
Abstract
This article addresses the child’s right to know their genetic origins in mitochondrial donation. It focuses on the UK’s public debate on mitochondrial replacement techniques and examines the claims-making activities that shaped the donor information regulations. During the public consultation, downplaying the significance of the mitochondria helped distinguish mitochondria donors from gamete donors and determine their relational status with the resulting child. As a result, according to the Mitochondrial Donation regulations, mitochondria donors, unlike gamete donors, will not be required to be identifiable to the resulting child. I argue that, in the UK, similar to donor conception, public understanding of mitochondrial donation is shaped by a “calculus of genes”: simplified accounts of how genes determine the resulting child’s characteristics and identity. While the donor conception regulations ascribe social meaning to the passage of genes, the mitochondria regulations strip the social meaning away from the donation based on the assumption that the genetic contribution made by the donor is quantitatively insignificant in influencing the identity of the resultant offspring. The nature of the genetic material itself should not be considered as a privileged standpoint from which to decide on social meaning of the donation or the rights attached to it.
Introduction
In the UK, the Human Fertilisation and Embryology Authority (HFEA) keeps a record of all donors, licensed treatments, and children born following the use of donated gametes and embryos. Initially, access to such information was limited. However, the law changed on April 1, 2005, with the implementation of the HFEA (Disclosure of Donor Information) Regulations 2004/1511. Fully anonymous donation was abolished and, once they reach the age of eighteen, those born with gametes donated after April 1, 2005, will be able to apply for identifying details of the donor.
The change in the UK’s law was a response to the “right to know one’s genetic origins” claims brought by donor–conceived individuals (Turkmendag, Dingwall, and Murphy 2008). The right-to-know claims in the context of donor conception are mainly based on a presumption that genetic information is an essential component of personal identity and consequently that it is in the best interest of children to know their genetic origins (Smart 2010). Increasingly, this is also linked to a rights-based argument: children have a legal right to know their genetic origins (Wallbank 2004; Smart 2010; Ravitsky 2010). 1 The right to know is also recognized by the international legal framework of human rights through the Art 8(1) of the United Nations (UN) Convention on the Rights of Child, which stipulates “the right of the child to preserve his or her identity” and through jurisprudential interpretation of Article 8 of the European Convention of Human Rights, which provides a right to respect for private and family life. 2
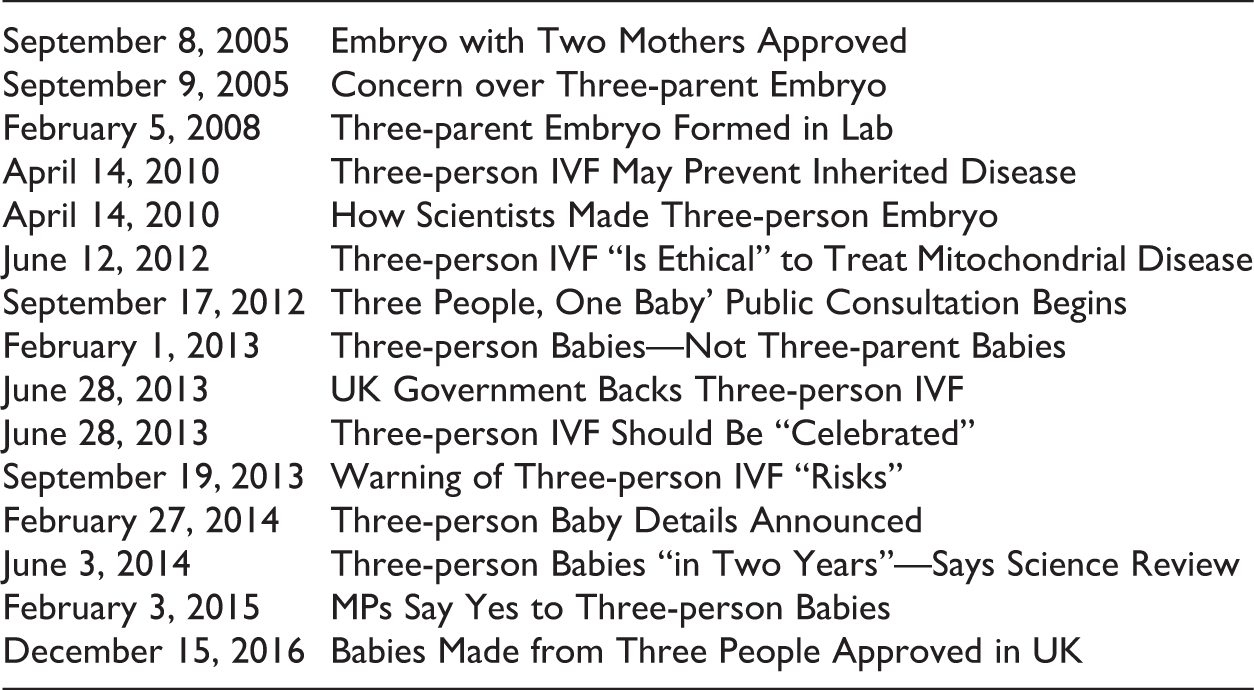
Shortly after the removal of donor anonymity, on September 9, 2005, a sensationalist headline about a new assisted conception technique appeared on MailOnline: “The Cloned Baby with Two Mothers.” Mailonline was referring to a new license granted by the UK’s HFEA to a research group at Newcastle University allowing them to develop a technique to prevent transmission of mitochondrial disease (HFEA 2005).
Mitochondrial disease is a maternally inherited genetic condition that may cause morbidity and mortality. The risk of transmitting a mitochondrial disease is hard to assess through prenatal diagnosis, hence women known to harbor mitochondrial mutations can use donated eggs to prevent transmission of the disease (Nesbitt et al. 2014). Mitochondrial replacement techniques (MRTs) promise hope to affected families that they will have a genetically connected child without faulty mitochondria. There are two central methods. In maternal spindle transfer, the spindle is removed from the intended mother’s egg and transferred into an egg from a donor that has had its maternal spindle removed. In pronuclear transfer, the pronuclei from the donor embryo are removed and replaced with the pronuclei from the intended parent’s embryo (Parliamentary Office of Science and Technology [POST] 2014). In either case, the maternal nuclear DNA remains in place.
The Newcastle University team leading this research in the UK reported success in 2008 in creating embryos that have nuclear DNA from both the intended parents and mitochondrial DNA from the donor (“Three Parent Embryo Formed in Lab,” February 5, 2008, BBC News). Between September and December 2012, HFEA, which oversees the use of embryos and gametes in research and fertility treatment, ran a consultation to explore the social and ethical impact of making these techniques available to patients (HFEA 2013a). In 2011, the HFEA also established a panel with broad-ranging scientific and clinical expertise to review the evidence; further reviews were carried out in 2013, 2014, and 2016 (HFEA 2016). 3 In March 2013, the HFEA advised the government that “there is general support for permitting mitochondrial donation in the UK, so long as it is safe enough to offer in a treatment setting and is done so within a regulatory framework” (HFEA 2013b, para. 1.7). Along with the HFEA, the Nuffield Council on Bioethics (NCoB), the UK’s independent body that examines the ethical issues around biomedicine, also recommended that MRT would be an ethical treatment option for affected families (NCoB 2012a). The Department of Health (DoH) ran a consultation between February 27 and May 21, 2014, to seek the views of stakeholders and the wider public (Health Science and Bioethics Division, DoH 2014a). The respondents were “generally positive” about the proposed provisions by the government (Health Science and Bioethics Division, DoH 2014a, 6).
After the public consultation process, the regulations passed in the parliament and the Human Fertilisation and Embryology (HFE; Mitochondrial Donation) Regulations came into effect on October 29, 2015, making the UK the first country permitting the clinical use of this technique on humans. On December 15, 2016, the HFEA announced that they have decided to permit, in principle, the use of MRT in clinics to prevent the transmission of mitochondrial disease.
The draft regulations were presented before parliament under section 45(4) of the HFE Act 1990 and made consequential amendments to provisions of the 1990 Act and the HFE Act from 2008, including provisions for donor information.
Having considered that some individuals born as a result of these techniques may wish to know more about the donor, the government took the view that mitochondrial donor–conceived individuals should not have access to identifiable information about their donors (Health Science and Bioethics Division, DoH 2014b). Specifically, according to the government, mitochondrial DNA is not as significant as nuclear DNA in determining one’s genetic identity (Health Science and Bioethics Division, DoH 2014b), and therefore there is a difference in respect to the information collected and made available. Overall, the view was that mitochondrial donation fell somewhere between gamete donation and organ/tissue donation. Accordingly, the HFE (Mitochondrial Donation) Regulations 11-15 modify the information provisions in the 1990 Act to enable children born following mitochondrial donation (referred to as “mitochondrial donor–conceived person”) to access limited, nonidentifying information about their “mitochondrial donor.” This allows individuals reaching the age of sixteen, who think they may have been born as the result of mitochondrial donation, to apply to the HFEA to see if it holds any information about them on its register and allow them to obtain nonidentifying information about the donor. 4
As explained earlier, the ethical and legal debate that led to the removal of donor anonymity in the UK was phrased in the language of the rights of the offspring [child] (Turkmendag 2012). Regarding the existing legal framework that protects the right to know one’s genetic origins, and the trend of openness in donor conception, it is worth asking why the position of mitochondrial donor–conceived persons were not aligned more closely with children born following gamete and embryo donation (thereafter referred as “donor–conceived person”).
Management of right to know in the context of MRT raises important questions about the meaning of genetic identity and what makes a human. Can we determine one’s genetic identity by simple calculations based on one’s genetic composition? Can such calculations be a valid reference point for granting or denying one’s human rights? These are the intertwining questions that I deal with in this article.
As Vaisman (2014) notes, new genetic technologies such as DNA identity testing are increasingly employed to establish individuals’ core characteristics, and these tests are also becoming a base for human rights claims. I argue that this trend can be observed in the context of both donor conception and MRT, where the right to know one’s genetic origins is decided based on assumptions about the genetic makeup of the offspring rather than the social context of conception. Both donor conception and MRT involve egg donation. In donor conception, the egg donor is perceived as a progenitor due to her (assumed 50 percent) genetic contribution. Accordingly, the regulations recognize the right to know of genetic origins for the individuals who are conceived by egg donation. In MRT, the mitochondria that the donor contributes (which is less than 0.1 percent of the total genetic makeup of the resulting child) is construed as insignificant to determine the personal characteristics of the offspring or relate the donor to the offspring. Therefore, mitochondrial donor–conceived individuals are denied the right to know.
5
This line of genetic thinking is evident in the UK government’s response to the consultation on MRT (Health Science and Bioethics Division, DoH 2014b, 15), which stresses that the donated mitochondrial DNA will not affect the personal characteristics or the traits of the child (Health Science and Bioethics Division, DoH 2014b, 30).
6
It is further explained that in reaching this view the government considered the evidence of the sequencing of the mitochondrial DNA (Health Science and Bioethics Division, DoH 2014b, 30), which indicates that “all of the mitochondrial DNA genes are involved in mitochondrial energy production and none are involved in governing personal characteristics and traits.” Accordingly, the government concludes: Any relationship between the mitochondrial donor and any resulting child is remote, and in so far that there is any connection this is recognised by the regulations allowing for the sharing of non-identifying information in the same way. (Health Science and Bioethics Division, DoH 2014b, 30)
In this article, building on my previous work that examined the public debate that led to the removal of donor anonymity from gamete donors in the UK, I focus on the “mitochondria debate,” the public debate concerning whether these novel techniques should be made available for treatment. I particularly focus on how right to know one’s genetic identity in MRT was constructed in media coverage of these techniques, public consultation documents, and reports. In my analysis, I use “claims-making” ––a term I borrow from social problems literature––to identify frames and claims that were influential in ethical debates and policy-making (Spector and Kitsuse 1977).
In the first part of this article, after briefly introducing my approach to claims-making, I provide a background to the child’s right-to-know discourse in the UK. In the second part of this article, I examine the themes emerging from the public debate, which explains the assumptions behind the donor information provisions in MRT regulations, including the mitochondrial donor–conceived individuals’ interest in having access to identifiable information about their donors.
Claims-making Activities
The terms claims-making and “claim-makers” were coined by Spector and Kitsuse (1977), who suggested that social problems are not objective conditions; they are “the activities of individuals or groups making assertions of grievances and claims with respect to some putative conditions” (p. 75). 7 According to Spector and Kitsuse (1977), a claim is a demand that one party makes upon another (e.g., demanding services, lodging complaints, and supporting and opposing some governmental practice or policy); claims-makers are the people who make claims; and audiences are the people who judge and evaluate the importance of these claims.
The MRT debate built on the previous public debate over donor anonymity where the conflicting interests of donors, offspring, and would-be parents are prevalent. In donor conception, both donors and recipients make competing claims about the right to know. While their interests are congruent, they later diverge when privacy clashes with the right to knowledge of identity. Donor anonymity is often associated with higher donor supplies. It is assumed that more donors will come forward when their identity is maintained, whereas the resulting individuals might want to find about the identity of their donors. The would-be parents seem to have divergent views about donor anonymity and disclosing the means of their origins to the donor–conceived children (Turkmendag, Dingwall, and Murphy 2008). I argue that the donor information provisions in MRT regulations are a result of successful claims-making activities by the supporters of MRT. In order to secure donor anonymity and avoid the conflict, the advocates of MRT pressed claims to distinguish these techniques from donor conception. Strategically, they framed MRT as a form of tissue donation to be used for therapeutic purposes rather than an assisted conception method that involves egg donation, which raises questions about genetic identity.
By examining the mitochondria debate in the public sphere, my aim is to identify the successful claims about genetic identity that shaped the donor information provisions in the current MRT regulations. In this article, I refer to claims-making as a rhetorical activity that involves construing socially acceptable accounts of the facts to promote a particular policy solution. Policy makers increasingly encourage wide-ranging public debate and consultation about emerging technologies (Williams, Kitzinger, and Henderson 2003). In many ways, the policy-making scene can be understood as a market place where claims-makers bid for public awareness, legal recognition, funding, and other scarce resources (Best 1987). Claims-makers learn ways to maintain public support, identify the key policy makers, and recognize the levers that can move policy (Best 1987). They also develop rhetorical strategies to shape the public’s sense of what the problem is and persuade the audiences about a putative solution (Best 1987).
One way of monitoring claims-making is to study the information available in the public sphere. As Conrad (1997) suggested, in order to understand the lenses through which people come to understand particular problems, an analyst needs to draw on the images and presentations available to the “public eye.” The public eye includes news, television documentaries, periodicals, fiction and the Internet, opinion polls, and government reports and statistics (Conrad 1997). Other sources include public consultation documents, parliamentary debates, political speeches, blogs, and comments in social media. In this article, through examination of media news items and public consultation documents, I identify the dominant constructions of MRT in the public eye and discuss how certain claims about genetic identity, genetic materiality, and genetic relatedness shaped the donor information provisions in MRT regulations.
Claims-making During the Removal of Donor Anonymity in the UK
In the UK, the removal of donor anonymity owes its existence to the successful claims-making of children’s organizations that started in 1990s, including the Children’s Society, which was the first organization that called for a change in the law so that donor–conceived children could access identifying information about their donors (Turkmendag, Dingwall, and Murphy 2008). The Children’s Society and other activists who campaigned for a change in the law stressed that children have the right to know their genetic origins, including having access to identifiable information about their donors (Turkmendag, Dingwall, and Murphy 2008). They made a few important claims, including that genealogical information is central to the development of personal identity and to ascertaining one’s medical history, that openness and transparency are attributes central to family life, that parents are more likely to disclose to the child her or his origins if donors are identifiable, and that the position of donor–conceived people should be aligned more closely with that of adopted people who have full access to identifying information about their “biological parents” (Turkmendag 2012). Campaigners such as British Association of Social Workers Project Group on Assisted Reproduction (PROGAR 2012) further claimed that children have a legal right to know their genetic origins.
Article 8 of the UN Convention on the Rights of Child explicitly recognizes the right to identity (de Andre 2010). The right to identity also has been recurrently invoked in the case law of the European Court of Human Rights in Strasbourg (de Andre 2010). For example, in Rose and Another v. Secretary of State for Health (2002) EWHC 1593 (Admin), in Judge Scott’s view, it was quite clear that Article 8 of the European Convention on Human Rights (ECHR) and the existing jurisprudence of the European Court of Human Rights supported the idea that “everyone should be able to establish details of his identity as a human being” and that this clearly included the “right to obtain information about a biological parent who will inevitably have contributed to the identity of his child” (Rose, op. cit., n. 19, paras. 47-48). There are also traces of the donor–conceived child’s “right to know” in Strasbourg case law on both paternity testing and the practice of anonymous birth (Mikulić v. Croatia [2002] 1 FCR 720; Odièvre v. France [2004] 38 EHRR 43; Godelli v. Italy[2012] ECHR 33783/09) and in provisions of Article 8(1) UN Convention on the Rights of the Child, which say that a child should be able to know her or his parents as far as possible. Similar debates happened elsewhere—notably in the United States (Bernstein 2010; Cohen 2012) and in Australia (Adams and Lorbach 2012), including the retrospective removal of donor anonymity. Recently, the Australian State of Victoria passed Assisted Reproductive Treatment Amendment Bill 2015, lifting donor anonymity retrospectively. 8
Claims-making During the Mitochondria Debate
In order to study the claims-making that led to the regulations that govern the donor information in MRT, I examined the public consultation documents by the HFEA and DoH, the NCoB’s reports on mitochondria donation and donor conception, and the relevant news reports published in the UK press. I searched for the terms “mitochondria” and “donation” in the Nexis Library database for the period between September 2005 (since the Newcastle team was granted a license for research) and December 2016, which contained ninety-four items (a majority of these items were published by The Times, The Guardian, The Independent, The Telegraph, and Daily Mail). I also searched for the same terms in BBC Online news archives for the same period and other web-based media sources. In this article, drawing on my examination of the public consultation documents and the news items, I present a number of themes that I identified in the claims of those who promoted MRT. Although I do not claim that these themes are the only lenses through which the public came to understand the “child’s right to know” in the context of mitochondria donation, I argue that they played a role in shaping the current donor policy. In what follows, I present these under four headings: “Concerns about the Donor Shortage,” “Three-parent Baby,” “Changing the Battery,” and “Calculus of Genes.” The first theme sets the scene for donor recruitment in the UK. As I describe in this section, for the supporters of MRT, it was essential to remove the (perceived) obstacles around donor recruitment to make these treatments available for clinical practice. The other three themes deal with the ways in which mitochondria were construed in public debate, as quantitatively immaterial, qualitatively insignificant, and “relationally” irrelevant. These themes are intertwined more broadly to explain the putative importance of genes in making us unique individuals.
Concerns about the Donor Shortage
There is an ongoing donor shortage in the UK. Today, increasing numbers of fertility patients who want to receive donor conception are seeking treatment abroad in countries that maintain donor anonymity. These patients report that the main reason for this travel for cross-border reproductive care is the shortage of sperm and eggs at home, a problem they associate with the removal of donor anonymity (Culley et al. 2011; Turkmendag 2013). 9 In 2011, following a public consultation the HFEA acknowledged that the demand for donor treatment in the UK was greater than the supply of donors and that the removal of donor anonymity might have exacerbated this shortage (HFEA 2011). As a result, the HFEA increased permitted levels of compensation for donors and established a National Donation Strategy Group (HFEA 2011). However, it is yet to be proven whether any of these measures can recover the number of donors and resolve the donor shortage.
According to Spector and Kitsuse (1977), claims-makers often have particular reasons for choosing particular rhetoric to address particular problems. The UK’s previous and ongoing donor shortage was one of the most important issues addressed during the mitochondria debate, as the social, legal, and ethical obstacles around the donor procurement had to be removed before these techniques became available for clinical application. The concern about the donor shortage was addressed in public consultation documents. For example, in their evidence to NCoB, the scientists working in the field noted that there is increasing demand for eggs for both clinical practice and research into treatments for infertility and the causes of genetic disease, and that the supply has not kept pace with demand, disadvantaging the research and practice (NCoB 2012b). As a response, in its report, the NCoB’s Working Group acknowledged that the legal status of the mitochondrial donor would affect the number and typical profile of donors who would come forward (para. 3.21). The potential donor recruitment problem was also acknowledged by the POST in the case of mitochondrial donors. It noted that because removal of donor anonymity is often cited as a contributory factor to the current shortage, whether there will be sufficient supplies of eggs may depend on whether mitochondrial donors are allowed to donate anonymously (POST 2014). In other words, both policy makers and the scientists acknowledged that one of the central issues around the MRT’s translation to clinical practice was the procurement of the egg donors. In her media brief to the Newcastle University’s press office, Professor Alison Murdoch of the Newcastle team showed support for the HFEA’s recommendation to protect the anonymity of the mitochondrial donors:
10
We welcome the HFEA’s recommendation that mitochondria donors should be thought of as tissue donors, protecting the anonymity of the donor. (March 20, 2013) In Newcastle we have an established practice that recruits egg donors for both fertility treatment and for research. We are confident that, as long as the anonymity of donors is assured, we will have an adequate recruitment rate to implement a mitochondrial replacement treatment program. (House of Commons Science and Technology Committee 2014, 11)
Arguably, these concerns played a role in the creation of a new donor category specific to the mitochondria replacement treatment: mitochondrial donor, a donor whose mitochondrial DNA (but not nuclear DNA) was used to make an egg or an embryo to be used in MRT. As Haimes and Taylor (2015) argue, these terms imply that the egg donor contributes only mitochondria. In fact, the egg contains “other cellular structures and chemical required by the intending parents’ nuclear DNA to direct the egg to develop into an embryo” (Haimes and Taylor 2015, 365). This framing is not accidental. As Haimes and Taylor note, it disguises the contribution of the egg donors and construes them as tissue donors.
“Three-parent” Baby
Often, mass media constitute a key public arena in which the voices of claims-makers are put on public display to compete (Best 1987). But the media also play a key role in how the claims-makers and claims are framed and which claims find credibility and legitimacy (Best 1987). When new developments in genetics raise complex ethical questions that are hard to answer quickly, the media often seek recourse by using metaphors to fill this ethical void—metaphors that may prepare the ground for normalizing and regularizing the new technology (Nerlich, Johnson, and Clarke 2010). These metaphors play an important role in shaping public understanding of new scientific developments, as for most people, a scientific fact is what they know from the press (Nelkin 1987). Accordingly, it is possible that the metaphors used by both the claims-makers and the media played a role in shaping public understanding of MRT. Using a corpus-based approach, Baker and Semino (2014) constructed a data set including all news reports (114 articles) published in the UK between April 2010 (when the Newcastle team announced the technique) and September 2014. There were four key phrases used to describe the technique and hence frame the truth around it: The three-parent baby/babies metaphor was the most frequently occurring phrase in the data (forty instances). The battery metaphor occurred thirty-eight times, making it the second most frequently occurring phrase, followed by designer baby/babies (thirty-three instances) and genetically modified babies (twelve instances).
Jones and Holme (2013) argue that the classification of a donor as a “parent” was the media’s starting point for understanding the contribution of the mitochondrial donor. When MRT was first presented to the Human Genetics Commission, the commission warned against regarding the mitochondrial donor as a “progenitor” or a “gamete donor” and the loaded term “parent” was also avoided by both the HFEA’s Ethics and Law Advisory Committee and the NCoB in its call for evidence (Jones and Holme 2013). The concerns about three-parent metaphor were also reflected by the Progress Educational Trust, in their correspondence to Science and Technology Committee. The trust reported that the parent metaphor was neither “helpful” nor “accurate” as a description of the relationship between the donor and the resultant child (House of Commons Science and Technology Committee 2014, 9).
The three-parent metaphor was also evident in the relevant parliamentary debates (Jones and Holme 2013) and in the public dialogue exercise and consultation conducted by the HFEA (HFEA 2013a). In its advice to government, the HFEA notes that people who oppose MRT argue that the techniques would constitute an interference with the natural or spiritual aspect of reproduction or that any manipulation of embryos is unethical (HFEA 2013a). The report also mentions that some media reports have referred to MRT as “three-parent In vitro fertilization (IVF),” as three individuals would be contributing DNA to create a child, and that respondents who referred to the donor as a third parent usually expressed concern about implications of MRT for the identity of the resultant person (HFEA 2013a). Similarly, during the government’s consultation on draft regulations, respondents who expressed the view that the donor should be regarded as a “third parent” were also opposed to the techniques being allowed in the UK (Health Science and Bioethics Division, DoH 2014b). The government’s response to these claims was as follows: We note that “three parent families” has been used in responses that wish to make a case for a strong link between the mitochondrial donor and the child. We regard this term as completely inappropriate. (p. 29) If the pronuclear and/or spindle transfer methods are adopted clinically […] any mitochondrial donor will be crucial to the outcome, namely to the birth of healthy offspring. But I personally do not think that we should get tangled up too much in a debate about whether they constitute a third parent or not. If I had eggs to give, I would be delighted that my mitochondria could help,
In the following extract, Professor Hugh Whithall, director of the NCoB, makes a similar comment about the insignificance of the mitochondria. He notes that because the donor’s contribution to the conception of the child is limited, the technique does not make the donor a parent. He further distinguishes the egg donors as “egg donors for IVF” and “mitochondria donors” and claims that the latter should not be required to be identifiable. Given that only some elements of the donor egg are used, not including the cell nucleus, we do not believe that it is legally or biologically correct to refer to the mitochondrial donor as “third parent” of the resulting child. We therefore argue that mitochondria donors should not be treated in the same way as egg donors for IVF, for example, they should not be required later to be identifiable to those born from their donation. (Science Media Centre, March 20, 2013)
The successful claims-making by the proponents of the research may have played a role in changing how the media framed these novel techniques. However, it is worth noting that although the shift in language can be observed in BBC’s titles, this was not the case for all the media news I examined. During the period I studied, MailOnline, The Independent, The Telegraph, and The Times continued to use term “three-parent babies” in the news coverage, even when the techniques were framed as a promising treatment for the affected families. For example, “150 babies a year could be born to three-parent families: Children with DNA from two eggs and one sperm could be saved potentially lethal genetic disease” (Mail Online, January 29, 2015), “Thousands of women could benefit from ‘three parent’ baby technique: New IVF techniques could cut some women’s risk of passing on genetic disease” (The Independent, January 28, 2015), “Three parent babies: There’s room for both the begotten and the made: There are far worse crimes than using reproductive science to help you or someone you love conceive a much-wanted, much loved child” (The Telegraph, June 29, 2013), and “Legalise three-parent babies, say Nobel winners”(The Times, January 29, 2015).
Changing the Battery
As well as challenging the traditional boundaries of parenthood and the family, the MRT also constitutes a form of genetic modification (altering the DNA of gametes and embryos in a way that the change can be passed to future generations). It therefore raises more complex ethical issues and human rights questions than other reproductive technologies such as donor conception, including the protection of human dignity and identity from harm, discrimination against genetic heritage, and potential risks of germ line modification for the future generations. Interventions on the human genome are prohibited by international instruments including the Universal Declaration on the Human Genome and Human Rights (UNESCO, November 11, 1997), The Convention for the Protection of Human Rights and Dignity Of The Human Being with Regard to the Application of Biology and Medicine (Council of Europe, Oviedo, April 4, 1997), and the Charter of Fundamental Rights of the European Union (EU, Nice, December 7, 2000). The declaration provides that germ-line interventions are contrary to human dignity (Article 24). The convention prohibits interventions on the human genome unless they are undertaken “for preventive, diagnostic or therapeutic purposes and only if its aim is not to introduce any modification in the genome of any descendants” (Article 13). The charter provides that particular respect must be given to the prohibition of eugenic practices, in particular those aiming at the selection of persons (Article 3). None of these instruments are legally binding in the UK.
One of the most prominent objections against germ-line modification is that altering the “essential characteristics” would violate the child’s right to an open future, a right originally identified by Joel Feinberg in 1980 (Bredenoord, Pennings, and de Wert 2008).
There are, however, different views on what constitutes a germ-line modification: some argue that only the nuclear DNA contains “essential characteristics” of a person and that the modification of the mitochondria should therefore be considered less controversial than modification of nuclear DNA. According to Bredenoord et al., “no matter whether one modifies a (pathogenic) nuclear gene or a (pathogenic) mitochondrial gene, the identity of the future person will be changed” (2011, 99). This is also the view taken by the Working Group when NCoB (2012a) examined the ethical issues raised by MRT. The Working Group considered the potential impact of MRT on multiple aspects of identity including “self-conception,” “qualitative identity,” “numerical identity,” and “genetic identity” (paras. 4.6-4.27). The Working Group took the view that mitochondrial disorders (or their absence) can affect the identity (para. 4.27), and therefore MRT is identity-altering. However, the group was skeptical of locating any distinction about the ethical acceptability of interventions on nuclear DNA or mitochondrial DNA in notions of identity, as any intervention would change the identity of the future person. The Working Group also felt that MRT “cannot be assumed to affect (or to negatively affect) their [the offspring’s] conception of ‘who they are,’” and it concludes that the resulting child’s right to an “open future,” as compared to not performing the therapy, is the key ethical test connected to identity (paras. 4.20-4.25).
During the mitochondria debate, some of the claims included different descriptions of the genetic identity. For example, The Independent reported Professor Dame Sally Davies’s statement that the mitochondria donation would not change the nucleus, which she construed as the essence of the identity: The majority of the DNA is in the nucleus—it’s the germline, I would use the analogy of simply replacing the battery in a pocket radio to explain what we are doing. What we’ve done is like changing the battery on a laptop. The energy supply now works properly,
During the consultation, in their correspondence submitted to the Science and Technology Committee, Professor Justin C. St. John of Monash University noted that his group has been skeptical about the MRT based on the safety of the procedure and continued potential for transmission of the genetic defect. In his correspondence, he highlighted: It is not appropriate to merely suggest that the mitochondrion and the mitochondrial genome influence energy within the cells, they have a far more sophisticated role to play during development. It is well documented in the literature that mitochondrial DNA haplotypes predispose or protect individuals against severe diseases such as cancer (13), diabetes (14), Parkinson’s disease (15) and many other neurological disorders. (House of Commons Science and Technology Committee 2014, 35, emphasis in original) But living organisms are simply not like computers: they are complex, whereas computers are merely complicated. Even were it true that the functions of mitochondria are restricted to generating ATP, the idea that energy metabolism can somehow be isolated from the rest of the physiology of the organism, is biologically laughable. (House of Commons Science and Technology Committee 2014, 41) My impression is [that] the Government is doing all it can to contain and define these kinds of terms in ways that favour mitochondrial replacement being introduced as an Mitochondria influence fertility, ageing, longevity, cognitive ability. All these diseases that are caused by faulty mitochondria, with all sorts of symptoms…that tells you something about what mitochondria are involved in. So to say that they’re not important because they are only 37 genes, and at the same time say, “Ah, but they cause all these terrible diseases”––logically, that doesn’t match up.
Calculus of Genes
One of the most remarkable characteristics of the mitochondria debate in the UK is the use of what I refer to as a “calculus of genes,” a form of quantitative reasoning which uses a percentage calculation of DNA transmitted through the mitochondrial donation as a base for determining the donor’s relational status to the offspring. As I discuss later on, this calculus of genes played a role both in distancing MRT from the donor conception and germ-line modification line of argument and in reinforcing the idea that MRT is more akin to organ donation.
Even though it has its own DNA, mitochondria mainly provide energy for the cell. Because the mitochondrial DNA constitutes 0.1 percent of the DNA of the cell, it is considered insignificant in terms of determining the characteristics of an individual. However, this is not a settled issue in science (Bredenoord et al. 2011). Little is known about the mitochondria’s functioning (Thorburn, Dahl, and Singh 2001), but a few studies have linked mitochondria to cognitive functioning, Alzheimer’s disease and susceptibility to alcoholism (Picard and McEwen 2014; Mancuso et al. 2009; Hoek, Cahill, and Pastorino 2002).
The distinction between nuclear DNA and mitochondrial DNA was perceived as very important in determining the legal status of the donor. In “Mitochondria Replacement Consultation: Advice to Government,” the HFEA (2013b) reports that people’s views on the significance of mitochondrial DNA also determined how they conceptualized the relationship between the donor and the child. While in the beginning of the consultation about a third of the participants held the view that a child should have the right to know about their donor, those who did not think the child had a right to know, increased during this process from 31 percent at the start to 45 percent at the end (HFEA 2013b). The respondents who felt that no information or nonidentifying information should be provided saw MRT as more like blood or tissue donation rather than egg or sperm donation, and so concluded that the donor’s identity need not be disclosed (para. 6.47). Accordingly, it is possible that the number of respondents who saw MRT more akin to tissue donation than donor conception increased during the consultation. The government’s response to the DoH’s consultation also reflects this genetic thinking: Gamete donors, who contribute 50 per cent of the genes of a child born as a consequence of their donation, are not treated as the legal parent of any resulting child and there is therefore no justification to regard mitochondrial donors, who would provide only 0.1 per cent of the child’s genes, as such. (p. 29) The biggest problem is that this has been described as three-parent IVF. In fact it is 2.001-parent IVF. Less than a tenth of one per cent of the genome is actually going to be affected. It is not part of what makes us genetically who we are. It doesn’t affect height, eye colour, intelligence, musicality. (“MPs Say Yes to Three-person Babies,” February 3, 2015)
However, the majority of those who participated in the consultation felt that mitochondria donation is unique and is not directly comparable to any other form of donation, and a child should not have the right to know about their donor, and that mitochondrial donors should be anonymous (HFEA 2013b, paras. 6.57-6.63). As a result, the HFEA advised the government that mitochondrial donors should have a similar status to that of tissue donors and that children born of mitochondria replacement should not have a right to access identifying information about the donor (para. 1.13). This view was also endorsed by the Nuffield Council of Bioethics (NCoB 2012a).
The reports that NCoB published on mitochondrial donation (2012a) and donor conception (2012b, 2013) provide important insights into how the right to know is construed differently in these two practices, partly because of the assumptions about the effect of these techniques on the offspring’s genetic identity and partly because of the concerns about how MRT will be perceived by the public.
In both reports, the NCoB is cautious to avoid taking a genetic essentialist view of identity. In the donor conception report, rather than insisting that possession of identifiable information about one’s gamete donor is an essential component of one’s identity, The Working Group concluded that context has to be center stage in considering management of donor information (NCoB 2013). Similarly, in its report on mitochondrial donation, the group took the view that the social and genealogical information sought in donor conception is more about “seeking social information or a narrative related to a specific, limited element” of one’s biological origins (NCoB 2012a, para. 4.23). The NCoB’s view is in line with the ECHR law, which “privileges a narrative and developmental idea of individual identity” (de Andrade 2010, 429). In general, the international legal framework of human rights supports the right to personal identity, although in this context, personal identity is perceived as a narrative that each person needs to build during their lives. de Andre notes that in human rights law, “the relevance and weight attributed to the concept of genetic identity (as the right to identity encompassing genetic characteristics) has not been extrapolated,” and this approach prevents engaging with genetic essentialism that reduces a person to her genetic characteristics (2010, 432).
However, regarding mitochondrial donation, rather than abandoning the notion of genetic identity, the Working Group of the NCoB introduced a new categorization of identity. The report notes that MRT would introduce “only a very small change to the resulting child’s mitochondrial genetic identity,” in that the techniques would enable a person to be born who is genetically distinct from the person who might have been naturally conceived by his or her parents (NCoB 2012a, para. 4.25). Similar to the putative distinction between the mitochondrial donor and the “egg donor,” this new categorization of genetic identity also distinguishes the mitochondrial donor–conceived person from a donor–conceived person, whose genetic identity was altered 50 percent. The Working Group compares the change in “mitochondrial genetic identity” to that of the genetic makeup of a donor–conceived person, based on a “calculus of genes,” and as a result of this calculation it ascribes MRT less social significance than donor conception: A gamete donor contributes 50 percent of the child’s unique nuclear genetic make-up, the full complement of the child’s genetic contribution from either the maternal or paternal source. Taken alone, mitochondrial genes do not uniquely link the resulting child to their donor in the same way that a donation of nuclear genes would do. (para. 4.113)
Overall, the NCoB’s Working Group felt that the legal status of the mitochondrial donor would influence the perception of recipient families as to any social relationship that could be created by MRT (para. 3.21). The Working Group took the view that mitochondrial donors should not be treated as gamete donors and should not be mandatorily required to be identifiable to the individuals born from their donation (para. 5.14), an approach that was taken in the Mitochondrial Donation Regulations. The view of NCoB on MRT does not necessarily suggest that the council encourages anonymous donation in general. In contrast, more recently, regarding the information sharing in practices of donor conception, the NCoB’s Working Group concluded that “other things being equal, it will usually be better for children to be told, by their parents and at an early age, that they are donor-conceived” (NCoB 2013, para. 6.3). The Working Group also called for the state to take action to increase awareness among past donors to become identifiable and “nudge” parents toward disclosure (NCoB 2013).
Conclusion
During the UK’s mitochondria debate, those who supported MRT based their claims on simplified and reductionist assumptions about how genes make us who we are. This calculus of genes was evident in both public consultation documents and the accounts of those who promoted MRT. Such claims largely drew on donor’s genetic contribution to the offspring’s genetic makeup, rather than on the potential meaning of the donation for the parties involved. Overall, the donors were rendered invisible (Haimes and Taylor 2015) during the mitochondria debate, possibly because the donor’s identity in the context of MRT was deemed too disruptive for both donor procurement and the traditional notions of parenthood and family. As a result, the mitochondrial donor–conceived child’s interest in access to identifiable information about the donor was given less weight. This also meant that individuals who are conceived by the use of donated eggs and embryos in the UK are granted different rights based on whether their conception involves using nuclear DNA or mitochondrial DNA.
The UK will soon be home to at least five different types of adults who are conceived by the use of donated egg, sperm, and embryos. Specifically, from 2023, when the first children to whom the 2005 amendment applies will have reached the age of eighteen, there will be (1) those born with gametes donated after April 1, 2005, who will have access through a register maintained by the HFEA to identifying information about their donors; (2) those born with gametes donated between August 1991 (when the HFE Act came into force) and April 1, 2005, who will have access to nonidentifying information but nothing more unless their donor “reregisters” with the HFEA; (3) those born before the act came into force who will have access to no information at all through the register (though there may be records that can help at the clinics where they were conceived); (4) those conceived through nonclinical arrangements for sperm donation; and (5) those conceived at clinics outside the UK. Neither of the latter two groups will have access to information via the register. However, there was no discrimination between these individuals based on the nature and quantity of the donated reproductive material (eggs, sperm, or embryos) used for their conception until the arrival of MRT, which added a sixth group (6) those conceived by “mitochondrial donation” who will have access to nonidentifying information about their donors.
Should individuals born as a result of mitochondria therapy, as is proposed, be denied the right to access identifying information about the donor that is available to individuals born of donated gametes? It seems that, in part, the driving force behind MRT regulations was the assumption that more donors would come forward to provide eggs if their anonymity was protected. However, if maintaining donor anonymity is an important factor for the sustainability of donor conception, the government should reconsider its donor policy rather than causing discrimination for individuals who will be born as a result of MRT. As proposed by Pennings (1997) in the context of donor conception, the most obvious alternative disclosure policy in all forms of third-party reproduction would be to left the parties decide for themselves.
I argue that under the current policy, donor–conceived individuals can access identifying information about their genetic origins, and so it is discriminative to deny this information to the mitochondrial donor–conceived individuals. After all, the children born from MRT will grow up in a culture where donor-conception families are repeatedly told that it is in a child’s best interests to be told about their origins, including having access to identifiable information about their donors. Although having access to their donor’s identity might not be important to MRT offspring, it is unlikely that they will accept the assumption that they have less interest in knowing their donors than donor–conceived individuals based on a simple calculus of genes. The question is not who should be entitled to their genetic origins, but whether a calculus of genetic relatedness is a good basis for considering a child’s interest in the right to know.
Griffiths (2016) argues that MRT is an example of how science and regulation seek to reconfigure traditional boundaries surrounding parenthood and the family without challenging the existing order, which is also at the center of UK’s family law and legislation (McCandless and Sheldon 2014). Yet, there are wider implications of the current mitochondrial donor policy. The public consultation documents and the media accounts of the promoters of MRT reveal a rhetorical strategy based on undermining the significance of mitochondrial DNA with respect to the nuclear DNA. The latter is often framed as the “essence of identity and the basis of human difference” (Nelkin 1994, 26). Dar-Nimrod and Heine (2011, 800) warn that genetic essentialism reinforced by the representations of genes in public discourses is dangerous, because “people are influenced by scientific arguments regarding the role of genes in their lives in some profound ways that are distinct from learning about other kinds of scientific arguments.” Genetic essentialist biases may play a role in shaping people’s understandings of race, gender, sexuality, disability, and disease, or even effect the ways they are treated by those who are in power, as exemplified by the dark history of eugenics (Kerr, Cunningham-Burley, and Amos 1998). The reductionist and simplified accounts of genes also influences the ways in which we understand what makes us human and the rights we have as humans. Although the current MRT policy might be desirable if the UK wants to be in the forefront of mitochondria research, we have to be mindful of the wider implications of such genetic thinking, which legitimizes defining human and human rights based on a calculus of genes.
Footnotes
Acknowledgments
I am grateful to Noa Vaisman for her thoughtful and detailed insights about the piece presented here. Many thanks to Edward J. Hackett and the anonymous reviewers for their constructive comments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.