
Abstract
While advances in medical treatment and technologies have the potential to improve the delivery of health care, their use typically involves making multiple, complex decisions. Patients and their medical providers may share in the decision-making processes and balance a variety of criteria and/or attributes in the pursuit of improved health. This necessitates a stronger understanding of the role of human behavior in health care processes and presents a timely opportunity to use decision analysis tools to contribute to this important aspect of health care operations. This article reports on the application of multiattribute preference elicitation to identify postsurgical rehabilitation setting options for elective hip and knee replacement patients and their discharge planning team prior to placement in these settings. These preferences are analyzed to identify trends in emphases across patients and the discharge planning team, including a comparison with actual outcomes to determine the extent of congruence with each other, an important component of patient-centered care. Variances are identified in what patients and the discharge planning team expected and what actually happened. Reasons for these variances are discussed.
Keywords
Introduction
In 2001, the Institute of Medicine (IOM) proposed six aims for improvement to address key dimensions that the 21st-century health care system should strive to attain (Institute of Medicine [IOM], 2001), including patient-centered care that is “responsive to individual patient preferences, needs, and values” (IOM, 2001, p. 40). The challenge, however, is to determine the correspondence between a patient’s wishes and those recommended by medical providers. For example, consider that treatment options for joint pain include both surgical or nonsurgical interventions and several rehabilitation setting options for postoperative physical therapy. While patients and medical providers may have some shared role in making decisions, their interests and preferences may not always be congruent. Understanding this variation in preferences is fundamental in achieving shared decision-making goals and improving options for patient-centered care.
Assessing shared medical decision making in postsurgical discharge planning involves characteristics common to many other complex decision-making situations. Multiple and (possibly) conflicting criteria and potentially dissimilar preferences held by the various parties require consideration. Multiattribute data collection methods and models have been developed in support of these considerations and are applicable to many health evaluation studies. However, because these methods have rarely been applied in health care settings, initial research was needed to determine the feasibility of such methodologies in a well-known health care context. As such, this article reports on the use of multiattribute preference elicitation to determine how patients and medical providers perceive physical rehabilitation setting options following hip or knee replacement surgery. This research is a case study; we recruited patients and their associated discharge planning team from a single orthopedic surgical site at a large urban teaching hospital in the Western United States.
Rehabilitation Setting Decisions
Major joint replacement (i.e., arthroplasty) is a common elective orthopedic procedure that entails various options for physical rehabilitation following surgery including (a) home with outpatient follow-up for physical therapy (i.e., discharged to the patient’s home residence); (b) home-based rehabilitation (i.e., home health physical therapy); (c) inpatient rehabilitation provided either in a specialized unit of a hospital or a separate rehabilitation facility; and (d) skilled nursing facilities that offer postacute care. Relative costs and care intensity of rehabilitation care are likely lowest for patients discharged to their home residence, then home health, with skilled nursing facilities generally less intensive than inpatient rehabilitation. Choice of rehabilitation setting has been definitively linked to improved outcome for some conditions. For example, inpatient rehabilitation is the venue associated with better outcomes following acute stroke. However, the evidence for the impact of setting on recovery from hip fracture repair is mixed, and there is little or no systematic evidence for major joint arthroplasty (Bronskill, Normand, McNeil, 2002; Hartley, Barton-Hanson, Finley, & Parkinson, 2002). Assessing the factors related to care setting choice is an important preliminary step in improving this decision process and is consistent with the IOM’s aim for patient-centered care.
The Medicare Payment Advisory Commission issued a report in June 2005 emphasizing that decisions about postacute care services should be based on patient characteristics and resource needs rather than Medicare payments (Deutsch et al., 2005). However, given the lack of clear evidence regarding the appropriateness of various care settings, payment incentives often impact the postacute care setting (Gage, 1999). Recent Medicare policy imposes limited access to intensive rehabilitation care for all joint replacement patients, not just patients with Medicare, who do not meet specific clinical criteria (U.S. Government Accountability Office, 2005a, 2005b). In 2007, Medicare implemented a rule that specifies 13 qualifying medical conditions that must make up at least 60% of each participating inpatient rehabilitation facilities discharges (Medicare Payment Advisory Commission [MedPac], 2008). The requirements for joint replacement to be included within these conditions are that the patient has both joints replaced immediately before inpatient rehabilitation facility admission, have a body mass index of 50 or higher, or be at least age 85. Thus, many patients with joint replacement procedures may have relatively limited access to inpatient rehabilitation following the implementation of this requirement.
In addition to payment considerations, the decision to use a particular rehabilitation setting is heavily dependent on its availability when the patient is ready for discharge (Buntin et al., 2005). Several recent studies have focused on local market factors and availability to explain variation in postacute care setting for Medicare patients, but none measure availability of resources at the time of discharge (Kane, Lin, & Blewett, 2002; Fisher et al., 2000). Lack of availability could either delay discharge or lead to the choice of a close substitute for an unavailable setting, such as discharge to a skilled nursing facility with available beds if there are no inpatient rehabilitation beds available, or vice versa.
Clinical characteristics of the patient or surgery, including both subjective and objective clinical judgments, are crucialin determining postacute care settings (Kane, 1997; Kelly & Ackerman, 1999). Opinions of the patient, surgeon, or hospital nursing team can be instrumental in discharge placement decisions but are difficult to quantify. In contrast, clinical criteria such as vital signs, pain, cognitive function, age, weight, and the occurrence of perioperative complications and comorbidities are easier to measure and almost certainly impact the rehabilitation setting decision. Patients expected to benefit from more intensive therapy may go into inpatient rehabilitation more frequently, just as others may benefit from home health physical therapy visits or outpatient follow-up for rehabilitation.
The goal for many arthroplasty patients is to return to their active lifestyles as quickly as possible (Kramer, 1997). Patients and medical providers expect that more intensive rehabilitation will result in more rapid recovery, although the data that support this expectation are limited (Kane et al., 2000). Inpatient rehabilitation may require intensive daily therapy while skilled nursing facilities offer daily on-site physical therapy, though the requirements and intensity are less than that offered through inpatient rehabilitation. Home-based rehabilitation and home with outpatient follow-up both generally entail less intensive daily therapy.
Issues of patient autonomy associated with rehabilitation setting is an important concern due to the link between self-direction and higher satisfaction with care; this factor is important in the movement toward realizing and improving patient-centered care (Ruland & Bakken, 2002; Sim, 1998). Many patients may prefer to return home following surgery, as this option allows them greater control over their daily activities and schedule, but other circumstances may mitigate this preference. For instance, following knee arthroplasty, a patient who lives in a multistory home may wish to return home immediately, but recognizes that intensive rehabilitation to ensure they can independently climb stairs will be required. Thus, inpatient rehabilitation or short stay in a skilled nursing unit prior to returning home may be indicated for such a patient. Necessarily, autonomy and recovery speed may be inversely related, as the settings that offer more intensive rehabilitation therapy are those where autonomy may be lower.
Method
Multiattribute Preference Elicitation
In order to obtain patient and discharge planning team preferences with respect to alternative settings and rehabilitation, multiple criteria analysis was used. There have been many multiattribute studies in the medical field which vary in intensity and completeness. A review of the work can be found in a recent article by Libertore and Nydick (2008). Complete multiattribute analysis including trade-offs and nonlinear relationships can be too challenging for individual decisions or cost-effectiveness studies (Hazen, 2004). However, many linear estimation methods provide a great deal of value with less cognitive burden for subjects. Analytic hierarchy process (AHP) has also been widely applied in the medical field (Libertore & Nydick, 2008) but has been criticized as arbitrary as it may have potential rank reversal when alternatives are added or deleted (Barzilai, Cook, & Golany, 1987; Belton & Gear, 1983). We note that the ideal form of AHP overcomes this limitation.
The simple multiattribute rating technique (SMART; Edwards & Barron, 1994; Olson, 1996) is a linear form of multiattribute analysis avoiding some of the arbitrariness criticized, while using a low level of cognitive burden for subjects. SMART operates by asking subjects to retain the elements being compared, then anchoring on an extremely rated element (i.e., best or worst) and asking the subject for a ratio value of relative importance for each element in turn. SMART identifies the relative importance of criteria using weights, and measures the relative performance of each alternative on each criterion with scores (Edwards, 1977; Olson, 1996). The general model is as follows:

In Equation 1, j represents each of the n alternatives evaluated and I represents each of m criteria having its own weight, and each alternative j has a score over each of the criteria. Swing weighting was used to obtain these weights, considering the relative value of swinging from the worst to best on each pair of criteria. Scores in SMART can be used to convert either subjective or objective performances to a Zero–One scale, where zero represents the worst acceptable performance level in the mind of the decision maker, and one represents the ideal, or possibly the best performance desired. Of course, these ratings are subjective since they are a function of individual preference.
Subjects
Our study sample was drawn from patients with a planned total hip or knee replacement procedure. Respondents originated from a community setting, answered a series of questions to establish intact cognitive abilities and did not have a formal caregiver at home prior to surgery. The clinician responsible for presurgical clinical assessment identified and approached qualified patients and asked them to participate in the study. Patients who agreed to participate met with a nurse data collector following their surgical intake appointment. The interview at surgical intake was the only direct contact with patients and generally lasted less than 20 min (range: 11–30 min). To establish the cognitive abilities of the potential study participants, four questions were initially posed: (a) How old are you? (b) When is your birthday? (c) What is your home phone number? and (d) What day is today? Patients who answered one question incorrectly were asked a fifth question: (e) Who is the President of the United States? Patients needed to answer at least four questions correctly to participate in the study.
The study sample was drawn from a single site and single surgical practice. The practice is located in a large, metropolitan area in the Western United States and is part of an academic health center. Institutional Review Board approval was obtained for the study protocol prior to data collection. The first patient was consented on February 15, 2006, and the last patient enrolled in the study consented to participate on July 26, 2006.
Data Collection
Patient p references for postsurgery placement were obtained using direct rankings of alternative care options, then SMART was applied to obtain continuous estimates of preference over those options. Discharge planning team preferences for postsurgery placement were obtained by rankings only. Assessments were made after clearly defining the alternatives: (a) home (i.e., patients return to their home and receive no other formal care except for follow-up from their physicians or other providers such as physical therapy that are scheduled by the patients), (b) home health (i.e., patients return to their home after surgery but receive visits from a physical therapist and/or other health professionals to assist them with their physical rehabilitation and recovery), (c) inpatient rehabilitation (i.e., a specialized unit within a hospital or a separate residential facility where patients receive at least 3 hr of physical rehabilitation therapy each day to assist them in their recovery and a physician sees them regularly during their stay), and (d) skilled nursing facility (i.e., this is typically a unit within a nursing home that provides patients with physical rehabilitation services, meals, and lodging and patients are visited by a physician at least once during their stay). Patient questionnaires obtained basic demographic data, check data for consent, and assessment of the importance of criteria. Similar assessments were conducted for the discharge planning team.
Following surgery, a study nurse attended the discharge planning meeting and obtained data from the discharge planning team and surgeon for each case. These meetings occurred at the inpatient facility within the 48 hr after surgery, yet before discharge. The typical meeting lasted less than 10 min. A list of study patients was matched to the list of surgeries prior to the discharge planning meeting. A standard questionnaire was used to focus the discussion for study cases. Additional information was provided by the discharge planning coordinator outside of the meeting to avoid disrupting usual clinical schedules.
Patients were asked to complete three questionnaires including the SF-12v2™ (a 12-item questionnaire that assesses multiple aspects of health status), either the Knee Osteoarthritis Outcomes survey (Roos, Roos, Ekdahl, & Lohmander, 1998a; Roos, Roos, Lohmander, Ekdahl, & Beynnon, 1998b) or Hip Osteoarthritis Outcomes Survey (Klassbo, Larsson, & Mannevik, 2003), and the study team’s own questionnaire that included items regarding setting characteristics and rehabilitation settings and ratings of attributes and settings. The discharge planning team and surgeon completed a single survey that included items regarding prognosis for rehabilitation, availability of rehabilitation resources, likely insurance coverage for various setting options, and items requesting rankings or relative suitability of various setting characteristics and rehabilitation settings.
Given the largely exploratory nature of this study and an enrollment target of 40 patients, traditional regression methods and multivariate analyses were not feasible. Thus, prior to applying the multivariate attribute methods, descriptive analysis including tests of mean differences for continuous variables, tests of reliability including the κ statistic as a measure of agreement between patients and the discharge planning team, percentage agreement, and tests of association for categorical variables were used.
Results
Thirty-nine participants were recruited for the study. Of those recruited, one withdrew from the study after consent and two participants did not have their surgery within the time frame of data collection resulting in a net sample of 36 patients. In the net sample, there were 25 female and 11 male patients and their modal age was 50–65 years.
A primary aim of this study was to understand which rehabilitation settings and setting attributes are important to patients and compare their rankings to that of the discharge planning team. The setting attribute definitions were as follows. “Fast recovery” captures the relative timeline to return to normal activities formerly limited by joint pain, and generally would entail greater intensity of physical rehabilitation. “Autonomy” refers to how much freedom a patient has in their daily activities or schedule, whereas “other clinical care needs” captures health concerns or conditions beyond the joint replacement that may require additional care. “Cost” refers to the expected out-of-pocket costs to the patient that can vary by setting. Last, “availability” refers to whether the setting had capability and capacity to accept new patients at the anticipated time of surgical discharge. For this attribute, the discharge planning team would assess each patient’s suitability for discharge during standing weekly meetings, knowing that most patients would be ready for discharge within 3 days from their surgical procedure. Typically, once the best setting and discharge date were determined, the discharge planning staff would contact providers to ensure availability.
Table 1 presents ranking frequencies and averages for patients compared to the discharge planning team for the setting attributes and rehabilitation settings. The discharge planning team, always consisting of the attending orthopedic surgeon, two nurses, and a discharge planning specialist, completed a single set of rankings for each patient. The surgeon completed the questions regarding each patient’s unique clinical needs. Note that a rank of 1 indicates most preferable, while a rank of 5 (for setting attribute) or 4 (for rehabilitation setting) indicates least preferable. Patients and the discharge planning team did not generally agree on the rankings of setting attributes. In fact, while not shown, none of the κ statistics for these tables exceeded .1, indicating that agreement was essentially at random. The attribute that patients most-frequently listed as most important was achieving a fast recovery, followed by autonomy, other health care needs, cost of care, and getting placed quickly. In contrast, the discharge planning team generally ranked fast recovery and other care needs as the most important considerations, followed by availability, cost to the patient, and autonomy. The major sources of disagreement for the setting attribute were related to autonomy and other care needs. Autonomy was ranked either second or third by 26 of the patients, whereas it was ranked fifth by the discharge planning team for 25 of the 36 patient assessments. In contrast, the setting attribute “other health care needs” was frequently ranked first by the discharge planning team but was not generally ranked as highly by patients. The discharge planning team was fairly consistent in its rankings, with a clustering of rankings for all of the setting attributes and rehabilitation settings. Variation in rankings by patients across setting attributes was higher, but nonetheless reflects some general patterns of preferences.
Average Rankings for Setting Attributes and Rehabilitation Settings by Patient and Discharge Team
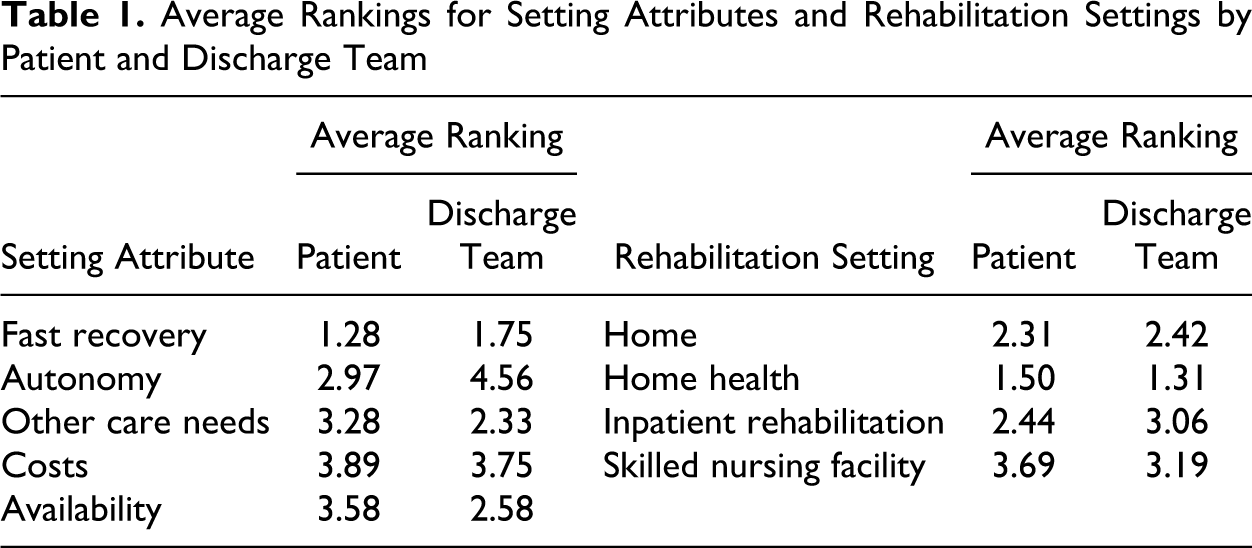
As shown in Table 1, for rankings of care setting, agreement between the patients and discharge planning teams was relatively higher. Patients were more likely to list home as their setting of choice, while the discharge planning team generally listed home health. Given that patients may have been focusing primarily on the residential versus rehabilitation aspects of the setting options, we interpret the two options as being relatively closely matched from the perspective of patients. While care was taken to ensure that the setting attributes were described in detail and distinguished for the patients, it is possible that some patients may not have perceived that health care delivered to them at their home (i.e., home health) was distinctly different from going home and having outpatient follow-up visits (i.e., home). As such, home and home health may have been viewed as very close substitutes by patients, while home versus a skilled nursing facility were seen as very distinct settings. Indeed, both the patients and the discharge planning team generally ranked the skilled nursing facility as the least preferable rehabilitation setting.
Most patients in our sample expected insurance to cover their postacute rehabilitation care. Full insurance coverage for home health services was reported for 30 cases, with 4 cases indicating they had at least partial coverage. Full insurance coverage for skilled nursing facilities and inpatient rehabilitation were reported for almost half of the patients and not known for others. The discharge planning team was efficient in exploring coverage for options that were under consideration for a given patient, but did not always explore it for settings that were unlikely for a particular patient.
Two questions regarding rehabilitation prognosis were asked of the surgeon who performed all of the surgeries. For all 36 cases, the physician reported a good prognosis for the patients. For two cases, one hip and one knee replacement, complications of the patients were listed that might influence the rehabilitation setting chosen. A patient with chronic pain was discharged to home and a patient with bleeding was assigned to inpatient rehabilitation. In both cases, the discharge setting matched the setting predicted by the discharge planning team.
Table 2 compares patient and provider choices for rehabilitation setting to the actual setting obtained from the hospital medical record after their discharge. Because there were no cases where either the patient or discharge planning team was considering a skilled nursing facility for rehabilitation and no cases where it was chosen, this option was omitted. Table 2 is interpreted as follows. The “Prediction from” columns provide the number of times that a particular rehabilitation setting was selected by the patients or discharge planning team. The “Actual from Medical Record” column represents the number of patients who were placed in the rehabilitation settings. Last, the “% Match” columns represent the percentage of patient or discharge planning team predictions that were correct, based on the actual result contained in the patient’s medical record. It is interesting to note that if “home” and “home health” were viewed the same by patients then the patient and the discharge planning team have virtually identical preferences. If so, this offers some preliminary evidence to indicate that the discharge planning team could be used as a proxy for the patient’s preferences.
Discharge Setting Prediction Versus Actual Setting
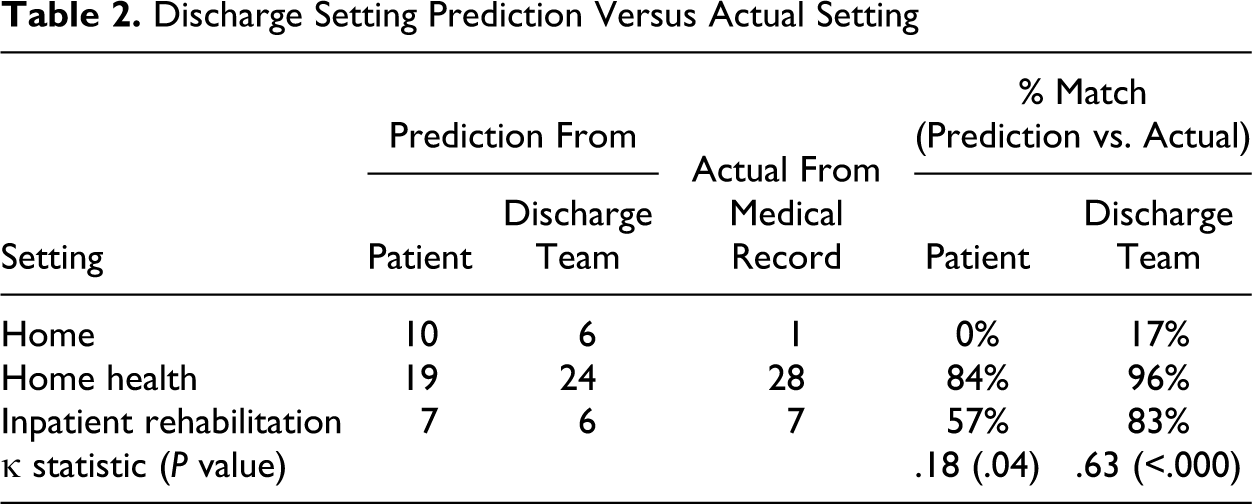
Agreement between the discharge planning team’s setting choice and the medical record was substantially better than that of the patient. In fact, the κ statistic of .63 for the discharge planning team reflects a relatively high level of interrater agreement and was statistically significant even with this small sample. Given that the discharge planning team is working to determine the best setting for patients after their release from inpatient surgical care, agreement for most cases would be expected. Lack of complete agreement is, therefore, somewhat surprising. The overall match rate for the discharge planning team predicting the discharge setting was 81% (i.e., 29 matches of the 36). Twenty patients (56%) correctly predicted their discharge location. Though the value for the κ statistic for patients was not above .50, the prediction rate was better than we expected with a p value of .04 for patient agreement with the medical record. The discharge planning team appeared to have a clear notion of eventual discharge location and provided generally accurate predictions of discharge setting.
Following the direct rankings analysis, we applied the SMART method to obtain a more complete measure of patient and discharge planning team intensity of preference, both for setting attributes and for rehabilitation setting. The research nurse presented a description of the settings and attributes to the patients and asked them to place cards with the setting or attribute names in order. Once ordered, the nurse asked the patient to describe “how much more important” the highest-ranked setting or attribute was compared to each of the others. She recorded their responses on a questionnaire. This provided the input data for the SMART method which yielded relative scores over the Zero–One scale for preference (scores adding to 1.0). Relative rankings were identical to those obtained from the direct rankings, but the SMART scores provide more information with respect to the degree of preference. This is because cardinal data (as obtained from SMART) has more information content than ordinal data (as obtained from simple rankings).
Figure 1 provides scatter diagrams of the average SMART score between patients and the discharge planning team. Each data point represents the average SMART score for the patients and the discharge planning team for a given attribute. For example, in Panel A, the data point corresponding to fast recovery has average SMART scores of .665 for patients and .299 for the discharge planning team. Ideally, if there is complete congruence between the two groups, the average SMART score should fall very close to a straight line in either panel. A 45-degree line is provided in both panels to indicate at-a-glance those attributes which are more strongly preferred by the patients (i.e., right side of the 45-degree line) and the discharge planning team (i.e., left side of the 45-degree line).
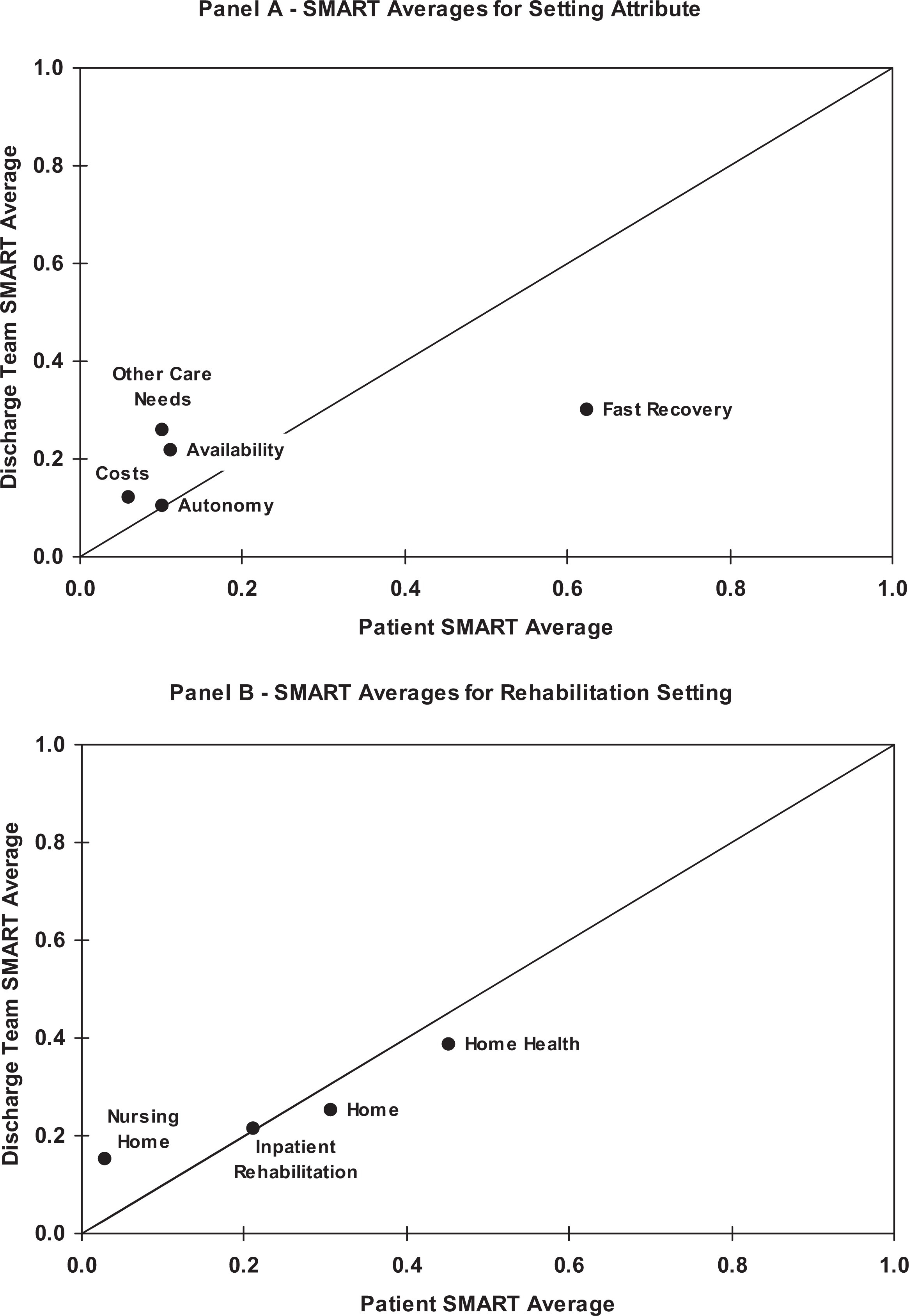
Scatter diagrams comparing simple multiattribute rating technique (SMART) averages by patient and discharge team.
When setting attributes are considered as in Panel A, patients overwhelmingly preferred fast recovery to all other setting attributes. For patients, the other setting attributes had average SMART scores that did not exceed .12. In contrast, the discharge planning team appeared to be relatively indifferent with respect to setting attributes as their average SMART scores had a relatively narrow range with a minimum of .105 for autonomy to a high of .299 for fast recovery. In Panel B, there is much greater consistency between the two groups for their rehabilitation setting preferences. For both groups, the provision of home health is the clear favorite location while discharge to a skilled nursing facility is least preferred.
The SMART results differed from rankings only in the matter of ties among choices. For patients, there were three cases where two options, home and home health, were ranked equally best and one case where three choices, home, home health, and inpatient rehabilitation, were ranked equally best. But when subjects expressed preferences with SMART, they gave equal importance to those items tied for first place. The potential benefit is emphasized by those few cases where there were actual ties in preference ratings.
Discussion
The relative importance of various rehabilitation setting characteristics and setting preferences is an important consideration in postdischarge placement decisions following elective total joint arthroplasty. Elective orthopedic procedures were chosen because they represent a growing demand for rehabilitation care (Gage, 1999). Patients choosing joint replacement tend to be younger and healthier than many patients with other conditions requiring physical rehabilitation care (e.g., those with hip fracture or stroke) and thus have a wider range of rehabilitation setting choices and perhaps different goals for their recovery (MedPac, 2005). Understanding these preferences from the perspective of the patient and discharge planning team was a primary goal for this study.
We found that both patients and the discharge planning team preferred home for recovery and actual placements after surgery heavily emphasized home health. Rankings showed that patients and the discharge team differed on what factors were important, with patients emphasizing fast recovery, while health professionals ranked availability of treatment and other care needs as nearly as important.
As our case study demonstrated, multiattribute preference elicitation can be successfully applied in health care settings and provide a rigorous evaluative approach. We used a simple methodological approach with a small sample size, since this research was intended to guide future studies where more thorough multivariate statistical and decision analysis methods could be applied. Preference information can provide a more complete picture of subject choice than does rankings but has the potential limitation of added complexity of information gathered. Of course, care given to the type of information elicited and careful data collection methods to minimize cognitive burden for subjects can provide the data needed for a more complete preference evaluation. Although our study site was an academically affiliated medical center with a diverse patient base, there is a variety of research that demonstrates small area variations in practice patterns, including the procedure rates for major joint replacements (Buntin et al., 2005; Kane et al., 2002). Though we believe our small-scale study provides important information regarding postacute care decisions, it is possible that care planning at our study site may differ from other practices or locations. As such, replication of our study is warranted to establish generalizability of our findings.
Because there is a clinical and health policy impetus toward shared medical decision making, our analysis provides an important first step to determine whether patients and their providers have similar preferences in elective or nonurgent care. Obviously, if the two parties are consistent in their rankings, then shared medical decision making will be easier to undertake. Greater consistency between patients and their providers could reduce the burden of data collection necessary for future studies seeking to measure how clinical outcomes may be related to discharge setting preferences.
Moving toward patient-centered care as defined by the IOM aim will require more activation of patients in care planning processes. We noted in our study that patients wanted both increased autonomy and fast recovery following their joint replacement, but would prefer to be in a home-based care setting. Current options for physical rehabilitation would seem to suggest that these preferences are often contradictory in practice, yet can offer insights for why patient and provider preferences are sometimes incongruent. Greater information sharing between patients and their providers, combined with more flexible care settings may help activate patients in care planning decisions and generate preferences that are congruent with realistic care options. While patient preferences were not explicitly incorporated into the medical decision-making process observed in our study setting, it appears that the majority of patients had their preference for home-based care met. Currently, shared decision aids and metrics are not used in orthopedic rehabilitation care planning in the United States. An important extension of this research is to create an information feedback process in which the patient has an explicit role in deciding their care setting following a medical or surgical procedure.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded in part by the School of Medicine at the University of Colorado Denver.