
Abstract
Post-secondary educational opportunities continue to grow for individuals with intellectual and developmental disabilities (I/DD), with many providing options for independent living. This has intensified the need to teach independent living skills to this population. Complex learning needs in this population often necessitate unique teaching approaches. A single case, multiple probe across behaviors design was used to determine the effectiveness of an augmented reality (AR) video modeling system with user controls delivered on a mobile device as a learning approach. The study examined whether the AR intervention helped participants living independently learn new skills and inquired about the social acceptability of the system. Three individuals, ages 18 – 21, participated in the study. Results indicate that the AR video models were an effective and socially acceptable means of skill acquisition while also increasing independence and autonomy when completing new tasks.
Keywords
A significant contributor to quality of life is the opportunity to live as independently as possible. Independent living can present a variety of challenges for anyone, but for those with deficits in adaptive skills and cognitive functioning, these issues can be significant. A substantial barrier to living independently for individuals with intellectual and developmental disabilities (I/DD) is their need for assistance to accomplish many of the tasks necessary to keep a home safe and functioning (Ryan et al., 2019). Access to instruction and repeated practice is paramount to the acquisition, fluency, and maintenance of the independent living skills needed to do so (Collins, 2022). Despite these challenges, many with I/DD could live independently or with some level of autonomy in their own homes given the right instruction and access to supports (Bridges et al., 2020).
The National Center for Education Statistics (2024) reports that 62% of students graduating high school in the United States immediately enter 2- or 4-year institutions. For many, this is the first time they will live independently. Historically, students with I/DD have not had the same opportunity to enter the traditional college setting or live on their own. Admission into institutions of higher education typically requires a high school diploma or equivalent, specific scores on exams, and other readiness factors used as entrance criteria. That has slowly been changing with the boom of inclusive post-secondary education programs (IPSE) aimed at providing post-secondary college opportunities for individuals with I/DD. ThinkCollege (2026), a project dedicated to inclusive educational opportunities for students with I/DD, reports that there are 359 IPSE programs at two- and four-year colleges and universities across the United States. These programs vary in their offerings, but most focus on transitional programming, teaching activities of daily living (ADLs), social skills, and access to the college experience for individuals with I/DD. As a result of these expanding options, students with I/DD can gain greater independence in activities of daily living, vocation, self-advocacy, and social skills accessing inclusive post-secondary opportunities (Scheef et al., 2020).
Research has shown that individuals with I/DD participating in post-secondary education settings with access to on-campus housing gain greater levels of autonomy because of living independently or with support while attending these programs (Prohn et al., 2018; Ross et al., 2013; Ryan et al., 2019). Two prominent organizations advocating for the rights of individuals with I/DD, TASH (2021) and the American Association on Intellectual and Developmental Disability (2016), both hold the position that all people, regardless of disability and support needs, should have the opportunity to access the individual liberties associated with independent living and access to community. As a result of these outcomes and advocacy aimed to increase independent living options, many college and university programs are working to expand these opportunities. According to Think College (2026), nearly 39% (n = 140) of IPSE programs have housing options available to participating students, reflecting a steady increase that coincides with the growth of IPSE programs for young adults with I/DD.
Augmented Reality and Video Modeling
Augmented reality (AR) is an effective teaching tool for individuals with I/DD for a range of academic and nonacademic behaviors. The foundations of AR are rooted in video modeling (VM), a teaching tool that involves participants viewing instructional videos showing performance of a targeted skill, with the subsequent direction to repeat that target behavior on their own (Alberto et al., 2005). AR shares the theoretical foundations of video modeling, which are firmly situated in the social and observational theories of Bandura (1986; 1977).
Benefits of AR technology include the ability to serve as a tool for delivering instruction and intervention while allowing for control in the order and rate of content delivery to learners (Kellems et al., 2021). Marker-based AR applications allow for the creation of a digitally enhanced learning experience by matching a visual marker to trigger user-created content that can include pictures, video, and/or audio (Cihak et al., 2016). This can be accomplished utilizing tablets and mobile phones. A key benefit to AR is the ability for the user to engage with digital information while still interacting and learning in their physical surroundings (Xue et al., 2025).The increased availably and usage of tablets and mobile devices along with continued advancement of AR technology has allowed researchers new avenues to support learning among people with I/DD (Bridges et al., 2020).
Augmented Reality Interventions for Individuals with I/DD
Skills taught using marker-based AR include task chaining (Cihak et al., 2016), independent living skills (Bridges et al., 2020; Wu & Tsai, 2024), social skills and problem solving (Root et al., 2021), and academics (Kellems et al., 2016, 2021; McMahon et al., 2016). Meta analyses conducted on the overall efficacy of AR as an intervention tool for individuals with disabilities have shown significant effect sizes and the immediacy of learning and maintenance of skills over time (Baragash, Al-Samarraie, Alzahrani, & Alfarraj, 2020, 2022; Denizli-Gulboy et al., 2023; Xue et al., 2025). Additionally, AR applications accessed via tablets and mobile phones reduce stigmas associated with receiving special services and accommodations while placing the power of learning access in the hands of the user (Bridges et al., 2020).
AR and Independent Living in Post-Secondary Settings
Several life skills can be learned on a college campus, including community navigation, personal and group safety, social and personal competencies, money management, and a wide range of recreational and leisure activities. An area of need for many young adults, including those with I/DD, is in the skills needed to successfully live on their own. Having access to a system that allows a person to practice skills repeatedly, free of support from another person, has the potential to provide a self-regulated form of learning.
Given the effectiveness of AR interventions presented in the research literature, and the opportunities IPSE programs have provided individuals with I/DD, additional examination of the benefits of this learning model in inclusive post-secondary settings is needed. Most AR interventions present the video model either in its entirety, or through video prompts as discrete skills in a larger task chain. Instructional videos are widely accessed as tools for learning, and user controls are regularly used in order to follow instructions and complete tasks (Tuncer et al., 2020). Evaluation on how user-controls (pause, rewind, and fast-forward) can be incorporated as on-demand options that allow participants the option to regulate how they interact with the instructional technology is also considered.
Evidence on the use of AR to support independent living among IPSE students is limited. The present study seeks to add to the already robust research on AR by considering its effectiveness as a teaching tool for independent living skills. This study adds to that literature base and looks to answer two questions about this learning format: (1) What are the effects of user-controlled, marker-based augmented reality video models on the acquisition and increased levels of independence of daily living skills of college students with I/DD living independently? (2) Do college students with I/DD find augmented reality to learn new daily living skills socially acceptable?
Method
Participants
Participant recruitment was completed during an independent living course with a group of 12 college age students in the IPSE program at the University. These students were all living independently with some support either in dorms on campus or in off-campus housing. Several students in the program still lived at home with family or other caregivers and were not enrolled in this course. All participants in the study had roommates and received some support from the IPSE program staff and peer mentors based on individual need.
Participation was optional and offered to all students who were currently living in an independent setting. Five male students expressed interest in the study, and a follow-up meeting was held with each to further review the program and obtain consent. Three of the five interested students had conservators, so a review of the study and permission forms for those students were provided to the conservators as well. Following this information session, two students with conservators and two students of age consent agreed and all completed consent or assent forms to participate in the study. Two participants, in a show of welcomed self-advocacy, decided not to participate. The first, despite conservator consent, asked to not begin the study. The second completed baseline sessions but, being in his final year with the IPSE program, decided the time commitment was more than he wished to undertake.
All students living independently in dorms or off-campus housing were evaluated using the Supports Intensity Scale – Adult Version (SIS—A), developed by the American Association of Intellectual and Developmental Disabilities (AAIDD) (Thompson et al., 2015). The SIS—A supports person-centered planning by examining preferences, needs, and levels of support for individuals with intellectual and/or developmental disabilities. Rankings correspond to the frequency, amount, and type of support needed for the stated activity. The results for each participant from the support needs section of the assessment are highlighted as this section of the assessment considers activities of daily living in their home environment, their community, at school and work, and in their social and safety skill domains.
Walter was 18 years old at the time of the study, in his first year with the program, and diagnosed with an autism spectrum disorder and an intellectual disability. Walter lived in a dorm with a roommate on campus. His ratings on the SIS—A indicated that he was a good candidate for living independently with support. In the home living activities subsection of the assessment, it was reported that Walter would need full physical assistance when preparing food, at least once a month for less than 30 minutes. His overall composite score placed him at the fourth percentile.
Rohan was 19 years old at the time of the study, is in his first year with the program, and is diagnosed with an autism spectrum disorder. Rohan lives in an off-campus apartment with two roommates near campus. His ratings on the SIS—A indicated that he was a good candidate for living independently with support. In the home living activities subsection of the assessment, it was reported that Rohan would need monitoring when preparing food, at least once a week for less than 30 minutes. His overall composite score placed him below the first percentile.
Jason was 21 years old at the time of the study, in his second year with the program, and has an intellectual disability. Jason lives in a dorm with a roommate on campus. His ratings on the SIS—A indicated that he was a good candidate for living independently with support. In the home living activities subsection of the assessment, it was reported that Jason would need monitoring when preparing food, at least once a month for less than 30 minutes. His overall composite score placed him at first percentile.
Setting
This study took place in a small, simulated dorm space on the campus of a large university in the Southeastern United States. The dorm space was set up with tables, chairs, shelving, a refrigerator, and the materials needed to complete each task. Enrollment at the University at the time was approximately 36,000 students (undergraduate and graduate). The affiliated program had approximately 20 enrollees at the time of this study. The program was developed to provide access to the college experience for young adults with disabilities. Students enrolled in the program take college courses among their peers in areas of interest, in addition to coursework focused on daily living, social, and life skills. Students also work on vocational skill development in internship programming, partnering with community and on-campus organizations. Participants have support through peer mentors to assist them with physical access to facilities when needed, help with classes, and work on skill development.
Materials
The activities of daily living selected for the study were centered on healthy breakfast items. A list of five different breakfast items was provided to the participants, and they were asked to rank them in order of which they were most interested to learn how to make. Each participant said they knew what the items were but were not sure how to make them without some help. The top three items by collective interest were selected. These included overnight oats, fruit smoothies, and coffee. The simulated dorm space was equipped with electricity, tables, shelves, a refrigerator, and all necessary items to complete each activity as if the participants were in their own living spaces. Food items and appliances necessary to make each item were supplied by the researcher.
To facilitate consistency and prevent use of the intervention outside of study sessions, all participants used the same iPhone 13 to access the AR intervention. An adjustable, universal phone stand was provided for participants to hold the mobile device in a fixed position to make viewing the video model more manageable if needed. Halo AR, an augmented reality application for mobile devices developed by LightUp (2020), was the platform for creating the AR tags and videos. Halo AR allows users to create interactive videos that generate digital content when oriented to a physical marker using tablets or mobile devices. All video models were recorded using the iPhone 13 and the PauseCam application (PauseVideo, 2021). PauseCam allowed the researcher to eliminate inactive time in each video, ensuring that the instructional videos were shorter.
A benefit of AR is that it allows a video model to be created specifically for an exact item. This allows for materials that are being used by the participants to be those depicted in the video models. Picture markers were created by the researcher to act as triggers for the initiation of the video models when the phone cameras were aimed at them. Videos followed the steps of task analyses that were developed to outline each individual step necessary to complete each identified daily living skill. Videos depicted the tasks to be completed by the participants on the exact equipment used during the study in the simulated dorm space where the study took place. Videos were recorded from a side point-of-view to provide a full visual of the task and model and included verbal directions along with the model completing the task chain. The primary researcher provided the model. All videos had inactive time (e.g., time for water to heat up, blending of the smoothie), which varied between activities, edited out to save for time and were replaced with a prompt to pause the video and wait. Video models had the additional functions of pause, restart, and fast-forward/rewind 10-s (see Figure 1). As a result, participants had the ability to approach the use of the AR video model in the way that best met their individual learning needs. Image depicting AR trigger and video with controls.
Procedure
A multiple probe design across behaviors for three participants, a variant of the multiple baseline design first explored by Horner and Baer (1978), was used to determine the effectiveness of the AR intervention on identified daily living skills. The flexibility in this design limits frustrations often felt by participants during extended baseline procedures where target skills are not in the participants repertoire and is ethically sound by not removing an effective intervention (Gast et al., 2018; Morgan & Morgan, 2009). Experimental control is demonstrated following stability in level and trend during baseline, when an immediate change in the dependent variable is observed with the introduction of the intervention. Functionality of the intervention is exhibited when the intervention successfully produces a significant behavior change while baseline levels remain stable for the other tasks.
The three identified ADL tasks were functionally independent of one another, so as not to have a direct impact on each other once the intervention was presented but were similar in behavior class. Participants’ ability to complete the steps of each task was measured over multiple days for each ADL skill set. When an antitherapeutic trend was observed using a task analysis for each behavior, the AR intervention was introduced. The criterion for the first behavior to be considered mastered was three consecutive trials of 80% or more steps performed independently on the task analysis.
Baseline
To combat maturation of skills and to avoid frustration and fatigue, multiple probes examining ADL task completion were staggered during the baseline phase. Each participant attempted each task over several days in the simulated dorm space to establish initial baseline data. Data were collected on participants ability to complete each step in the task analysis independently following the attentional cue and verbal prompt, “Let’s make…,” followed by the task being measured during that observation. A 10-s time delay was then allowed for the participant to start the next step. No additional prompts were offered to the participant during the baseline phase. No errors in the steps were corrected, and feedback was not provided regarding the participants’ performance (Bridges et al., 2020). Each participant was assigned different behaviors to begin and progress through the intervention phase. This limited observational effects among participants and increased internal validity. Once an anti-therapeutic or stable trend was established for at least three probes, the introduction of the intervention phase for the first behavior began. Data collection and visual analysis of graphed performance were used to establish the trend and determine when to move to the AR intervention phase. The other two behaviors for all participants continued in the baseline phase, but with periodic probes to ensure the task completion trend stayed stable and did not improve when probed over time while the first behavior was receiving intervention (Gast et al., 2018).
Pre-intervention training
Participants were provided with the iPhone 13 and taught how to unlock the phone, navigate to the Halo AR App, open the app, and scan an AR Marker to initiate a video. An AR marker was created that initiated a video congratulating the participant on successfully engaging the AR video. The primary investigator assisted participants using the “I do, we do, you do” model of explicit instruction to activate the application and orient the camera to the AR trigger, activating the video. Participants were shown how to use the pause, rewind, and fast-forward functions. Independent practice time for each step was provided. Once participants learned how to use the AR app and were comfortable accessing the video models on their own, they were allowed freedom in how they interacted with the videos during intervention.
Measures
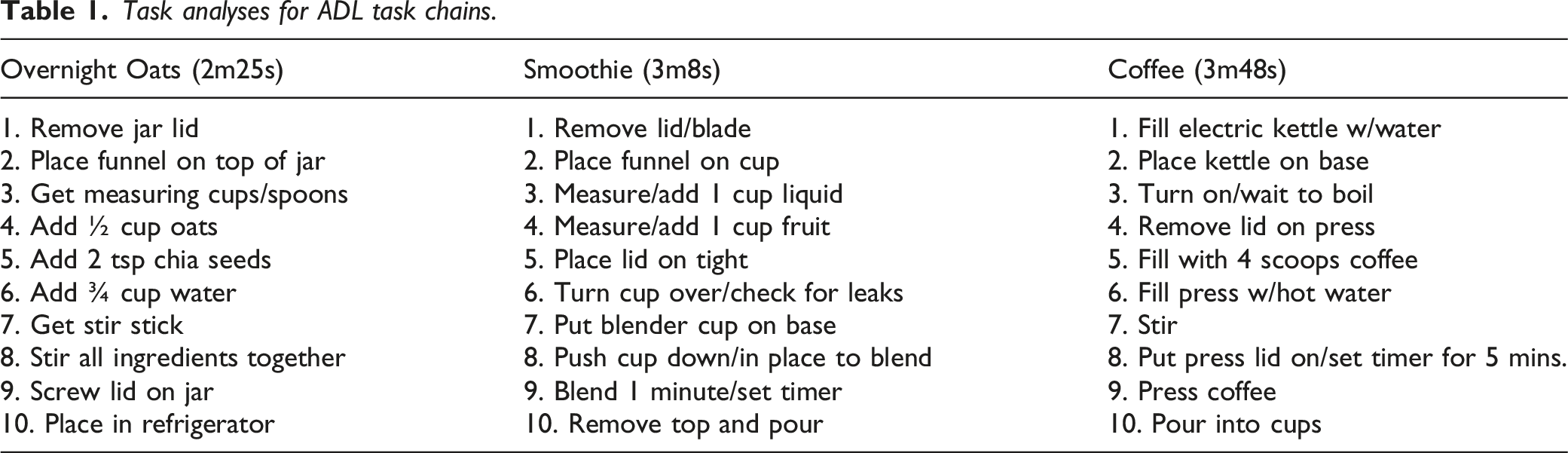
Task analyses for ADL task chains.
Intervention
Each participant, following stable baseline for the first task chain, entered into the intervention phase for the initial target behavior. Sessions took place in the simulated dorm room with the researcher. A second observer was also present in person or virtually for approximately 25% of sessions to collect data and monitor implementation fidelity. Time of day for sessions was established by coordinating schedules with the participants to accommodate for when they had work, class, or other personally scheduled events.
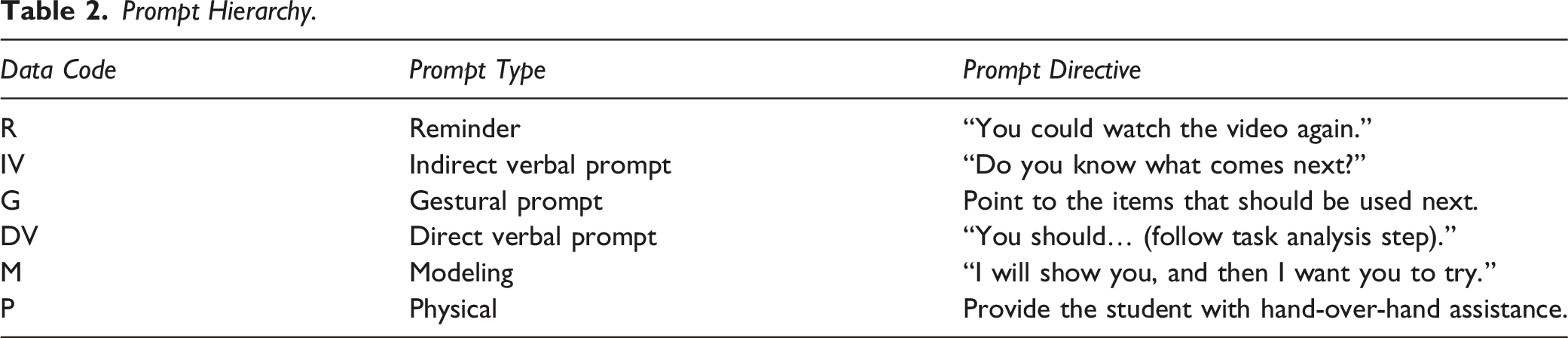
Prompt Hierarchy.
Correct responses were defined by unprompted completion of the specified step in the task. Criterion for moving on to the next task was defined as having performed 80% of the steps on the task analysis independently three sessions in a row. Each task chain was to be initiated within 30 seconds of viewing the video model, and each step was to be completed within 1 minute of the step prior. Participants were allowed to initiate the AR triggered video as often as needed to observe the model completing the task. If the student used the video again, no matter how many times, a note was recorded to examine how often participants reengaged with the marker-based video model. The percentage of task completion was calculated by taking the total number of independent steps completed and dividing that number by the total number of steps to complete the entire task chain.
Maintenance
Once criterion levels were met, the goal was for the learner to be able to complete each targeted behavior chain independently. A maintenance probe was conducted on each behavior, for each participant, at least one week from the last time they performed the measured behavior in the intervention phase. If the participants needed to use the AR video model, they had access to it via the mobile device and the Halo App. The task was still considered to be completed independently if they used the video as they were completing the task chain without prompting or support from someone else. Sessions ended when the learner accomplished all steps in the task analysis to completion. Should participants require support during a session, the researcher returned to the baseline prompting protocol. This allowed for the researcher to ask participants if they knew what to do next but not provide any feedback or error correction. If the student used the video again, no matter how many times, a note was recorded to examine how often participants reengaged with the marker-based video model.
Interobserver Agreement (IOA)
IOA data were collected using two methods: virtual and in-person. A second observer was present for at least of 25% of sessions to collect interobserver agreement (IOA) data during all phases of the study. Each observer had extensive experience working with students who have I/DD and collecting data on student behaviors and were trained for the specifics of this project. The researcher stayed to one side of the participant within view of his actions and the second observer was on the opposite side of the study setting. Both observers collected data simultaneously and separate from each other on the number of steps independently completed and those that required prompting. One observer took data in the same space as the primary researcher while assisting with IOA, while the second observer collected data on different days virtually. Virtual data were collected using an overhead camera connected to an online meeting interface. Virtual data collection was done live. No sessions were recorded. Additional probes were conducted during baseline and intervention phases when second observers were present to meet the 25% threshold for IOA, which explains extra data points on some graphs.
Data collection for each skill was done on separate data sheets. Each step in the task analysis was compared following completion of the session to observe agreement. Disagreements in the data were marked on the main data sheets, and a note was made to signify the percentages of task completion for each participant when a disagreement occurred. The primary researcher used the data point that they recorded when a disagreement occurred, regardless of whether it was a higher or lower percentage on the task analysis. Disagreements were minimal, only being differences in single steps for a task when they occurred, and all came when using the virtual data collection method. There was not a pattern that showed a certain task or participant where disagreements occurred more often. The only observable pattern was in misinterpretations of a prompt given when it was inaudible to the second observer collecting the IOA data. The percentage of IOA was calculated for each participant by adding the number of agreements and dividing by the total number of agreements and disagreements, then multiplying that number by 100. The overall IOA was 87%.
Treatment Integrity
Treatment integrity data were collected using an implementation fidelity checklist which outlined the steps for each phase of the study. Each phase and the corresponding tasks were implemented with the exact same procedures to ensure the interventions were not influenced by external factors that could be controlled. The researcher implemented all phases of the study. Research assistants collected treatment integrity data for approximately 25% of intervention sessions. The research assistants had a printed copy of the fidelity checklist, and during each session that they were present, they collected treatment integrity data. The second observer marked on the checklist each time a procedure was observed or if the primary researcher missed a step. Treatment integrity was determined by dividing the number of observed researcher behaviors by the number of anticipated instructor behaviors and multiplying by 100 (Billingsley et al., 1980). The overall treatment integrity mean was 100%.
Results
Participants exhibited different levels of performance on the various skills during baseline. Each had some knowledge of at least one of the tasks and how to complete it, but none could complete any of the three task chains from start to finish successfully or independently. Once an antitherapeutic trend was established in baseline for the first skill measured, participants entered the first intervention phase. In intervention, the criterion for moving to the next skill was 80% of steps in the task analysis completed independently over three sessions. The mean for all baseline behaviors across participants was 17%. The means for all behaviors separately across participants in baseline were 3% for making coffee, 26% for making a smoothie, and 21% for making overnight oats. Immediate improvements following the introduction of the intervention suggest that having access to the AR video models with the option of user controls served as effective learning tool for task initiation, learning, and skill maintenance.
Visual analysis of all data indicated that the AR video models were an effective method for teaching each skill. The mean for all intervention phases for each behavior across participants was 94%. The means for all behaviors separately across participants during intervention were 90% for making coffee, 94% for making a smoothie, and 98% for making overnight oats. Percentage of non-overlapping data (Scruggs et al., 1987; Scruggs & Mastropieri, 2001) was calculated between baseline and intervention for each task for all participants as well as across all tasks and all participants. PND was 100% for all behaviors across participants. A PND of 90% or greater is reflective of a highly effective intervention. Additionally, Tau-U was measured for all participants for each behavior tier and across all behaviors using an online Tau-U calculator (Vannest et al., 2016). Tau-U a nonparametric effect size for single-case research designs, measures non-overlap between phases and can be adjusted to control for baseline trend as needed (Parker et al., 2011). Effect sizes are reported as small (0–.31), medium (.32–.84), and large (.85–1.0).
Walter
Walter’s mean performance on each skill was as follows: smoothie (baseline 3%, intervention 98%), oats (baseline 4%, intervention 95%), and coffee (0%, 93%). His overall independent performance of all skills during baseline was a mean of 2% (range: 0%–4%). Following implementation of the AR video model intervention, Walter’s completion of all behaviors increased to a mean of 95% (range: 93%–98%). During the maintenance probes, Walter completed all three tasks independently at 100%. The PND for Walter for each behavior was 100%. Tau-U was calculated for each behavior. Results indicate large effects for making smoothies (Tau-U = 1.0, 95% CI [0.40, 1.00], p < .001), oats (Tau-U = 1.0, 95% CI [0.43, 1.00], p < .001), and coffee (Tau-U = 1.0, 95% CI [0.35, 1.00], p < .002). Tau-U was calculated across all behaviors for Walter. Results indicated a large effect (Tau-U = 1.0, 95% CI [0.50, 1.00], p < .001). During the maintenance probes, Walter completed all three tasks independently at 100%.
Walter engaged with the intervention differently from Jason and Rohan. He watched each step and then perform the step, using the pause feature to allow him to return to where he was in each task following completion of the step. If he was unsure of a step even after viewing it, he would carefully rewind, view that step again, and then complete the step. He used this video prompting method throughout the intervention and maintenance phases. Walter’s results are displayed in Figure 2. Results for Walter.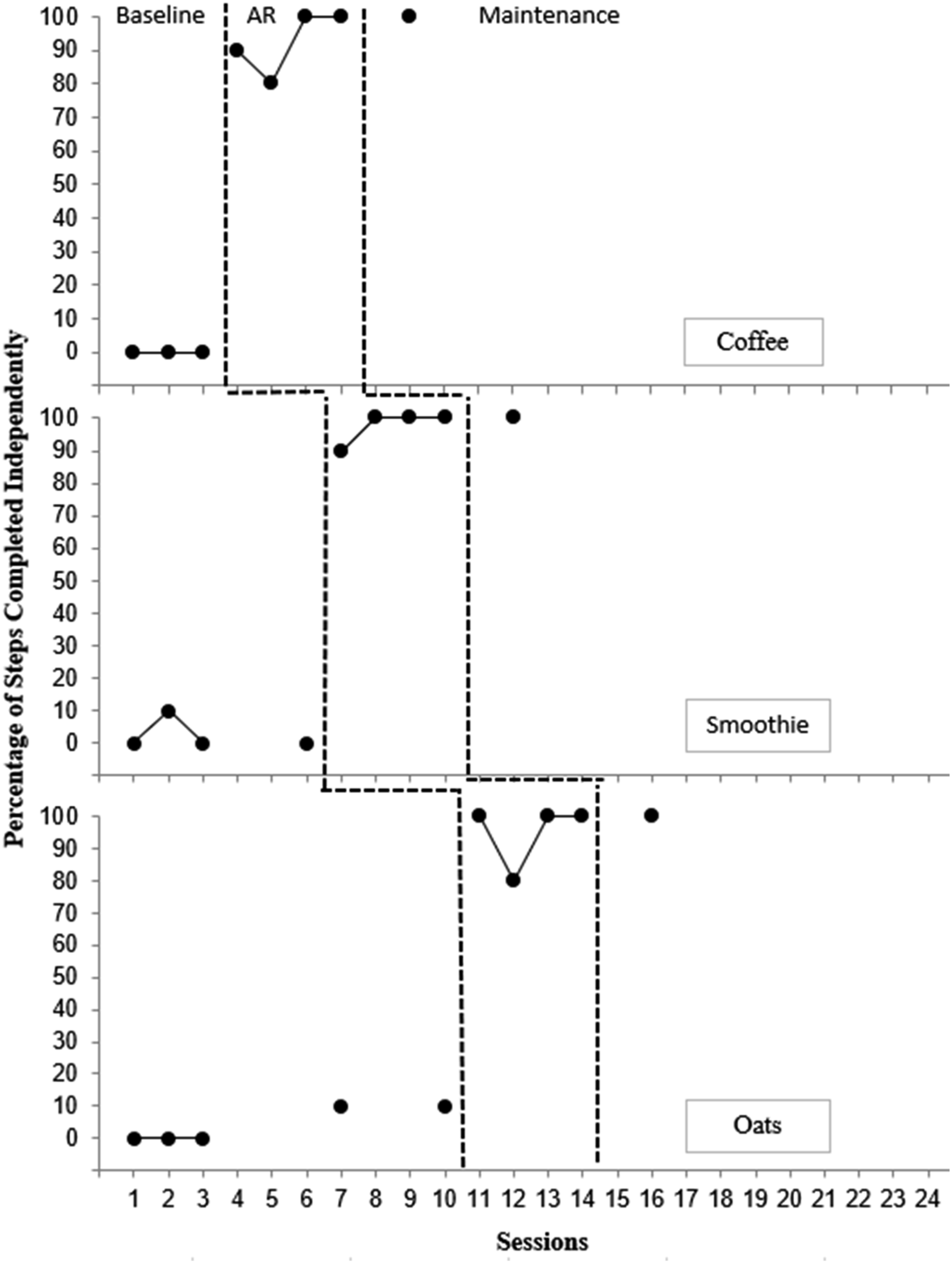
Jason
Jason’s mean performance on each skill was as follows: smoothie (baseline 38%, intervention 87%), oats (baseline 35%, intervention 98%), and coffee (0%, 93%). His overall independent performance of all skills during baseline was a mean of 24% (range: 0%–38%). Following implementation of the AR video model intervention, Jason’s completion of all behaviors increased to a mean of 93% (range: 87%–98%). The PND for Jason for each task was 100%. Tau-U was calculated for each behavior. Results indicate large effects for making smoothies (Tau-U = 1.0, 95% CI [0.35, 1.00], p < .003), oats (Tau-U = 1.0, 95% CI [0.40, 1.00], p < .001), and coffee (Tau-U = 1.0, 95% CI [0.40, 1.00], p < .001). Tau-U was calculated across all behaviors for Jason and results indicated a large effect (Tau-U = 1.0, 95% CI [0.40, 1.00], p < .001). During the maintenance probes, Jason completed all three tasks independently at 100%.
During intervention, Jason watched each AR video model in its entirety and then performed each task. During the maintenance phase, Jason used the pause and rewind options for making overnight oats. He watched the AR video model once through for the smoothie, not using any of the additional functions. He decided to not watch the AR video model when making the coffee, choosing to do this task from memory. Jason’s results are displayed in Figure 3. Results for Jason.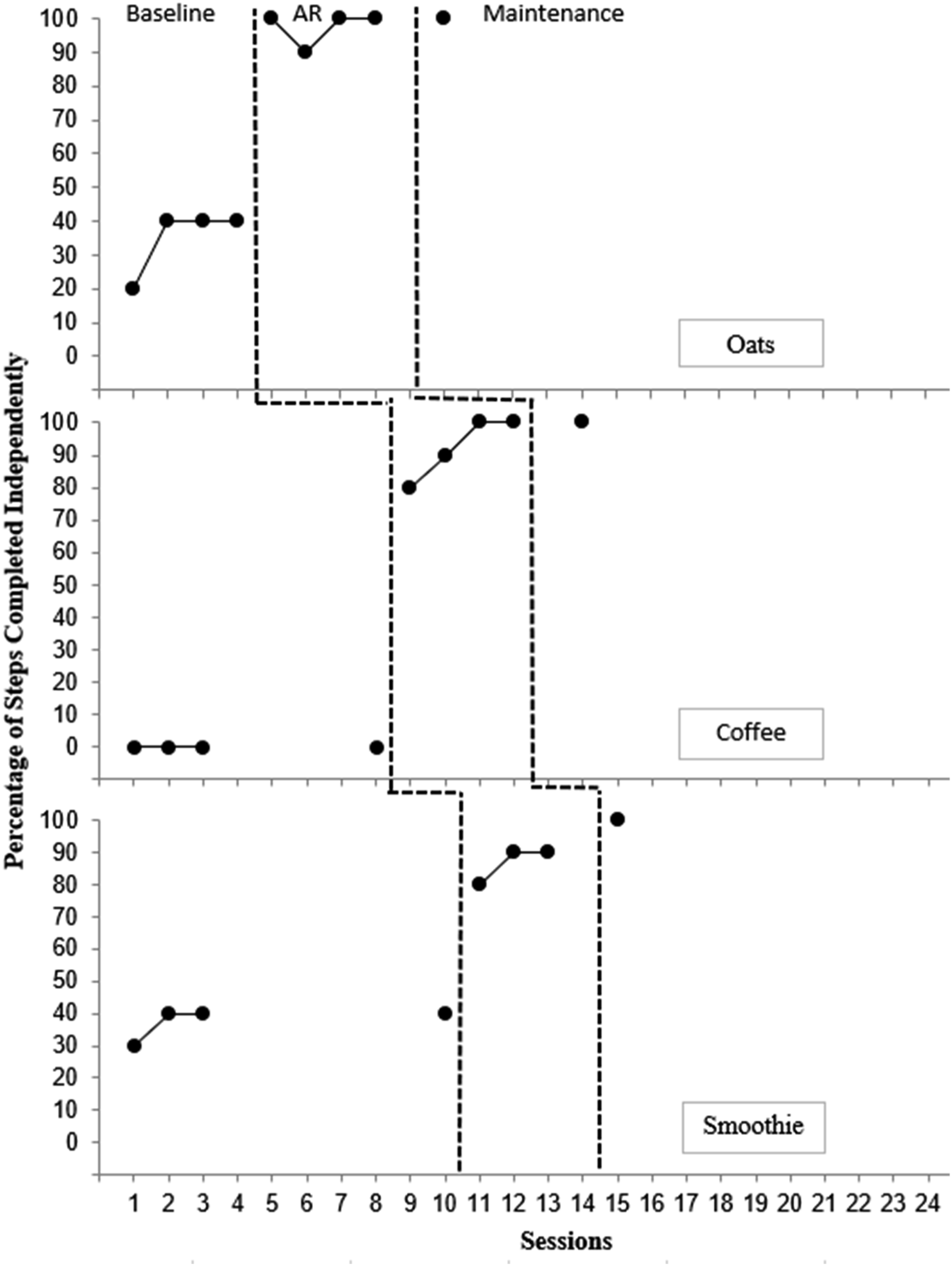
Rohan
Rohan’s mean performance on each skill was as follows: smoothie (baseline 38%, intervention 84%), oats (baseline 24%, intervention 100%), and coffee (8%, 97%). His overall independent performance of all skills during baseline was a mean of 23% (range: 8%–38%). Following implementation of the AR video model intervention, Rohan’s completion of all behaviors increased to a mean of 94% (range: 84%–100%). The PND for Rohan for each behavior was 100%. Tau-U was calculated for each behavior. Results indicate large effects for making smoothies (Tau-U = 1.0, 95% CI [0.43, 1.00], p < .001), oats (Tau-U = 1.0, 95% CI [0.43, 1.00], p < .001), and coffee (Tau-U = 1.0, 95% CI [0.38, 1.00], p < .002). Tau-U was calculated across all behaviors for Rohan. Results indicated a large effect (Tau-U = 1.0, 95% CI [0.52, 1,00], p < .001). During the maintenance probes, Rohan completed all three tasks independently at 100% (Figure 4). Results for Rohan.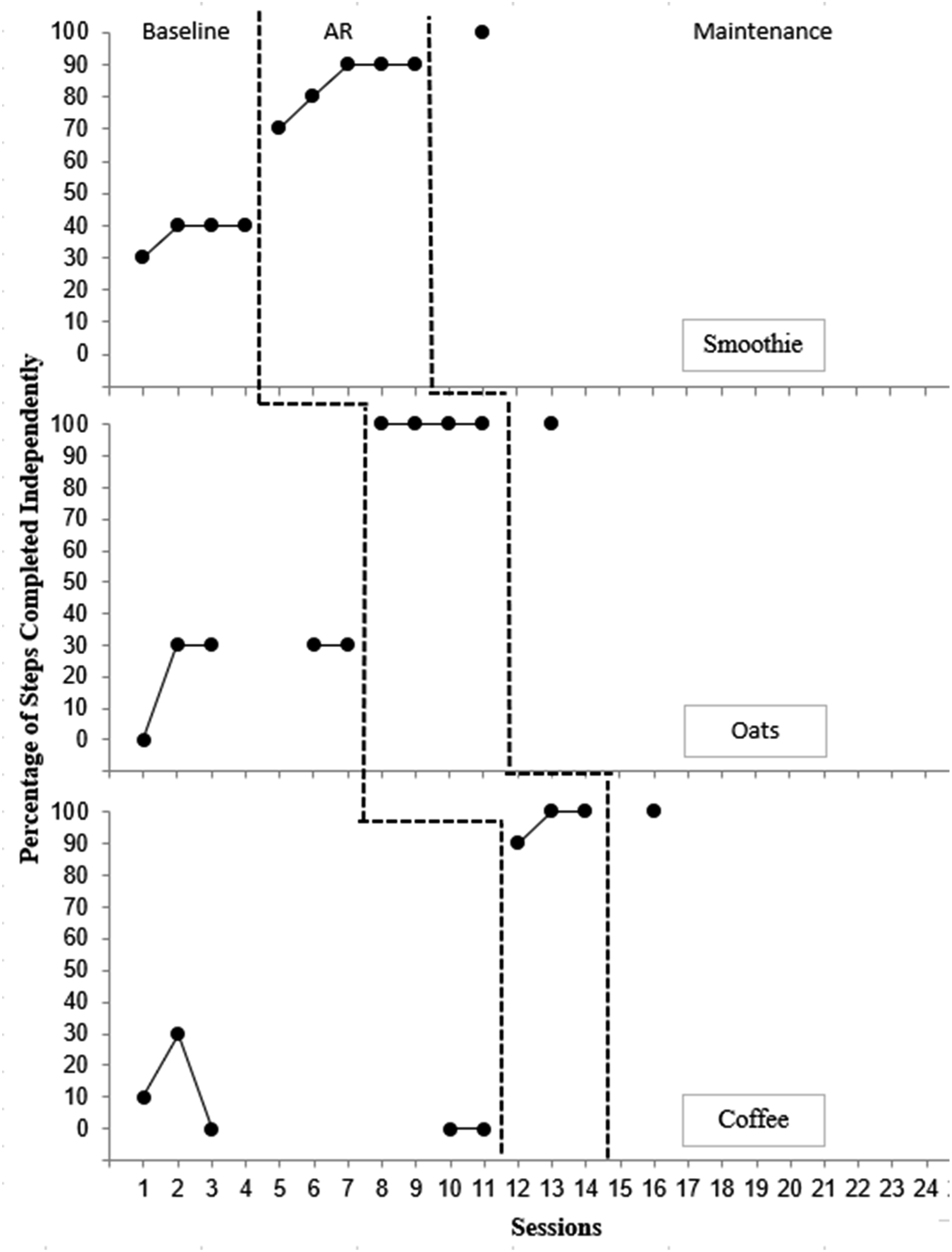
During intervention, Rohan elected to watch the entire AR video model and then complete the task chains, only re-engaging with the AR video models when he was unsure of a step. This was only done twice during the making of a smoothie to check the measurement amounts for fruit and liquid. In these instances, he would use the fast forward and rewind functions to find the step he needed to review. Rohan completed each maintenance probe by watching the AR video model one time through and then completing the skill.
Social Validity
A social validity measure was completed at the end of the maintenance phases with each participant. The first part of the survey was comprised of six Likert-style questions, with response of disagree (thumbs down), neutral (thumbs in the middle), and agree (thumbs up) The Likert-style questions revealed that all participants agreed that the intervention helpful, easy, and that AR video models would be a way they would like to learn new skills in the future. In addition to the Likert-scale responses, two open-ended questions were also asked. First, when asked what other skills participants thought they could learn using AR video models, they responded with things like cooking, work tasks, laundry, and cleaning. The second question asked why they liked or disliked the AR intervention. Replies focused on liking it because it helped them learn skills on their own and that it reminded them of using online video platforms they were used to using.
Discussion
This study looked at participants living independently as a part of IPSE programs and the functionality of an AR intervention as a learning tool with increased useability features for them. The findings suggest that AR video models can successfully support instruction on independent living skills. The intervention provides transition-aged youth with I/DD a potential means of skill acquisition without continuous support from others within this control context that is socially acceptable, especially those participating in IPSE programs.
This study extends the research base on the efficacy of augmented reality interventions using AR as a learning tool when teaching activities of daily living skills to individuals with I/DD (Bridges et al., 2020; Cihak et al., 2016; Kang & Chang, 2020; McMahon et al., 2013; Wu & Tsai, 2024). A contributing factor for conducting this study with college-aged participants was the fact that most students, with or without disabilities, find themselves struggling to complete a myriad of tasks associated with living away from home for the first time. AR capable video models could provide a conventional and modern means of instruction on a range of skills to assist in this transitional period for all individuals seeking to live more independently.
In addition to the immediacy of effect on participant learning, a major contribution of this study was in the inclusion of user-controlled features within the AR video models and how participants interacted with these features. All participants gained new skills using the AR intervention but did so in distinct ways that met their individual needs. This is important because it suggests that marker-based AR could support different learning pathways that allow individuals the opportunity to engage with the AR instruction in ways that align with their specific cognitive and self-regulatory needs. The inclusion of choice in approach shows that users can learn new skills with self in mind. The individually found function of the AR intervention took precedence over the form as evidenced by participant success in skill attainment.
Participant approach to the AR intervention is important to consider as each adopted a unique way of interacting with the user control options. Walter consistently used the controls to allow for step-by-step directions on each discrete skill in the task chain, mirroring video prompting. While this took more time to reach task completion, he was able to process the information and improve accuracy and skill attainment. Jason approached the video models as a whole chain before attempting the task until he reached the maintenance phase, where he faded the support and tried each skill independent of the intervention. Rohan also took the approach of watching the video models as a whole chain but occasionally used the rewind option to recheck his work on steps that required measurement, ensuring that he had accurately done those discrete skills in the task chain.
These individual approaches show that the AR intervention can serve as a flexible access point for self-regulated learning. This could allow users to consider their own needs in skill development as opposed to limiting the learning process to a single, prescribed instructional process. This personal approach to learning could be important when considered in the post-secondary and independent living setting where autonomy, choice, and decision-making skills are critical.
A common theme among participants was a collective confusion about why they would be asked to do a task we knew they were unable to complete. A best effort was made to explain the process of the research design to each participant, but this acknowledgment from each participant highlights a drawback to designs with extended baseline phases. Immediacy of effect and participant excitement about their ability to learn in a new way quickly replaced frustration. This suggests that the opportunity to access and use the AR video models could function as a motivating and effective learning scaffold for task initiation and skill completion.
Limitations
While a functional relation was established between the independent variable and the dependent variable, there were still limitations to this study. As a single-case design, this study included a small number of participants (n = 3). While the findings add to the research, larger scale replications of this and other AR applications would better represent the impact the intervention could have.
Even with maintenance data showing participant ability to sustain performance of the skills and independent access of the AR intervention, the lack of a generalization phase is a major limitation. Conducting the study for a longer period of time would have allowed for extended intervention periods, additional maintenance probes, and the opportunity to see if the skills would generalize. Without a generalization phase, and because the study was conducted in a controlled space, it is hard to say if students can carry these skills over to their actual residential spaces or with different materials. Extending the study for a longer period of time would have allowed for additional intervention periods, additional maintenance probes, and examination of generalization. These factors constitute an additional limitation to be considered going forward.
Participant frustration during baseline can be looked at as a limitation, albeit a small one. While the study used a multiple probe design, which helps limit frustration, there is no way to completely eliminate those feelings for participants. When asking them to attempt to complete skills multiple times while knowing that they are unable to do so will inevitably produce frustration. The affordance that a multiple probe design provides by removing continuous baseline probes, allowing for periodic data sessions, does help. However, it still leaves participants wondering why they are asked multiple times to complete a task they have indicated they are unable to perform.
Implications for Future Research and Practice
Due to the low number of participants, an increase in study participation would provide greater insights into the usefulness of this line of research. Studies that continue to explore a variety of skills, especially those associated with activities of daily living and independence will add to the research literature and further the established evidence base for AR interventions in special education settings. Doing so with a larger participant pool will help establish a more meaningful research base.
Future research using the AR intervention in the actual dorm rooms or homes of the participants or in a work setting or commercial space would provide a new perspective on the intervention. Additionally, scaling the intervention up to include multiple post-secondary programs and their students who live independently would be a meaningful way to examine the efficacy of the AR video models in a variety of environments and with a wider range of the special education population. This line of research could also serve as an addition when looking at a universal design for learning lens. Adding AR triggers to the living spaces of college freshmen with and without disabilities could be a way to target the skill deficits many young people face when living independently for the first time.
Comparative study and assessment of preference of the user-controlled aspects of the AR intervention would be a new direction to take the examination of AR interventions, especially with transition aged individuals with I/DD. Most AR video modeling studies have taken the traditional VM approaches of video prompting for discrete skills or whole task video models. Self-regulated learning is important for students working on greater independence skills in any environment. The angle of self-advocacy in how someone accesses the supports they use for learning or in maintaining a skill could lead to meaningful opportunities for co-design of interventions between researchers and the individuals with disabilities. Investigation into the benefits of the added functions could produce interesting findings for the research community. Additional comparison studies might include the exploration of similar interventions using different modalities of the extended reality continuum.
Conclusion
As more opportunities for post-secondary inclusivity grow, so too does the need to support individuals with disabilities access those spaces with a greater level of independence. Due to the rise in the usage of mobile devices, it is no longer socially stigmatizing to use a device to learn new skills. The prominence of video creation across our interconnected world, with its heavy dosage of do-it-yourself and learn how content, has made this method of learning accessible to all. While traditional teaching methodology remains key, new and innovative tools like AR are helping people learn a myriad of skills. Technological additions to the learning landscape such as AR should energize those who work in the field of special education, as it blazes new pathways to a more inclusive world for all. The findings of this study contribute to the literature by showing how a marker-based AR intervention can allow for flexible, user-specific opportunities for self-regulated learning of independent living skills. This goes beyond just an effective intervention and considers future opportunities for individualized learning, self-reflection, and how participants might advocate for how more personalized learning experiences are created.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.