
Abstract
This article examines the phenomenology of nursing care delivered through Välkky, a full-body teleoperated humanoid robot trialed in a Finnish hospital ward in 2023. Bringing science and technology studies into dialogue with phenomenology, we analyze qualitative data from observations, focus groups, and interviews with nurse-operators, managers, roboticists, and one patient involved in the pilot. We argue that Välkky's deployment constituted a “robot drama” in which the frictions between robotic imaginaries and situated clinical practice produced “infrastructural inversions,” making visible normally tacit dimensions of nursing care. To conceptualize these dimensions, we develop the notion of “experiential care infrastructures”: the embodied, affective, and relational conditions that underpin care but can be overlooked in task-based approaches to robot design. Our analysis shows that Välkky afforded limited experiences of telepresence, and that nurses found the technology to interrupt rather than enable caring relations. We conclude that the design and deployment of telepresence robots in healthcare settings must attend to experiential infrastructures that make ethical and relational care possible.
Introduction
Recent science and technology studies (STS) scholarship has interrogated the techno-solutionist narratives of robots solving the “care crisis” (Dowling 2021), where aging populations, crises of funding, poor care staff retention, and burn out will be purportedly solved by introducing humanoid robots to perform basic care tasks (Maibaum et al. 2021; Bender 2025). While the status and utility of care robots in healthcare remains contested, development of these technologies continues at pace, partly driven by innovation and funding policy (Maibaum et al. 2021), coupled with a sci-fi infused imaginary of what robots should, and hopefully will, be able to do (Sparrow 2019; DeFalco 2020). Moreover, the interest in care robots, particularly telepresence robots, intensified during the COVID-19 pandemic, when robots were explicitly positioned as solutions for automation and infection control (Khan, Siddique, and Lee 2020; Aymerich-Franch and Ferrer 2022; Sumartojo and Lugli 2022). Telepresence robots are not autonomous, but controlled remotely by clinicians, and can be used for consultations, family visits and, in some cases, to perform basic clinical tasks at a distance (e.g., from another room, town, or even country).
Using a telepresence robot in a clinical context is a form of “telemedicine” and “telecare,” describing the phenomena where healthcare is delivered at a distance and mediated through technology (Oudshoorn 2011; Craig and Patterson 2017; Greene 2022). When a clinician uses a telepresence robot, they are no longer physically copresent with the patient they are caring for. Instead, they are “in” the robot, and their “presence” with patients is mediated through the robot who acts as their avatar. Although they lend “presence” to remotely local clinicians, insofar as clinicians can be proximate to patients through a mediating technology, most existing telepresence robots in medical settings are “restricted to communication” and, as Laitinen, Nielmelä, and Pirhonen (2019, 379) note, “cannot provide equally embodied interaction,” resulting in consultations that amount to the conveying of “instructions instead of action.” Addressing these limitations, telepresence robots have been developed to provide more “hands-on” clinical interventions (e.g., Akibot, RP-Vita robot), enabling more complex clinical tasks at a distance, including physical examinations and possible diagnoses.
In this paper, we explore the case study of a hands-on telepresence robot, Välkky, a full-body teleoperated humanoid robot developed by Touchlab, an Edinburgh-based deep tech robotics company (Figure 1). Our aim is to bring STS and phenomenology together to explore how the experience of operating the robot, particularly the phenomenology of “presence,” has implications for nursing care where telepresence robots are positioned as a viable vehicle for care delivery on hospital wards. Välkky has been created to provide physical contact through enhanced haptic capabilities, and in 2023 was deployed in a Finnish hospital to trial the provision of nursing care at a distance to patients on a busy adult ward. Nurse-operators controlled Välkky to move around the hospital ward and to interact with patients, other staff, and family members. The Välkky robot is a recent example of more “enriched” telepresence in healthcare contexts. Not only can clinicians see, hear, and talk through the robot, Välkky is also equipped with e-skin, which permits haptic sensitivity, along with an articulated human-like hand, which creates the potential for fine motor control and subtle movements, potentially enabling a safe and close physical contact between the robot and patients. In this way, Välkky is a medium that can act as a “conduit” for the remote user, conveying and projecting their actions and communication appropriately into the remote environment (Guevarra 2018, 746).
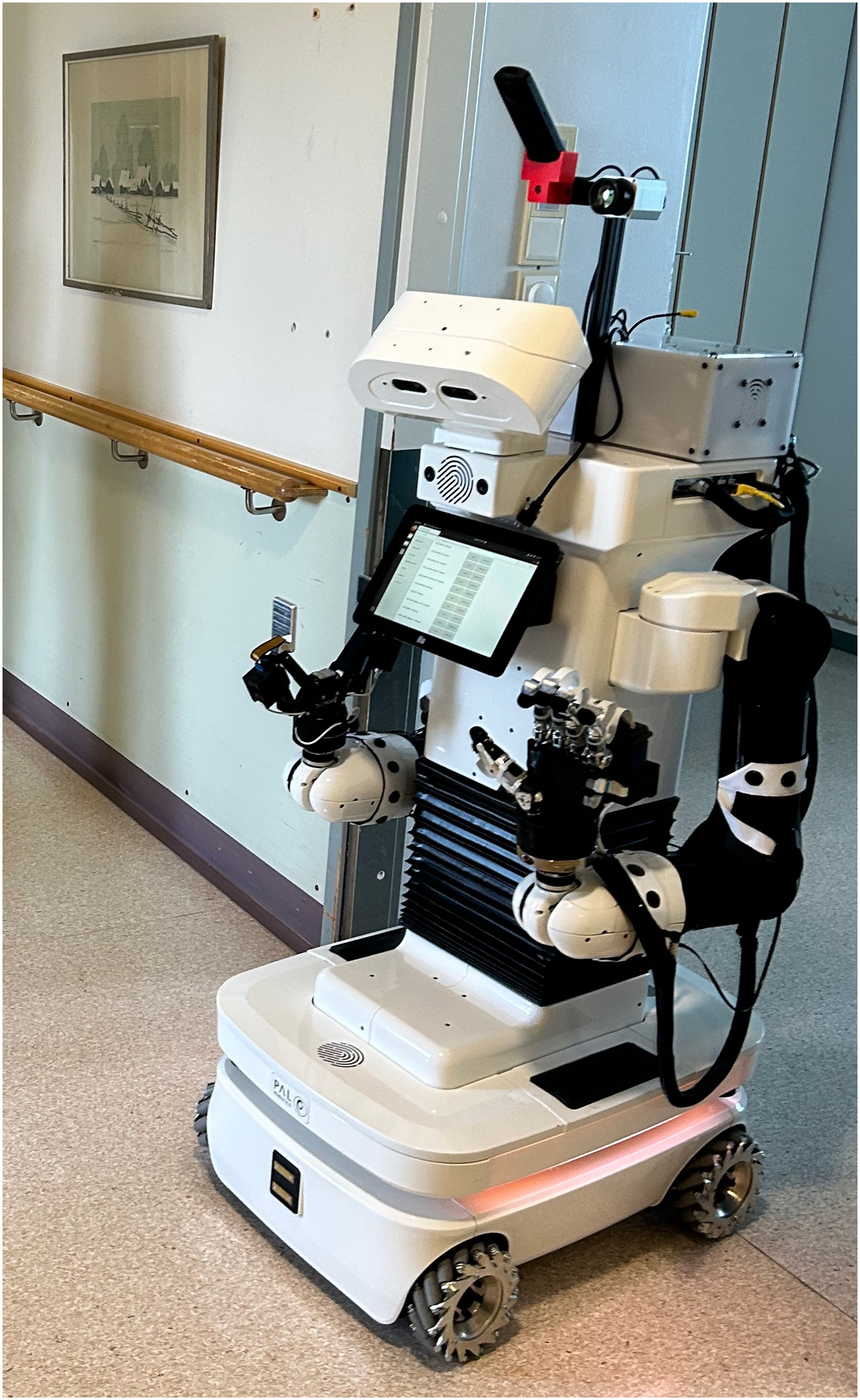
Välkky robot. The photo shows Välkky in a hospital corridor. The robot is a white PAL Robotics modified TIAGo robot. It is white, has a basic humanoid form—two arms, torso, head—on a mobile base with wheels. The robot has articulated arms, with one human-like hand, with four fingers and a thumb, and the other “hand” is a gripper tool. There is a screen display at the robot's chest area facing outward, and a microphone and camera above the robot's head. Image taken on May 27, 2023, Helsinki, Finland.
When operating the Välkky robot, nurses sat in a scorpion chair, an ergonomically optimized chair which causes less strain to a user's neck or back, designed to encourage a sense of immersion in the technologically mediated world. A virtual reality (VR) headset was used to create further immersion and relayed 360-degree camera input from Välkky, while basic joystick controls were used to move and turn the robot (Figure 2). Välkky is a modified PAL Robotics TIAGo robot with a mobile base, with a basic anthropomorphic form: it has arms, a torso, a head that turns, facial features, one human-like hand, and one gripper hand. When the nurse-operator turns their head, Välkky's head turns too. When operating Välkky, nurses could “visit” the ward through “telepresence,” a form of mediated presence (Lee 2004, 29), and interact with patients, staff, and family members through “teleaction” (Hirche 2010, iii), enabled by the robot avatar. In the post-COVID medical landscape, Välkky has been positioned as offering a solution to infection control (Helsinki 2023), and as a techno-solution for an aspect of the “care crisis,” specifically poor staff retention. It has also been discussed explicitly as a technology that could improve clinician workload and help with physically taxing or repetitive tasks (OPSI 2023).

Teleoperator with trainer. The photo shows one of the research team members sitting in the scorpion chair using a virtual reality (VR) headset and hand controls to operate Välkky. May 27, 2023, Helsinki, Finland.
To bring phenomenology further into dialogue with STS scholarship (Zeiler and Käll 2025), we draw on Lipp's (2022) conceptualization of a “robot drama,” along with Bowker and Star's (2000) theorization of “infrastructural inversion” to critically examine the phenomenological experiences of nurses trained to teleoperate Välkky to deliver care at a distance. Through our discussion, we explore what we term “experiential care infrastructures,” which includes the phenomenological aspects of care delivery—such as embodied contact, vulnerability, affect, intimacy, trust, and recognition—that are foundational to infrastructures of care in clinical spaces. These “experiential care infrastructures” are often taken-for-granted aspects of care tasks. This means these experiential aspects of care are usually the tacit background for care delivery, and consequently, are frequently overlooked in the development and design of care robots (Liedo, Van Grunsven, and Marin 2024). Hence, the reductive task-based approach to care—where complex acts of care are “fragmented, dissectible into discrete tasks that can be matched with certain robotic capabilities” (Lipp 2022, 6)—dominates the design, development, and deployment of robots in clinical settings (Wynsberghe 2013). By exploring experiential care infrastructures within robot dramas, we argue that the development of assistive telepresence robots, such as Välkky—which directly enact human care from a distance, mediating the “human touch”—must explicitly consider the affective and experiential dimensions of care in how robots are designed and deployed. In particular, we argue that understanding the phenomenology of telepresence, or how clinicians experience “presence” (or not being present) when using telepresence technologies, can reveal important dimensions that are usually tacit and taken-for-granted about how care is delivered and experienced in clinical settings.
We will develop our argument by examining the phenomenology of telepresence (i.e., the experiences nurses had when attempting to deliver telecare while “in” Välkky). In doing so, we will examine the invisible and experiential “infrastructural arrangements” (Bowker and Star 2000) underpinning the successful delivery of care, and how these were disrupted or sometimes broke down when Välkky was in use. By framing the analysis of our fieldwork through “robot dramas” and “experiential care infrastructures,” we show how the phenomenological experiences of nurses operating Välkky are made possible through technological “transparency,” an experience where technology is “incorporated” into one's body schema and recedes from awareness. Välkky is a mediating technology, which affords nurses a feeling akin to being on the ward with patients. When coupled with successful skill acquisition, Välkky does not “get in the way” of care, but rather enables motor action in a remote environment. Building from this, we examine two modalities of social presence that nurses strived to achieve through their control of Välkky: (i) presence felt through affective and social resonance, where interpersonal presence and relations of care are transmitted through the robot avatar; and (ii) presence enabled through recognition, where nurses strived to have their social and human existence affirmed while operating the robot. We will discuss how Välkky's presence on the hospital ward, and the nurse-clinicians’ own attempts to “strive for presence” through Välkky, revealed the deeply embedded experiential care infrastructures (that were usually unnoticed and taken-for-granted) that govern the practices and expectations of nursing in hospital settings.
Our analysis highlights the current limitations in telepresence robotics when considering experiences that are central to ethical care, such as affect, recognition, vulnerability, trust, and intimacy (Liedo, Van Grunsven, and Marin 2024). We argue that these user experiences need to be central to robot design, development, and deployment. However, our contribution is broader, as the Välkky case study shows the possibilities of innovation and experimentation in how healthcare is delivered. Specifically, we argue that the “infrastructural inversions” enacted by Välkky's presence on the ward can inform posthuman, technologically driven re-imaginings of what care could be, or might become.
Robot Drama and Experiential Care Infrastructures
Lipp (2022, 12, 11) theorizes a “robot drama” to be the “staging” that happens in robotics trials and test situations, where environments are changed and controlled, in “order to support the robot's operation.” The trial of a robot in a care or clinical space is a drama that unfolds with various “actors” (e.g., end users, roboticists, engineers, patients, clinical staff, and their managers) and theatrical logics, where “scenes” are “staged” to test task-based capabilities. In the case of a care robot entering a clinical space, the robot is inserted into an existing “infrastructural arrangement” (Bowker and Star 2000), where an “infrastructure” (Bowker and Star 2000; Bowker et al. 2010) can be understood as the embedded, installed, and largely unnoticed systems, practices, material objects, standards, and social arrangements that “shape and enable practice” (Weiner and Will 2018, 271). Infrastructures recede into the background of a system or practice and become the tacit, and hence the “natural” or “normal” background against which the action happens.
STS scholars have largely discussed infrastructures as being made up of materials, technologies, and spaces, such as physical entities and artifacts (e.g., buildings, objects, forms, plugs) and classification and standardization systems (e.g., conventions regarding measurements, temporality, work practices) (Bowker and Star 2000, 35ff). Moreover, recent discussions about “care infrastructures” have pointed to the “work” carried out by health professionals and others as maintaining the infrastructures of care in clinical and other spaces (Langstrup 2013; Weiner and Will 2018; Carboni et al. 2025). Clinicians, patients, family members, and others in clinical settings do “constant work” for the “maintenance of an infrastructure” so that it can “remain durable” (Langstrup 2013, 1010). Hence, a care infrastructure does not rely merely on materials, artifacts, technologies, and spaces to function and endure, but there is a crucial experiential dimension, or “phenomenology” inherent to the success of any infrastructure of care (Bowker and Star 2000, 47). Namely, care is embodied; human actors are enacting tasks, practices, and interactions, which underpin the successful delivery and receiving of care. For infrastructures of care to be “embedded,” “transparent,” and “invisible” (Bowker and Star 2000, 35), the work done by care professionals in clinical spaces must also become embedded, and a “naturalized familiarity” must be part of the phenomenology of the experience of both care workers, and those receiving care. Hence, care infrastructures necessarily have an experiential dimension, and we discuss experiential care infrastructures as the taken-for-granted and embedded work that underpins, and makes possible, the delivery of care. Experiential care infrastructures consist of elements such as touch, other embodied contact, intercorporeality, emotion, vulnerability, affects, intimacy, trust, and recognition.
In his theorization of robot dramas, Lipp discusses a case study of a robot deployed in an apartment within a care home—the existing infrastructural arrangement into which the robot was inserted. In other words, the space was not designed and built with the robot in mind, but was a pre-existing material and spatial arrangement into which the robot was artificially placed. As Lipp describes, during the course of this particular “robot drama,” expectations about what the robot should be able to do were recalibrated, and the test site (the apartment) was modified to accommodate and test the robot platform (e.g., shelves are emptied, carpets are removed, decorations are covered). As Lipp (2022, 6, 7) explains, the drama unfolds in “friction between vision and demonstration,” or in other words “between the imaginations about what to expect from robots and the technical practices of programming, building, and operating those machines in concrete environments.” The robot drama involves the theatrics of roboticists staging, controlling, and modifying experiments, where the robot in situ creates a series of what Bowker and Star (2000, 34) identify as “infrastructural inversions,” where “normally invisible” technical networks and standards making up an infrastructure are foregrounded and made prominent. For instance, the usually “invisible” presence of the carpet in the apartment is rendered salient when the robot is unable to drive over it (Lipp 2023).
The trial, which brought Välkky to a Finnish hospital, was a classic “robot drama” involving hospital wards as the infrastructural setting into which the robot was inserted. The actors were nurse-clinicians, roboticists, nurse managers, and patients. Roboticists from Touchlab attempted to enact their “visions of care robotics,” which had piqued the interest of hospital managers, funders, and investors, and to “test phenomena of human–robot interaction” in order to refine and improve their prototype technology (Lipp 2022, 2). Unlike the assistance robot discussed by Lipp, Välkky is a telepresence robot, a mobile machine that can enable an operator to be “embodied” in the form of the robot from a remote or distant location (Choi and Kwak 2017). The nurse-operators were trained to work through Välkky—a robot that is both a “medium” and a “social being” (Guevarra 2018, 746)—in order to enact and maintain the (tacit, invisible, taken-for-granted) care infrastructures of that hospital ward.
Hence, the Välkky “robot drama” involved a robot inserted into an existing care infrastructure with human actors negotiating the “scenes” and “stages” of robot functionality and interaction. In addition, as a teleoperated robot, Välkky brought the human into the robot. Välkky is both human and technology “mangled” together, to invoke Pickering's (2008, 1) reconceptualization of research practice in science and technology, where “the human and the nonhuman are recognized as open-endedly becoming, taking on emergent forms in an intrinsically temporal ‘dance of agency.’” The nurses operating Välkky were at the heart of the “drama,” and the phenomenology of their experiences of trying to deliver care through teleoperation and telepresence—the “dance of agency” enabled by enmeshing human and technology—are the foundation from which the experiential care infrastructures were made salient.
In the case of Välkky, STS conceptual framings about how norms and bodies “co-emerge with healthcare practices and models of knowing” (i.e., infrastructures) must be coupled with phenomenological analyses that can show how “one's taken-for-granted lived body and habits” are shaped and reified by normative practices (Zeiler 2022, 132, 128). Following recent feminist scholarship, in the analysis that follows, we bring phenomenology and STS approaches together (Zeiler and Käll 2025). This enables us to garner a deeper understanding of how subjectivity is embodied through lived experience in addition to being shaped through interactions and entanglements with objects, discourses and power structures. In doing so, our analysis will focus on how the experience of telepresence disrupted taken-for-granted expectations of what delivering care on a hospital ward consists of. This justifies our argument that the development of assistive telepresence robots must explicitly consider the affective and experiential dimensions of care in how robots are designed and deployed.
Study Design and Methods
Our analysis draws on qualitative research data generated during a study involving sociologists and a philosopher participating in a pilot project led by Touchlab (Nettleton et al. 2024). In late 2023, Touchlab roboticists installed Välkky in Laakso Hospital in Helsinki, Finland, and delivered training for nurses, to teach them how to operate Välkky in both an empty ward and a busy adult ward. The 2023 trial was a world-first attempt to bring a nurse-operated social telepresence robot into a hospital ward to perform basic clinical tasks, while interacting with patients.
Our team collaborated with Touchlab to collect qualitative data during the trial, which comprised fieldwork observations on both wards during training sessions; conversations with key informants (roboticists, designers, nurses, patients); focus group discussions with nurses (n = 3 groups of four, four, and two participants); as well as semistructured interviews with nurse-operators (NO, n = 6), nurse managers (n = 2), and one patient (n = 1). Five other patients had agreed to participate, but for various reasons (e.g., illness, hospital discharge, medical procedures) only one patient interview was completed. Focus groups were carried out on the first site visit when training had only just started (May 2023); the other interviews were all conducted some months into the pilot (end of August 2023). The nurses in the group interviewed at the start of the pilot were introduced to the teleoperated robot at an event held beneath a large shopping mall in Helsinki, where there was a network of rooms with architectural design templates of the new hospital.
The focus groups and interviews were conducted in a functioning hospital on a nonoperational ward next to the teleoperation site. All participants were complete novices when it came to operating a telepresence robot, although some of them had experience with other technologies (such as video games or operating complex vehicles). Most of the nurses received one or two introductory training sessions on the telepresence system. The six individual in-person interviews with nurses were carried out two months later, further into their training and after they had worked alongside the robot in the wards. The interviewer observed training sessions (which usually lasted an hour or more) during which time she also followed Välkky in the operational ward, as it was teleoperated by a nurse supported by one of the design team. Qualitative in-person interviews, following written informed consent, were conducted by the researcher together with a Finnish researcher who was able to translate when needed. All but two interviews were conducted in English, and the remaining two were a mix of Finnish and English. Further meetings with the engineers prior to and after the site visits provided updates on progress, hitches, developments, and possibilities for care work. Observations and data collection spanned varying sites, including the hospital wards, the site of the prototype new hospital under construction, and the training laboratory.
Recorded interviews were transcribed and, along with fieldnotes, uploaded to a secure shared drive and read by all authors. Analysis of the empirical material for this paper comprised familiarization where the philosopher and sociologists on the team read the data to summarize recurrent issues. Themes were also identified iteratively through discussion informed by the research team's expertise in STS, embodiment, phenomenology, and healthcare policy and practice. The data were then coded to facilitate retrieval. Ethical approval was secured in Finland from the City of Helsinki (Helsinki Helsingfors—Research permit application Ansökan om Aorskningstillstånd Social and Health Care, Social and Health Sector, December 14, 2022), and informed consent was obtained from all participants.
Telepresence on a Hospital Ward
Embodied social presence—or “being with” a patient such that trust, intimacy, vulnerability, and emotions can be experienced—is a fundamental, and usually tacit, part of the “work” that happens in care delivery. While care is a multivalent and complex concept, which is necessarily “ambivalent” and “contextual,” there is no doubt that it is also “relational” (Martin, Myers, and Viseu 2015, 631). Embodied social presence is a form of affective copresence that makes possible the execution of caring in a hospital ward setting, rather than just the execution of “fragmented” or “discrete tasks” that might lead to a physical or material outcome related to care delivery (Lipp 2022, 6). As such, the “work” performed to enact care within a hospital ward setting is not only functional and pragmatic (e.g., changing bed sheets, mopping floors, dispensing medication), but also involves human relational practices of trust, vulnerability, attention, attachment, touching, intimacy, and feeling, among others (Murphy 2015; Liedo, Van Grunsven, and Marin 2024). A key challenge of using a telepresence system to deliver relational care is that the usually tacit and taken-for-granted experience of “being in the same room” needs to be recreated and reconstructed through the use of technology. In the case of Välkky, nurses are “in” the robot, and their “presence” on the ward with patients is mediated through the robot, which acts as their avatar.
In order to feel embodied and “present” on the ward—and hence available and able to perform acts of care—the corporeal and sensory demands of the local site (where a nurse's body is located) must recede from awareness. In particular, the technology the nurse is using, and their own physical body must not dominate their awareness and perception—these must be “transparent.” A simple example from the phenomenologist Don Ihde illustrates this. When we wear eyeglasses, we quickly become used to the weight of the glasses on the ears and nose, and they become incorporated into the body's tacit sense of itself: “My glasses become part of the way I ordinarily experience my surroundings; they ‘withdraw’ and are barely noticed, if at all” (Ihde 1990, 73). The relation of mediation between “I-glasses-world” becomes “(I-glasses)-world” (Ihde 1990, 73). The “mundane technology” becomes “incorporated” into one's tacit bodily boundaries and intrinsic to our relation with our environment, ultimately “expanding affordances” (Michael 2000, 115). Similarly, technologies that enable telepresence in a remote location must likewise be incorporated into a body's tacit sense of itself, such that these technologies (headsets, joysticks) are not perceived as a technological “medium,” but recede into the background of awareness through an experienced “transparency,” enabling the focus of perception, attention, and action to be transported to the remote environment.
Roboticists trained nurses to use the equipment (scorpion chair, joystick, VR headset), which enabled basic control of Välkky on the ward (i.e., moving through the physical hospital infrastructures, down corridors, and into and out of hospital rooms without bumping into door frames, walls, or people). When “in” Välkky, the infrastructures that previously disappeared from awareness, thoroughly taken-for-granted and naturalized, became salient for the nurse-operators. For instance, instead of tacitly “knowing” the width of a doorway, the nurses had to explicitly “figure out” how wide the entrance to a hospital room was, and precisely where to position their robot body in order to be able to pass through it (Figure 3). Being “in” Välkky immediately afforded infrastructural inversions for the nurse-operators who were immersed in a phenomenological reality where the tacit and taken-for-granted perceptions and motor actions that had previously characterized their presence on the hospital ward had to be painstakingly relearned and renegotiated.

Välkky moving through a hospital room doorway. May 26, 2023, Helsinki, Finland.
For the most part, participants reported that experiences of “presence,” or of “being there,” were fleeting or disrupted, with a feeling of being in two places at once, or having attention split between the local and remote locations frequently reported (NO1, NO2). Participants described how their own bodies or the limitations of the technology “got in the way” of them feeling “present” on the ward. For some participants, using the VR headset led to nausea, dizziness, and headaches, common side-effects when using head-mounted displays (Cash and Prescott 2019). Ongoing issues with the bandwidth available on the hospital's internet network led to low resolution, along with experiences of lag and jumpiness in the video feedback.
In addition, achieving meaningful presence on the ward was also dependent on being able to successfully operate Välkky and achieve a technologically nested experience that, following Idhe, can be configured in this manner ((body-[headset + joystick + chair])-Välkky)-world. This involved a training process where nurse-operators acquired the embodied skills to remotely control Välkky through the ward, and execute more subtle motor movements such as approaching people, lifting objects, and handing objects to others. Participants reported varying levels of ease and comfort with learning how to operate the robot avatar. Those with experience using similar joystick controls or multitasking through technological mediation, for example, in gaming, or in one case due to being trained to operate a complex vehicle, reported that they found it easier, or more intuitive, to remotely control Välkky.
Our data clearly demonstrated that limitations in feeling physical “presence” on the ward were shared by all the nurses who took part in our study. This was likely due to short time spans for training, coupled with ongoing broadband issues that limited Välkky's functionality and sensory capability (e.g., the e-skin technology enabling touch was not functional for most of the trial). To varying degrees, all participants reported the technology at the local site (e.g., headset) not being experienced as transparent, and “getting in the way” of their perception of the ward. As a result, there was always some need for conscious attention to movement and action in the remote site, as opposed to the prereflective skilled movement that characterizes motor agency when it is functioning successfully (Dreyfus 1999; Benner 2004; Merleau-Ponty 2012). Roboticists had hoped that Välkky would enable experiences of “robotic re-embodiment,” where the essential phenomenological features of embodiment, namely perception, the ability to execute embodied skills, agency and action, communication, and sociality, are present in the remote environment via a robot avatar (Dolezal 2009, 220; Besmer 2015). However, for the most part, the experience of re-embodiment remained elusive.
Despite these limitations, all participants reported being able to achieve some degree of social presence with the patients they visited while they were “in” Välkky, and there was a concrete sense among most nurses and other hospital staff that the technology would eventually improve, and it would not be long before meaningful “presence” through Välkky was a concrete possibility.
In the next two sections, we explore two modalities of embodied social presence that nurses strived to achieve and which the data revealed to be key to successful care and nursing practice: (i) presence felt through affective, intracorporeal, and social resonance, where interpersonal presence and relations of care are transmitted through the robot avatar; and (ii) presence enabled through recognition, where nurses strived to have their social and human existence affirmed while operating the robot. By examining these experiential dimensions of care infrastructures, some of the invisibilized practices and taken-for-granted relational acts that are part of the embedded and usually transparent fabric of life in a hospital ward were “inverted” and revealed. These experiences made salient the affective and experiential dimensions of what might be considered “successful” care practice, and how these insights might in turn guide telepresence robot development, design, and deployment in clinical settings.
Feeling Embodied and Social Presence with Patients on the Ward
Nursing work on hospital wards is care work: a relational and physical practice which often involves close, intimate contact between human bodies. It is “body work” too, which is premised on the idea of “direct, hands-on activities” (Twigg et al. 2011, 172). This necessitates a physical copresence (Cohen 2011) because “to make a difference in another's suffering, a nurse needs to be close” (W.J. Austin 2011, 162). In fact, “presence” is frequently positioned as central to good nursing practice. In his book La Souffrance, the French philosopher Bertrand Vergely writes: “A nurse is a giver of presence, a giver of listening, a giver of gestures and of words” (W.J. Austin 2011, 162). Effective nursing practice hence involves intimacy, trust, emotions, and touch (Van Dongen and Elema 2010), where human touch is frequently positioned as an “essential part of nursing” that can influence patients’ well-being and sense of security, while enhancing nurses’ job satisfaction (De Luca et al. 2021). Through being physically and emotionally “present” with a patient, a nurse can address a patient's physical, emotional, and psychosocial care needs.
However, this conception of nursing practice has increasingly become an idealized abstraction and many nurses frequently bemoan the “loss of their human connection to their patients” (Gordon 2006, 309). Contemporary healthcare landscapes increasingly prioritize task-based care, heuristic checklists, and mechanistic models of communication over genuine human connection (Hartrick 1997; W.J. Austin 2011; Sims et al. 2020), resulting in a trope of the nurse as a “robot” coming up repeatedly in the literature. Task-based models of care fragment work and care pathways (Fernández-Basanta, Lois-Sandá, and Movilla-Fernández 2023). As Gordon writes, the nurse “becomes a mechanical robot fulfilling a certain number of predetermined tasks” (Gordon 2006, 281). In Austin et al.'s study about compassion fatigue in nursing, one nurse explains: “you must feel like you’re a robot. You’re going through the motions, but there is some disconnection… [you’re] not really feeling their suffering” (W. Austin et al. 2009, 204).
In task-based, rather than relational, care, what becomes attenuated or lost is a “mutual vulnerability” that is “inherent” to the nurse–patient relationship (W.J. Austin 2011, 161), and this, nursing scholars argue, diminishes the potential for relational capacities, such as authenticity, responsiveness, intentionality in relating, and the honoring of complexity and ambiguity, that are theorized to be central to effective and humane nursing care (Hartrick 1997). With that loss is an attenuation of the tacit bodily exchange that characterizes genuinely being with another subject; a back-and-forth between bodies that is both affective and physical (Harrison, Elizabeth, and DeLuca 2019). In more relational modes of caring, through what has been termed an “interbodily resonance” (Fuchs and de Jaegher 2019), nurses and patients can “tune into” each other's bodies to varying degrees, leading to a level of communication and embodied responsiveness that enable the flow of social interaction and can lead to meaning-making (Harrison, Elizabeth, and DeLuca 2019) and different sorts of “ethical affordances” (Keane 2014). These concerns about dehumanization—becoming robotic with patients—come hand-in-hand with worries about diminished emotional and social presence. While being physically copresent with a patient, the nurse is not afforded the time or resources to be emotionally or socially present.
The parsing out of physical presence from the ability to be socially and emotionally present with patients was key to the experiences reported by the nurses who were operating Välkky. In what should perhaps not be surprising at all, since nurses became literal, and not just figurative, robots on the ward, participants indicated that they had to adopt a more mechanistic model of relating to patients and others (e.g., staff, family members, researchers) on the ward. All participants pointed to how the tacit embodied exchange between their bodies and their patients was unsettled or lost when engaging through Välkky. In other words, experiential care infrastructures were disrupted by delivering care “as” Välkky. It was, therefore, more difficult for nurses to pick up on embodied cues and to respond spontaneously and appropriately: NO2: To be honest, it is quite difficult to keep up the conversation through the robot with the patients, because I can’t see their expressions and their non-verbal hints. NO3: It is awkward and interesting like I am having difficulty interacting with patients with the robot, like part of it is with the camera quality. I am having a hard time recognizing the patients, I have to go pretty close to see them. Today we had some audio difficulties like there had been some changes to the audio to try to address the voice loop from the operator but then it also made everything around me unclear, like if there are more than one people speaking around me then it is very unclear. But in the ward, moving around in the ward is okay but interacting with patients is kind of unnatural to me, because...there is lots of lacking in the interaction. NO6: As a human if I want to hear the patient better, I would lean over, but as a robot I can’t. As a human I can extend the arms and the arms can get close but the robot itself can’t. If I increase the volume, it doesn’t only increase the volume of what I hear from the patient, it increases all the other noises as well, so that doesn’t help. [translated from Finnish] NO4: I don’t think the robot could replace a nurse. Interviewer: Why not? NO4: Because a nurse really needs to be present with the patient, and feel the patient's feelings and emotions and offer support to patients…I think you could be going through the ward talking to patients, maybe giving them a glass of water but still it doesn’t feel, it's not the same as a human nurse. NO5: The patient wants…[moves arm to indicate physical touch] compassion, but if the patient just wants something like that, I don’t think the robot can do that kind of thing, emotional support for the patient.
Presence Enabled Through Recognition
As Välkky moved about the ward, patients and nurses regularly greeted the robot as Välkky, interacting with the robot as though it were an autonomous entity. Välkky became a character on the ward, enacting a different kind of “robot drama:” when Välkky raised its arms patients commented “it's angry,” when it shimmied sideways, staff and patients laughed at its “dancing,” and when Välkky waved, patients and staff waved back and chattered informally with it (Nettleton et al. 2024). In fact, for many on the ward, it was not initially clear that there was a nurse-operator controlling Välkky's movements and actions: NO1: one time a visitor greeted me, and I talked to them and they said “Oh the robot is talking” and then they realized I was operating the robot and talking. They didn’t realize, and the nurses explained it was me talking while operating the robot. They were a bit surprised at first that the robot was talking. NO3: For myself I feel that I am rolling through the door and waving and asking questions but I think it is hard to make...a fluent and natural conversation as a robot. Interviewer: You say they recognize your voice—do you feel as though they are talking to you or to Välkky? Or to both. NO3: To the robot I feel. Interviewer: So, you don’t feel they are talking to you? NO3: No. Interviewer: What makes you think that? NO3: Maybe like my own feeling, but then I am talking to them they are handing me stuff like for the robot. I’m just the person controlling [it] and they are interacting with the robot. They really haven’t mentioned my name, it's not like they say, “Hey you are the nurse from the morning.” It's not like that. But I am also introducing myself as “Oh hey, I’m Välkky.”
Recognition is enacted politically through the conferring of rights and respect through legal protections (Honneth 1995), but it is something that is also enacted on a micro-level, through interpersonal interactions (Honneth 2001). One's own recognition—and concomitantly conferring recognition to others—is a central component of the tacit embodied exchange, or back-and-forth between bodies that characterizes human encounters. When there is a lack of expressive acknowledgment, experiences of nonrecognition and misrecognition might occur. These experiences can lead to feelings of dehumanization, disempowerment, alienation, and invisibility within social interactions (Honneth 1995; Petherbridge 2022).
The patients receiving care from Välkky did not immediately know (nor could they see) which nurse was “in” Välkky at any given time. The “making visible” of the person in an interaction, which Honneth points to as crucial for recognition, is not immediately achieved through Välkky's engagement with patients. For some on the ward, the “presence” of the nurse was not at all apparent when Välkky appeared. They just saw a robot that appeared to act autonomously. For others, even when a nurse was recognized as “present” “in” or “behind” Välkky, they were not seen, nor easily heard or communicated with.
Conclusion
Following concerns about achieving embodied and social presence, along with recognition on the ward, our analysis raises questions about how Välkky's robot body stands in for flesh-and-blood nurses on the ward. These questions arise because of the “frictions between vision and demonstration” in the Välkky “robot drama,” and the repeated inversion of experiential care infrastructures, where previously tacit and taken-for-granted aspects of care (e.g., being able to spontaneously touch a patient in order to comfort them), are disrupted by the use of the robot avatar. There has been important work highlighting the need for ethics, care, and a consideration of emotions to be central in care robot design (Wynsberghe 2013; Liedo, Van Grunsven, and Marin 2024). Drawing on the concrete aspects of what was highlighted in the Välkky trial, we argue that the design and development of telepresence robots that directly transmit human care from a distance must explicitly consider the affective and experiential dimensions of care, and integrate these into how robots are implemented into healthcare systems.
As a telepresence robot, Välkky has a fixed morphology; in other words, it looks the same no matter who is operating it. Unlike avatar identities in online video games, where a user's appearance, expressivity, and vitality can express their identity (Ekdhal and Osler 2023), a telepresence robot avatar has a fixed appearance. As a result, nurses’ identity characteristics related to race, ethnicity, gender, age, and ability, among others, are not apparent, even if patients can hear a nurse's voice. No matter which nurse was operating Välkky, their physical identity was homogenized “behind” Välkky's robot morphology—a shiny white boxy humanoid robot.
Consequently, telepresence robots in clinical settings run the risk of turning nurses into “interchangeable commodities” (W.J. Austin 2011, 164), rather than human actors forging authentic, vulnerable, and caring relationships with others. As Mohammadi et al. (2024, 1486) suggest, nurses bringing their “historical and cultural background to the nursing situation” is key to successful communication, which has been shown to increase the quality of patient care, while also decreasing its cost. The effacement of one's historical and cultural background, along with one's identity characteristics, has implications for “ethical affordances” to return to Keane's idea, and also for broader questions of diversity and inclusion. As Mark Paterson points out, “robots do not look like people or interact with people in ways that reflect even basic aspects of society's diversity” (Paterson 2024). This is particularly significant in European healthcare contexts, where there are disproportionate numbers of female, immigrant, and minority workers. Moreover, recent research argues that encouraging cultural diversity among healthcare workers has an overall positive effect to “address health inequality, build trust, minimize workplace conflict, retain nurses, and address nursing shortages” (Atanga, Mwangi, and Ghimire 2022). Effacing race and ethnicity, and other forms of diversity, through the use of homogeneous robot avatars could compromise these opportunities for improved social, organizational, and health outcomes.
In addition, the use of “white” robots, such as Välkky, points to one aspect of what Robert Sparrow (2019, 539) calls the “race problem” for roboticists, where the typical “whiteness” of robot bodies and surfaces are: “likely to be perceived as White, exposing their designers to accusations of (arguably mostly unintentional) racism.” While accusations of racism may seem a stretch, it is easy to see how the widespread adoption of robots like Välkky could obscure “the uneven racial and gendered relations of labor, power, and social relations that underlie the contemporary conditions of capitalist production” (Atanasoski and Vora 2019, 4), and that also underlie the contemporary realities of European healthcare systems that increasingly rely on foreign-trained professionals to fill gaps in labor markets (Eurostat 2026).
Without further data from patients, it is not possible to ascertain how reciprocal experiences of recognition might play out between a robot avatar and a human patient, nor how simple modifications, such as having a display monitor on Välkky which shows a nurse's photograph and gives basic identity information (e.g., name, title, age, gender) might transform or modify experiences of recognition and transform the nature of nurse–patient communication. In addition, the Välkky robot is still in an early phase of development, and the roboticists have engaged in this phenomenological study to embed a deeper understanding of the experiential dimensions of care into the design and implementation of the robot. However, what is clear from the data is that “presence” afforded to nurses by being “in” Välkky was still some way away from enabling existing experiential care infrastructures that underpin the sort of care, intimacy, embodied contact, trust, communication, and recognition that is commonplace in hospital wards.
As we have seen, expectations for Välkky's capacity to enable re-embodiment, especially through the haptic feedback enabled by Touchlab's novel e-skin technology, which was not operational for most of the duration of fieldwork, were radically reconfigured through the “robot drama” when Välkky got into “the wild” (Jung and Hinds 2018). The limitations in the broadband supporting the Välkky trial, along with the trial's relatively short timespan, mean that we don’t know whether and how nurse-operators’ experiences of presence or attitudes toward the possibility of care would shift in time. It was clear from the study that roboticists and engineers need to attend not only to the avatar design, but also to advance the telepresence technology for it to facilitate a deeper and more immediate sense of presence, re-embodiment, and bodily resonance between the robot avatar and patients. Perhaps, if the technology develops and improves, experiences like caring touch, trust, vulnerability, emotional expression, compassion, and recognition could be performed satisfactorily, for both patients and nurses.
While perhaps falling short of imaginaries about what robots should be able to do in the present day, care robot innovations such as Välkky still offer some innovative insights about how to “re-embody” clinical work, offering possibilities for what scholars have called “posthuman care” (DeFalco 2020). The idea of posthuman care disrupts the general cultural tendency to equate “good care” with “human care” (DeFalco 2020, 33), where a dominant narrative of the 20th century positioned care as “other to technology” (Mol, Poser, and Pols 2010). Of course, care and technology are inextricably intertwined, and innovations such as Välkky do not offer a radical break from “care as we know it,” but instead further extend our understanding of human and clinical care opportunities.
Välkky serves as a useful experiment for posthuman care, which, as DeFalco (2020, 49) argues, “is not about replacing human care, it is about augmenting and hybridizing it. Or, more precisely, it is about exposing the hybridity, the cross-species organic/inorganic networks already at play and ripe for exposure, expansion and augmentation.” Experimenting with robots like Välkky in clinical spaces might not “replace existing relations of care” but instead “set in motion feedback loops” that entangle “acts of care in processes of experimentation and innovation” (Bender 2025, 11). Through these sites of experience and experiment—and emerging from the frictions and inversions within robot dramas—there is the possibility for new experiential care infrastructures to emerge. In fact, technological mediation in patient care has already been shown to have benefits in some contexts, where those receiving care report experiences such as increased patient autonomy (Pols 2012); less experience of objectification from healthcare providers (Grīnfelde 2023); and less shame and self-consciousness when asking for and receiving care (Pugh 2018; Palmer and Schwan 2021).
Bringing STS scholarship together with phenomenology gives us more resources to understand the nuance of embodied, affective, and relational experiences of clinicians and patients in care contexts, alongside the broader infrastructures and structures shaped by power and sociopolitical realities. Highlighting how experience is a constitutive element of care infrastructures gives us theoretical and practical tools to explore the acceptability and utility of emerging care technologies such as Välkky.
Footnotes
Acknowledgments
We are grateful to Zaki Hussein, Laura Garcia Caberol, and the entire team at Touchlab Limited. The project was funded by an Economic and Social Research Council Impact Accelerator Award (University of York), and author Luna Dolezal is additionally funded by the Wellcome Trust (Grant number [214963/B/18/Z]). For the purpose of Open Access, the author has applied a CC BY public copyright license to any Author Accepted Manuscript version arising from this submission. Images included in the article were taken by the research team during a site visit.
Ethical Considerations
The research received ethical approval from the Helsinki Helsingfors—Research permit application Ansökan om Aorskningstillstånd Social and Health Care, Social and Health Sector, December 14, 2022.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Wellcome Trust (Grant Number 214963/B/18/Z) and an Economic and Social Research Council Impact Accelerator Award (University of York).