
Abstract
This study investigates the effectiveness of a continuous nursing model in the postoperative rehabilitation of patients with lower extremity varicose veins. Using a randomised controlled trial design, we compared the outcomes of patients receiving continuous nursing care with those receiving routine care. The study included 120 patients divided equally into control and experimental groups. Outcomes were measured in terms of rehabilitation quality (wound healing time, lower extremity functional scale scores, complication rates) and quality of life (QoL). Significant improvements were seen in the experimental group across multiple measures, including faster wound healing (p < .05), better functional recovery (p < .01) and higher QoL scores (p < .01). These findings suggest that implementing a continuous nursing model can significantly enhance the postoperative rehabilitation and overall well-being of patients with lower extremity varicose veins.
Introduction
Lower extremity varicose veins present a common vascular disorder affecting a significant portion of the adult population worldwide. Epidemiological studies indicate a prevalence ranging from 20% to 64% in industrialised countries, with the risk factors including age, gender, obesity and occupations requiring prolonged standing (Fu et al., 2024; Yoo et al., 2024; Zhang et al., 2024). This condition not only impacts the aesthetic appearance of affected individuals but can also lead to significant discomfort, pain and, in severe cases, complications, such as venous ulcers and thrombosis (Urano et al., 2024).
The pathogenesis of primary varicose veins is complex and multifactorial, involving genetic predisposition, changes in vein wall structure and valvular incompetence (Liu et al., 2024). Understanding these underlying mechanisms is crucial for developing effective treatment and rehabilitation strategies. Moreover, the risk of recurrence following treatment remains a significant concern, highlighting the need for comprehensive long-term management approaches (Ghanaati et al., 2024; Gwozdzinski et al., 2024).
The importance of postoperative rehabilitation in varicose vein treatment cannot be overstated. While surgical interventions, including stripping, ligation and newer minimally invasive techniques, effectively address the immediate vascular issues, the recovery process plays a crucial role in determining long-term outcomes (Jiang et al., 2024). Proper rehabilitation ensures optimal wound healing, reduces the risk of complications and facilitates a quicker return to normal activities. Moreover, it significantly influences the patient’s quality of life (QoL) and satisfaction with the treatment (Fan et al., 2023; Yin et al., 2024).
Current clinical practice guidelines emphasise the need for comprehensive care of patients with varicose veins and associated chronic venous diseases (Pei et al., 2023; Rochon et al., 2023). These guidelines recommend a holistic approach to management, including lifestyle modifications, compression therapy and appropriate follow-up care. However, implementing these recommendations in the postoperative period often presents challenges, particularly when patients transition from hospital to home care.
The continuous nursing care model has been increasingly adopted across various medical fields, including cardiac rehabilitation, diabetes management and post-stroke care, demonstrating improved patient outcomes in these areas (Dai et al., 2022; Liu et al., 2019; Wang et al., 2019). This model extends beyond the traditional boundaries of in-hospital care, providing ongoing support and guidance to patients as they transition from hospital to home environments. Continuous nursing aims to bridge the gap between acute care and long-term recovery, ensuring that patients receive consistent, high-quality care throughout their rehabilitation journey (El-Sharkawy, 2023; Liu et al., 2023).
Recent advancements in varicose vein treatment, such as endovenous ablation techniques and foam sclerotherapy, have shown promising results in terms of efficacy and patient comfort (Huang & Lin, 2023; Kanber, 2023). However, these new treatment modalities also necessitate adapted postoperative care strategies to optimise outcomes and patient satisfaction.
The duration and intensity of postoperative care, particularly compression therapy, remain subjects of debate in the field. A meta-analysis by Huang et al. (2013) indicated that the optimal duration of compression therapy following varicose vein surgery varies depending on the specific procedure and patient characteristics. This highlights the need for personalised, continuous care approaches that can be adapted to individual patient needs over time.
Despite the recognised importance of comprehensive postoperative care, there is a paucity of research specifically examining the impact of continuous nursing models in the context of varicose vein surgery rehabilitation. This gap in the literature presents an opportunity to investigate whether the benefits observed in other areas of healthcare can be replicated for patients recovering from varicose vein procedures.
Therefore, this study develops and implements a comprehensive postoperative continuous nursing care protocol specifically tailored for patients undergoing lower extremity varicose vein surgery and evaluates its impact on rehabilitation quality and overall QoL. By addressing these objectives, we aim to contribute valuable insights to the field of vascular surgery nursing and potentially improve the standard of care for patients undergoing varicose vein treatments.
Methods
Study Design
This research employed a randomised controlled trial design to evaluate the effectiveness of a continuous nursing model in the postoperative rehabilitation of patients with lower extremity varicose veins. The study was conducted between January 2023 and December 2023. This design was chosen for its ability to minimise bias and provide robust evidence for the efficacy of the intervention. The study was registered at the ISRCTN registry (https://www.isrctn.com/; registration number: ISRCTN13537163).
Participants
This single-centre study was conducted at the Department of Vascular Surgery of Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences. Participants were recruited from consecutive admissions between January 2023 and December 2023. All patients who met the inclusion criteria during this period were invited to participate in the study. The inclusion criteria encompassed patients diagnosed with lower extremity varicose veins who were undergoing surgical treatment, aged 18–75 years and willing and able to provide informed consent. The exclusion criteria included the presence of severe comorbidities (e.g. uncontrolled diabetes or severe cardiovascular disease), cognitive impairments that could interfere with following postoperative instructions, participation in other clinical trials and pregnancy or breastfeeding.
Sample Size and Randomisation
A total of 120 patients meeting the inclusion criteria were recruited for the study. The sample size calculation was based on previous studies, assuming a medium effect size with a power of 0.80 and a significance level of 0.05. Participants were randomly assigned to either the control group (n = 60) or the experimental group (n = 60) using a computer-generated randomisation sequence. Allocation concealment was ensured using sequentially numbered, opaque sealed envelopes.
Intervention
This study compared two groups: a control group receiving standard postoperative care and an experimental group receiving a continuous nursing intervention. The control group received standard care at the hospital’s outpatient vascular clinic, including (1) initial wound care education during hospital stay (days 1–3 post-surgery); (2) scheduled clinic follow-ups at weeks 2, 6 and 12 post-discharge; and (3) standard wound care and compression therapy instructions. The experimental group received the continuous nursing intervention starting 48 hours before discharge, continuing through home-based care, with specified hospital clinic visits matching the control group’s schedule to maintain assessment consistency. The experimental group received a comprehensive intervention delivered by certified vascular nurse specialists (with a minimum of 5 years experience) who completed standardised training in the continuous nursing protocol (see Appendix 1 for the detailed protocol). The intervention included (1) pre-discharge education comprising two 60-min sessions conducted 48 hours before discharge using standardised educational materials and competency checklists; (2) weekly telephone consultations (15–30 minutes each) conducted by the same nurse specialist; (3) bi-weekly home visits (45–60 minutes each) for the first month, followed by monthly visits for 2 months; (4) 24/7 hotline access staffed by rotating nurse specialists; and (5) quality assurance through monthly team meetings and intervention fidelity checklists.
Outcome Measures
Primary outcomes included rehabilitation quality, assessed using the following measures. (1) The wound healing time, measured in days until complete epithelialisation (100% wound closure with no drainage). (2) The lower extremity functional scale (LEFS) (Binkley et al., 1999). This is a 20-item questionnaire scored 0–80, with higher scores indicating better function. Each item is rated on a 5-point scale (0–4), with total scores interpreted as 0–20 (extreme difficulty/unable to perform activities), 21–40 (quite a bit of difficulty), 41–60 (moderate difficulty) and 61–80 (minimal to no difficulty). The minimal clinically important difference is 9 points. (3) The visual analogue scale (VAS) for pain (Price et al., 1983). This is a 0–100-mm scale with higher scores indicating greater pain intensity. Scores are categorised as no pain (0–4 mm), mild pain (5–44 mm), moderate pain (45–74 mm) and severe pain (75–100 mm). The minimal clinically important difference is 13 mm. (4) Walking distance, measured using a standardised 6-min walk test protocol (ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories, 2002), with established test-retest reliability (intraclass correlation coefficient = 0.90) and a minimal clinically important difference of 50 m in patients with vascular disease. (5) The 36-item short-form health survey (SF-36) questionnaire (Ware & Sherbourne, 1992). This consists of eight scaled scores (0–100) measuring different aspects of health, with higher scores indicating better health status. Secondary measures included (1) the Beck depression inventory (Beck et al., 1996), a 21-item scale (0–63) with scores interpreted as 0–13 (minimal), 14–19 (mild), 20–28 (moderate) and 29–63 (severe depression); (2) the self-rating anxiety scale (Zung, 1971), a 20-item scale (20–80), with scores ≥45 indicating clinical anxiety; and (3) activities of daily living (ADL) (Mahoney & Barthel, 1965), measured using the Barthel index (0–100), with higher scores indicating greater independence. All outcomes were assessed at 1, 3 and 6 months post-surgery. Patient satisfaction was measured in terms of satisfaction with nursing care and overall treatment satisfaction.
Data Collection
Data were collected at baseline (pre-surgery) and 1, 3 and 6 months post-surgery. Trained research nurses, blinded to group allocation, conducted assessments and administered questionnaires. Physical examinations were performed by vascular surgeons who were also blinded to group assignment.
Statistical Analysis
All data were analysed using SPSS version 25.0 (IBM Corp, Armonk, NY, USA). Descriptive statistics were used to summarise baseline characteristics, with continuous variables expressed as means ± standard deviations and categorical variables presented as frequencies and percentages. For comparing outcomes between the control and experimental groups, independent t-tests were used for normally distributed continuous variables, Mann–Whitney U tests for non-normally distributed continuous variables and chi-squared tests or Fisher’s exact tests for categorical variables. Repeated measures analysis of variance (ANOVA) was employed to analyse changes in outcomes over time within and between groups. A p-value of <0.05 was considered statistically significant for all analyses.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki and approved by the institutional review board of our hospital. All participants provided written informed consent before enrolment. Patient confidentiality was maintained throughout the study, and participants were informed of their right to withdraw at any time without affecting their standard of care.
Results
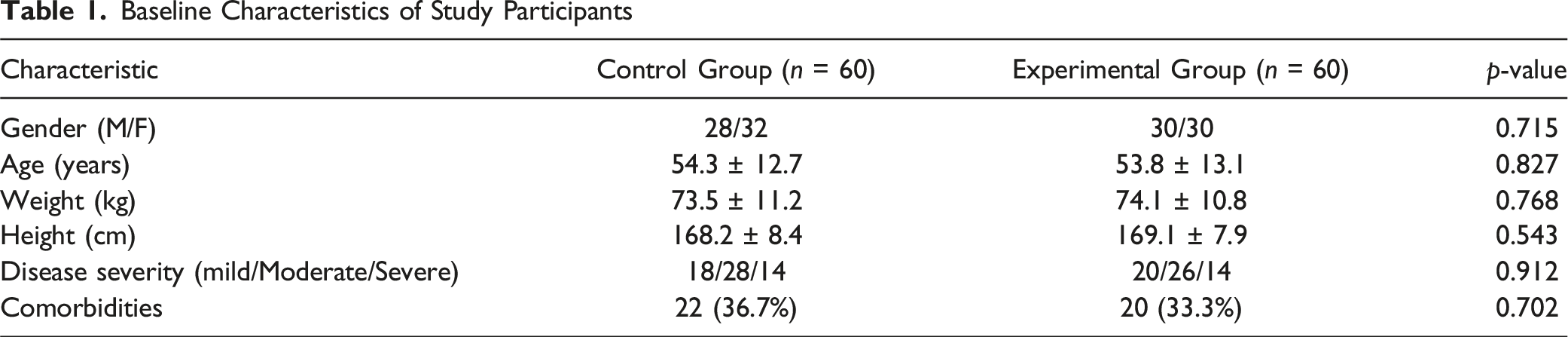
Baseline Characteristics
Baseline Characteristics of Study Participants
Rehabilitation Quality Outcomes
Primary and Secondary Outcomes at Baseline and Follow-Up Time Points
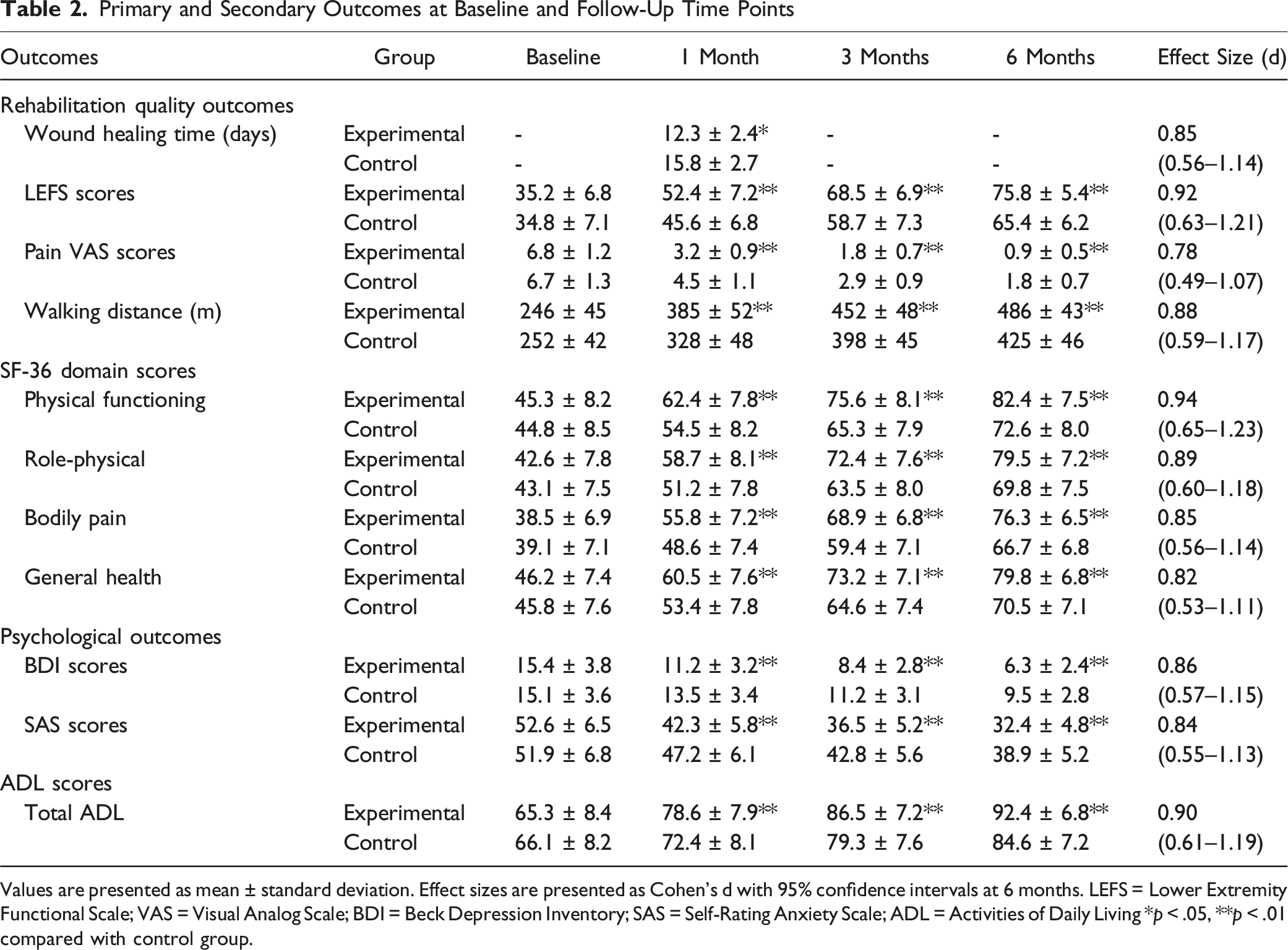
Values are presented as mean ± standard deviation. Effect sizes are presented as Cohen’s d with 95% confidence intervals at 6 months. LEFS = Lower Extremity Functional Scale; VAS = Visual Analog Scale; BDI = Beck Depression Inventory; SAS = Self-Rating Anxiety Scale; ADL = Activities of Daily Living *p < .05, **p < .01 compared with control group.
Quality of Life Outcomes
Table 2 presents the SF-36 scores for both groups at 6 months post-surgery. The experimental group demonstrated significantly higher scores across all SF-36 domains, indicating better overall QoL at 6 months post-surgery.
Psychological Outcomes
Table 2 shows the psychological assessment results for both groups at 6 months post-surgery. The experimental group showed significantly lower depression and anxiety scores, as well as higher life satisfaction ratings compared with the control group.
Activities of Daily Living
Table 2 presents the ADL scores for both groups at different time points. The experimental group consistently showed higher ADL scores at all time points, indicating better functional recovery and independence in daily activities.
Patient Satisfaction
Patient satisfaction scores revealed significantly higher ratings in the experimental group compared with the control group for both nursing care satisfaction (9.2 ± 0.8 vs. 7.8 ± 1.3, p < .001) and overall treatment satisfaction (9.3 ± 0.7 vs. 8.1 ± 1.1, p < .001)
Discussion
Impact of Continuous Nursing on Rehabilitation Quality
The results of this study demonstrate a significant positive impact of the continuous nursing model on the rehabilitation quality of patients recovering from lower extremity varicose vein surgery. The experimental group, which received the continuous nursing intervention, showed markedly better outcomes across all measured parameters of rehabilitation quality.
The significantly shorter wound healing time observed in the experimental group can be attributed to several factors within the continuous nursing model. The pre-discharge education on proper wound care techniques, coupled with regular follow-ups and home visits, likely contributed to better adherence to wound care protocols. This finding aligns with previous studies that have highlighted the importance of patient education and regular monitoring in promoting wound healing and preventing complications, such as venous ulcers (Carroll et al., 2013).
The LEFS scores were consistently higher in the experimental group at all time points (1, 3 and 6 months post-surgery). This improved functional recovery can be linked to the personalised exercise regimens and gradual activity resumption guidelines provided as part of the continuous nursing intervention. The structured approach to rehabilitation, with ongoing support and adjustments, appears to have facilitated a more efficient and effective recovery of lower limb function. These results are consistent with the recommendations outlined in clinical practice guidelines for the management of chronic venous disease (Wittens et al., 2015).
The lower complication rate observed in the experimental group is a particularly noteworthy finding. This reduction in complications can be attributed to several aspects of the continuous nursing model, including early detection and management of potential issues through regular follow-ups, better patient compliance with post-operative instructions and improved overall care continuity. The importance of preventing complications in varicose vein surgery cannot be overstated, as complications can significantly impact patient recovery and long-term outcomes (Brake et al., 2013).
Pain management, as measured by the VAS, was also more effective in the experimental group. The lower pain scores at 1 month post-surgery suggest that the continuous nursing model provided better pain management strategies and support. This could be due to the combination of appropriate medication guidance, non-pharmacological pain management techniques and psychological support offered as part of the intervention. These findings align with studies emphasising the importance of comprehensive pain management in improving patient outcomes and satisfaction following varicose vein surgery (Mackenzie et al., 2002).
The significantly greater walking distance achieved by the experimental group at 1 month post-surgery is indicative of faster physical recovery and improved mobility. This outcome is likely a result of the structured exercise programmes and activity guidelines provided through the continuous nursing model. The ability to walk longer distances not only reflects better physical recovery but also contributes to overall well-being and QoL, as highlighted in previous research on the impact of varicose vein treatment on patient-reported outcomes (Darvall et al., 2012).
Impact of Continuous Nursing on Quality of Life
The SF-36 scores at 6 months post-surgery provide compelling evidence of the positive impact of the continuous nursing model on patients’ QoL. The experimental group showed significantly higher scores across all eight domains of the SF-36, indicating a comprehensive improvement in both physical and mental aspects of health-related QoL.
The most substantial improvements were observed in the ‘physical functioning’ and ‘role–physical’ domains. These results suggest that patients who received continuous nursing care were better able to perform physical activities and fulfil their roles without limitations due to physical health. This aligns with the improved LEFS scores and walking distances observed in the rehabilitation quality outcomes and supports the findings of previous studies on the relationship between successful varicose vein treatment and improved QoL (Carroll et al., 2013).
Notably, the ‘mental health’ and ‘social functioning’ domains also showed significant improvements. This indicates that the continuous nursing model had a positive impact not only on physical recovery but also on psychological well-being and social interactions. The psychological support and coping strategies provided as part of the intervention likely contributed to these improvements. These findings are particularly important given the known impact of chronic venous disease on patients’ mental health and social functioning (Lurie et al., 2020).
The enhanced scores in the ‘vitality’ domain suggest that patients in the experimental group experienced higher energy levels and less fatigue. This could be attributed to the combination of better physical recovery, pain management and psychological support offered through the continuous nursing model. The improvement in vitality is consistent with previous research demonstrating the positive effects of comprehensive care approaches on patient-reported energy levels and overall well-being (Van den Bos et al., 2009).
Implications for Clinical Practice
The findings of this study have several important implications for clinical practice in the management of patients undergoing varicose vein surgery. First, they support the implementation of continuous nursing models as a standard of care for these patients, given the comprehensive benefits observed across multiple outcome measures. The components of the continuous nursing model used in this study, including pre-discharge education, personalised home-based care plans, scheduled follow-ups and psychological support, provide a framework that can be adapted and implemented in various healthcare settings.
The improved outcomes and high patient satisfaction rates suggest that investing in such comprehensive care models could be cost-effective in the long run, potentially reducing readmissions and complications. This aligns with the growing emphasis on value-based healthcare and the need for interventions that improve patient outcomes while optimising resource utilisation (O’Flynn et al., 2014).
Moreover, the study highlights the importance of personalised care approaches in varicose vein treatment. The continuous nursing model allowed for ongoing assessment and adjustment of care plans based on individual patient needs and progress. This personalised approach is particularly relevant given the variability in patient responses to treatment and the need for tailored postoperative care strategies, as noted in recent clinical guidelines (Marsden et al., 2013).
The study also underscores the importance of addressing both physical and psychological aspects of recovery following varicose vein surgery. The integration of psychological support and coping strategies within the continuous nursing model contributed to improved mental health outcomes and overall QoL. This holistic approach aligns with the contemporary understanding of the biopsychosocial model of health and the interconnectedness of physical and mental well-being (Lurie et al., 2020).
Limitations and Future Directions
Although this study provides strong evidence for the efficacy of continuous nursing models in varicose vein surgery rehabilitation, it has several limitations that should be addressed in future research. First, as a single-centre study, the generalisability of the findings to other healthcare settings or patient populations may be limited. Multicentre studies are needed to validate these findings across diverse healthcare contexts.
Second, while the 6-month follow-up period provided valuable insights into short- and medium-term outcomes, longer-term studies are needed to assess the durability of the observed benefits and the potential impact on disease recurrence rates. This is particularly important given the known risk of varicose vein recurrence and the need for long-term management strategies.
Future research should also explore the specific components of the continuous nursing model that contribute most significantly to improved outcomes. This could help optimise and streamline the intervention, making it more feasible to implement in resource-constrained settings. Additionally, cost-effectiveness analyses would be valuable in quantifying the economic impact of implementing continuous nursing models in varicose vein surgery care.
Finally, with the ongoing advancement of minimally invasive techniques for varicose vein treatment, future studies should investigate how continuous nursing models can be adapted to support patients undergoing these newer procedures. This could include exploring the integration of telemedicine and mobile health applications to further improve the accessibility and efficiency of care delivery.
Conclusion
The adoption of continuous nursing models has the potential to significantly enhance the quality of care and outcomes for patients undergoing varicose vein surgery. As healthcare continues to evolve towards more patient-centred and integrated care models, the findings of this study contribute valuable evidence to support this transition in the field of vascular surgery and rehabilitation.
Supplemental Material
Supplemental Material - Research on the Application of Continuous Nursing Model in Postoperative Rehabilitation of Patients With Lower Extremity Varicose Veins
Supplemental Material for Research on the Application of Continuous Nursing Model in Postoperative Rehabilitation of Patients With Lower Extremity Varicose Veins by Junxia Du, Yuan Bai, and Ying Yu in Evaluation & the Health Professions
Supplemental Material
Supplemental Material - Research on the Application of Continuous Nursing Model in Postoperative Rehabilitation of Patients With Lower Extremity Varicose Veins
Supplemental Material for Research on the Application of Continuous Nursing Model in Postoperative Rehabilitation of Patients With Lower Extremity Varicose Veins by Junxia Du, Yuan Bai, and Ying Yu in Evaluation & the Health Professions
Footnotes
Authors’ Contributions
Conception and design of the work: Du JX; Data collection: Bai Y, Yu Y; Supervision: Du JX; Analysis and interpretation of the data: Bai Y, Yu Y; Statistical analysis: Du JX, Yu Y; Drafting the manuscript: Du JX; Critical revision of the manuscript: all authors; Approval of the final manuscript: all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.