
Abstract
The success of integrated care interventions is highly dependent on the internal and collective capabilities of the organizations in which they are implemented. Yet, organizational capabilities are rarely described, understood, or measured with sufficient depth and breadth in empirical studies or in practice. Assessing these capabilities can contribute to understanding why some integrated care interventions are more effective than others. We identified, organized, and assessed survey instruments that measure the internal and collective organizational capabilities required for integrated care delivery. We conducted an expert consultation and searched Medline and Google Scholar databases for survey instruments measuring factors outlined in the Context and Capabilities for Integrating Care Framework. A total of 58 instruments were included in the review and assessed based on their psychometric properties, practical considerations, and applicability to integrated care efforts. This study provides a bank of psychometrically sound instruments for describing and comparing organizational capabilities. Greater use of these instruments across integrated care interventions and studies can enhance standardized comparative analyses and inform change management. Further research is needed to build an evidence base for these instruments and to explore the associations between organizational capabilities and integrated care processes and outcomes.
Keywords
As populations age, health system reform efforts in many countries emphasize integrated care as a means to better manage the complex health and social care needs of the elderly and other vulnerable patient groups (Johri, Beland, & Bergman, 2003; Pham, 2010; Wodchis, Dixon, Anderson, & Goodwin, 2015). Integrated care interventions bring together multiple health and/or social service professionals and organizations to replace fragmented care with care that is better coordinated, patient centered, and cost effective (Singer et al., 2011). Despite the growth of integrated care interventions, evidence of their effectiveness is mixed and relatively little is known about what factors are associated with successful implementation over time and across diverse contexts (Bardsley, Steventon, Smith, & Dixon, 2013; Low, Yap, & Brodaty, 2011). As a result, experts often challenge the transferability of successful integrated care interventions and emphasize adaptation to the local context as a prerequisite for success (Goodwin, Dixon, Anderson, & Wodchis, 2014; Stewart, Georgiou, & Westbrook, 2013). The success of integrated care interventions may thus be strongly influenced by the context and associated capabilities of the organizations in which they are implemented (Bardsley et al., 2013; Curry & Ham, 2010; Woolf & Johnson, 2005). Assessing these capabilities is challenging, as there are many relevant concepts and measures linked to improved care integration.
We define “organizational capabilities” as the ability and capacity of an organization, or group of organizations, to perform coordinated sets of tasks that support integrated care delivery. This definition encompasses both the internal capabilities of individual organizations and the collective interorganizational capabilities needed to leverage and combine knowledge and resources from multiple organizations. Organizational capabilities derive from the knowledge and skills of the people in the organization as well as organizational structures, processes, and norms supporting integration (Teece, Pisano, & Shuen, 1990). Organizational capabilities can include leadership, governance, and information technology as well as key processes such as improving quality of care. Such factors are widely recognized as influencing the success or failure of integrated care interventions (Curry & Ham, 2010; Friedman & Goes, 2001; Gillies, Shortell, Anderson, Mitchell, & Morgan, 1993; Ling, Brereton, Conklin, Newbould, & Roland, 2012; Suter, Oelke, Adair, & Armitage, 2009), but the current knowledge base lacks specificity about when and how these factors matter. This gap in knowledge is attributable, in large part, to the limited description and measurement of organizational capabilities in empirical studies on integrated care.
Many studies evaluating integrated care interventions describe the organizations involved in implementing the intervention in a few sentences, if at all (e.g., Baillie et al., 2014; Kautz, Gittell, Weinberg, Lusenhop, & Wright, 2007; Solberg et al., 2009), or incorporate a few, easily measureable variables such as the organizations’ age, size, and staff mix (Burns et al., 2001; Lin & Wan, 1999; Wan, Ma, & Lin, 2001). Some integrated care studies provide more detailed assessments of organizational capabilities but use qualitative case study methods (e.g., Williams & Sullivan, 2009; Kreindler et al., 2012), limiting standardized comparative analyses. The growth of efforts in many settings to integrate care speaks to the broad need for more systematic and standardized approaches, utilizing both qualitative and quantitative methods, to measure and evaluate the organizational capabilities required to implement and sustain integrated care interventions (Wodchis et al., 2015). To date few measurement systems have been developed with the aim of rigorously characterizing and comparing a wide range of organizational capabilities, spanning structural, process, and sociocultural elements (e.g., Estabrooks, Squires, Cummings, Birdsell, & Norton, 2009).
The aim of this article was to identify, organize, and assess survey instruments and scales for describing and comparing the organizational capabilities required for effective integrated care delivery and to examine the extent to which identified instruments have been used to study integrated care interventions. Using a systematic approach, we developed a bank of psychometrically sound instruments to describe and compare a range of organizational capabilities; to aid the standardization of data collection on organizational capabilities across integrated care delivery models, settings, and studies; and to inform change management efforts.
Method
We used the Context and Capabilities for Integrating Care (CCIC) Framework to conceptualize organizational capabilities and to guide the identification of instruments. The CCIC Framework was developed through a literature review of integrated care and revised and validated through semistructured interviews with leaders and care providers engaged in the implementation and operation of integrated care networks in Ontario, Canada (Evans, Grudniewicz, Baker, & Wodchis, 2016). Participants represented over 35 distinct integrated care networks from across the province of Ontario and hailed from diverse organizations including primary care practices, hospitals, and community-based health and social service organizations. The CCIC Framework consists of 18 organizational and interorganizational capabilities in three categories: (1) basic structures, (2) people and values, and (3) key processes (Table 1). The framework shows how these organizational capabilities interact with characteristics of the integrated care intervention and characteristics of the patient population to shape the implementation and outcomes of integrated care interventions.
Context and Capabilities for Integrating Care (CCIC) Framework: Definitions and Examples.
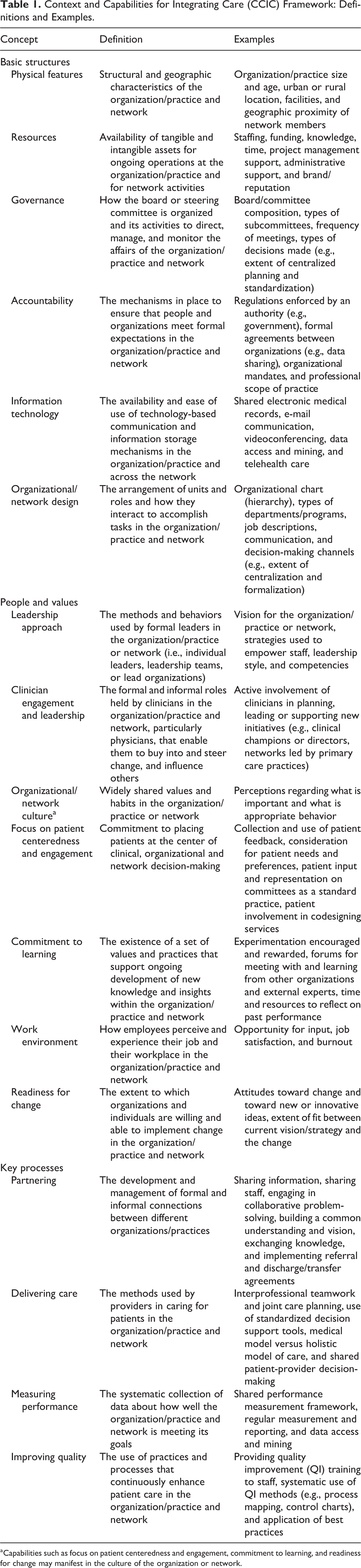
aCapabilities such as focus on patient centeredness and engagement, commitment to learning, and readiness for change may manifest in the culture of the organization or network.
Independent, iterative searches were conducted for each concept in the CCIC Framework using Medline and Google Scholar. Test searches were conducted to gauge the yield and foci of papers, and terms were modified accordingly to enhance relevance. The results of the database searches were displayed in order of relevance using each database’s sort function. We screened titles and abstracts for a minimum of the first 100 results and a maximum of the first 350 results; the average number of papers screened per factor was 284. We terminated screening when at least 30 consecutive papers were deemed irrelevant based on the inclusion criteria. To ensure that the remaining, unscreened references did not include potentially relevant studies, as part of our initial scoping searches we reviewed for relevancy five randomly selected titles/abstracts per search from among those that would not be screened based on our search strategy. None of the papers reviewed were relevant. Additional details on the search strategy are available upon request from the authors.
Abstracts and the full text of potentially relevant papers were screened for inclusion by two authors (J.M.E. and A.G.). Papers had to meet the following criteria for inclusion: (a) written in the English language, (b) description of the development and/or use of the quantitative instrument (or scale) in sufficient detail to enable assessment of its content, (c) the instrument measures one or more constructs in the conceptual framework, (d) the intended respondents of the instrument include health-care leaders and/or care providers (not exclusively patients or family members who may be unable to assess most dimensions), (e) a full copy of the instrument is accessible or can be obtained from the author(s) free of charge, and (f) the instrument has been used in a health-care setting. Papers published up to and including the year 2013 were included. We excluded proprietary instruments, as their cost may limit use by researchers and practitioners. We also excluded instruments that do not have details on their development and measurement properties in peer-reviewed publications, such as those described in books and theses. Systematic reviews of instruments that emerged during our search and the reference lists of included papers were also reviewed to identify potentially relevant papers for screening.
We supplemented our literature search with an expert consultation. A convenience sample of experts in health services management research across Canada were asked to identify instruments that measure the organizational capabilities outlined in the CCIC Framework. Expert consultation is commonly used in scoping and systematic reviews (Levac, Colquhoun, & O’Brien, 2010; Petticrew & Roberts, 2005), including reviews of measurement instruments (e.g., Kaplan et al., 2010; Scott, Mannion, Davies, & Marshall, 2003). Investigators with the Health System Performance Research Network (www.hsprn.ca) and other Canadian experts known to members of the research team were contacted. A total of 40 experts responded and collectively identified 30 instruments/papers.
The following data were extracted from each included paper: purpose of the study, study design, setting, respondents, name of the instrument, purpose of the instrument, instrument dimensions and definitions, theoretical basis of the instrument, number of survey items, type of scale, and psychometric properties. The data extraction table was organized by instrument and focused primarily on the original paper that introduced and tested the instrument.
Three key criteria were used to assess the instruments. The first criterion was psychometric properties. Using the Consensus-based Standards for the selection of health Measurement Instruments (COSMIN) Checklist (http://www.cosmin.nl/the-cosmin-checklist_8_5.html) and the work of Brennan, Bosch, Buchan, and Green (2012, 2013) as guides, we examined each instrument’s psychometric properties (validity and reliability). The second criterion was practical considerations, including cognitive complexity, length, previous response rates, and complex administration requirements (e.g., group consensus method with facilitator). Instruments with very weak psychometric properties, insufficient detail on psychometric properties, or high respondent or researcher burden were excluded at this stage. The third criterion was applicability to integrated care interventions. Two questions guided assessment of instrument applicability: (1) Has the instrument been used with an integrated care intervention? If not, can it be readily applied or easily modified for use with an integrated care intervention? and (2) to what extent is the instrument applicable to the diverse types of care providers and organizations that may be involved in an integrated care intervention (e.g., primary care providers, acute care hospitals, home care providers, public health units, and social service organizations)? If not widely applicable, can the instrument be easily modified to enhance relevance to multiple health-care settings? To determine use in an integrated care intervention or setting, we searched Google Scholar using the instrument name paired with the term “integrated care.” Relevant academic as well as gray literature publications were included. Instruments deemed too specific to a particular context (e.g., intensive care units) or set of professionals (e.g., doctor–nurse relationships), and not easily modified for broader applicability, were excluded at this stage. Only instruments that passed all criteria described above are reported on here (n = 58).
Results
A total of 4,580 titles and abstracts were screened for inclusion based on the database searches and the expert consultation. After the removal of irrelevant papers, 175 underwent full-text screening and an additional 32 papers were excluded for irrelevancy. The remaining 143 papers/instruments were reviewed against the inclusion criteria, and 60 instruments were excluded. Several relevant instruments were excluded at this stage because the instruments were proprietary, not publicly available, authors were unreachable, or authors did not respond to our request for a copy of the instrument. Examples of very promising proprietary instruments that were excluded include the Multifactor Leadership Questionnaire (Bass & Avolio, 1990) and the Organizational Social Context Measure (Glisson et al., 2008). The 83 remaining instruments were assessed for psychometric properties, practical considerations, and applicability to integrated care interventions, and 25 survey instruments were subsequently excluded. Reasons for exclusion were related primarily to a lack of information on scale development and/or psychometric properties and to weak applicability to integrated care interventions (e.g., survey items that were specific to a particular health-care setting, interprofessional relationship, or clinical innovation). Figure 1 summarizes the screening process. Table 2 outlines the name of included instruments (n = 58) as well as which factor(s) in the CCIC Framework each instrument measures. Appendices outlining the characteristics of the included instruments and their psychometric properties are available online as supplementary materials.
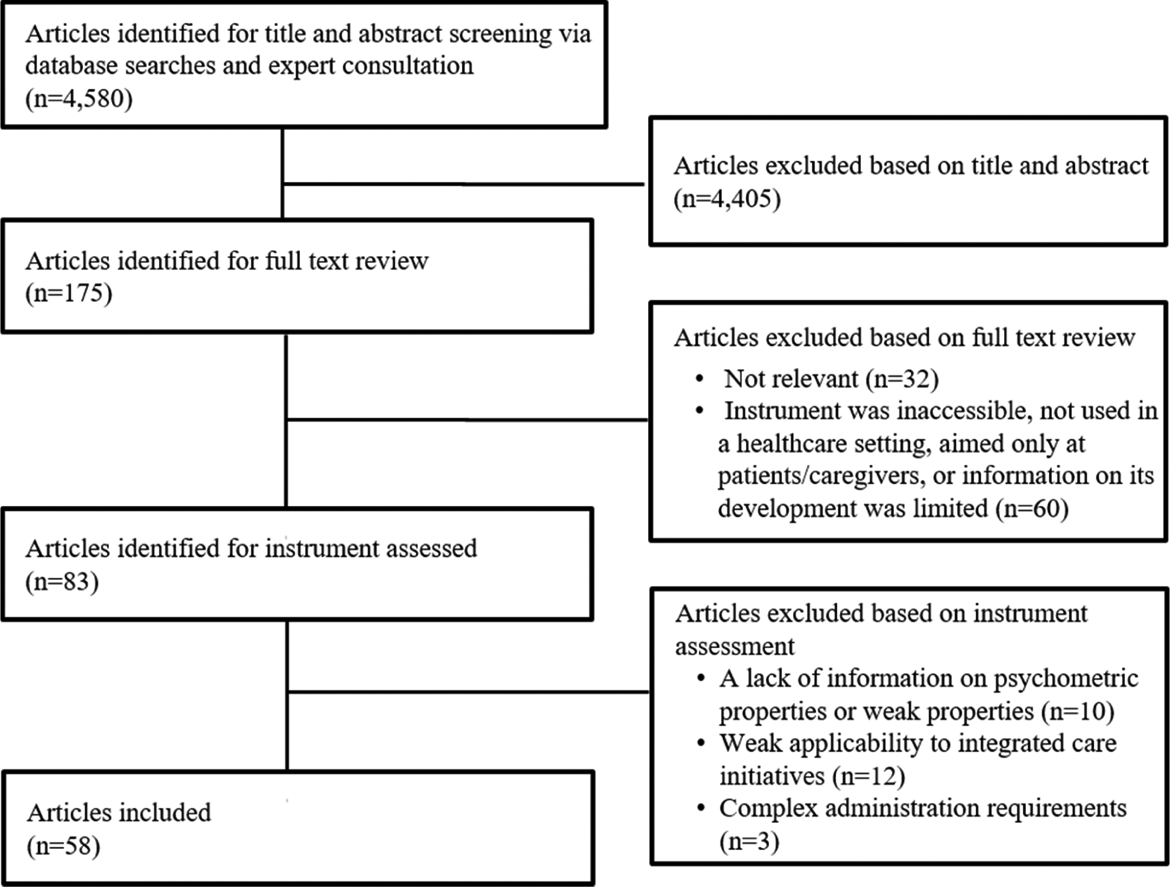
Flowchart of screening process.
Included Instruments and Organizational Factors Measured.

aDue to the high number of instruments specifically on teamwork, we categorized these instruments as “teamwork/delivering care” to distinguish them from four other instruments categorized under “delivering care” which do not examine teamwork.
Although most of the instruments were designed for use in health-care settings, some were originally developed and tested in business settings and later adapted for use in health care (n = 14). All of the instruments were self-administered questionnaires with ordinal scales. Most of the instruments measured factors captured under “people and values” (n = 26) and “key processes” (n = 30) as opposed to “basic structures” (n = 2). Organizational factors with the greatest selection of instruments include teamwork (n = 19, under the heading “delivering care”), work environment (n = 11), and readiness for change (n = 7). Only one instrument was identified for each of senior leadership approach and clinician engagement and leadership factors. There were also several factors, primarily under basic structures, for which no dedicated instruments were identified, including physical features, resources, governance, accountability, organizational design, measuring performance, and focus on patient centeredness and engagement. However, as Table 2 depicts, several instruments have survey items that reflect these elements. For example, the Partnership Self-Assessment Tool (PSAT) includes subscales on leadership and resources (Weiss, Anderson, & Lasker, 2002); the Alberta Context Tool includes subscales on work environment, culture, leadership, resources, and measuring performance (Estabrooks et al., 2009); the Survey of Organizational Attributes in Primary Care (SOAPC) includes items on clinician engagement, measuring performance, and organizational design (Ohman-Strickland et al., 2007); and the Care Process Self-Evaluation Tool (CPSET) includes items on teamwork, focus on patient centeredness and engagement, measuring performance, and partnering (Vanhaecht et al., 2007).
Instrument Development and Psychometric Properties
The development of all included instruments involved, at minimum, a literature review with reference to relevant theories. However, the quality or depth of the reviews and descriptions of the underlying instrument domains varied widely. The instruments were developed and/or applied in various countries, including the United States, the United Kingdom, Canada, Australia, New Zealand, Italy, Spain, France, Germany, Norway, Belgium, Denmark, Finland, Sweden, and the Netherlands. Common methods used during the development of the instruments included expert assessment (n = 21), stakeholder interviews or focus groups (n = 18), and pretesting or pilot testing (n = 19); most studies used a combination of these methods. Only four studies used cognitive testing. Most of the instruments underwent exploratory and/or confirmatory factor analysis to determine dimensionality (only 5 did not) as well as hypothesis testing to examine validity (12 did not). Internal consistency of the instruments and their scales, measured using Cronbach’s α, was usually above the standard threshold of .70; however, 16 instruments contained one or more scales that fell within the range of .52–.69. Interrater reliability and test–retest reliability were rarely measured.
Practical Considerations
Most of the instruments were moderate in length (between 20 and 40 items; n = 20), but several were also very short (less than 10 items; n = 7), short (less than 20 items; n = 14), lengthy (between 41 and 60 items; n = 11), or very lengthy (more than 60 items; n = 6). Response rates varied, but the majority were well above 60%, which may indicate that, in general, the instruments are easy to understand and complete.
Applicability to Integrated Care Interventions
The instruments were most often tested in hospital settings, though a few studies examined instruments in mental health, rehabilitation, or home care settings. The most common respondents consisted of nurses, physicians, and leaders/managers as well as members of multidisciplinary clinical teams. Only nine instruments require minor modifications to the wording of some items to enhance applicability across multiple health-care settings (e.g., replacing the term “hospital” with “organization” and “physician” with “clinician” or the insertion of specific professional groups or information systems).
Although all of the identified instruments may be applicable in assessing integrated care, only eight of the identified instruments have been used or explicitly recommended for use with integrated care interventions. The Organizational Culture Assessment Instrument (Zammuto & Krakower, 1991) was used by Maharaj (2010) to examine how organizational culture influenced the implementation of a care model aimed at integrating mental illness and substance use services. The Learning Organization Survey (Garvin, Edmondson, & Gino, 2008; Singer, Moore, Meterko, & Williams, 2012) was recommended for use by Mechanic, Perloff, Zinner, Razavi, and Keane (2012) in a report describing an evaluation plan for assessing health system reforms in the United States aimed, in part, at coordinating care and improving integrated delivery systems. The Team Climate Inventory Short-Form (Kivimaki & Elovainio, 1999) was used by Gibbon et al. (2002) to examine the impact of integrated care pathways and team notes on multidisciplinary teamwork in stroke care and rehabilitation and by Ouwens et al. (2009) to examine team climate before and after the implementation of an integrated care program for patients with head and neck cancers. The Relational Coordination Survey (Gittell, 2002) and the PSAT (Weiss et al., 2002) were used by Cramm and Nieboer (2012) to evaluate 19 chronic disease management programs that linked multidisciplinary professionals as well as primary care practices and hospitals. The PSAT was also recommended by Bainbridge, Brazil, Krueger, Ploeg, and Taniguchi (2010) to evaluate integrated palliative care. The Quality Improvement Implementation Survey II (Shortell et al., 2000) was used by Strandberg-Larsen et al. (2010) to compare levels of clinical integration in Kaiser Permanente Northern California and the Danish health-care system. The SOAPC (Ohman-Strickland et al., 2007) was used to evaluate two health promotion interventions in Spain involving interprofessional and interorganizational collaboration (Sanchez et al., 2009). Finally, the CPSET (Vanhaecht et al., 2007) was used by Vanhaecht et al. (2010) to examine the impact of clinical pathways on the organization of care for patients undergoing total joint replacement.
Discussion
This study identified 58 instruments that are currently available to assess organizational capabilities for integrated care delivery. Only eight of these instruments have been used, or recommended for use, with integrated care interventions. The eight instruments are focused primarily on organizational processes, such as teamwork, improving quality, and partnering, and were used in interventions focused on integrating specific sets of services associated with a single condition (e.g., cancer) or care sector (e.g., mental health) and mostly within as opposed to across organizational boundaries. These findings support our assessment that limited attention has been given to measuring organizational capabilities in empirical research on integrated care. Instead, the focus tends to be on understanding and measuring progress toward integrated care delivery in particular interventions rather than underlying organizational capabilities and conditions. In order to explain the effectiveness of integrated care interventions, explicit measures of the outcomes of integrated care must be supplemented by measures of organizational capabilities for integrated care including senior leadership style, organizational learning, work climate, and readiness for change, among others. Despite widespread recognition of the influence of these factors on the success of integrated care initiatives (Friedman & Goes, 2001; Ham & Walsh, 2013; Hartgerink et al., 2013; Ling et al., 2012; Martin-Rodriguez, Beaulieu, D’Amour, & Ferrada-Videla, 2005; Shortell, Gillies, Anderson, Mitchell, & Morgan, 1993; Suter et al., 2009; Williams & Sullivan, 2009), evidence is lacking on when and how these factors matter. Research needs to move beyond general statements about variations in the performance of integrated care interventions being due, for example, to “culture” or “leadership,” to more specific assessments of these capabilities. For example, which aspects of leadership are important at each stage of implementation and by which leaders (e.g., administrative or clinical)?
Collecting data on organizational capabilities as part of the planning, implementation, and/or evaluation stages of integrated care interventions could yield new insights on their outcomes and performance. Differing internal and collective capabilities among the organizations involved in integrating care may help explain the mixed outcomes reported in the literature (Bardsley et al., 2013; Curry & Ham, 2010). In practice, issues and challenges related to organizational capabilities, in particular to the compatibility and alignment (or lack thereof) among partnering organizations, are identified informally and only after considerable time and resources have been invested in implementation and change management (Burns & Pauly, 2002; Williams & Sullivan, 2009). An understanding of organizational capabilities early on in the implementation process across diverse organizations and practices may inform partner selection, the development of shared understandings of strengths and weaknesses among partners, and the design of targeted change management strategies.
Building a more robust evidence base on integrated care to inform practice requires the use of common instruments and consistent data collection methods across integrated care settings, interventions, and studies. Future research should explore links between the organizational capabilities in the CCIC Framework and integrated care delivery using some of the identified instruments. In order to generate sample sizes large enough to detect significant differences, the instruments can be used to promote standardization and improve evaluation in system-wide transformation efforts involving integrated care, such as the Health Links in Ontario, Canada, or the Integrated Care Pioneers Program in England as well as in U.S. demonstration projects involving integrated care, such as Accountable Care Organizations, Patient-Centered Medical Homes, or the Program for All-Inclusive Care for the Elderly.
This review provides a bank of validated survey instruments for researchers and practitioners to select from. A contingency perspective may assist in comparing and selecting instruments for use when critical constructs are identified a priori. Some instruments focus on a single construct, while others measure multiple constructs from the CCIC Framework, as Table 2 demonstrates. Focused instruments are useful for in-depth analysis of a specific area previously identified as important. Broader instruments, on the other hand, may be used as diagnostic tools to identify strengths and weaknesses across multiple organizational capabilities. Furthermore, some instruments may be particularly well suited for use in practice given their length and low cognitive complexity, while others with more depth, breadth, or theoretical grounding may be preferred for use in research studies. Finally, the instruments may be used at one point in time or at multiple points over time. However, multiple administrations may erode the sensitivity of some instruments.
Previous papers have attempted to systematically identify, compare, and recommend instruments for use in research and practice. However, these assessments tend to focus on specific capabilities, such as organizational culture or teamwork, and comprehensive up-to-date assessments are not available for all relevant factors. A notable exception is the recent work by Brennan et al. (2012, 2013) in which the authors systematically collated, categorized, and reviewed quantitative self-report instruments measuring organizational, process, and team-level and individual-level factors thought to influence the success of continuous quality improvement interventions. The latter results do not adequately address issues related to the spanning of interventions across diverse organizations applicable to integrated care interventions. Furthermore, despite some overlap in the inclusion of constructs such as teamwork, quality improvement, and readiness for change, the CCIC Framework incorporates additional constructs such as governance, focus on patient centeredness and engagement, delivering care, and information technology, among others.
This review also complements and extends Project INTEGRATE, a European initiative which involved the development of a common methodological framework and set of tools for evaluating and comparing integrated care interventions (Cash-Gibson & Rosenmoller, 2014). Their data collection tool kit consists of a case study report template that incorporates guidelines for retrospective process and data analysis as well as semistructured interviews with stakeholders. Their methods focus primarily on describing integrated care initiatives and their implementation. A section on the context for integrated care is also included in which five broad, open-ended questions are provided to aid in the identification of key enablers and barriers. The present review identifies validated quantitative survey instruments that may be implemented alongside the qualitative and secondary analysis methods proposed by Project INTEGRATE.
This study has some limitations. The instrument search strategy was based on the CCIC Framework and thus omits literature on topics not included in the framework. Furthermore, conducting a comprehensive and rigorous review of instruments is challenged by our focus on numerous constructs, many of which represent rich bodies of academic literature. As a result, it is possible that relevant papers and instruments were missed. The potential for inadvertently excluding applicable instruments is exacerbated by our search methods which involved using two databases, screening only the first 100–350 papers ordered by relevance, limiting our search terms to “measurement tool” and “measurement instrument,” and including instruments published in the academic literature and used in a health-care setting. However, our scoping searches suggest good coverage using Medline and Google Scholar, and a focus on health care ensures that the instruments reviewed can be readily applied to integrated care initiatives. We also expect that the expert consultation, while limited to selected experts in Canada, minimized the risk of missing relevant instruments. Nevertheless, some relevant instruments were ultimately excluded because we were unable to obtain a copy of the instrument for assessment.
Conclusion
This study provides a bank of psychometrically sound survey instruments to describe and compare a range of organizational capabilities. The results can be used to standardize data collection on organizational capabilities across integrated care interventions, settings, and studies. The use of standardized survey instruments will encourage comparison across both studies and settings, and facilitate longitudinal data collection to help inform our understanding of the influence of internal and collective organizational capabilities on performance and how these capabilities evolve over time. The application of standardized survey instruments across organizations and practices involved in an integrated care intervention can also inform change management efforts and possibly improve integrated care delivery as well as sustainability. Additional research is needed to build an evidence base for many of the tools reported here, validate their use in integrated care settings, test their sensitivity to changes in organizational capabilities over time, and explore the associations between organizational capabilities and various measures of integrated care processes and outcomes.
As policy interest in integrated care continues to grow, and with it demands for evidence of improved outcomes, providers and organizations are under increasing pressure to identify strategies to enhance the probability that their integrated care interventions will succeed. In this article, we support explicit attention to standardized measurement of organizational capabilities for the implementation, management, performance, and sustainability of integrated care interventions.
Footnotes
Authors’ Note
The views expressed in this article are those of the authors and do not necessarily reflect those of the funders.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Canadian Institutes of Health Research (CIHR, funding reference number TTF-128263) and from the Ontario Ministry of Health and Long-term Care Health System Performance Research Network (HSPRN, Grant # 06034).