
Abstract
This study looks at the interactions between health workers, physical space, surgical tools, and the “patient-body” in an operating theater. My aim is to explore the approaches of Katz, Rawlings, and Collins and to show that when rituals, restrictive entrance procedures, and clothing requirements are not in place, when rules are not observed for reasons that this article addresses, the boundary between the operating theater and its surroundings blurs. It becomes a trivialized space. Data were collected in the regional hospital of one major town of the Extrême Nord of Cameroon. I describe a context of crisis and a lack of equipment and personnel that narrow the boundaries of the operating room (the limits of which are supposed to be kept sterile and isolated) but do not erase them. Restrictive entrance procedures, clothing requirements, rituals, and rules that are supposed to separate the operating theater from its surroundings, as Katz has shown, are not observed. Instead, the theater is connected to its surroundings through an “intriguing combination of practices” consistent with the analyses of Rawling and Collins. Thus, the operating theater is not a closed and limited area inside the hospital that can be completely isolated from its surroundings. There is continuity between the interior and the exterior.
Introduction
The operating room is familiar to many people through media images. Surgeons seem willing to allow television into their theaters, while dramas set in hospitals make use of the operating theater’s physical organization and unusual dress codes (Fox 1997). However, observational studies of operating theaters are relatively scarce, as Hirschauer (1991) also noticed.
Goffman (2002) studied role distance in the operating theater, and the surgeon’s jocular self-presentation as a means of making subordinate team members accept the surgical hierarchy. Katz (1981) analyzed the elaborate rituals and technical procedures of the modern hospital operating room, and argued that even though they are manifestly designed to prevent infection, they better serve certain latent functions. They contribute to the efficiency of surgery by granting autonomy of action to the participants and enabling them to function in circumstances of ambiguity. Both Cassel (1986, 1987, 1991) and Pouchelle (2007) analyzed the surgeons’ work and the personality traits it requires. Rawlings (1989) studied the symbolism of dirt and cleanliness and the symbolic use of organizational rules in a Theater Sterile Services Unit (TSSU), a setting designed to produce and maintain highest standards of hygiene. Hirschauer (1991) described the surgical procedure as an encounter of two “disciplined bodies” (a “parceled patient-body” and “an aggregated surgeon-body”). Collins (1994) compared surgery to other assaults on the body in a variety of contexts, extending the depersonalization thesis of Hirschauer. Fox (1997) studied the operating theater and its built environment to explore the relationship of the physical layout with the interactions that take place within it. Finally, Zolesio (2009) examined some of the gender issues related to the profession of surgery.
For the current study, the most relevant works are Katz’s (1981) analysis of rituals in the operating room, Rawlings’s (1989) study of the symbolic aspects of dirt and cleanliness in a TSSU and Collins’s (1994) study of surgery, mainly because of their dynamic perspectives. The current study describes interactions between health workers, the physical environment, surgical tools, and the patient in an operating theater, while taking into account the specific economic context in which these interactions occur. My aim is to explore three specific ideas and their larger implications, drawn from the work of Katz (1981), Collins (1994), and Rawlings (1989): Rituals, restrictive entrance procedures, and clothing requirements help establish the operating room as a separate place, discontinuous from its surroundings; in doing so, they define categories of appropriate and inappropriate behavior (Katz 1981). Clothing requirements, entrance procedures, and rituals in the operating room have the effect of “making” the activity of surgery “full of germs” (Collins 1994, 318). “The existence of a set of rules which is technically based and organizationally administered inherently give[s] rise to the possibility of their differential observation” (Rawlings 1989, 288). Consequently, as I will try to show, when rituals, restrictive entrance procedures, and clothing requirements are not in place, and when rules are not observed for the various reasons that this article addresses, boundaries blur between the operating theater and its surroundings; the theater becomes trivialized, a common space where “intriguing combinations of practices” occur (Mol 2009) as doctors, nurses, and anesthetists tinker to perform surgeries in a context of poverty, lack of equipments, and human resources.
Method
My data were collected in the Extrême Nord region of Cameroon, where a large public hospital in one of the major towns served as the study site. 1 This hospital draws patients from the region and from neighboring countries, mainly Chad. A total of 102 people work in the hospital. These include three general practitioners and three specialists (gynecologist, urologist, and radiologist); 2 the other 96 staff members are nurses, midwives, nursing assistants, laboratory technicians, and administrative staff. I have chosen not to identify the informants, the town, or the hospital in which the study was conducted.
By way of background, this was my third fieldwork visit in the hospital. I had no background in medical science when I started doing fieldwork there in 2005 for my PhD dissertation in social anthropology. 3 During my fieldwork, I observed health workers trying to manage and adjust to their poor working conditions, which included inadequate working space, lack of equipment, role conflict, lack of rewards and fairness, and so on, all of which are factors that cause burnout (Gillespie and Cohen 1984; Maslach and Leiter 1997). Taking into account the links between tuberculosis and AIDS that have now been widely studied (Méda et al. 2013; Daftary and Padayatchi 2012; Chum et al. 1996, among others), I proposed a postdoctoral research project aimed at testing the hypothesis of burnout syndrome among health workers (Maslach and Leiter 1997; Truchot 2004), and its impact on care for people with HIV/AIDS. The project received the requested funding 4 and I went back to the same hospital in 2007. I was also involved in the evaluation of two projects implemented in this town and hospital. One of them focused on the management of obstetric emergency care in 2006, and the other, in 2009, on access to reproductive health care. 5,6 Since 2011, I have been the principal investigator of a research project funded by the Fondation de France. 7 These experiences have allowed me to become familiar with the language, tools, and practices of medicine in this resource-poor country. They have also helped me to build relations of confidence with health workers and administrative staff, which is a great asset. While all of these have contributed to my analyses, the data presented in this article were gathered during my third stay in the town. Throughout my time in the field, I relied on observations, in-depth interviews, and informal interviews as research tools.
Observations
With the approval of the hospital administration and the chief surgeon, I was able to observe all types of surgical procedures, daily hospital rounds, and the chief surgeon’s consultations. I did not observe the anesthetists “disciplining the patient-body to become immobilized” (Hirschauer 1991, 286). Rather, I chose to wait in the operating theaters, mainly out of a sense of decency. I was sometimes asked to hand over gloves, gowns, towels, and antiseptics, open up packages of sterile instruments, remove an electric cord, answer the telephone, move a cell phone closer to the surgeon’s ear, and other sundry tasks. I took notes that became a “fieldwork diary.” The observation period was also used to collect health workers’ comments on their working conditions through informal interviews.
Interviews
Interviews with doctors, nurses, and nursing assistants took place as I accompanied them in the course of their duties. Usually, I asked questions about their roles and tasks; these prompted discussion of issues related to equipment, the working environment and working conditions in general. As the observations took place over a prolonged period of time, these informal interviews became friendly conversations. I relied heavily on these informal interviews, listening to what people were saying and sometimes asking questions as I observed their daily life at work. In contrast, in-depth interviews with heads of services and their assistants were generally arranged as formal, scheduled meetings with informants; interview guides were used and the interviews were recorded and transcribed verbatim. Additional data were collected in focus group discussions.
Focus Group Discussions
Focus groups took place spontaneously as workers congregated on a veranda during rest periods. I both listened to discussions (focusing on professional status, working conditions, and tensions with colleagues or family members) and prompted people to talk about issues related to my topic. The groups consisted of four to six persons. As the discussions took place spontaneously, I choose not to record them in order to maintain the flow. I took notes and subsequently explored key issues more deeply during in-depth or informal interviews. Data were coded and analyzed thematically. The following section presents the results of this work and is divided into three parts.
The first part describes the general context and the specificities of the Extrême Nord in terms of health services provision. This background gives insight into the structural constraints that influence the working environment in the hospital. The second part describes the hospital and its surgical facility, showing how structural constraints are shaped at a local level and how this contributes to creating continuity (rather than discontinuity) between the operating theater and its surroundings. The third part looks at surgery as an activity and how it is performed in this context. I show how the constraints as well as the tools, physical space, human agency, and the technical skills required for surgery contribute to redefining roles, and to shaping both interactions and the overall process of surgeries.
Structural Constraints
The Health Care System in Cameroon
The Cameroonian health system consists of a general service providing prevention and care for prevailing health problems, and vertical health programs implemented for specific health conditions such as HIV/AIDS, tuberculosis, malaria, diabetes, and so on. The country has more than 1,500 health facilities (Minsanté 2006), most of which are underequipped; this lack of equipment has been discussed since the late 1970s (Médard 1977). The health system is pluralistic, with the characteristics of an “unregulated” market as Standing and Chowdhury (2008) described in their study of Bangladesh. 8 Public, private, traditional providers, and nongovernmental organizations (NGOs) function with varying “reach” and quality. The boundaries of the underfunded public sector are porous, with private doctors who maintain links with publicly owned medical facilities and public sector providers who work privately. There is a strong urban bias in the distribution of qualified staff, and it is difficult to retain them in rural postings. Many health workers are not physically in their posts, and problems such as informal payments and poor provider attitudes are common (Gruénais 2001; Okalla and LeVigouroux 2001; Nkollo and Claude 2007).
The economic crisis of the early 1990s resulted in a drastic reduction of the public health budget. Hiring was suspended for all categories of health workers apart from medical doctors; positions that opened up because of retirements or deaths were not renewed. In June 2000, staffing ratios were as follows: one physician per 10,083 inhabitants, one nurse per 2,249 inhabitants, and one nursing assistant per 3,000 inhabitants (Médard 2001; Okalla and LeVigouroux 2001; Minsanté 2002). 9 A recruitment of about 30,920 workers at all levels is estimated to be required to meet the health system’s needs (Nkollo and Claude 2007).
The economic crisis and Structural Adjustment Programs implemented in Cameroon also brought a decline in civil servants’ wages in general. Wages were increased in the early 2000s but are still perceived as insufficient (Beyeme Ondoua 2002). 10 Thus, many doctors provide care in private clinics in addition to their hospital duties. They also make it a priority to attend seminars organized to monitor vertical health programs. These seminars are perceived by health workers to be an attractive source of additional income, as participants’ per diems sometimes exceed their monthly wage. The specific relation of health workers to per diems in some African countries has been termed perdiemitis, and “acute perdiemitis” has been referred to as one of the most prevalent illnesses in African public health projects (Ridde 2010). It has been said to reduce the effectiveness of interventions, dilute health sector resources, and be a contributing factor in Africa’s expected failure to achieve the Millennium Development Goals by 2015. All these issues are exacerbated in the Extrême Nord.
The Punishment of Remoteness: Structural Constraints at a Local Level
The Extrême Nord is the most beautiful, populous (at least 17 percent of Cameroon’s estimated 18 million inhabitants live there) and poorest region of the country. 11 North–South connections (transportation and phone) and Internet access are difficult, and sometimes suspended. Cholera and meningitis strike the population regularly. For many Southerners, it is “a place to visit, but not to stay there,” as one of my informants put it. Civil servants from the South of the country perceive assignment to this province as punishment. Many arrive to take up their duties and immediately return to the capital where, while working in private clinics, they use their social networks to get a change of assignment. Those who stay there always have in mind “being ready to leave at any moment, without worrying about relocation.” Many await the day when they will leave the place definitively. As one of them put it emphatically, “I cannot lie. When I travel here from Yaoundé, I always have tears in my eyes. I feel like a man who is about to be thrown in prison. I look calm in the train but my heart bleeds. I speak to myself: ‘When will you go to back to Yaoundé definitively?’” This attitude of Southern civil servants to the Extrême Nord, which is not new, prompted the former head of the State, Ahmadou Ahidjo, to develop incentives in order to retain staff. During the grandes vacances (summer holidays), for example, the State provided an airplane ticket to staff from the South, so that they might visit their family members. But as a nurse at the hospital put it, “We need something to motivate us, but there is nothing.”
Moreover, working in the region deprives staff of additional income. The majority of physicians and some of the professional nurses who were working in Yaoundé and Douala before being assigned to the Extrême Nord expressed regret at having left. These cities host the most prestigious training institutions, reference hospitals, and private clinics of large capacity. Working in these facilities provides attractive additional incomes. “At the university hospital,” says a nurse, “everyone knows that a general consultation costs $2 and a specialist one $4. At the end of the month, this amount is shared by the team… Some nurses receive $400 in their share, and this does not include activities in private clinics. Do you think it’s for nothing that people do not want to come here?” These towns also host the health programs of international NGOs and international development agencies. When involved in these programs, one gains in experience, income, and symbolic recognition. In contrast, the Extrême Nord region is, to borrow from Blundo and Olivier de Sardan (2007), a place of dry, remote, isolated outposts, where the quality of life is poor, opportunities for enrichment limited, and one runs the risk of being forgotten by the hierarchy.
The mortality rate is the highest in the country, and the ratio of health workers to population (about 3,193,055 people) 12 is the lowest. For example, in 2004, there was one doctor for 73,553 inhabitants, one nurse for 6,403 inhabitants, whereas the means for the country are one physician per 26,483 inhabitants and one nurse for 2,202 inhabitants (Institut National de la Statistique du Cameroun 2004). Two years ago, there was one gynecologist for the entire province; today there is none. There is a horizontal service for general care and vertical health programs for specific conditions (HIV/AIDS, tuberculosis, and malaria). In the hospital where I did my fieldwork, a gynecologist, a urologist (chief surgeon), and a general surgeon use the operating theater. Beyond their work as specialists, they also give general consultations. Five nurses (men) and one volunteer (female), complete the team, two of whom are specialized in anesthesiology. Team schedules are rarely available because of absenteeism. Thus, the surgeons are often obliged to work with whichever team members are in the ward at a given moment. Sometimes, they are all present and the entire team will join the surgeon in the operating room. But at other moments, there is no one else on the ward. In one instance that I observed, the surgeon had to call on an anesthetist who was off duty.
There is also a chronic lack of equipment. It extends to items necessary for routine care activities and for daily life at work (running and potable water, toilets, textbooks, paper, pens, etc.), and obstructs the provision of care. On one occasion, for example, a patient was brought into the operating room, and the team was waiting for the surgeon. He entered the room, burst into anger, and demanded that the director of the hospital come and acknowledge the unacceptable state of the operating room before he started surgery.
Shortage of human resources and equipment, poor planning and poor communication within health facilities and health authorities, and conflicting relations with coworkers also contribute to a broader feeling of isolation (Tantchou 2007).
Physical Space: The Operating Theater in the Hospital
Prior (1988) has shown that the structure of a space can best be understood in relation to the discursive practices of which it forms a part. For example, hospital plans are records that encapsulate a genealogy of medical knowledge. The study of alterations in hospital and ward design can reveal changing objects of medical attention, or disclose principles concerning the conceptualization of disease and illness. Furthermore, elements of ward and hospital design are capable of revealing details concerning the manner in which diagnoses such as insanity or practices such as surgery were theorized in different decades. Thus, the architectural plan lays bare the spatial expressions in which medical knowledge and therapeutic practices are constituted. Space can also be revealing about human action, and about political and ideological relationships. For example, Prior suggests that a ward is a point for the intersection of social and medical practices. Originally, she noted, the design of the “pavilion” hospital was linked with the miasmic theory of disease. With the diffusion of “germ theory,” the ward design changed. The acceptance of this new theory found its initial expression in the design of the operating theater and the laboratory, and from there it moved outward and into the wards. The architecture of hospitals is thus inextricably linked with the forms of medical theorizing and medical practices that reigned at the time they were constructed, and all subsequent modifications to hospital design can be seen as a product of changes in medical discourse. Thus, she concluded, architectural features have no existence outside and beyond the forms of thought and practice that produced them (Prior 1988).
Fox’s (1997) analysis of “circuits of hygiene” in the operating theater is consistent with Prior’s ideas. From his perspective, there is congruity between architecture and the intended function of a space; architecture may make available to actors a set of signs with which they will support their discursive activities. It may also contribute to an understanding of things such as how to behave, who may behave in certain ways, and who is ascribed particular privileges. Thus, physical space may offer cues to actors as to how they might engage with the environment and with others.
In order to analyze the internal divisions and forms of categorization that are expressed in a hospital ward, and how actors engage with it and with others, we must turn neither to the computer nor to the conscious human actor, but to the fields of human thought and practice that are utilized in the very interiors we want to study (Prior 1988); the emphasis should be on the “reading” of spaces by actors (Fox 1997). This is the approach I have taken in my analysis of structural constraints, physical space, medical tools, and human agency in the operating theater of the regional hospital in Cameroon.
The operating theater is situated in the center of the hospital (Figure 1). One accesses the operating theater through two doors leading to two verandas (Figure 2). The first door leads to the sterilization room. Its veranda leads to the surgeon’s office. The chief surgeon usually leaves the ward through this door, which allows him to avoid patients’ family members who are awaiting the end of the procedure. The second door leads via a gloomy corridor to a veranda equipped with benches, where nurses sit during breaks. This door is the most frequently used. On the left side of the corridor are the chief nurse’s office and two recovery rooms. Usually, patients awaiting surgery lie there before the procedure. It is also in these rooms that the process of “disciplining the patient-body” for surgery (Hirschauer 1991) is performed. Each recovery room has two doorways. The first doorway links them to the scrubbing room. Only nurses use it, transporting patients from the recovery rooms to the operating theater and, at the end of the procedure, from the operating theater to the recovery rooms. The second doorway leads to a large courtyard connecting the surgical area to the high standing ward. This doorway is used by patients, family members, and visitors. On the right side of the gloomy corridor are the anesthetists’ office, a lounge for nurses, and the scrubbing room. One doorway on each side of the scrubbing room leads to an operating room.
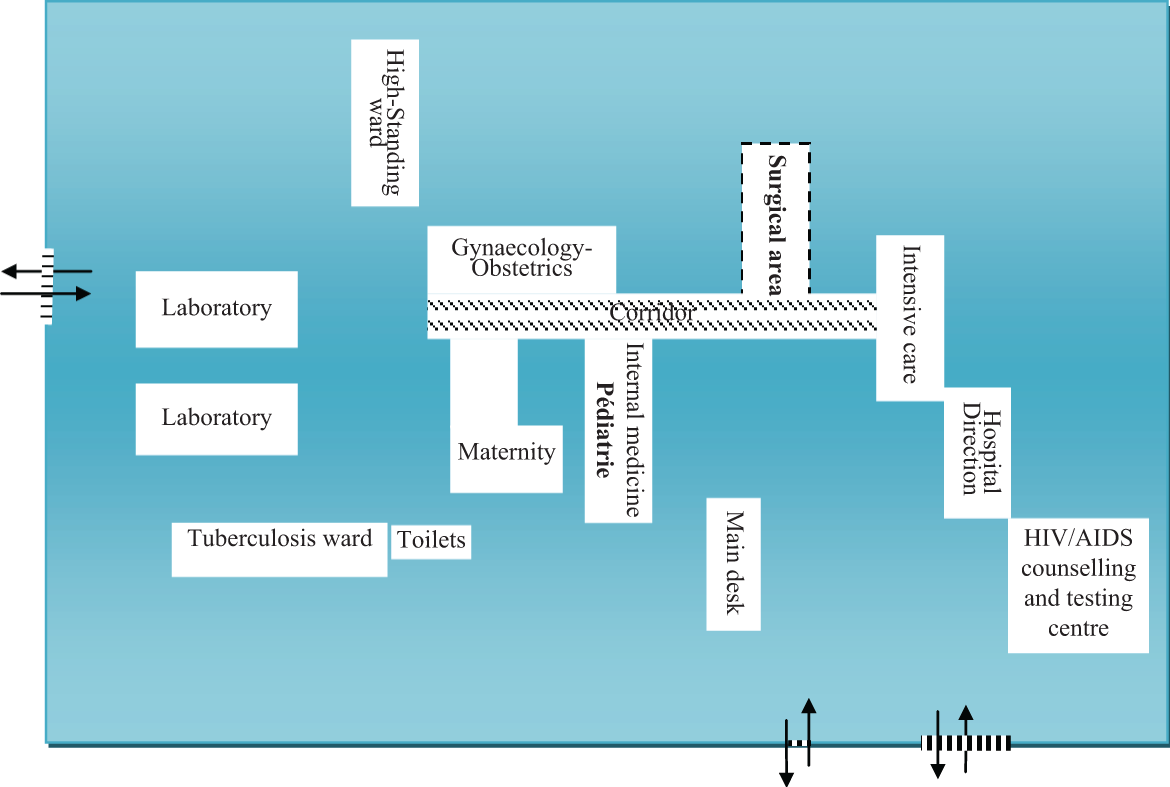
Surgical area in the hospital.

The operating theater.
My first contact with “surgical space” in the hospital was disconcerting (Figures 3 and 4), familiar though I was with operating theaters through pictures and TV dramas. Its very basic and rather dirty equipment contrasted starkly with the photos and televised images I was used to, making it look like a storage room for out-of-service or worn out furniture. The ward nurses did not hesitate to tell me, “If we were to comply with the [international] standards, our operating rooms would have been closed a long time ago.” Surgical equipment sets were incomplete, and the sterilizing machine dedicated to high-volume sterilizations was out of service. I wondered who was undergoing surgery in these rooms, for what reasons, and for which pathologies? These questions seemed all the more legitimate when I observed an encounter between the surgeon and a female patient. The surgeon said how lucky the patient was that he was available to save her and her community members’ lives. She replied scornfully, “Me? In there? Never! I go to Dubai”. 13

The sterilization room.

Operating room at the end of a procedure.
Could the rules to ensure asepsis and maintain sterility be respected in this environment, I asked myself? I also wondered what might explain the rare occurrence of postoperative infections, since I was aware that no incidents of postoperative infections were recorded in the ward registers. At this point, two interpretations to this apparent fact suggested themselves: the tight physical boundaries are sufficient to ensure the safety of surgeries; complications that occur after the patients have been dismissed are not dealt with or recorded as being the results of surgery and therefore are managed by other services or health facilities.
In any case, the head of service boasted about the performance of his service despite the poor working conditions. He said he was planning to write an article on surgical practice in resource-poor contexts to show that, even if the conditions were difficult and sometimes frustrating, he still succeeded in managing the situation and saving lives, which was ultimately what mattered.
Katz (1981) reminds us that despite its elaborate rituals and rigorous application of advanced scientific knowledge, infections do occur as a result of surgery. I asked myself if the procedures aiming at isolating and sterilizing the surgical area were related to the surgeon’s legal responsibility and to the obsession with risk that has become a major feature of contemporary Western societies (Beck 2003). I was aware of the observation of Collins (1994) that clinical sterility is inherently complex, and even if an essentially scientific issue, it is subject to local interpretations and adaptations to different contexts that do not have any scientifically proven basis. In line with Rawlings’s (1989, 284) research, it seemed to me that either my strict notions of clinical hygiene were correct and people were breaking the rules and putting patients at risk or the concepts themselves were more complicated than I had realized.
Marking Areas: Clothing Requirements and Entrance Procedures
In her study of rituals in operating rooms, Katz (1981, 336) noted that identification and separation of cleanliness and dirt are the most important principles in operating rooms. They govern the organization of surgeries, the spatial organization of rooms and objects, and the clothing worn, as well as most of the rituals. Restrictive entrance procedures and clothing requirements are designed to maintain cleanliness and prevent contamination in these areas. Entrance to the surgical area is restricted to those who are properly clothed and who are familiar with the rituals within. These include surgeons, anesthetists, pathologists, radiologists, operating room and recovery room nurses, student doctors, nurses, and ward orderlies who work in that area. All the people in the surgery area wear clothes that identify both their general role in the hospital and the specific areas within the surgical space that they are permitted to enter. One exception to these roles is the patient who is unfamiliar with the rituals. These restrictions impose a peculiar management of space in the operating theater and rooms. Thus, while walking toward the operating rooms, one moves from dirty into clean areas, with increasingly stringent rules regulating access and requirements regarding clothing (Katz 1981). This, as Hirschauer (1991) also notes, allows the complete separation of the operating theater from everyday situations.
According to the principles of sterility and contamination, Katz divided an operating theater into four areas: the “periphery,” “the outer area,” the “middle,” and the “innermost” areas.
Physical barriers separate these four areas; they function to prevent contamination entering from dirtier areas into cleaner ones, and from outside to inside. The periphery is the least clean area; it usually includes the offices of the anesthetists, dressing rooms for men and women, and lounges for nurses and doctors. To enter the periphery area, a person must wear a white jacket for identification as a member of the medical staff. The outer area is separated from the periphery by a sliding door. Entrance to the outer area is restricted to patients and to those medical personnel who wear blue or green costumes. A nurse can prevent the sliding door from opening if an unauthorized person tries to enter. The middle area consists of “aseptic cores.” They contain sterilizing machines, carts, and shelves containing surgical equipment, sheets, and towels. In order to enter an aseptic core, a person must wear a mask that covers the mouth and nose, coverings for shoes and hair, and a blue or green outfit. The innermost area contains the operating rooms and small laundry rooms (Figure 5). Katz did not mention clothing requirements for entering the operating room; however, following her argument, they ought to be similar to those required to enter the aseptic cores. In line with her conception of the operating theater based on notions of “cleanliness,” “dirt,” and entrance procedures that ideally should be applied, the operating theater in the Extrême Nord hospital can be schematized as shown in Figure 6. However, the clothing requirements, entrance procedures and rituals necessary to maintain a discontinuity between the operating theater and its surroundings can be seen to mal-function in this context, thus undermining the clean/dirty typology, and contribute to maintaining continuity between the operating theater and its surroundings.
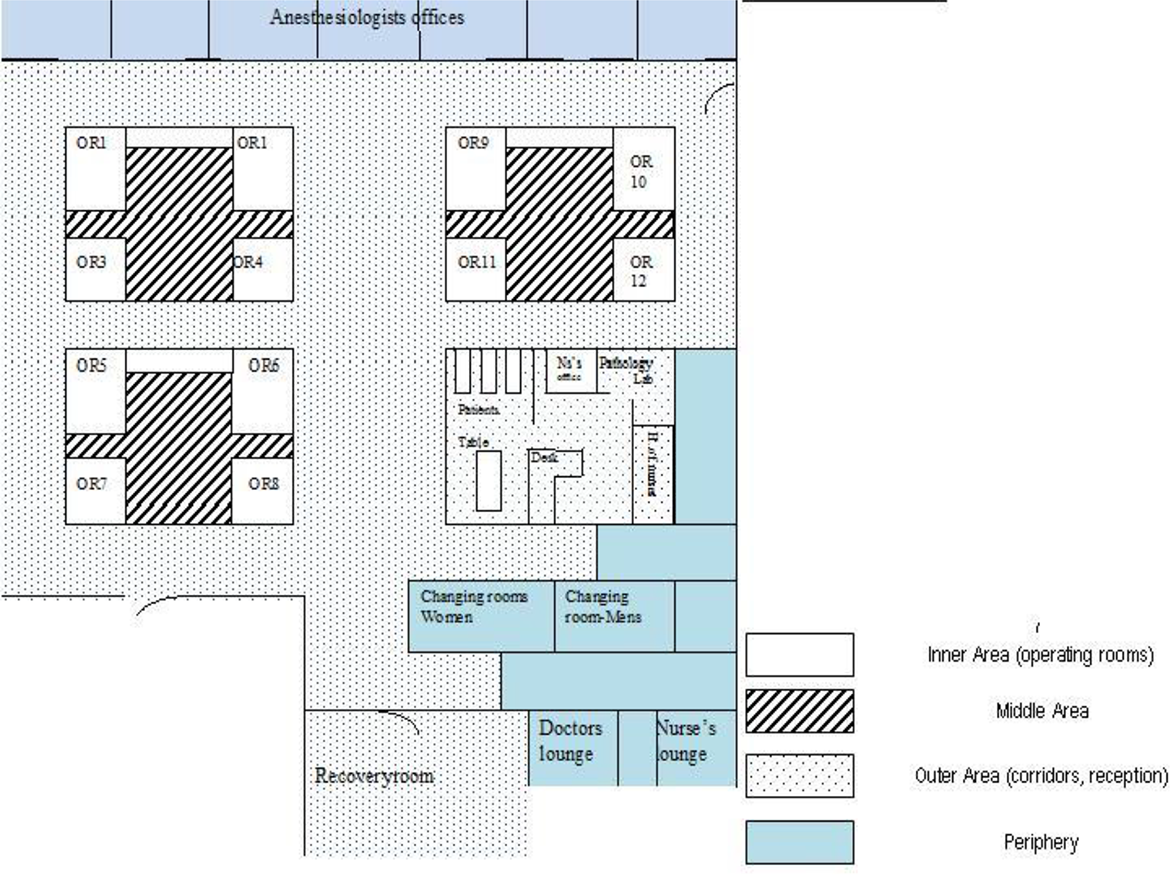
Operating theater.
The operating theater according to Katz (1981) categories.
The hospital does not provide nurses with the operating room clothing. Usually, they enter the operating room wearing their white jacket, which identifies them as members of the medical staff. At times, a nurse will wear the same disposable mask and headcap for several days. Indeed, were there a stringent regulation on clothing, only surgeons and possibly their assistants would have access to the operating rooms. In my own experience, I was instructed to wear a white coat, a covering for my hair, and a mask to cover my mouth and nose before entering the operating rooms. But I could not do so because they were not available. This forced me to keep at a distance from the operating table, in order to limit my exposure to blood and other fluids.
During one procedure, the surgeon’s assistant recalled the above-mentioned incident when the surgeon had angrily called for the hospital director to come and see the unacceptable state of the operating room. As they were discussing this, the assistant mentioned a man who had come to sell operating theater outfits. A complete set (green trousers and jacket, mask for mouth and nose, and headcap) was sold for US$33. “We bought nothing,” he said. “It is not our responsibility. There is a budget for it. So the man wasn’t successful with his business here. See, some of us don’t have even the white jacket, never mind the headcap. They have to start by giving white gowns to all of us.” He told the surgeon, “If you really want to apply the rules, you should ask your two anesthetists to get out because they are wearing neither a green gown nor a head-cap. Just ask them to get out, and let’s see who you’ll have left to work with!”
Implicit in this quote, and consistent with the data collected through my observations and informal interviews, is an accusation or suspicion of corruption against the hospital administration and the surgeon. This is not unique to this hospital. Several studies conducted among health workers in Africa address the issue of corruption and informal economic activities (McPake et al. 1999; Israr 2000; Jaffré and Olivier de Sardan 2003; Vidal, Salam Fall, and Gadou 2005; Hane 2007). Corruption is almost systemic in health facilities, as it is in all public services (Médard 1977, 1998, 2001). Tensions related to accusations and suspicions of corruption taint professional relations and collaboration between services (Tantchou 2007, forthcoming). Patients and family members are encouraged to pay the fee for surgeries directly to the surgeon, who is supposed to share the amount with the entire staff.
14
But he sometimes keeps the money for himself, and when asked by his colleagues for their share, he hands over an amount that is below what he really received. Unfortunately, for one reason or another, family members or patients may complain to the anesthetists or nurses about the amount they paid. Inevitably, they will be asked what they actually paid and there will generally be a mismatch with what the surgeon said. This frequently leads to tensions and quarrels. In the case of the hospital administration, the problem mainly concerns the unfair redistribution of shares, which fuels tensions (Tantchou forthcoming). Implicit in the assistant’s quote above are three assumptions: The hospital administration and chief surgeon have the responsibility and resources to furnish the team with sets of clothing. The hospital has a budget for this type of expenditure that must be used for this purpose. With the amount of money received from patients that he does not share, the surgeon could provide the entire team with appropriate clothing.
One day while I was onsite, the hospital received a visit from a European medical team. On this occasion, the gynecologist required that the European nurse, who wanted to attend surgeries and had previously been admitted to the operating room with her casual trousers and tee shirt, should wear the appropriate clothing. The nurse answered she did not have any of the clothing needed and was sent with a nursing assistant to the gynecologist’s secretary. 15 About thirty minutes later, she came back dressed as required, in green trousers and jacket, mask for nose and mouth, and hair covering. Only the appropriate shoes were lacking, so she entered the operating room in her normal shoes, which were uncovered.
But even when people were aware that they needed to be clothed appropriately before entering the operating room, the staff at the main entrance did not perceive it as a strict requirement. I observed one occasion when, at the time the gynecologist was removing a malignant tumor from a patient, the door to the operating room was suddenly opened by a colleague who wanted to make a rendezvous with him while he was in town. The gynecologist reminded him that he was not clothed appropriately, to which his colleague retorted that he had mentioned this to the nurse at the main entrance, and she answered that it was not a problem. In fact, in the operating room at that moment, the entire team apart from the surgeon and his assistant was not clothed appropriately. Nonetheless, they had been admitted and were working inside. From this point of view, the answer of the nurse at the entrance seems logical. Moreover, the gynecologist made no further comment and thus legitimized the answer. The visiting colleague left a few minutes later, having obtained an appointment.
Barbara Rawling’s (1989) study of the symbolism of dirt and cleanliness in a TSSU is helpful on this issue. She noted that the hygiene theories of microbiology and clinical sterility are fundamentally complex and science-based. In order to apply these theories to achieving and maintaining sterility, they must be translated into rules of good practice, on the assumption that if the rules are observed, the requirements of hygiene theory will be addressed properly. But the relationship between organizational rules and underlying concepts is a symbolic one (the rules stand for the values but do not fully describe them). Because of this indirect relationship, the staff who are involved in maintaining sterility treat the rules as practical issues that are invoked, suspended, or followed with reference to other contextual features. Thus, the meaning of a rule is not a stable feature external to the activities of the people concerned; rather, it is a matter for their situated practical judgments (p. 281). Someone who is well acquainted with the exceptions and qualifications of the underlying concepts does not need the rules to maintain the required standard of hygiene. For rules to be “acceptably” disregarded, those who police the rules must assume that certain people or categories of people possess the underlying knowledge to which the rules relate. One can therefore make the working assumption that a doctor who is seen disregarding the rules is doing so on the basis of technical knowledge, that is, he is assumed to know that the rules do not apply in the specific case, because he possesses the relevant technical knowledge. But there is no need for the rule-flouter to be a doctor; in fact, flouting a rule may be a sufficient indication to an observer that the flouter “knows what he or she is doing.” Thus, Rawlings suggests, a junior nurse might stick rigidly to the rules but be happy to let a senior nurse break them. A stranger may be “allowed” to break the rules on the tacit grounds that his behavior shows him to be “knowledgeable” or a “special case.” In summary, then, the existence of a set of rules which is technically based and organizationally administered gives rise to the possibility of their differential observation (Rawlings 1989, 288), as the paragraphs below will demonstrate.
Blurring Boundaries: Movement in the Operating Theater
Nurses, patients, and relatives who walk around the corridor rarely go beyond the anesthetists’ office if not invited. Equally, patients and family members who enter the sterilization room seldom venture beyond it. This behavior was also observed among nurses from the other wards. Sometimes, volunteers are assigned to the ward, but without precise tasks. 16 Hence, they attend surgeries of their choice. Their movements in the ward and the operating rooms are not subject to any control, nor is their clothing. An orderly is in charge of cleaning the rooms before and after surgeries, and of removing weeds around the ward grounds. He is also in charge of monitoring autoclaves in the sterilizing room (Figure 3). While cleaning and sweeping, he may be asked to help move a patient to the recovery room. 17 In doing so, he will enter and exit the operating room without taking any hygienic precautions. Occasionally, he will bring baby boys who have just been circumcised into the sterilization room in order to disinfect the wound, again without having to comply with any specific hygienic constraints.
Patients waiting for surgery or under postoperative monitoring are generally accompanied by one or several relatives who act as nursing auxiliaries. They help “their” patient to wash, take care of the meals, and administer drugs. As the ward does not offer any hosting facilities, they usually lay mattresses beside patients’ beds and spend the night there. Similar to Zaman’s (2004) findings in Bangladesh, such relatives in Cameroon receive all sorts of humiliation and criticism from the ward staff. The staff members say that relatives are unruly and hamper the normal flow of work. They are accused of stealing things from the ward, and of making it dirty. The staff members often complain about relatives’ noncompliance with the surgical team’s instructions. In fact, however, relatives have to leave the rooms when daily rounds start; they are also expected to facilitate the team’s movements in the rooms by removing their mattresses, making sure the patients have their breakfast, washing up and arranging dishes and so on, before the surgeon and his team enter the rooms. At the same time, nurses often do have to walk over relatives’ mats and find their way around thermoses and dirty or half-empty dishes. This is a great source of tension between patients, relatives, and staff who constantly have to ask them to “empty the floor of everything that is lying around and leave the room.” However, because some patients are unconscious or unable to speak French (the language used by health workers, especially those who are not native to the area), the team has to resort to relatives to translate or answer questions about the “case” (Has the patient eaten all of his or her meal? Did they sleep well? Have they complained about pain?). In this respect, I witnessed daily scenes when relatives were sent out of the ward in an unpleasant manner and called back shortly thereafter to answer the surgeon’s questions. In summary, although relatives have to exit the rooms when daily rounds start for practical reasons such as airing the room and permitting the team to move about easily, their presence is essential to patients and useful to surgeons.
Although they usually stay in the recovery rooms, relatives can also be seen in the corridor (the “outer area,” theoretically reserved to nurses) when they need information about medicine use, when a patient has been complaining about pain, or when a drip needs replacement. They can even be called into the scrubbing room (middle area) for several reasons. For example, when relatives go to the hospital pharmacy to purchase the products prescribed by the surgeon before surgery, they are given whatever thread and needles are available, even though these are not necessarily suitable for surgery (e.g., some needles and thread break more easily than others). Yet anesthetists, like most nurses, have stocks of frequently used products that they often sell to patients’ relatives. The surgeon may have to ask them (the anesthetist or nurse) to look for the right product in their stocks and for these products to be invoiced. When this happens, the patients’ relatives are invited to come to the door of the operating room to be informed about it. Just as the nurse at the main desk (who is supposed to “know the rules”) authorizes a “stranger” to enter the operating theater, the surgeon (also assumed to “know what he is doing”) is the one authorizing family members to enter the “inner space,” or calling the maintenance orderly into the operating theater to help bring a patient from the operating room to the recovery room. I would therefore agree with Rawlings that the concept of sterility has no meaning in isolation from the practices used for its accomplishment. As she says, “It is more revealing to study how standards are achieved and maintained than it is to take them for granted as resources for explaining organizational data” (Rawlings 1989, 279).
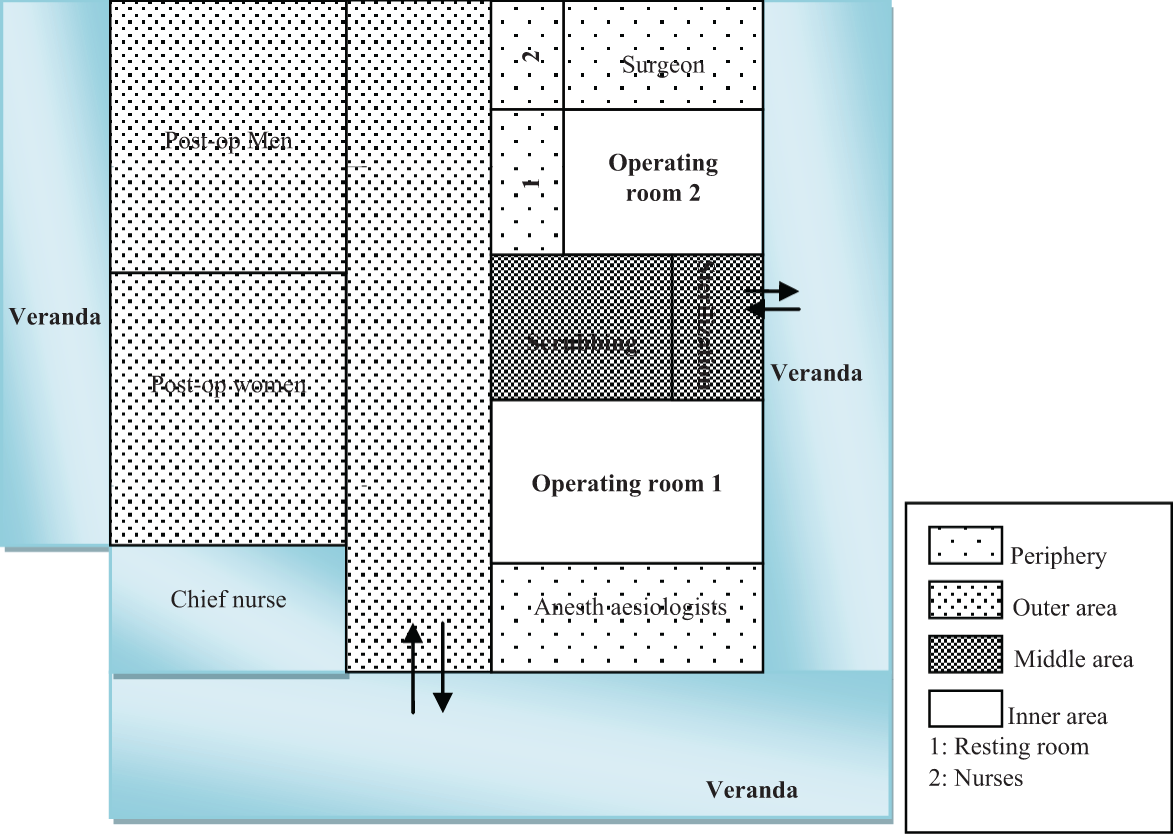
Taking into account clothing requirements and entrance restrictions applied in this operating theater on one hand, and Katz’s analyses on the other, the surgical area in the Extrême Nord hospital can be mapped as follows (see also Figure 7). There are three categories of area: The functional typology. The periphery with the postoperative rooms (open to health workers, patients, family members, and visitors), verandas and courtyard (spaces of sociability), and the surgeon’s office. The outer area with the corridor, anesthetists and nurses offices, and the scrubbing and sterilization rooms. The inner area with the operating rooms.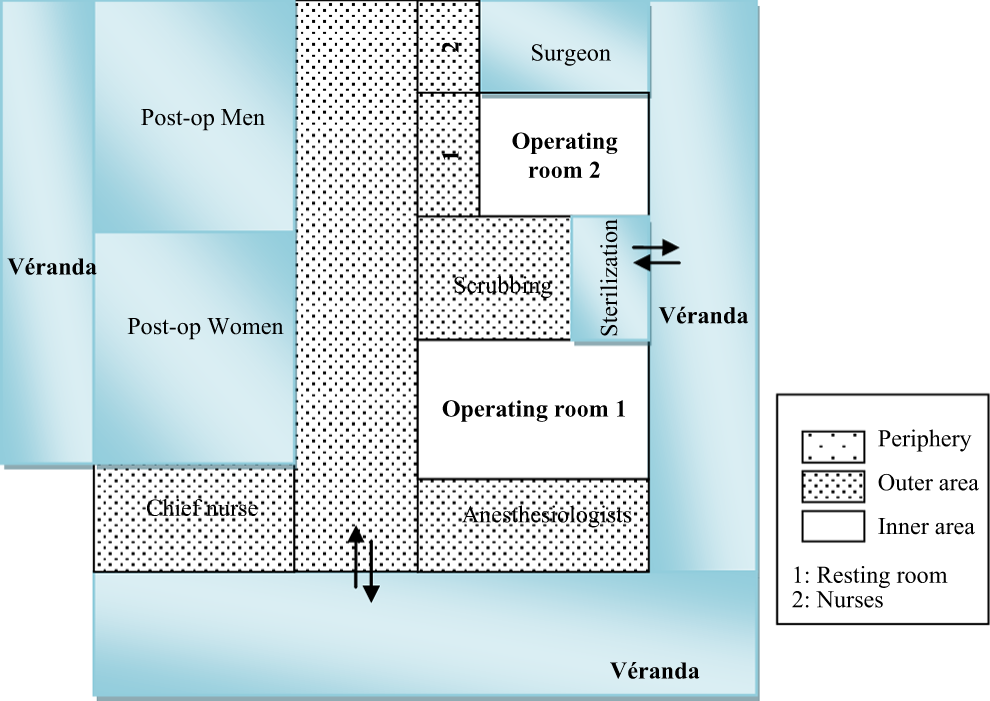
This area thus features three areas instead of the four (periphery, outer area, middle area, and inner area) as Katz (1981) structured the surgical area that she studied. How do team members manage to deal with surgeries in this space?
It has been recognized that nonhuman actors have agency and are not merely passive entities, and that they are part of the production of knowledge and practices (Mol 2009). Therefore, an operating theater as a specific space in the hospital has agency. In the following paragraphs, I consider the relations/workings of space, human, nonhuman agencies as “boundaries makers” and coproducing.
Performing Surgeries: Discontinuities, Physical Space, Tools, and Human Agency
“Turning the Surgeon into an Instrument:” 18 Scrubbing or Washing?
Surgeries performed in this operating theater deal with medical problems ranging from benign tumors and prostatic tumors to ectopic pregnancies and may include procedures such as hysterectomies, laparotomies, caesarean sections, and amputations. As already mentioned, they cannot be planned in advance because patients, for the most part, are poor. The average cost of a procedure exceeds by far the income of the majority of patients. Often, when they have been diagnosed, it takes them some time to gather the amount of money required to pay for the surgery. If by chance, following a consultation, a patient declares he can bear the cost, the surgery will be performed that very day or within the following twenty-four hours at the latest. In such cases, after prescribing a few tests, the surgeon will send the patient to the anesthetist. The latter will make out a prescription (suturing thread and needles, scalpel, narcotics, drips, antiseptics, gloves, etc.). The patient or his relatives will then go to the hospital pharmacy to buy the required items and to the laboratory for the prescribed tests. Once this process is completed and test results are available, the anesthetist will send a message (short message send or SMS) to the surgeon, asking if he can proceed with the patient’s preoperative preparation. At that point, the surgeon will warn people in his waiting room that consultations will be interrupted for a while. When the process of preparing the patient for the operation is completed, the anesthetist sends a second short message to the surgeon, who goes into his examination room, takes off his white jacket, gets undressed, and dons a green coat and trousers, green cap, and plastic boots. With his brief case and cell phone in hand, he leaves his office. When he reaches the operating theater, he first of all opens the door of the operating room, glances into it, closes the door, and scrubs.
Scrubbing is a procedure by which selected personnel wash their hands and lower arms according to rigidly prescribed timing and movements. Among surgeons, it is also a substitute term for operating, for example, to indicate that they helped operate on a particular patient, some will say they “scrubbed” on that case. A surgeon will ask if he may scrub when he wishes to assist in an operation (Cassel 1991). In Cassel’s (1991) study, a surgeon described scrubbing mainly as a ritual, despite its scientific rationale. The purpose is to remove as many bacteria as possible from the fingers, nails, hands, and arms to the elbows. However, as discussed above, Collins (1994) suggests that each scrub “makes” germs, because it affirms their existence and thus reinforces the principles of sterility.
The people who scrub are those who actually carry out, or directly assist in the surgery (Katz 1981). In the Extrême Nord operating theater, this includes at least the surgeon, one assistant, and one anesthetist; however, only the surgeon and his assistant actually scrub. Moreover, the ritual process is not as precise as the one described by Katz. In her study, before a person begins scrubbing, he or she checks the clock in order to time the seven-minute procedure (Hirschauer 1991). “He turns on the water by pushing a button with his hip, and reaches for a package which contains a nail file, a brush, and a sponge that is saturated with an antiseptic solution. For two minutes, he cleans under each of his nails with the nail file. For two and a half minutes, he scrubs his fingers, hands, and arms to his elbows, intermittently wetting the sponge and brush with running water. Using a circular motion, he scrubs the entire surface of his fingers on one hand, and his arm to the elbow. After rinsing that arm under running water, he repeats the procedure for two and a half minutes on his second hand. After seven minutes of scrubbing, he discards the sponge, brush, file, and paper, and turns off the water by pressing a button on the sink with his hip” (Katz 1981, 338).
In contrast, the “scrubbing room” of the operating theater consists of two unsanitary washbasins and a derelict metal closet. It is neither equipped with a clock, nor with nail files, brushes, or sponges. Sometimes, even antiseptic solutions are lacking. Usually, the surgeon and his assistant turn on the water and soak their arms. With a piece of soap, they use one hand to soap the other hand, from the fingers to the elbows; they then rub vigorously between the fingers, use the right index and thumb nails to scour under the left hand fingernails and the left index and thumb nails to scour under the right fingernails. They let the water run over their arms starting from the elbow, between the fingers, and use thumb and index fingernails to rinse under the nails. When scrubbing is completed, they turn off the water with the hands they have just scrubbed. They then enter the operating room by pushing the door with their hips or feet, holding their lower arms and hands in an upright position. Ideally, their scrubbed hands and arms should not come into contact with anything or person. But this is not always the case. Sometimes, when the surgeon’s assistant enters the operating room (generally, the surgeon is the last to come in), it is empty. If so, he sits on a chair maintaining his arm in an upright position until the volunteer nurse or an anesthetist comes in. The latter opens up a container from which the surgeon’s assistant picks a towel or a green sheet to dry his arms. Each finger is dried separately, and the towel is thrown on the floor or the surgery bench. The volunteer nurse or the anesthetist then opens another container full of sterile gowns; the surgeon’s assistant takes a gown, puts it on, and turns to the nursing assistant or the anesthetist to knot the string behind the gown.
In her study, Katz observed that a scrub nurse holds the outside, sterile part of the gown out for the surgeon and his assistant to don. They insert their hands through the sleeves without allowing their hands to touch the outside of the gown. Their hands, although scrubbed and clean, are not sterile, while the outside of the gown is sterile. In contrast, scrub nurses do not exist as professional category in the hospital. Usually, the volunteer nurse or the anesthetist will perform the role of a scrub nurse. (I also performed this role during the course of my observations.) These people have not scrubbed, but they may be in contact with the back of the surgeon’s assistant, which will not touch the instruments, the operating table, the body to be operated on, and so on, all of which are sterile. They will do the same for the surgeon, but his assistant will knot the string. The process is completed when the surgeon and his assistant put on their gloves. The anesthetist or the volunteer nurse opens the gloves’ paper wrapping. While opening the paper, they make sure that their fingers are not in contact with the gloves. They hold the paper in their hands while the surgeon’s assistant or the surgeon inserts his fingers in the gloves. While doing so, he has to make sure that his fingers do not come in contact with the outer part of the gloves. When the fingers of each hand have been inserted, he can use one hand to finish the process on the other. He pulls up the gloves and slips the ends of his gown sleeves into the gloves, so they will not be soaked in the blood, come into contact with an organ or instrument, or otherwise interfere during the procedure. Sometimes, as he is waiting for the anesthetist or the volunteer nurse, the surgeon’s assistant sits down, his hands on his knees, the palms of his hands facing the ceiling. His trousers, which are the one he wears all day long, are dirty, potentially contaminating his hands. When he puts on his gloves, his dirty hands may contaminate the inside of the gloves, but the outer part will remain sterile as he manages to avoid having his fingers touch the outer sides of the gloves. In this context, the process of turning the aggregated surgeon-body (Hirschauer 1991) into a sterile instrument is not linear, flowing, and continuous. It is interrupted at different moments. However, although the entire process is discontinuous, in the end only the sterile clothing and equipment of the surgeon and his assistant will come into contact with the sterile parts of the patients, until they become dirty during the procedure.
Cassel (1991, 47) describes telling an American surgeon how a friend of hers had observed operations in Russia, where elaborate precautions were not followed; the surgeon responded that “sometimes he operates in street clothes and things turn out pretty well.” She goes on to quote a female surgeon, who says that “Surgery is a lot of ritual and a little science.” As Katz (1981) pointed out, the rituals enacted, the restricted entrances, the specific clothing required, the special language used, the classification and segregation of objects into sterile and non-sterile, and the dispassionate emotional reactions to human body parts are exclusive to that setting and establish a discontinuity between the operating room and the outside. They symbolize separation of areas containing microorganisms from areas free of microorganisms, realms of sterility from realms of dirt (contamination). For Collins (1994), the clothing requirements, entrance procedures, and other rituals actually contribute in “making” the world of surgeons full of germs. This is because they are an affirmation of their existence. Analyzing surgery as a process, he notes that is difficult to kill all germs. To kill germs on the skin, for example, the surgeon or the nursing team must shave the patient and swab the skin over and over again with strong antiseptics. This takes a long time, is only practical for a very small area of the body, and is much less effective than autoclaving. He concludes “The antisepsis story, however, has nothing to do with the real existence or infectiousness of germs, only with the place of the idea of germs in the life-world of surgeons. Certainly, one could not make sense of a world of surgery that was full of germs but involved no scrubbing and draping; the scrubbing and draping and the conceptual world containing germs are inextricable elements in surgeons’ form of life. Interpreted this way, one would say that the shrouds and so forth were ‘constitutive’ of germs. Whether one believes that the germs are really there makes no difference to this story” (Collins 1994, 318).
Inside the Operating Room: Places as Status Markers
In the operating room, people and objects or parts of objects are classified either as sterile or non-sterile. Non-sterile objects are further classified as clean, dirty, or contaminated. To remain sterile, objects may only come into contact with other objects that are sterile. They may become non-sterile, and thus contaminated, through contact with any objects that are not sterile. When contaminated, objects can only be restored to sterility by placing them in an autoclave for a specified period of time, or, in the case of a person’s clothes or gloves, by discarding the contaminated clothes and replacing them with sterile clothes. “Fields of sterility and cleanliness” are mapped out. Some of these, such as those surrounding the patient, are invisible, while others are distinguished by green-colored sterile paper sheets (Katz 1981, 338–340).
As mentioned, the team in the hospital generally includes at least the surgeon, one assistant, and one anesthetist, each of whom stands at specified places with specific tasks to perform. The surgeon stands next to the operating table on one side of the patient, his assistant facing him on the opposite side. The assistant threads needles, holds forceps, removes blood with the suction machine or a green sheet, holds back other organs from the one on which the surgeon is working, and so on. He enables the easy progression of the surgeon’s hands instruments hybrid inside the anesthetized patient’s body. Sometimes, the surgeon stops to look at his work, and the assistant’s role is then to make sure that nothing (blood, instruments, and sheets) obstructs the entire picture. The assistant is usually the last to leave the operating room.
As for the anesthetist, when he is in the operating room he stands behind a green curtain at the head of the patient. Writing on anesthesia as a process, Mort et al. (2005, 2027) noted that during anesthesia the patient must surrender vital functions to the care of clinicians “who will act for, and advocate for the patient during the surgical procedure.” Anesthetic practice is, in their view, “not only at the frontier of conscious/unconsciousness but also at the human/machine frontier, where a range of technologies act as both delegates and intermediaries between patient and practitioner.” In the studied hospital, the anesthetist has only one tool to monitor the patient: his fingers, specifically the thumb, index, and middle fingers. During the procedure, he will regularly touch the patient’s wrist to feel the pulse; this is the only way for him to monitor the patient. It must not be assumed that this is a simple task. Touch is inextricable from technique (Prentice 2007). To acquire personal technique and depend only on touch, one must acquire a sense of what feels “normal.” The two anesthetists have been working in the hospital for twenty years. They say that they have witnessed all types of surgeons at work: male, female, black, white, well qualified, unqualified, younger, and older. Throughout their professional career, working with various types of professionals, they have observed, listened, and therefore acquired insights about both biology and the use of certain tools. Sometimes they try to use this knowledge by questioning the surgeons, proposing a different way of doing things, or suggesting another explanation for the visual appearance of an organ, and so on. Since they are monitoring the entire situation, their presence allows the surgeon to pull back from a systemic vision of the body for a moment and to concentrate on one organ, thus reconfirming his specialty. Prentice (2007, 538) notes that “space, time, and clothing [and practices, I would add] in the operating room create a positive economy that reinforces bodily discipline and social hierarchy,” a hierarchy that “places surgeons at the center and all the others at the periphery.”
When, to use Hirschauer’s phrase, the process of “turning the surgeon [and his assistant] into an instrument” is completed, they move closer to the operating table on which the patient-body has been installed. The surgeon glances at the instrument tray and checks whether his assistant and the anesthetist are ready. He picks up a sterile scalpel from the tray and palpates the body part to be operated on; sometimes he draws the incision on the body or performs a dry run, then starts the surgery. This first incision, according to Katz (1981), marks the first stage of the procedure.
At this point in our analysis, Doreen Massey’s conception of space is helpful. She considered space to be: The product of interrelations, constituted through interactions, from the immensity of the global to the intimately tiny. The sphere of possibility of the existence of multiplicity […], a sphere in which distinct trajectories coexist; a sphere of coexisting heterogeneity. […] A product of relations which are necessarily embedded in material practices which have to be carried out; always under construction, never finished, never closed. Space does not exist prior to identities/entities and their relations. Identities/entities, the relations between them and the spatiality which is part of them, are all constitutive (Massey 2005, 9).
These propositions are important to understanding the ways through which space, (professional) identities and entities (tools) work together and contribute to shaping how the operating theater is “read” by actors (Fox 1997). In the following paragraphs, I consider human agency and the use of tools during surgery. I focus on new definitions of boundaries and of sterility/non-sterility that emerge during the process of surgery.
Going into the Patient-Body: New Boundaries
First of all, we note as Katz (1981) did that before the first incision, the operating room is considered to be clean. But as soon as this first incision is made, new definitions of sterile and non-sterile are introduced. For example, the patient’s blood and internal organs, which were considered non-sterile before the operation, are considered sterile once the operation starts. The surgeon’s blood however remains non-sterile. The patient’s skin, although cleansed with antiseptic before the operation, becomes non-sterile once the operation begins and the incision is made. For this reason, the differentiation of spaces leads to controlled behaviors in the operating theater (Katz 1981; Pouchelle 2007).
Hirschauer (1991) and Moreira (2006) indicate that although the initial incision might seem the most dramatic and exciting moment to an outside observer, to the surgeons and nurses it is an undramatic routine. For them, the tension comes at other times. During my fieldwork, I noted the silence and tension that prevail at the first stage of the operation, as Katz (1981) also observed. This tension varies according to the procedure and the frequency with which it has been carried out. An example occurred when the chief surgeon had to perform an amputation. It was the first amputation he had ever performed, both in his career and training, and there was a mixture of tension and excitement in the operating theater. The two anesthetists were present. A specific set of instruments was sterilized. All the team members stood at the feet of the patient, even the anesthetists. The already-high tension seemed to be rising. The surgeon took a saw from the instrument tray. He stood silently with the saw in his hand, facing the leg he was supposed to cut. All the team members were looking at the feet, waiting for the surgeon. He did not move. His assistant snatched the saw from his hand and began to cut violently. The surgeon put his arm on the instruments tray, watched his assistant at work, and commented, “I was able to do it.” However, he left the assistant to perform the entire procedure, after which he sutured. As we mentioned earlier, physical space, time, clothing, and practices create a positive economy that reinforces the social hierarchy of the operating room and places surgeons at the center and all others at the periphery (Prentice 2007). This incident was a complete inversion of roles. The surgeon was pushed into the periphery by his assistant, who was therefore at the center. One can argue that this was an unusual situation, but as the chief surgeon often commented, all surgical procedures are unusual. Surgery is not a routine. The technical parts of it and the different steps of a procedure can be standardized and followed repeatedly, but the term routine cannot be applied to the entire process because patients are not the same. Different bodies have different reactions to the same tools, medicines, and procedures. This contrasts with Collins’s (1994, 311) suggestion that we “understand the surgeons’ world as routine.”
Our data reinforce the idea that space does not exist prior to identities/entities and their relations (Massey 2005). To repeat Massey’s (2005) words quoted above, identities/entities, the relations between them and the spatiality that is part of them, are all constitutive. Throughout the process of going into the patient’s body, the surgeon will use a combination of skills, tools, and techniques, as well as his eyes, fingers, and nose to evaluate the body’s reactions to surgery. This eventually redefines places, functions, interactions with his assistant, tools, the patient’s body, and the anesthetist.
From my fieldwork diary: “The second stage of the surgery, which consists of isolation and excision of the organ, is in process. The surgeon stops and looks silently at his finger. The assistant is still looking inside the patient-body. Then he notes the interruption, lifts up his head, looks at the surgeon: did you prick your finger? No, I touched it lightly. He re-introduces his hand in the open body: this is the abscess. I can feel it. Push your hand, here, see, no, stretch your hand here to evaluate it better. The assistant stretches his hand, but he neither can “feel” nor “see” it. The surgeon asks for an expander. One anesthetist brings the container; he picks it up. He tries to use it, the body bleeds. He asks for the suction machine. The second assistant, who is in the operating room at that time, connects the machine to an electric socket. It makes a dreadful noise. This seems not to bother anyone. The surgeon is searching inside the body while the assistant applies suction to the bloody organs. Their hands touch, cross, mingle. Then the surgeon: “There is a smell of stool.” They observe that he has some difficulties isolating the organ. Everyone makes its suggestions. Finally, he judges that the incision is not large enough and decides to widen it: “I can ‘see’ it, I can ‘feel’ it, but it must be exposed.” Then: “Here it is! This is the appendix.” The anesthetists and second assistant draw near to him and watch. “Very bad,” the surgeon says as they are looking. “Give me pliers.” The second assistant brings a container and the first assistant picks up a set of pliers and gives it to the surgeon. He fixes four pliers around the appendix and inspects each of the organs next to it.”
The surgeon “feels” through his hands and nose; he “sees” through his eyes and hands. This specific way of seeing has already been mentioned. As Good (1994) writes, entry into the world of medicine is accomplished not only by learning the language and knowledge base of medicine, but by learning quite fundamental practices through which medical practitioners engage and formulate reality in a specifically “medical way.” These also include specialized ways of “seeing.” Medical education begins with visual entry into the human body through the microscope, through contemporary radiologic imaging, or presented by scientists, then physically in the anatomy lab; through these various means, the body is revealed in infinite, hierarchical details. In training for surgery, it also involves acquiring two bodies: the surgeon’s own trained body and the abstract body that has been learned “from dead substitutes like books and corpses” (Hirschauer 1991, 309), or in other words, defamiliarizing the student with his or her body and installing new schemes of perception and thought. Disciplining of body and hands, keeping them sterile, learning how to position them and always to be conscious of what one touches, are among the early lessons of surgery. Guided by senior surgeons and residents, student surgeons come to embody surgical being as they somatically experience the procedure and learn the “feel” of doing it correctly (Prentice 2007). Thus, surgery consists of tactile impressions, embodied assessment of patients’ state, and technical procedures that can lead to a re-articulation of the case (Moreira 2006). These tactile impressions are a continuous superimposition of the surgeon’s body and the abstract body that is continuously present in the surgeon’s mind and guides the anatomical imagination necessary to think ahead during procedures (Hirschauer 1991). Sometimes, the surgeon pauses during surgeries, straights his neck or takes a step back with his two hands still inside the patient-body, and takes an overview of the tissues arranged horizontally before him. He then steps forward and continues the surgery, perhaps after commenting on the color of an organ, or without any comments. (To my knowledge, this contemplative aspect of surgery has not been studied.)
Taking these points into account, we can conclude that, through the above-mentioned insertion using his hands and his eyes, the surgeon analyses the relation between the patient’s body and the abstract anatomical body. Throughout the “step by step occupation of the patient’s body” (Hirschauer 1991), the surgeon names the organs encountered, and asks his assistant if he recognizes them or if he can find a particular organ. He comments on difficulties, sometimes foreseeing another surgery for the patient or dealing with the problem if it is possible. The aim of this stage is to identify the mismatch between the two bodies (the patient’s body and the abstract body), and the overall process will be an attempt to have the former approach the latter. Here, as Hirschauer suggested, the relationship between the surgeon and the patient-body is also mediated by the anatomical body.
From my fieldwork diary: (Same procedure) The organ has been isolated, excised, and put on the operating room bench. The surgeon is rearranging the internal organs. One anesthetist who wasn’t there previously enters the operating room. The surgeon: “This is the appendix. Please come and see. This is its base, here, it’s long! I am surprised! Why is this so long? The thread is not strong. This appendix is bizarre, I’m surprised. It does not resemble the others, I mean the end of it. These pliers are not holding the thread, is there nothing else? Tell me, what about his blood pressure? I observe an abdominal dilation; I hope there isn’t any perforation. Tell the family members to prepare the money. See, our shoes are worn out. There is a budget for dressing.” They stop, waiting for the appropriate needles. “What I smell makes me think of a perforation. But if there was any, we would have seen it through the abdomen. Certainly, her appendix was big enough.” While he is speaking, his assistant is putting the various pieces of the appendix together to form the original organ. “These are difficult procedures because if you aren’t careful you will perforate the intestine. Last time, when the minister came to visit us, they did not allow me to speak. The director of the hospital came and stood between the minister and me. He knew what I was going to tell the minister about this operating theater. Maybe we made a mistake by opening the peritoneum. I will see tomorrow.” Then the needles are provided. He does the entire suturing himself.
Usually during this third stage, the surgeon adjusts the inner body tissues and leaves the outer ones to his assistant. He removes his gloves and gown, which he throws on the floor, and leaves the operating room. The assistant sutures the outer tissues, calls the orderly in charge of cleaning the space, throws his gloves and gown on the floor, and leaves the room. The anesthetist and the orderly move the patient from the operating theater. The body is expected to begin its recovery and the patient to come out of anesthesia.
In Katz (1981), the third stage of the operation begins with the final counting of the materials used in surgery. In the studied hospital, there is no counting of the material used. Katz noted that the silence and tension that prevail during the second stage is replaced in the third stage by considerable talking, including jokes and small talk. Most of the joking revolves around events that occurred during the second stage and references are made to actual or potential dangers during this stage. I did not notice such a clear-cut division of talking and joking in the operating theater studied. The tension did not automatically prevent the team from joking or talking about subjects that were far from the ongoing procedures, such as gossip. During all the procedures I observed, the surgeon always showed the pleasure he takes in operating on patients. When surgeries are not scheduled, he appears sad. One day as we were talking in his office, he said, “I haven’t operated for two days. I’m not well.” Cassel (1986) similarly reported this, noting that “a surgeon is never as happy as when he’s operating, said a chief, singing tunelessly as he scrubbed for an operation, while a senior registrar remarked, after operation, I was in such a bad mood and now I feel good. I love to operate, it always makes me feel good.” The same can be said about the surgeons in the Extrême Nord hospital.
Conclusion
The objective of this study was to describe interactions among health workers, physical space, tools, and the patient in an operating theater, taking into account the specific economic context in which they occur. The aim was to pursue certain arguments advanced by Katz (1981), Collins (1994), and Rawlings (1989): Rituals, restrictive entrance procedures, and clothing requirements help establish the operating room as a separate place, discontinuous from its surroundings (Katz 1981, 344). Clothing requirements, entrance procedures, and all the rituals in the operating room “make” the world of surgeons full of germs (Collins 1994, 318). The existence of a set of rules that are technically based and organizationally administered gives rise to the possibility of their differential observation (Rawlings 1989, 288). When rituals, restrictive entrance procedures, and clothing requirements are not in place, when rules are not observed for the various reasons discussed in this article, the boundary between the operating theater and its surroundings blurs; it becomes trivialized, a common space, giving place to “intriguing combination of practices,” as health workers tinker to perform surgeries in a context of poverty and poor working conditions.
It has been shown that medical practice does not adhere to universal rules and categories. It can be transformed under the influence of locally creative usages and the process of becoming embedded in a given historical, cultural, social, or economic context. Medicine is produced reproduced, reformulated, and sometimes resisted within diverse cultural settings. Thus, it becomes a situated practice when transported (Mol 2002, 2009). The economic context within Cameroon explains much in the studied hospital. The country’s economic performance has been poor, which has affected its ability to sustain and invest in health services and health care (Kushner, Mannion, and Muyco 2004; Dovlo 2005). As described, there is a chronic lack of equipment, and health workers are not provided with the appropriate clothing for their jobs. Surgical equipment sets are incomplete. The sterilizing machine dedicated to high-volume sterilizations is out of service. The sterilization room needs a complete restoration. Patient monitoring has been reduced to its most basic. In such a space, the principles of sterility seem to vanish.
What I have described here suggests continuity between the operating theater and its surroundings, resulting in what I have called a trivialized operating theater. But despite this trivialization, family members and health workers from other services do not venture beyond a certain point when approaching it. Whatever the reasons for it, the fact is that the operating theater remains a special setting within the hospital, and outsiders do not enter it under any circumstances.
Writing about boundaries, Thornton (1980) remarked that a boundary by definition creates a closed and limited region inside and distinguishes it from an open and unlimited region outside. The existence of a boundary does not necessarily imply, in formal terms, that the inside region it defines is continuous. It is also simply connected; that is, it is not divided internally by any other boundaries or cuts. Any point within the region may be connected with every other point without intersecting a boundary. If this condition holds, the region defined and limited by the boundary is simply connected. This applies to the Extrême Nord hospital that I studied where a context of crisis and lack of equipment and personnel reduces the boundaries of the operating room—the limits of what is supposed to be kept sterile and out of contact—but do not erase them. The restrictive entrance procedures, clothing requirements, rituals, and rules that are supposed to create a discontinuity between the operating theater and its surroundings are not fully observed. Thus, its operating theater is not a completely closed, limited region inside the hospital that can be distinguished from its surroundings. Rather, it is connected to its surroundings, and there is continuity between the inside of the theater and the outside.
Why is it that we still speak of an operating theater and that it can be recognized as such in photographs? What makes it an operating theater, not a laboratory, a consulting room, a gynecologist office, or a storage room for out-of-service equipment? I would answer this question with Mol and Law’s (1994) analysis of the hemoglobin network. A network, they state, is a series of elements with well-defined relations between them. Network elements may include machines or gestures. Places with a similar set of elements and similar relations between these elements are “close to one another.” Thus, however, many kilometers there may be between two operating theaters in a network topology, they are close to one another. That is precisely the reason why, despite the fact that it looks much like a storage room for worn out equipment, the operating theater can be recognized as such. The key elements here are the green sheets, the tools on the tray, the operating table, the sterilizing room. These are the “immutable mobiles” (Latour 1987). Applying this concept to their own work, Mol and Law (1994, 653) define an “immutable mobile” as an arrangement that remains stable under a wider range of circumstances. It is mobile because from the point of view of regional topology, it displaces itself from one place to another (p. 649). So, the “space-time travel” of these mobiles is only “space-time travel” from the point of view of a regional topology (p. 649). These immutable mobiles contribute to “making” this an operating theater. The relations between the different elements of the network are not as rigorous as they should be, but they still exist. The anesthetist does not operate; the green sheets, needles, thread, and surgery table are used for what they were designed for.
Money, doors, washbasins, soap, clock, nail files and sponges, antiseptic solutions, nurses, clothing, the patient’s body, and family members—all have agency, in the sense that their structure (doors and washbasins), absence (clock, antiseptic solutions, nurses, etc.) or presence can transform interactions and relationships between health workers, tools and the space on one hand, and the patient’s body, family members, health workers, tools and space on the other. This article therefore supports Massey’s (2005) conception of space as “always under construction,” constituted through interactions with identities and entities, a sphere in which distinct trajectories coexist, and thus, a sphere of coexisting heterogeneity.
Footnotes
Author’s Note
A preliminary version of this article was published in Revue d’Anthropologie des Connaissances.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author received financial support from the Agence Nationale de Recherche sur le Sida et les Hépatites (ANRS). Grant: 12 144.