
Abstract
Racial microaggressions are everyday subtle or ambiguous racially related insults, slights, mistreatment, or invalidations. Racial microaggressions are a type of perceived racism that may negatively impact the health and well-being of people of color in the United States. This study examined the reliability and validity of the Racial Microaggression Scale distress subscales, which measure the perceived stressfulness of six types of microaggression experiences in a racially and ethnically diverse sample. These subscales exhibited acceptable to good internal consistency. The distress subscales also evidenced good convergent validity; the distress subscales were positively correlated with additional measures of stressfulness due to experiencing microaggressions or everyday discrimination. When controlling for the frequency of one’s exposure to microaggression incidents, some racial/ethnic group differences were found. Asian Americans reported comparatively lower distress and Latinos reporting comparatively higher distress in response to Foreigner, Low-Achieving, Invisibility, and Environmental microaggressions. African Americans reported higher distress than the other groups in response to Environmental microaggressions. Results suggest that the Racial Microaggressions Scale distress subscales may aid health professionals in assessing the distress elicited by different types of microaggressions. In turn, this may facilitate diagnosis and treatment planning in order to provide multiculturally competent care for African American, Latino, and Asian American clients.
Much research has found that perceived and implicit discrimination is related to psychological outcomes and likely contributes to health disparities among racial and ethnic minorities in the United States (Carter, 2007; Torres, Driscoll, & Burrow, 2010; Williams & Mohammed, 2009). Racial microaggressions are a form of perceived racism that have recently received considerable attention (Sue, Capodilupo, et al., 2007). Pierce, Carew, Pierce-Gonzalez, and Wills (1977) defined the term racial microaggressions as intentional or unintentional daily verbal, behavioral, and environmental actions that may indicate negative racial insults perceived by the targeted person or group. Microaggressions have been conceptualized as broadly affecting people from racial and ethnic minorities due to their inherently subordinate status in U.S. society.
Racism includes both attitudinal and behavioral components. The term racism can include the belief that one race is superior to another and discrimination, the behavioral manifestations of such racial attitudes (McNeilly et al., 1996). The idea of racial discrimination is based upon the idea of race, a socially constructed rather than a true biological construct, which nonetheless purports the idea of essentialized and innate ancestral, cultural, or phenotypical differences (Paradies, 2006). Paradies (2006), in a systemic review of the literature, found that self-reported racism tended to be conceptualized as either exposure to various types of race-related experiences (racist behaviors/actions, racist attacks, harassment, exclusion, major life events such as being fired, or daily hassles due to race) or as a form of chronic stress. Perceived racism refers to one’s exposure and emotional reactions to behavioral manifestations of racism, such as discrimination or the prejudicial attitudes of others (McNeilly et al., 1996). Self-reported or perceived racism has been labeled in many different ways, such as perceived discrimination (Pascoe & Richman, 2009), racial battle fatigue (Smith, Allen, & Danley, 2007), race-related stress (Utsey & Ponterotto, 1996), or race-based traumatic stress (Carter, 2007).
Sue, Capodilupo, et al. (2007) described racial microaggressions as being more subtle or ambiguous than other forms of perceived discrimination, such as hostile racism. They used the term microaggressions to describe the everyday manifestation of racism on an interpersonal level, as compared to systemic racial oppression manifested through the existence of discriminatory laws and policies. They also described microaggression experiences as situations where the intent of the perpetrator may be hard to discern. These experiences have also been termed everyday discrimination by some researchers (i.e., Stucky et al., 2011), which refers to chronic, everyday, and routine minor experiences with discrimination. Although there is considerable overlap between everyday discrimination and microaggressions, Sue and colleagues use the term microaggressions to specifically include microassaults, which involve hostile name calling and racial slurs; microinsults, which are communications that are perceived as rude, offensive, or insulting; and microinvalidations, which include communications that marginalize, exclude, or nullify the thoughts, ideas, values, experiences, or perspectives of people of color. Thus, microaggressions do not include incidents such as racial violence or racial discrimination in the workplace or the housing market. Rather, microaggressions are interpersonal or environmental situations where the prejudicial beliefs of the perpetrator are manifested consciously or unconsciously in their communication styles or behaviors toward a person of color.
This view of microaggressions as being subtle and hard to uncover fits well with social psychological research investigating the nature of contemporary forms of racism. Overt racism, which involves explicitly endorsing an ideology of White superiority, is increasingly less common. However, some White individuals who explicitly endorse antiracist, egalitarian attitudes may also hold implicit racial attitudes which unconsciously cause one to behave in a racially biased manner (Dovidio, 2001; Quillian, 2008). Individuals are more likely to allow prejudicial racial attitudes to affect their behaviors in ambiguous situations where multiple explanations are possible (Dovidio, 2001). This allows the perpetrator to disavow racial attitudes because if someone questions their behavior, they can provide other plausible explanations (i.e., I didn’t hire him because he was a poor candidate, not because he was Latino; I asked for her ID because she was acting suspiciously, not because she was Black). In contrast, an individual with negative racial attitudes is unlikely to behave in a racially biased manner when the only explanation for differential treatment could be race, such as in the situation of whether to hire a highly qualified racial minority candidate over a less qualified White candidate (Dovidio, 2001). Therefore, subtle behavioral manifestations of racial prejudice may be hard to detect and address because they are more likely to occur in situations where multiple explanations are possible.
Despite the ambiguous nature of these interactions, people from racial and ethnic minority groups do appear to be able to detect these racially related incidents. Individuals have consistently reported experiencing these kinds of racially related interactions across many research studies and with individuals from diverse racial and ethnic groups, including African Americans (Constantine, 2007; Constantine & Sue, 2007; Sue, Capodilupo, & Holder, 2008; Sue, Nadal, et al., 2008; Torres et al., 2011; Solorzano, Ceja, & Yosso, 2007; Smith et al., 2007), Latinos (Yosso, Smith, Ceja, & Solorzano, 2009), Asian Americans (Ong, Burrow, Fuller-Rowell, Ja, & Sue, 2013; Sue, Bucerri, Lin, Nadal, & Torino, 2007; Wang, Leu, & Shoda, 2011), American Indians (Clark, Spanierman, Reed, Soble, & Cabana, 2011), and British Asians (Burdsey, 2011). Researchers have suggested that microaggressions, thought seemingly trivial, may provoke considerable distress and might cause even more distress than overt racism experiences (Sue, Capodilupo, et al., 2007; Wang et al., 2011). Microaggressions may be especially stressful because individuals might not know how or whether to respond to such “mild” incidents of racism. They may also be harmful because, although mild, their frequency may cause negative cumulative effects. Finally, experiencing microaggressions may be harmful because they serve as painful reminders of one’s lower status in society and contribute to a negative or hostile racial climate (Solorzano et al., 2000; Sue, Capodilupo, et al., 2007; Wang et al., 2011).
Understanding the nature of microaggressions and their effects is particularly important for health professionals because experiencing microaggressions may be a unique chronic stressor with detrimental effects on physical and mental health of people of color (Sue, Capodilupo, et al., 2007). Researchers have consistently found links between exposure to racism and negative impacts on psychological and physical health (for more comprehensive overviews, please see Carter, 2007; Paradies, 2006; and Pascoe & Richman, 2009), so it is likely that racism contributes to existing health disparities for people of color in the United States (Carter, 2007; Torres et al., 2010). Thus, it is important for health professionals to examine whether racial microaggressions, which are more subtle and seemingly more benign form of racism, might have similar impacts on health when compared to other forms of racism, in order to provide multiculturally competent care.
Many researchers (i.e., Carter, 2007; Clark, Anderson, Clark, & Williams, 1999; Harrell et al., 2011; Helms, Nicolas, & Green, 2010; King, 2005; Landrine, Klonoff, Corral, Fernandez, & Roesch, 2006; Meyer, 2003) have utilized a stress or cognitive appraisal framework for understanding the impact of racism on the health and well-being of people from racial and ethnic minority groups. When specifically examining the impact of racial microaggressions, individuals have reported an array of negative psychological, physical, and psychosocial outcomes in quantitative and qualitative investigations. These effects have included increased anxiety, depression, perceived stress, anger, frustration, scorn/contempt, resentment, anxiety, shame, embarrassment, self-doubt, frustration, fatigue/exhaustion, discouragement, negative affect, somatic symptoms, alcohol misuse, and feeling powerless or invisible (Blume, Lovato, Thyken, & Denny, 2012; Ong et al., 2013; Solorzano et al., 2000; Sue et al., 2008; Torres et al., 2010; Wang et al., 2011). Individuals exposed to racial microaggressions have also reported negative impacts on the quality of interpersonal relationships with therapists, work or school peers, instructors/professors, and training supervisors (Constantine, 2007; Constantine & Sue, 2007; Solorzano et al., 2000; Sue et al., 2008). While many studies have found significant long-term links between either racism or racial microaggressions and health and well-being, comparatively few have examined the immediate stressful reactions or distress which might mediate the link between racism-related experiences and longer term impacts on physical and psychological health (Carter & Forsyth, 2010; Noh, Kaspar, & Wickrama, 2007). Carter and Forsyth (2010) found that individuals who had experienced racial discrimination also experienced a range of immediate emotional reactions to those specific incidents, including feeling angry, disrespected, insulted, disappointed, frustrated, outraged, hurt, or shocked. Their study did not focus specifically on the immediate reactions to microaggressions, but more broadly to a range of discrimination experiences (i.e., dealing with hostile work environment, verbal or physical racial assaults, being profiled, or stereotyped). Similarly, Noh, Kaspar, and Wickrama (2007) found that individuals who experienced subtle, but not overt racial discrimination, were more likely to experience emotional arousal such as sadness, anger, aggression, and cognitive appraisal reactions such as experiencing exclusion, powerlessness, and shame.
Until recently, the distress elicited by microaggressions was difficult to assess because of a lack of instruments to measure experiences with microaggressions. The Racial and Ethnic Microaggressions Scale (REMS; Nadal, 2011) and the Racial Microaggressions Scale (RMAS; Torres-Harding, Andrade, & Diaz Romero, 2012) have been developed to measure the frequency of microaggression experiences in people from racial and ethnic minority backgrounds. Both groups of researchers used Sue, Capodilupo, et al.’s (2007) microaggression taxonomy as the primary theoretical foundation for the development of their respective scales. The REMS (Nadal, 2011) measures the frequency of microaggression experiences across six factors derived from principal components analysis and confirmatory factor analysis: Assumptions of Inferiority, Second Class Citizen and Assumptions of Criminality, Microinvalidations, Exoticization/Assumptions of Similarity, Environmental Microaggressions, and Workplace and School Microaggressions. Similarly, the RMAS (Torres-Harding et al., 2012) measures the frequency of perceived microaggressions across six factors derived from exploratory factor analysis and confirmatory factor analysis: Low-Achieving/Dysfunctional Culture, Foreigner/Not Belonging, Sexualization, Criminality, Invisibility, and Environmental Microaggressions. However, neither investigation reported a measure to assess the stressful reactions to these microaggression experiences.
Mercer, Zeigler-Hill, Wallace, and Hayes (2011) developed a scale to measure the distress elicited by microaggressions committed against Black Americans, the Inventory of Microaggressions against Black Individuals (IMABI). This scale was intended to closely mirror the Index of Race Related Stress (IRRS; Utsey & Ponterotto, 1996). Therefore, like the IRRS, it used a Likert-type response choice that combined both the occurrence of a given microaggression (i.e., whether it had occurred vs. not) and its perceived stressfulness if it had occurred. Unlike the REMS and the RMAS, the final scale fit best with a unidimensional model and the items included in the final scale consisted predominantly of microinvalidations, or experiences where one’s ideas, values, contributions, or viewpoints are ignored, dismissed, marginalized, or minimized. The results of this study found that invalidation experiences might be particularly distressing for African Americans, suggesting that this is an important dimension to measure. More recently, Huynh (2012) developed the Ethnic Microaggressions Scale (EMA) to measure ethnic microaggressions in Latino and Asian American youth. This scale included three subscales (Denial of Racial Reality, Emphasis on Differences, and Negative Treatment) and measured not only the frequency of these experiences but also the stated stressfulness for microaggressions believed to be especially pertinent to Asian Americans and Latinos. This study found differences in the reported level of types of microaggression experiences (frequency) when comparing the Asian American and Latino youth; however, Huynh noted no differences in the young people’s appraisal of the stressfulness of these experiences when present. This suggests that measuring distress in addition to the frequency of microaggressions is an important separate dimension that may impact psychological functioning and that distress may be similarly impactful across racial/ethnic groups. However, the Ethnic Microaggression Scale and the IMABIs were developed to measure microaggressions in either Latinos and Asian Americans (EMA), or in Black Americans (IMBI), respectively. The current investigation seeks to address this gap by testing a scale that measures distress more broadly across these three racial/ethnic groups.
In addition, many scales exist to measure perceived racism, everyday discrimination, or perceived discrimination, which are related constructs. These scales include the Perceived Ethnic Discrimination Questionnaire (Brondolo et al., 2005), the IRRS (Utsey & Ponterotto, 1996), the Everyday Discrimination Scale (EDS; Williams, Yu, Jackson, & Anderson, 1997), the Perceptions of Racism Scale (Green, 1995), the Perceived Racism Scale (McNeilly et al., 1996), the Schedule of Racist Events (Landrine & Klonoff, 1996), and the General Ethnic Discrimination Scale (GEDS; Landrine et al., 2006). These scales vary in terms of whether they combine or separate the experience of the frequency of the discrimination experiences from the emotional or stressful/cognitive appraisal of these experiences. The Schedule of Racist Events (Landrine & Klonoff, 1996), the GEDS (Landrine et al., 2006), which is a modification of the Schedule of Racist Events, and the Perceived Racism Scale (McNeilly et al., 1996) measure both the frequency of racism related events and the distress elicited by those events. However, these scales pool distress or emotional reactions across situations, so that the distress elicited by specific types of racist incidents, such as microaggressions, cannot be distinguished from more overt forms of racism. Additionally, each assesses a broad range of racism related experiences which can include microaggressions, but they do not measure the distress specifically elicited by different types of microaggressions as described by Sue, Capodilupo et al.’s (2007) theoretical model.
Huynh, Devos, and Dunbars (2012) proposed that the perceived racism frequency and perceived stressfulness/emotional reactions to racism-related events are dimensions that should be assessed separately. They noted that some people may respond to seemingly “milder” experiences of racism in the moment by denying that the event has any emotional impact whatsoever. Thus, racism experiences may not always necessarily lead to a stated emotional appraisal as the incident causing distress or an emotional impact. Many factors might mediate the individual’s perception of whether they experience the event as distressing, such as the use of coping strategies, racial/ethnic identity, individual resilience factors, differences in attribution of responsibility, or attempts to deny or minimize the impact of such events. Self-stereotyping, internalization of the view that racism is no longer a problem in today’s society, or simple fatigue/exhaustion of dealing with such events may cause some people to be motivated to discount or ignore the stressful impact of these recurrent events. However, in the case of more “mild” forms of perceived racism, such as with microaggressions, Huynh et al. (2012) suggested that there may be differences in stated stressfulness, which they describe as the self-reported stressfulness of a given experience, and derived stressfulness, which they defined as the impact of racism experiences on one’s psychological health which may occur outside of a person’s awareness. Thus, they argue that it is critical to measure both the occurrence and frequency of racism-related experiences and the self-reported perceived stressfulness of such experiences because these might have differential impacts on psychological or physical health.
The current study seeks to validate six new subscales of the Racial Microaggression Scale (RMAS: Torres-Harding et al., 2012) that assess the distress elicited by racial microaggression events. These distress subscales correspond to Huynh et al.’s (2012) concept of stated stressfulness as well as mirror the scale structure of other scales which separately measure the frequency and the appraisal of stress evoked by such experiences (i.e., the Schedule of Racist Events and the GEDS). As stated previously, measuring the distress elicited by seemingly “mild” or innocuous microaggressions experiences is important so that researchers and health professionals might ultimately determine whether microaggressions are in fact harmful. The development of these distress scales would allow health professionals to measure the perceived stressfulness of the incident and more fully understand the impact of these events on their clients.
Two studies were conducted to test the reliability and validity of the RMAS distress subscales. In the first study, the reliability of these microaggression distress subscales was assessed to determine whether these subscales were found to be internally consistent, as evidenced by a Cronbach’s α of .70 or higher (DeVellis, 2003). Second, as suggested by microaggression theory, it was expected that individuals who reported more frequent microaggression experiences would also report more distress resulting from these incidents because of a presumed cumulative effect (Sue, Capodilupo, et al., 2007). Thus, correlational analyses were conducted to examine the relationship between the RMAS frequency subscales and each corresponding distress subscale. It was also expected that these correlations might exhibit a small to medium effect size, as defined by Cohen (1992), because the general racism and health literature has found small effect sizes in the relationship between exposure to racism and health (Pascoe & Richman, 2009). Third, it was expected that the distress levels would be similar across racial/ethnic groups and that no group differences would be found in terms of how stressful or upsetting the respondents found the microaggression experiences, as suggested by Huynh (2012). Thus, analyses were conducted to examine whether any racial or ethnic group differences might occur in responses to the six distress subscales.
To establish convergent validity, a second study was conducted to examine the associations between the six RMAS distress subscales and three measures of either racial microaggressions or subtle, everyday experiences with racism: the GEDS (Landrine et al., 2006), the EMA (Huynh, 2012), and the EDS (Williams et al. 1997). Both the GEDS and the EMA include subscales that measure the stated stressfulness, distress, or stress reactivity/appraisal in response to enduring microaggression experiences in everyday life. It was expected that RMAS distress subscales would be significantly correlated with the GEDS appraised discrimination subscale and the three EMA reactivity subscales.
General Methods
Procedure
An implied consent procedure was used to preserve anonymity of the study responses. All participants were recruited from a medium-sized private Midwestern university setting. Participants were recruited through the use of an online research scheduling system, classroom announcements, by visiting student groups’ meetings, and by disseminating links to the survey to student organizations who directly served students of color. After reading an implied consent statement, participants completed an anonymous online survey. This study was reviewed and approved by the university Institutional Review Board to ensure that all ethical standards were fully met in the conduct of the study. Only individuals who identified as being a member of a racial or ethnic minority group were included in the study analysis. Individuals who identified as White or Caucasian were excluded from all study analyses.
Study 1: Reliability of the RMAS Distress Scales
Methods
First, data were collected from 374 individuals. These individuals completed only the RMAS (Torres-Harding et al., 2012). All data were collected using an online anonymous survey. The data were drawn from a larger study examining the impact of microaggressions on health and well-being.
Measures
RMAS: (Torres-Harding et al., 2012)
The RMAS measures how frequently individuals experience specific racial microaggressions incidents and the distress elicited by these incidents. For each item, respondents were asked “How often does this happen to you?” with no specific time frame given. All of the items on the subscales measuring microaggression frequency were assessed on a 4-point Likert-type ordered categorical scale, with 0 = never, 1= a little/rarely, 2 = sometimes or a moderate amount, and 3 = often/frequently.
The reliability and validity of the original six RMAS frequency subscales were examined by Torres-Harding, Andrade, and Diaz Romero (2012). Exploratory and confirmatory factor analyses were used to examine the derived factors, and these factors were compared to the theoretical categories of microaggressions proposed by Sue, Capodilupo, et al. (2007). The Foreigner subscale measured how often individuals reported being treated as a foreigner, as not American, or as if they didn’t belong in a given setting. The Low-Achieving subscale measured how frequently individuals were treated as if their racial culture was dysfunctional, low achieving, or undesirable, and how frequently others viewed academic success as due to affirmative action or as an, “exception to the rule.” The Sexualization subscale measured how frequently individuals reported that others treated them in an overly sexual manner or sexually stereotyped them because of their race. The Criminality subscale measured how frequently individuals reported others treating them as if they were aggressive or likely to engage in criminal behavior. The Invisibility subscale measured how frequently individuals reported that others overlooked, invalidated, or dismissed their views or contributions because of their racial heritage, and the extent to which they felt marginalized by others. The Environmental subscale measured how frequently individuals found themselves in settings in which they are the “only one,” and to what extent they observed the absence of people from their own racial heritage in work settings, school settings, media, or positions of authority. Reliability of the original subscales, as measured by Cronbach’s α analyses, was found to be very good: Foreigner = .70; Low-Achieving = .87; Sexualization; .83; Criminality = .85; Invisibility = .89; and Environmental = .81 (Torres-Harding et al., 2012).
For the current study, a second set of subscales was derived examining the distress elicited by each category of microaggression experience. Each item on the RMAS included an additional query assessing how stressful, bothersome, or upsetting they found the incident (i.e., “If this does happen to you, how stressful, upsetting, or bothersome is this for you?”). Individuals indicated how distressing they found a particular incident on a 1–4 Likert-type scale, where 0 = not at all, 1 = a little, 2= moderate level, and 3 = high level. If the individual reported experiencing a particular racial incident at all (i.e., at least a 1 for the frequency of the experience), they were asked to indicate their stressful reaction to the particular item. If the individual reported not experiencing a microaggression, they were coded as a “0” for the distress item.
Demographic questionnaire
In addition to the RMAS scale, demographic information was collected from the participants, including age, gender, race status, whether one identified as either heterosexual or nonheterosexual (i.e., lesbian, gay, bisexual, transsexual/transgender, queer, or questioning [LGBTQ]), immigration/generational status, and disability status.
Results
Participants
This sample of 374 individuals included 132 (35.3%) African Americans, 110 (29.4%) Latinos, 89 (23.8%) Asian American, South Asian, or Middle-Eastern individuals, and 43 (11.5%) individuals who identified as being biracial or multiracial. Within the biracial/multiracial group, the ethnicities reported were varied and included individuals who were White and African American/Black (7; 17.1%), Hispanic/Latino and White (8; 19.5%), Asian American and Latino (4; 9.8%), Black and Hispanic (4; 9.8%). Black and Asian (1; 2.4%); American Indian and White (3; 7.3%), Asian and White (2; 4.9%); Black and American Indian (1; 2.4%), three or more ethnicities (5; 12.2%); and some who identified only multiracial or biracial with no additional identifiers (8; 14.6%). Because some individuals identify being Latino/Hispanic as their ethnic group and either White or Black as their race, we only classified these individuals as biracial if they indicated two clearly separate cultural heritages (e.g., “Puerto Rican and Irish,” “Mexican and Italian”). If individuals identified with only one Latino or Hispanic heritage, they were classified as “Latino/Hispanic.” The average age of the participants was 23.76 years old (SD = 6.08; age range from 18 to 52 years old). The sample was predominantly female (297; 79.4%), with 74 (19.8%) males and 3 (.8%) people not indicating their gender. Ten (2.7%) participants identified as having a disability. Three hundred and thirty individuals (88.2%) were heterosexual, 32 (8.6%) identified as being LGBTQ, and 12 (3.2%) declined to identify their sexual orientation status. Regarding immigration/generational status, 40 (10.7%) were first-generation immigrants (born outside the United States); 133 (35.6%) were second-generation (born in United States, either parent born outside the United States); 33 (8.8%) were third-generation immigrants (any grandparent born outside the United States), 7 (1.9%) individuals identified as foreign nationals, and 161 (43.0%) indicated as the question not being applicable.
Internality Consistency of the Distress Subscales
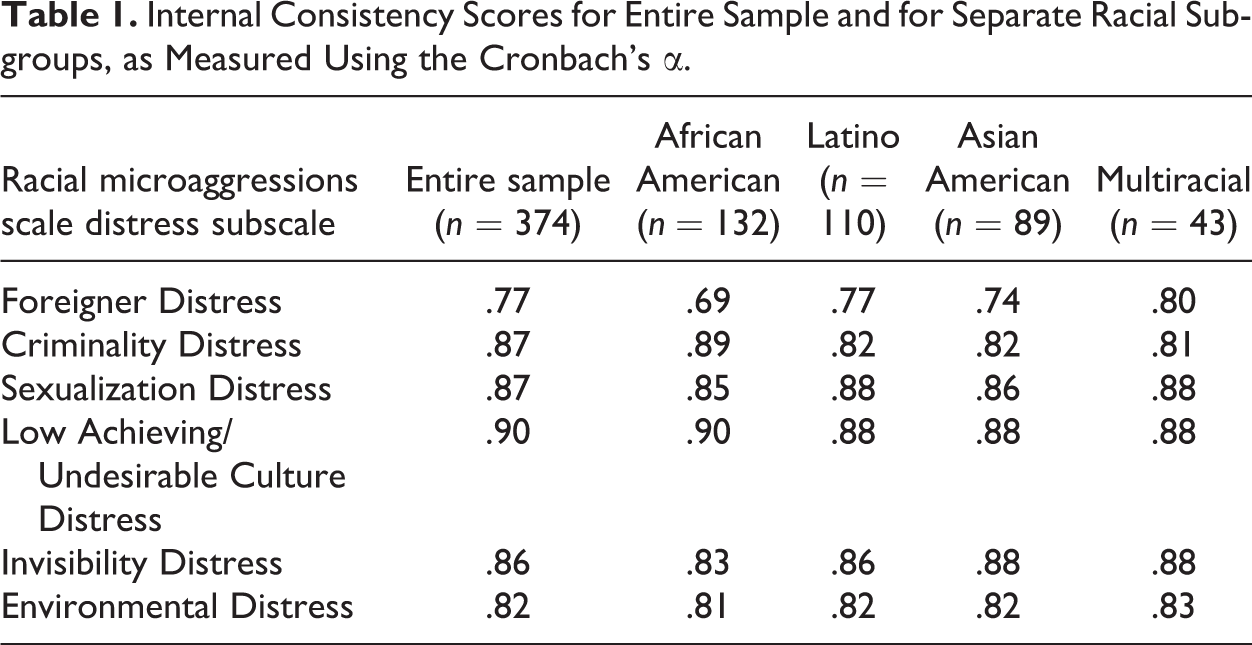
First, analyses were conducted to evaluate the reliability of the distress subscales. Cronbach’s αs were computed to examine the internal consistency of each distress subscale for the entire sample and for each of the racial/ethnic groups (see Table 1). All of the distress subscales were found to exhibit reliabilities of .70 or higher, indicating very good reliability of all of the subscales in the entire sample and in almost all of the subscales as measured in each ethnic/racial group. The exception to this was the Foreigner Distress subscale as measured in the African Americans. The Cronbach’s α for this subscale was .69, indicating moderately acceptable reliability.
Internal Consistency Scores for Entire Sample and for Separate Racial Subgroups, as Measured Using the Cronbach’s α.
Comparison With RMAS Frequency Subscales
Next, the distress subscales were compared to the previously developed frequency subscales (Torres-Harding et al., 2012) within the entire sample and across the four racial/ethnic groups. Table 2 reports results of the Pearson correlation coefficient analyses for each pair of frequency and distress subscales. As expected, the results indicate that a higher frequency of reported microaggression experiences within each category was associated with higher perceived stressfulness of those experiences. These correlations ranged from .50 (Environmental frequency and distress for Asian Americans) to .89 (Invisibility frequency and distress for Latinos).
Pearson’s r Correlation Coefficients Between the Frequency Scales and the Corresponding Distress Scales.
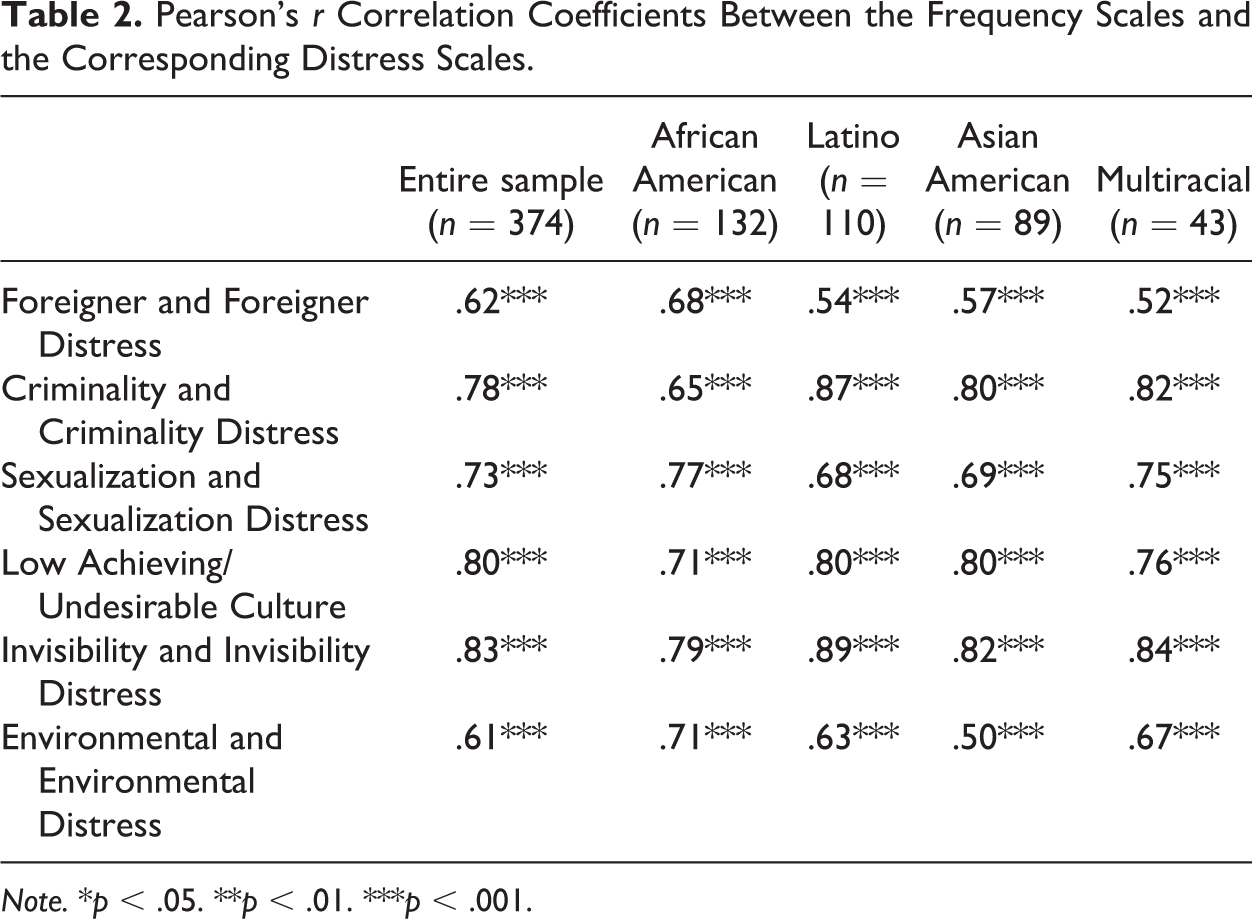
Note. *p < .05. **p < .01. ***p < .001.
Demographic Comparisons
Finally, multiple regression analyses were used to examine whether differences occurred across racial/ethnic group categories in self-reported microaggression distress. Using multiple regression analyses allowed for the inclusion of the microaggression frequency scale scores as independent variables into these analyses. Guidelines presented by Cohen, Cohen, West, and Aiken (2003) were used to dummy code race, a four-level categorical variable (African American, Latino, Asian American, and Multiracial). Three comparison groups were created: Multiracial versus all others, Latinos versus all others, and Asian Americans versus all others. The African Americans were chosen as the reference group because they represented a well-defined group with a proportionally larger sample size, as recommended by Cohen et al. (2003).
In these multiple regression analyses, after controlling for the frequency of reported microaggressions, no racial/ethnic group differences were found for the Criminality Distress or the Sexuality Distress subscales. However, racial/ethnic group differences were found for Foreigner Distress, F(4, 309) = 50.61, p = .000; Low-Achieving Distress, F(4, 309) = 17.41, p = .000; Invisibility Distress, F(4, 309) = 151.31, p = .000; and Environmental Distress, F(4, 309) = 54.61, p = .000. In order to examine the effect size of the racial/ethnic group differences, partial correlation coefficients of the dummy-coded variables were computed, as suggested by Cohen et al. (2003). These analyses indicated, after controlling for microaggression frequency, Latinos were more likely to exhibit Foreigner Distress (r = .13, p = .003), Low-Achieving Distress (r = .18, p = .001), Invisibility Distress (r = .12, p = .031), and Environmental Distress (r = .16, p = .005) when compared to the other racial/ethnic groups. Asian Americans were less likely to exhibit Foreigner Distress (r = −.14, p = .017), Low-Achieving Distress (r = −.14, p = .014), Invisibility Distress (r = −.18, p = .001), and Environmental Distress (r = .29, p < .001) than the other groups. African Americans were more likely to exhibit Environmental Distress (r = .15, p = .008). There were no differences between the multiracial participants and the other racial/ethnic group members on any of the six distress subscales.
Study 2
Procedure
In order to test the convergent validity of the four scales, data were collected from a second group of 84 research participants. Participants completed an anonymous online survey.
Measures
The RMAS was completed by all of the participants. Additionally, the following measures were administered.
GEDS
The GEDS is a scale containing 18 items (Landrine et al., 2006). For each item, individuals were asked to report how frequently they had experienced the event during the past year, during their entire lifetime, and the level of stress provoked by the experience. Examples of racist events measured in this scale included being treated unfairly because of one’s race by teachers or neighbors, being called racist names, experiencing violence or physical threats because of one’s race, or experiencing negative emotional reactions in response to racist treatment. Landrine and colleagues reported very good internal consistency for the Appraised Discrimination (α = .95), Recent Discrimination (α = .94), and Lifetime Discrimination (α = .94) subscales (Landrine et al., 2006).
EMA: ( Huynh, 2012)
The Ethnic Microaggression scale measures an individual’s experiences with subtle discrimination during the previous year. This scale was developed by Huynh (2012) and used with Latino and Asian American adolescents. This scale assesses three types of microaggression categories: Emphasis on Differences assesses whether one is treated as a foreigner; Denial of Racial Reality assesses the experience of having others invalidate the reality of bias and discrimination; and Negative Treatment assesses the degree to which an individual is ignored or treated as a second-class citizen. Each category includes a Frequency subscale, which measures how often the individual experiences a given microaggression, and a Reactivity subscale, which measures how much the event bothered them. The frequency items are measured using a 6-point scale (0 = 0 times/never, 1 = once a year (rarely), 2 = 3–4 time a year (sometimes), 3 = once a month (somewhat frequently), 4 = once a week (frequently), and 5 = almost every day (all the time)). The reactivity items are measured on a 5-point scale (1 = this event made me feel good, 2 = It did not bother me, 3 = It bothered me slightly, 4 = It upset me, 5 = This event upset me extremely). The reliability of these subscales was found by Huynh (2012) to be in the acceptable to good range: Emphasis on Differences Frequency, α = .71 and Reactivity, α = .66; Denial of Racial Reality Frequency, α = .71, and Reactivity, α = .76; and Negative Treatment Frequency, α = .71, and Reactivity, α = .72.
EDS: (Williams et al., 1997)
This scale measured unfair treatment and more chronic, routine, and minor experiences of discrimination. This scale included 9 items assessing experiences such as being treated with less courtesy than others, receiving poorer service in restaurants and stores, being treated as if one is less intelligent, or being threatened or harassed. For each item, respondents were asked to indicate “In your day-to-day life, how often do any of the following things happen to you?” with no specific time frame indicated. Respondents indicated the frequency of encountering these types of experiences using a 6-point Likert-type style, with 0 = never, and 6 = almost every day. The responses were summed in order to derive a total score. Williams, Yu, Jackson, and Anderson (1997) reported excellent reliability, α = .88.
Results
Participants
Of this sample, 32 (38.1%) were African American, 23 (27.4%) were Latino, 16 (19.0% were Asian American, and 13 (15.5%) were multiracial. Within the biracial/multiracial group, the ethnicities reported included individuals who were White and African American/Black (2; 15.4%), Hispanic/Latino and White (2; 15.4%), Asian American and Latino (1; 7.7%), Black and Hispanic (2; 15.4%); Black and Asian (1; 7.7%); three or more ethnicities (2; 15.4%); and some who identified only as multiracial or biracial with no additional identifiers (3; 23.1%). Because some individuals identify being Latino/Hispanic as their ethnic group and either White or Black as their race, we only classified these individuals as biracial if they indicated two clearly separate cultural identities. Sixteen (19.0%) participants were male, 67 (79.8%) were female, and 1 (1.2%) identified as transgender. Eight participants (9.5%) identified as having a disability. The average age in this sample was 23.50 (SD = 6.55; range = 18 to 58 years old). Eleven participants (13.1%) identified as being LGBTQ, with 73 (86.9%) identifying as heterosexual.
Convergent validity
In order to test the convergent validity of the RMAS distress subscales and the additional measure subscales, Pearson correlation coefficients were computed among all of the measure subscales scores. As hypothesized, all of the RMAS distress subscales were found to exhibit significant positive moderate-level correlations with all additional subscales that assessed stressfulness or distress. Correlations between the GED Appraised Discrimination subscale and the RMAS distress subscales were as follows: Foreigner Distress, r = .53, p < .001; Sexualization Distress, r = .53, p < .001; Criminality Distress, r = .54, p < .001; Low-Achieving Distress, r = .60, p < .001; Environmental Distress, r =.61, p < .001; Invisibility Distress, r = .77, p < .001. Correlations between the EMA Emphasis on Differences reactivity subscale the RMAS distress subscales were as follows: Sexualization Distress, r = .43, p < .001; Low-Achieving Distress, r = .43, p < .001; Criminality Distress, r = .44, p < .001; Invisibility Distress, r = .52, p < .001; Foreigner Distress, r = .57, p < .001; Environmental Distress, r = .57, p < .001. Correlations between the EMA Denial of Racial Reality reactivity and the distress subscales were as follows: Foreigner Distress, r = .23, p = .024, Sexualization Distress, r = .30, p = .007; Environmental Distress, r = .36, p = .001; Criminality Distress, r = .38, p < .001; Invisibility Distress, r = .44, p < .001; Low-Achieving Distress, r = .56, p < .001. Finally, correlations between the EMA Negative Treatment reactivity subscale and the distress subscales were as follows: Sexualization Distress, r = .32, p = .003; Criminality Distress, r = .48, p < .001; Foreigner Distress, r = .49, p < .001; Environmental Distress, r = .54, p < .001; Invisibility Distress, r = .64, p < .001; Low-Achieving Distress, r = .67, p < .001.
The RMAS distress subscales were also found to be positively associated with the additional subscales assessing the frequency of microaggressions. The distress subscales were significantly positively associated with all of the GEDS subscales, with associations ranging from .33 (Sexualization Distress with Recent Discrimination) to .75 (Invisibility Distress with Lifetime Discrimination). The RMAS distress subscales were positively associated with many of the EMA frequency subscales (range of correlations: .27–.60), with the exception of the association between Criminality distress and Emphasis on Differences frequency, and the association between Low Achieving distress and Emphasis on Differences frequency, which were not statistically significant. The RMAS distress subscales were positively associated with the EDS total score (range of correlations: .33–.62), with the exception of the association with Sexualization Distress. Similarly, the RMAS frequency subscales were also found to be positively significantly associated with most of the frequency and stressfulness subscales (range of correlations: .23–.78), with the following exceptions: Foreigner Frequency and EMA Denial of Racial Reality Frequency, Criminality Frequency with EMA Emphasis on Differences Frequency, and Sexualization Frequency with the EDS total score.
Discussion
These studies provide preliminary evidence for the reliability and validity of the RMAS distress subscales. The original RMAS subscales (Torres-Harding et al., 2012) examined the degree of frequency with which one might experience different types of microaggression experiences. Developing and validating the additional distress subscales is important because other researchers have found that the impact of stress on physical and mental health is mediated by one’s cognitive appraisal of that particular environmental stress or demand (Huynh et al., 2012).
The internal consistency of the RMAS distress scales appeared to be very good. The Foreigner Distress subscale exhibited somewhat lower reliability for African Americans, but this still fell within the moderately acceptable level of reliability (α =.69). It is unclear why this subscale was somewhat lower for this group when compared to the other racial/ethnic groups. Only five (3.8%) of the African American group reported being a first generation immigrant (i.e., born outside of the United States), so the majority of this group were U.S.-born. It is possible that they were less likely to be treated as if they were a foreigner or perhaps they felt that these questions were less relevant to them when compared to the other groups.
Regarding the convergent validity, all six subscales were found to correlate well with the Appraised Discrimination subscale from the GEDS, a general measure of how much racism-related experiences are upsetting or troublesome to an individual. Correlations ranged from .50 to .76 with the Appraised Discrimination subscale. Additionally, all six RMAS distress subscales were significantly correlated with the three reactivity subscales from the EMA, which also measures how upsetting or bothersome the respondents found specific microaggression experiences. Correlations with the Emphasis on Differences, Denial of Racial Reality, and Negative Treatment reactivity subscales ranged from .25 to .67.
Additionally, the distress subscales were all found to be significantly associated with their corresponding original RMAS subscale measuring the frequency of microaggression experiences. Correlations between the RMAS frequency subscales and their corresponding distress subscales ranged from .50 to .89. The positive correlations between frequency and distress subscales fit with microaggression theory, which contends that microaggression experiences have a cumulative effect on emotional distress (Sue, Capodilupo, et al., 2007). These results also fit well with results reported by Huynh et al. (2012) who found that frequency of racial discrimination and stated stressfulness were significantly modestly correlated (i.e., r = .40) when using the Schedule of Racist Events Scale. The finding of associations between many of the RMAS distress subscales and the Ethnic Microaggression Scale frequency subscales, the GEDS recent and lifetime discrimination frequency, and the EDS score again suggests that there is a relationship between frequency of microaggression experiences and distress elicited by these experiences.
Regarding the differences among the racial/ethnic groups, we did find some variation across the following subscales, even after controlling for microaggression frequency: Low-Achieving Distress, Foreigner Distress, Invisibility Distress, and Environmental Distress. Latinos appeared to be more likely to report distress after experiencing Foreigner microaggressions, Invisibility microaggressions, Low-Achieving microaggressions, and Environmental microaggressions. Asian Americans, in contrast, reported comparatively less distress after Foreigner microaggressions, Invisibility microaggressions, Low-achieving microaggressions, and Environmental microaggressions. Finally, African Americans reported comparatively more distress after Environmental microaggression, but the level of reported distress with the other distress subscales did not vary from the other racial/ethnic groups. The multiracial group’s distress level did not vary from the other racial/ethnic groups on any of the distress measures. It is important to note that the effect sizes for these relationships were small (i.e., between .12 and .15), and the size of these differences were smaller than the effect sizes for the microaggression frequency’s impact on distress. In the multiple regression analyses, microaggression frequency exhibited large effect sizes (β = .60–.79) when examining the relationship between each microaggression frequency subscale and its corresponding distress subscale.
However, although small, these differences were statistically significant. Thus, Latinos may have exhibited more distress than the other groups, and Asian Americans comparatively less distress. This contrasts with results reported by Huynh (2012), who found differences between Latino and Asian American adolescents in the frequency of some types of microaggressions, but no differences in the self-reported stressfulness of these microaggressions across Latinos and Asian Americans. It is possible that reminders of physical and linguistic exclusion, such as “English only” laws or anti-immigration policies aimed predominantly at Latinos, might lead to comparatively more distress when a Latino has to confront these microaggressions. Given the current media attention on immigration reform, activism around pro-immigration legislation such as the DREAM Act, and ongoing deportations of undocumented people in the United States, experiencing racial microaggressions may seem particularly threatening to members of this group. It is possible that Asian Americans reported comparatively less distress in the face of these microaggressions because Asian Americans are stereotyped as the model minority (Sue, Bucerri, et al., 2007). The sample consisted entirely of university students, so this setting may have especially primed respondents to the stereotypes of Asian Americans as being more intelligent and academically more competent, thus lessening the comparative impact of these microaggression experiences when compared to the other racial/ethnic groups.
Also, it is possible that there may have been differences in generational status between the Asian Americans and the other group. If one group was more likely to be foreign-born, then this might have affected reported distress. In the first study, 20 (23%) of the Asian Americans were first-generation immigrants (i.e., born outside the United States), when compared to only 13 (11.9%) of the Latinos, 2 (4.7%) of the multiracial individuals, and 5 (3.8%) of the African Americans. It is possible that Asian Americans experienced less Foreigner distress because they were somewhat more likely to have been foreign-born. Further, research conducted by Noh and Kaspar (2003) suggested that, for Asian Americans, contextual factors such as immigration/generational or refugee status may impact reactions to discrimination because of differences in social and cultural resources, such as family support, employment stability, income, and educational levels. Availability of these resources might impact the types of emotional reactions that individuals experience in response to discrimination experiences (Noh & Kaspar, 2003). Finally, it is important to note that, even for Asian Americans, microaggression experiences were still perceived as stressful and may be harmful to the sense of well-being, security, and feelings of belonging, although perhaps somewhat less when compared to the other racial/ethnic groups.
Regarding the clinical implications of this study, it is important for clinicians to understand the impact of microaggression experiences in order to provide multiculturally competent care. Microaggression experiences are, by their nature, ambiguous and difficult to discern (Sue, Capidilupo, et al., 2007). Thus, therapists, especially White therapists, may have a difficult time recognizing when these racism-related experiences have occurred or may not fully understand how upsetting or distressing these experiences may be for some clients of color. Assessment of microaggression experience and the resulting distress fits well with the most recent Diagnostic and Statistical Manual, Fifth edition (DSM-5; American Psychiatric Association, 2013) cultural formulation interview. In the current DSM-5 system, the focus has shifted away from cultural bound syndromes toward using a more flexible assessment approach to understand the differential impact of culturally important variables such as discrimination experiences on the development of psychopathology. The cultural formulation interview generally assesses the client’s perceptions of stressors, such as discrimination. However, this interview does not specifically assess microaggression-related distress. Using this scale to assess microaggression distress in conjunction with the DSM-5 cultural formulation interview may help clinicians to integrate racism-related stressors in their conceptualization of the client’s difficulties and help the clinician to avoid inappropriately attributing distress to intrapsychic or personality factors. This will also help the clinician to more fully understand how microaggression-related distress may elicit or maintain emotional difficulties, such as depression or anxiety, or whether it may underlie ineffective coping strategies.
Finally, understanding the distress elicited by microaggressions is important to help guide the treatment process and the development of trust within the therapeutic relationship. Some clients may be reluctant to bring up any race-related issues because of cultural mistrust, which involves avoiding discussing issues of race in therapy because of fear of being told that they are paranoid about racism, being oversensitive to racial issues, or being pathologized as overly resistant and suspicious (Whaley, 2001). Also, if microaggressions occur within the clinical therapeutic relationship, it can lead to increased mistrust, attrition, or lack of compliance, and may negatively impact the quality of care experienced by people of color within the health care system (Constantine, 2007). These incidents are harmful because they delegitimize the patients’ “racial reality” and privilege the worldview and perspective of the clinician over that of the clients (Sue, Capodilupo, et al., 2007). Asking clients about racism-related distress as part of an intake assessment allows the clinician to acknowledge that racism-related issues are legitimate concerns to be addressed in therapy (Whaley, 2001). Awareness of microaggressions and the resulting distress for their client may help the clinician avoid engaging in microaggressions in therapy.
Finally, clinicians may be able to assist clients with understanding how microaggressions may be impacting their prevailing mood or ongoing psychological difficulties. Helping clients to develop effective short-term coping strategies for the emotional arousal caused by microaggression experiences may be helpful. Clinicians might be able to help clients figure out how to function more effectively at work or at school in the face of experiencing upsetting microaggressions from peers, coworkers, professors, supervisors, and others. Clinicians might also explore with clients how experiencing specific microaggressions, such as being treated as if one is from a dysfunctional culture, might impact their sense of self, self-worth, and identity. Finally, clinicians can help to empower clients by placing these distressing experiences into a larger sociopolitical context and then facilitating the client’s own choices about how to confront these experiences. Ultimately, this may enhance the client’s self-efficacy and competence. Clinicians can help the client avoid self-blame and resist these harmful racial stereotypes, so that they may eventually develop healthy and positive racial and cultural identities.
Limitations of the study include the fact that the current sample consisted of a convenience sample of university students, so generalizability to other populations or other settings is unclear. The scale was administered in English, and the current analyses excluded individuals who spoke Spanish or other languages. Therefore, generalizability to Spanish-speaking Latinos or to Asian Americans whose predominant language is not English is unclear. Also, it is important to note that the partial correlation coefficients for the racial groups were computed using dummy coded variables, and, according to Cohen et al. (2003), the exact correlation coefficient value using a dummy coding method may underestimate the value of the proportion of each racial group to the overall sample size. However, Cohen et al. (2003) notes that this likely is not a significant issue if the proportion of the sample is similar to that of the population from which it is drawn. For the current study, the racial/ethnic composition was similar in proportion to the larger university setting’s racial/ethnic composition; thus, it is likely that the estimates are accurate. However, more research should be done to further examine racial/ethnic group differences in the reported stressfulness of these microaggression experiences. Finally, more sophisticated methods for evaluating the psychometric properties of the subscales, such as using Item Response Theory, were not conducted. Therefore, these analyses should be considered preliminary and more research needs to be done in the future to more fully test the reliability and validity of these subscales.
Summary
Analyses examining the reliability and validity of these distress subscales were conducted to determine whether these subscales might serve as useful tools for researchers and clinicians seeking to measure the perceived stressfulness of microaggression experiences for individuals from diverse racial and ethnic backgrounds. This study found preliminary evidence for the reliability and validity of the distress scales in a sample of African American, Latino, Asian American, and multiracial adults. The subscales generally appeared to be reliable and to be associated with similar measures of racism-related distress. This suggests that these distress subscales may be promising tools for exploring the potential impacts of microaggression experiences. However, additional research should be conducted to more fully assess the utility of these scales across settings.
Examining the immediate distress elicited by racial microaggression experiences may allow health researchers and health professionals to more fully understand the distress evoked by these seemingly mild but recurrent forms of racism. The current analyses suggest that individuals do report immediate distress in response to these experiences, but the significance and long-term impact of this stressful response in racially diverse individuals should be further explored in future research. Development of the distress scales might aid investigations into the stress appraisal process, the emotional reactions of people of color, and the short-term and long-term impacts on physical and psychological health due to these microaggression experiences. Finally, it is important for health professionals to become aware of the impacts of microaggressions on the health and well-being of their clients, so that they don’t inadvertently marginalize their patients but, rather, provide the highest possible quality of care.
Footnotes
Authors’ Note
The Racial Microaggressions Scale is available upon request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.