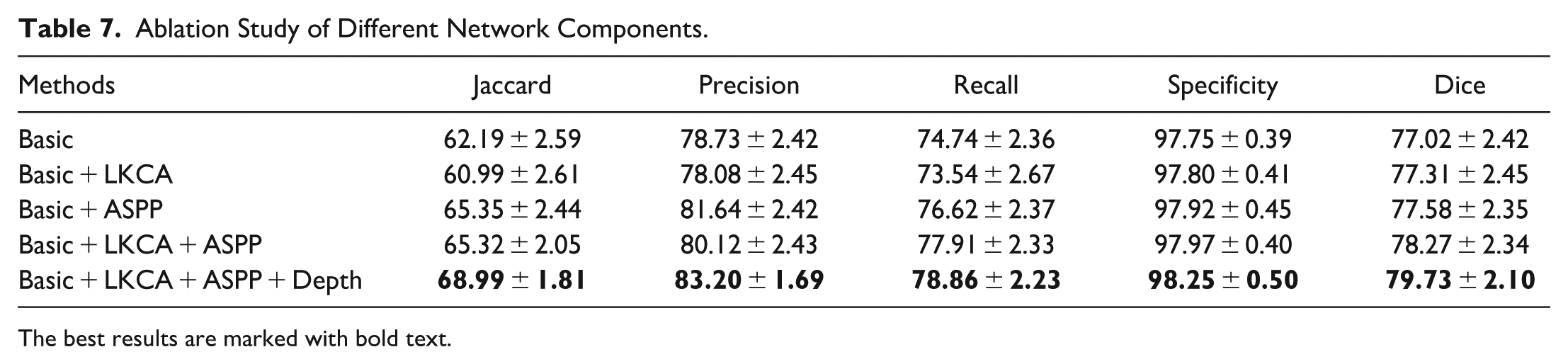
The best results are marked with bold text.
The “Basic” model refers to the original nnU-Net, which follows a five-layer U-Net-based encoder-decoder structure. “Basic + ASPP” integrates the ASPP module into the baseline to enhance multi-scale feature extraction. “Basic + LKCA” introduces the proposed LKCA module to capture rich spatial context and precise positional information. “Basic + ASPP + LKCA” combines both ASPP and LKCA modules. The final configuration, “Basic + LKCA + ASPP + Depth,” represents the full version of our proposed LKCAU-Net, incorporating both modules along with increased network depth, resulting in an eight-layer encoder–decoder architecture.
The experimental results show that the introduction of each module has a positive impact on the model performance. Specifically, the introduction of the LKCA module alone increases the Dice coefficient from 77.02 to 77.31, an increase of 0.3%, which verifies its effectiveness in enhancing spatial context perception and feature expression; after integrating the ASPP module, the Dice score is increased to 77.58, an increase of 0.56% compared with the baseline, reflecting the significant promotion of multi-scale context modeling on segmentation performance. When the two modules are used together, the Dice score is further improved to 78.27, an increase of 1.25% over the baseline model, indicating that LKCA and ASPP have good complementarity in spatial modeling and scale perception. Finally, when a deeper network structure is introduced on this basis, the complete LKCAU-Net achieves a Dice score of 79.73, an overall improvement of 2.71%.
Figure 7 provides a visual comparison of segmentation results across different component configurations. In the first and second examples, the “Basic” model incorrectly identifies non-tumor regions as tumor regions. Although both the “Basic+ASPP” and “Basic+LKCA” configurations eliminate these false positives, they also fail to capture parts of the actual tumor. The “Basic+LKCA+ASPP” configuration demonstrates improved tumor localization, while the full “LKCA-UNet” achieves accurate identification of the tumor regions. In the third and fourth examples, the “Basic” model fails to detect the tumor areas. However, progressive integration of ASPP and LKCA modules enhances the recognition performance, with the “LKCA-UNet” again showing the most accurate segmentation results. These results fully demonstrate the potential and advantages of the proposed method in breast tumor ultrasound image segmentation.
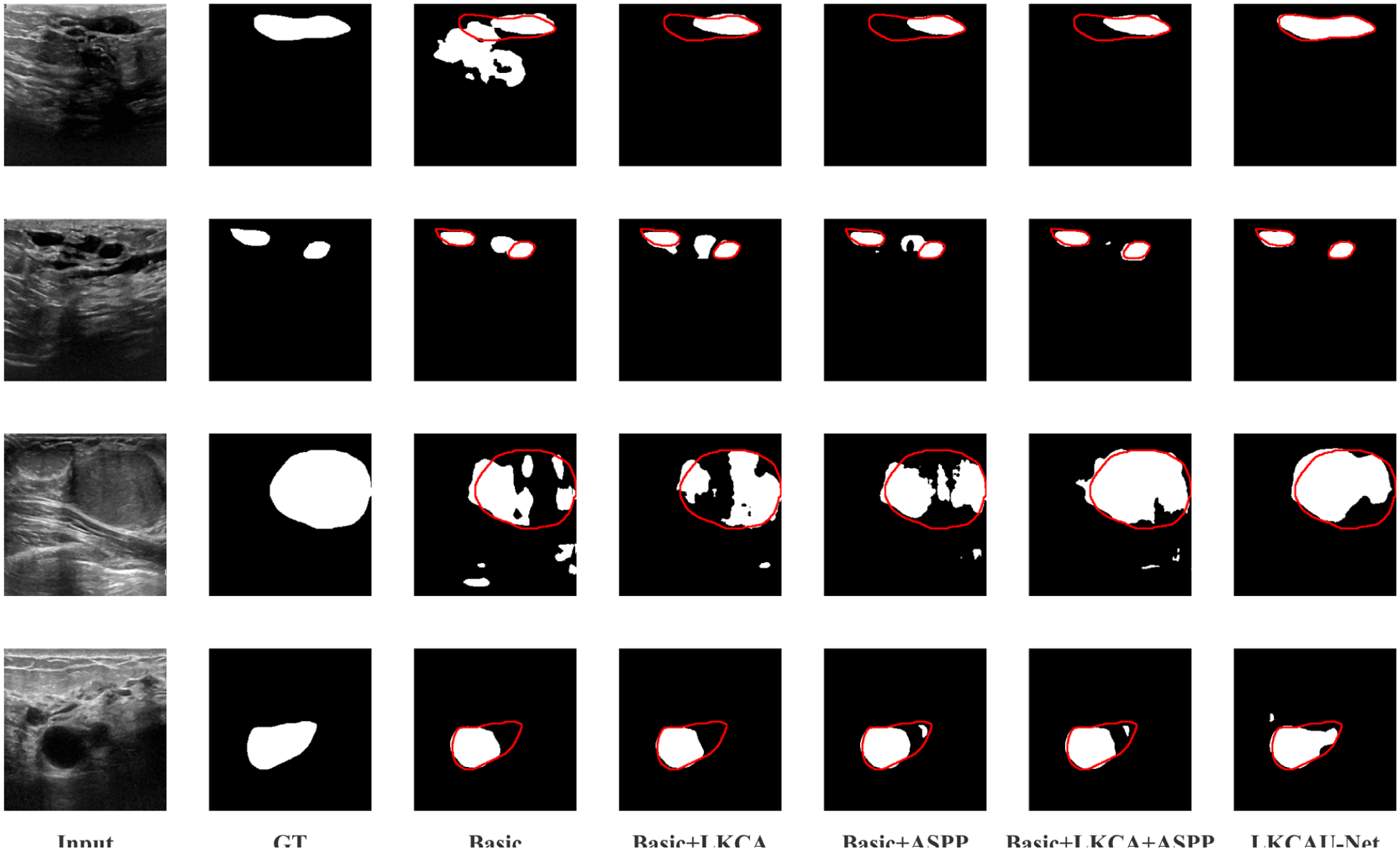
Representative visual outcomes from the module ablation analysis, based on four breast ultrasound images sourced from the BUSI dataset, illustrating the effect of each component.
LKCA module ablation
To further investigate the effectiveness of the LKCA module, additional ablation experiments are conducted on the BUSI dataset to evaluate two key design components within LKCA: the convolution structure in the LKSA module and the CA mechanism. Three configurations are considered: the full LKCA configuration, the configuration in which the proposed
The Ablation of the LKCA Module, Comparing Different Configurations of the LKCA Architecture, Including the Removal of the
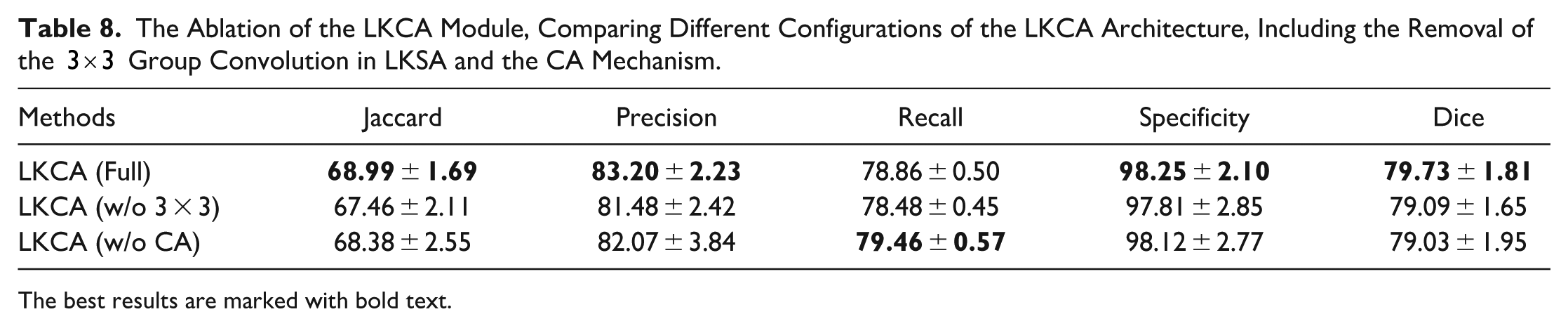
The best results are marked with bold text.
The results show that the complete LKCA configuration achieves the best performance across most evaluation metrics. Compared with the variant using conventional convolutions, the introduction of group convolutions in the LKSA module improves the Dice score from 79.09 to 79.73 and increases the IoU from 67.46 to 68.99. This improvement indicates that the convolution design in the large-kernel spatial attention module plays an important role in segmentation performance. By expanding the effective receptive field while maintaining relatively low computational complexity, group convolutions enable the network to capture richer spatial contextual information. In breast ultrasound images, where tumor boundaries are often ambiguous, such contextual modeling is critical for accurate segmentation.
A similar trend can be observed for the CA mechanism. By introducing the CA module, the Dice score increases from 79.03 to 79.73, and the IoU improves from 68.38 to 68.99. These results demonstrate the effectiveness of the CA mechanism in enhancing segmentation performance. The CA mechanism encodes spatial positional information by decomposing global pooling into two one-dimensional feature encodings along the horizontal and vertical directions, enabling the model to capture long-range dependencies while preserving precise location information. This design allows the network to focus more accurately on spatially relevant regions.
However, removing the CA mechanism results in an increase in the recall score. This phenomenon may be related to the stronger spatial localization. By embedding positional information into channel attention, the CA mechanism encourages the network to focus more precisely on spatially relevant regions and suppress background interference. While this improves the model’s ability to distinguish lesion and non-lesion regions, it may also lead to more conservative predictions in areas with ambiguous boundaries. As a result, some subtle lesion regions may not be fully captured, resulting in a marginal decrease in recall.
Overall, these results verify the complementary contributions of the two components within the LKCA module. The LKSA module enhances spatial context modeling by enlarging the receptive field, while the CA mechanism improves spatial localization by embedding positional information into channel attention. The combination of these two mechanisms enables the network to simultaneously capture long-range contextual dependencies and precise spatial features, thereby improving the accuracy and robustness of breast tumor segmentation in ultrasound images.
Depth ablation
To investigate the influence of network depth, we conducted depth ablation experiments on four datasets: BUSI, Dataset B, BUSBRA and QAMEBI. As illustrated in Figure 8, the segmentation performance generally improves as the network depth increases from 5 to 8 layers across all datasets. The best performance is consistently achieved when the depth reaches eight layers, yielding Dice scores of 79.73, 82.15, 90.85 and 88.15 on BUSI, DatasetB, BUSBRA and QAMEBI, respectively. When the depth is further increased to nine layers, the performance declines on all datasets, indicating that excessively deep architectures may introduce redundant parameters and reduce training stability. These results demonstrate that an eight-layer architecture provides a balanced trade-off between representational capacity and optimization stability, leading to the most reliable segmentation performance.
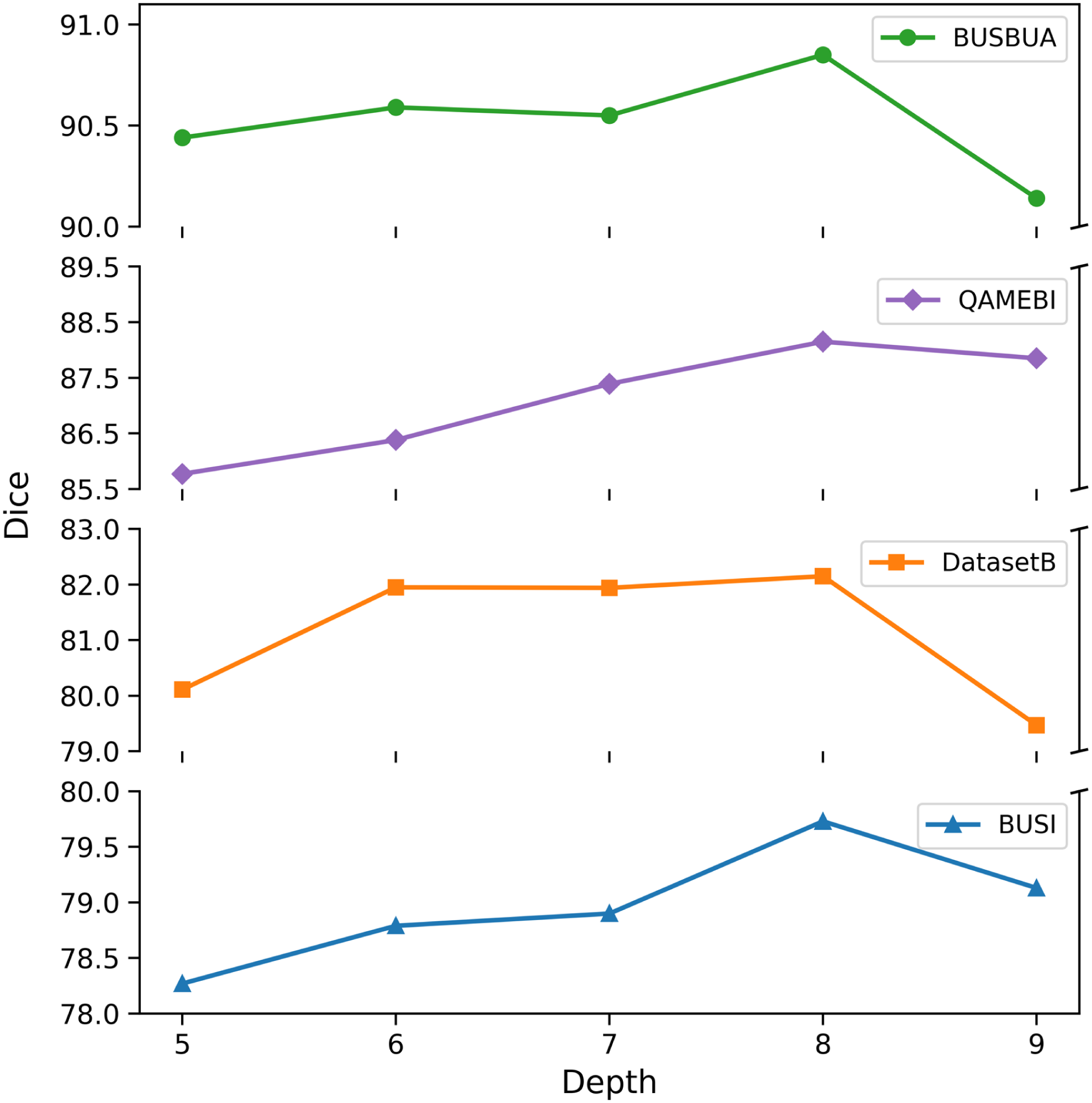
The ablation of increasing the depth of network on the segmentation results of BUSI, DatasetB, BUSBRA and QAMEBI.
Figure 9 further provides visual comparisons of segmentation results across different depths using representative samples from the BUSI dataset, clearly demonstrating that the eight-layer model produces the most accurate and reliable outcomes. Specifically, in the first, second, and fourth examples, the 5-layer, 6-layer, 7-layer, and 9-layer models all misidentified non-tumor regions as tumor areas, while the 8-layer model accurately segmented the true tumor regions. In the third example, although all models roughly identified the tumor area, the 5-layer, 6-layer, 7-layer, and 9-layer configurations failed to delineate the tumor boundaries precisely. In contrast, the 8-layer model achieved significantly better edge segmentation.
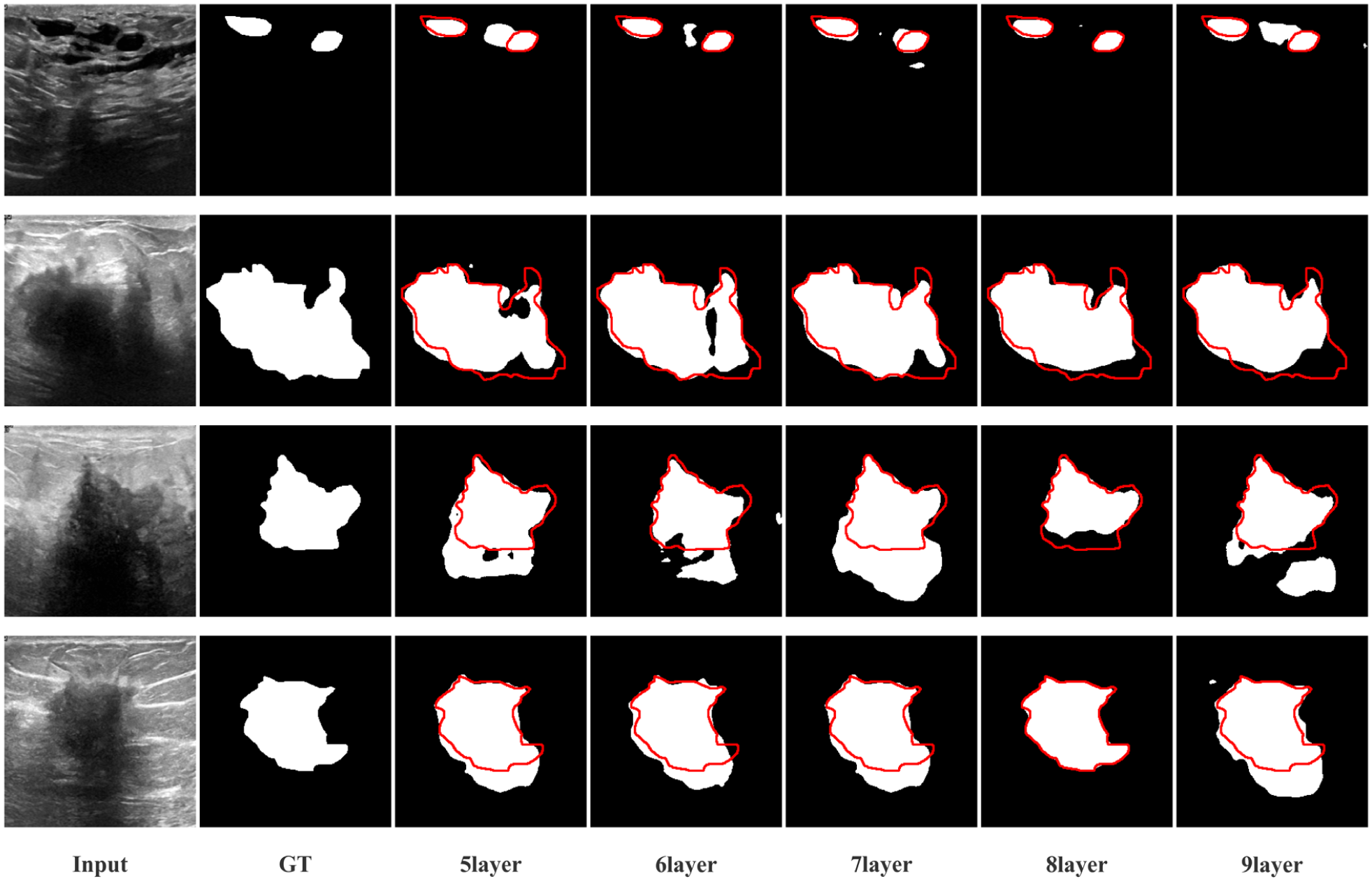
Representative visual results from the depth ablation experiments, demonstrated using four breast ultrasound images selected from the BUSI dataset to highlight the impact of network depth.
These findings validate that appropriately increasing the network depth substantially enhances the model’s ability to capture complex spatial features, thereby improving segmentation performance in breast tumor analysis. Based on these observations, we adopt the eight-layer configuration as the final architecture of our model.
Computational Complexity Analysis
To evaluate the computational complexity of the proposed model, this section analyzes the number of parameters (Params), floating-point operations (FLOPs) and Computational Time of different architectural configurations. These configurations correspond to the models used in the module ablation study.
Table 9 reports the Params, FLOPs and Computational Time of different model architectures. When the ASPP module is introduced, Params increase from 38.48 M to 47.40 M, corresponding to an increase of 23.2%, while FLOPs increase from 260.03 G to 277.74 G, corresponding to an increase of 6.8%. The Computational Time increases from 141.93 to 146.46 ms, corresponding to an increase of 3.2%. This increase mainly results from the additional multi-branch atrous convolution operations within the ASPP module, which enhance the network’s ability to capture multi-scale contextual information. Meanwhile, as shown in Table 5, the Dice score improves from 77.02 to 77.58, indicating that the moderate increase in model complexity effectively improves the model’s ability to capture tumor structures at different scales and leads to improved segmentation performance.
Computational Complexity Comparison of Different Architectural Configurations Corresponding to the Module Ablation Study, Reporting the Number of Parameters (Params), Floating-Point Operations (FLOPs) and Computational Time.
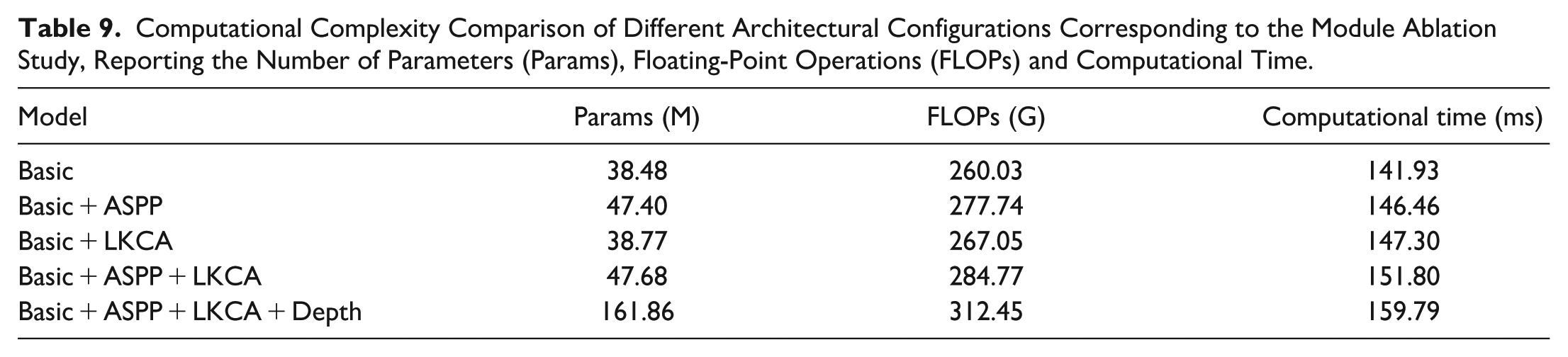
When the LKCA module is introduced alone, Params increase from 38.48 M to 38.77 M, corresponding to an increase of only 0.7%, while FLOPs increase from 260.03 G to 267.05 G, corresponding to an increase of 2.7%. The Computational Time increases from 141.93 to 147.30 ms, corresponding to an increase of 3.8%. Despite this minimal overhead, the Dice score still improves from 77.02 to 77.31. These results indicate that the LKCA module enhances spatial context modeling and positional feature representation while introducing only negligible additional computational overhead.
When both the ASPP and LKCA modules are incorporated, Params increase to 47.68 M and FLOPs increase to 284.77 G, corresponding to increases of 23.9% and 9.5% relative to the baseline model. The Computational Time increases from 141.93 to 151.80 ms, corresponding to an increase of 6.9%. At the same time, the Dice score further improves to 78.27, representing an improvement of 1.25 compared with the baseline model. These results indicate that the two modules complement each other in spatial feature modeling and multi-scale contextual perception, enabling noticeable segmentation performance gains with a moderate increase in computational complexity.
In the final architecture, a deeper encoder–decoder structure is introduced to strengthen hierarchical feature representation. Compared with the Basic+ASPP+LKCA configuration, Params increase from 47.68 M to 161.86 M, corresponding to an increase of 239.4%, while FLOPs increase from 284.77 G to 312.45 G, corresponding to an increase of 9.7%. The Computational Time increases from 151.80 to 159.79 ms, corresponding to an increase of 5.3%. The substantial increase in Params mainly results from the adoption of an eight-layer encoder–decoder architecture, which introduces additional convolutional blocks and higher-dimensional feature channels in deeper stages. However, the increase in FLOPs and Computational Time remains relatively moderate, indicating that the deeper architecture primarily enhances representational capacity rather than proportionally increasing computational operations. This is because the deeper layers mainly operate on progressively downsampled feature maps, where the spatial resolution becomes smaller and the computational cost of convolution is therefore reduced.
More importantly, as shown in Table 5, introducing the deeper architecture further improves the Dice score from 78.27 to 79.73, achieving an improvement of 1.46. Considering the characteristics of breast ultrasound images, which often exhibit low contrast, blurred tumor boundaries, and heterogeneous lesion morphology, stronger hierarchical feature extraction is necessary to capture both global contextual information and fine-grained structural details. The deeper architecture enables the network to integrate multi-level semantic features more effectively, thereby improving tumor boundary delineation and segmentation robustness.
Overall, although the final architecture introduces additional Params due to the deeper network structure, the corresponding increase in FLOPs and Computational Time remains relatively moderate. More importantly, the segmentation performance improvements shown in Table 5 demonstrate that the increased model capacity significantly enhances the accuracy and reliability of breast tumor segmentation. Therefore, the proposed architecture improves segmentation performance while introducing only a moderate increase in computational complexity.
Furthermore, it should be noted that the primary objective of this study is to improve the accuracy and robustness of breast ultrasound image segmentation rather than to develop a lightweight model. In complex medical imaging scenarios, moderately increasing model capacity to obtain more reliable segmentation performance represents a reasonable and necessary design choice.
Discussion
These results clearly show that our proposed model outperforms existing methods in multiple key indicators such as Jaccard, Dice, Accuracy and Specificity, showing excellent segmentation performance. However, false detections and missed detections are more specific and severe problems faced by ultrasound image segmentation in clinical applications, because they are directly related to the accuracy and completeness of lesion identification. To this end, we will further explore the actual effect of the model in reducing false detections and missed detections in this section.
False detections refer to the misidentification of normal tissue as a tumor area, resulting in over-segmentation, which in turn increases the risk of misdiagnosis, usually manifested as a false positive. 49 In model evaluation, accuracy and specificity can effectively reflect its ability to control false detections. The experimental results show that on Dataset B, the accuracy of the model was improved to 87.97%, which was 4.3% higher than nnU-Net’s 84.33%, and the specificity was also improved from 99.36% to 99.49%. On the BUSI dataset, the accuracy of the model was improved to 83.20%, which was 5.6% higher than nnU-Net’s 77.64%, and the specificity was also improved from 97.75% to 98.25%. On the QAMEBI dataset, the accuracy of the model was improved to 89.93%, which was 0.3% higher than nnU-Net’s 89.60%, and the specificity was also improved from 97.65% to 99.49%. These results fully demonstrate that LKCAU-Net has significant advantages in reducing the risk of misdiagnosis.
This performance improvement is primarily attributed to several architectural-level optimizations. As demonstrated by the module ablation results in Table 5, the inclusion of the LKCA module increased specificity from 97.75% to 97.80%. By integrating large-kernel convolution with a coordinate attention mechanism, the LKCA module significantly enhances the model’s ability to capture long-range dependencies and encode spatial location information. The large-kernel spatial attention expands the model’s receptive field, enabling it to capture richer contextual cues and better distinguish between lesion and non-lesion regions. Meanwhile, the coordinate attention mechanism introduces explicit positional signals, which strengthen the model’s focus on tumor boundaries. This synergy between contextual semantic enhancement and spatial localization refinement effectively reduces the likelihood of misidentifying background regions with texture similarities, thereby lowering the false positive rate.
Furthermore, the addition of the ASPP module alone leads to a notable improvement in segmentation performance, with accuracy rising from 78.73% to 81.64% and specificity increasing from 97.75% to 97.97%. ASPP enhances the model’s ability to capture multi-scale features by applying parallel convolutions with varying dilation rates. This allows the network to more accurately segment tumors with diverse shapes, sizes, and blurred boundaries. Its multi-scale perception capability also mitigates the impact of local noise and structural irregularities, reducing the risk of erroneous segmentation.
Building on the foundation of LKCA and ASPP, further increasing the network depth elevates accuracy and specificity to 83.20% and 98.25%, respectively—representing improvements of 3.8% and 0.28% over the model with only LKCA and ASPP (accuracy of 80.12%, specificity of 97.97%). The deeper architecture provides the model with stronger representational power and more comprehensive semantic understanding. In breast ultrasound images, tumor regions often exhibit complex boundaries and atypical morphologies. A deeper network enables better integration of high-level global context with fine-grained local details, improving lesion recognition. At the same time, the increased depth helps to construct more sophisticated decision boundaries, enhancing the model’s discrimination capability in non-lesion areas and further reducing false positives.
In summary, the synergistic integration of the LKCA and ASPP modules, combined with increased network depth, not only boosts the model’s sensitivity to lesion regions but also significantly improves its suppression of non-lesion areas. This leads to a substantial reduction in false detections and improves the overall accuracy and robustness of breast tumor segmentation in ultrasound images.
In contrast, missed detections refer to cases in which the model fails to identify actual lesion regions, leading to under-segmentation and a potentially increased risk of missed diagnoses. 49 This issue is typically reflected by a lower recall value, as it corresponds to false negative predictions. Although LKCAU-Net improves recall compared with the baseline model nnU-Net, 16 increasing from 74.74% to 78.86% as shown in Table 4, a performance gap still remains compared with AAU-Net. 33 On Dataset B, 7 LKCAU-Net achieves a recall of 79.37%, which is lower than the 82.22% reported by AAU-Net. Similarly, on the BUSI dataset, 9 LKCAU-Net achieves a recall of 78.86%, which is still below the 81.10% obtained by AAU-Net.
In this study, samples with missed detections mainly refer to cases in which the recall value is noticeably lower than the dataset average while other evaluation metrics, such as precision and specificity, remain close to their average levels. These samples are therefore more likely associated with missed lesion regions rather than excessive false positive predictions. As illustrated in Figure 10, the predicted masks tend to capture the main lesion regions but fail to fully cover the complete lesion extent, especially along the boundaries. The red contours, which represent the ground truth boundaries, clearly reveal that parts of the lesions are not detected by the model, indicating under-segmentation.
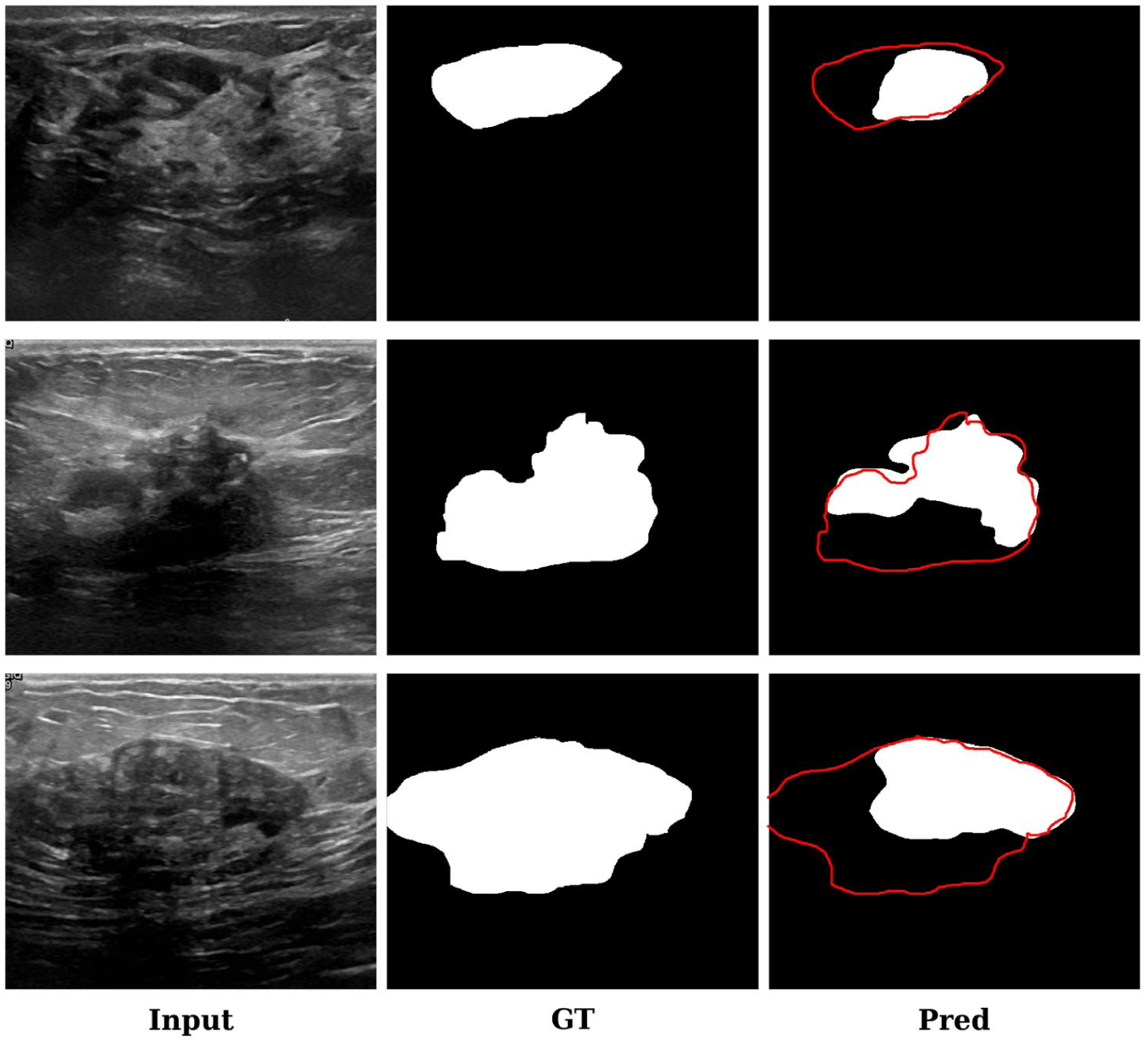
Representative visual examples of missed detections, demonstrated using selected breast ultrasound images from the BUSI dataset. From left to right: ultrasound input images, ground truth (GT) masks, and predictions from LKCAU-Net. The red contours denote the ground truth boundaries overlaid on the predictions.
A qualitative inspection of these samples suggests that many missed detections occur in regions where lesion boundaries are extremely blurred or where tumor contrast is very low relative to the surrounding tissues. Under such conditions, the visual appearance of lesions becomes highly similar to adjacent tissue structures, making it challenging for the model to reliably distinguish subtle tumor regions.
This observation may also be related to the ablation results presented in Table 6. As shown in the LKCA module ablation experiment, removing the CA mechanism leads to a slight increase in the recall score. The CA mechanism introduces positional information into channel attention, which may enhance the network’s spatial awareness and enable it to focus more accurately on spatially relevant regions while suppressing background interference. While this improved localization capability can help reduce false positives and enhance segmentation reliability, it may also encourage the model to adopt a more conservative segmentation strategy. In regions where tumor boundaries are ambiguous or contrast is low, such conservative predictions may fail to fully capture subtle lesion areas, which could partly explain the marginal reduction in recall.
To further improve the overall performance of the model, especially in reducing missed detections, future research may explore more effective loss function designs, 50 including both the selection of appropriate loss functions and the adjustment of loss weight configurations. For example, combining Dice Loss with Focal Loss 51 may enhance the model’s attention to difficult-to-separate regions. In addition, introducing an adaptive threshold mechanism 52 or a multi-stage segmentation strategy 53 may strengthen the model’s response to low-contrast lesions. Furthermore, integrating multimodal information, such as ultrasound elastography imaging, 54 may further improve the model’s ability to identify potential lesions, thereby reducing the risk of missed detections and improving overall segmentation performance.
In summary, LKCAU-Net performs well in false positive control. With precise spatial modeling and multi-scale feature fusion, it effectively reduces the false positive rate. However, in areas with blurred boundaries or low contrast, the model still has a certain risk of missed detection, resulting in a slightly lower recall rate. This shows that its segmentation strategy is conservative and needs to be further optimized to balance accuracy and completeness. In the future, the model’s ability to identify potential lesions can be improved by improving the loss function, introducing adaptive strategies or multimodal information, thereby achieving a more robust segmentation effect.
Conclusion
In this study, we proposed LKCAU-Net, a novel hybrid segmentation framework designed to reduce false detections and missed detections in breast ultrasound image segmentation. By embedding the Large Kernel Coordinate Attention (LKCA) module and the Atrous Spatial Pyramid Pooling (ASPP) module into a deep U-Net architecture, our model effectively enhances spatial localization, strengthens contextual feature extraction, and improves tumor detection accuracy.
Comprehensive experiments on four widely used public BUS datasets, including BUSI, Dataset B, BUSBRA and QAMEBI, demonstrate the superiority of LKCAU-Net over existing state-of-the-art segmentation models. Our approach consistently achieves higher scores in core metrics such as Dice coefficient, Jaccard index, Precision, and Specificity, reflecting its robust performance in accurate tumor delineation and false detection reduction. However, the slightly lower recall observed across datasets suggests a tendency toward missed detections, particularly in low-contrast or highly irregular tumor regions. This limitation highlights the need for further refinement in sensitivity-oriented aspects, such as incorporating adaptive thresholding or multi-stage segmentation strategies.
Overall, the results validate the effectiveness of the LKCAU-Net design, which integrates large receptive fields, positional attention, and multi-scale contextual learning to better capture complex tumor characteristics. This work provides a feasible and impactful solution for improving breast cancer segmentation, contributing significantly to early detection and effective clinical management.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.