
Abstract
Global geopolitical tensions are quickly increasing the threat of significant transboundary radiological emergencies. The past nuclear and radiological disasters have highlighted critical deficiencies, yet the international healthcare system is still inadequately equipped for extensive nuclear and radiological crises. Our analysis of contemporary vulnerabilities, focusing on ongoing near-miss scenarios at the Zaporizhzhia Nuclear Power Plant and persistent systemic gaps in low- and middle-income countries (LMICs). The primary gap is the misalignment between global policy frameworks and frontline clinical preparedness. We suggest enhancing healthcare education, incorporating mental health into emergency preparedness strategies, strengthening early warning systems and transboundary radiological emergency response, and improving the availability of medical countermeasures. A standardized strategy is essential to enhance resilience in the face of future nuclear and radiological emergencies.
Introduction
The danger of a significant nuclear and radiological crisis is an immediate and growing risk to worldwide safety. By January 2025, an estimated 12,241 nuclear warheads remain in the global arsenal, with 2,100 maintained in a high state of readiness, marking the end of the post-Cold War era of arms reduction (Institute, 2025). Ongoing military activities around critical infrastructure, particularly the Zaporizhzhia nuclear power plant (ZNPP), which has experienced 12 complete off-site power outages since February 2022, and rapid global arms modernization have intensified concerns (Agency, 2025). However, healthcare systems remain inadequately prepared for these hazards. Even with WHO and IAEA frameworks, critical preparedness gaps persist, particularly in low- and middle-income countries (LMICs). We identify four urgent priorities: workforce training, early warning systems, mental health support, and stockpiling medical countermeasures.
Current Gaps and Challenges
Past nuclear and radiological disasters revealed major weaknesses in healthcare preparedness. The Fukushima Daiichi disaster showed systemic underpreparedness: at Futaba Hospital, 39 of 338 (11.5%) inpatients died before evacuation could be completed due to inadequate planning and fragmented communication (Sawano et al., 2022). A survey of Japan’s Nuclear Emergency Core Hospitals found only 31% anticipated a radiation disaster, and under 10% of radiological technologists at these facilities received formal disaster medicine training (Nagata et al., 2022). Western countries face similar threats; disaster-team affiliation among US emergency medical technicians is lower than in Japan (24.5% vs. 42.7%) (Dallas et al., 2017). The nursing workforce is especially underprepared: about 75% of US nursing schools offer either no radiation-related content or less than 1 hour of it in their curricula (Bowen et al., 2020). These deficits are urgent near conflict zones, where atmospheric modeling suggests a major ZNPP radionuclide release could affect large parts of Europe, the Middle East, and North Africa (Sharifi et al., 2022). Many LMICs still lack standardized radiation-response training, coordinated monitoring systems, mental health support, and adequate medical stockpiles. Global implementation of radiation-disaster training remains inconsistent.
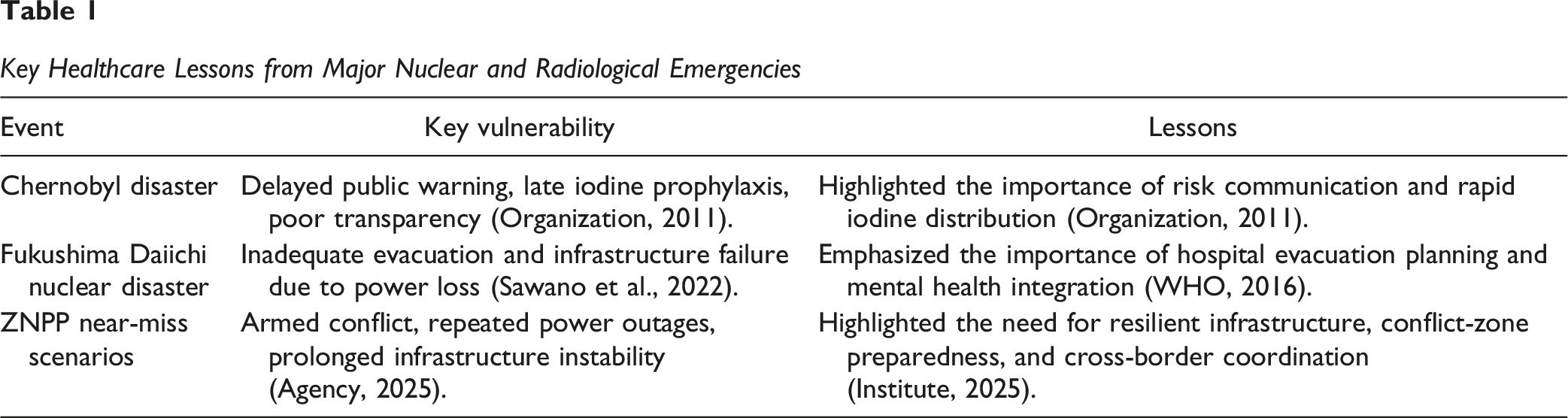
Key Healthcare Lessons From Major Nuclear and Radiological Emergencies
Key Healthcare Lessons from Major Nuclear and Radiological Emergencies
Recent events demonstrate the growing global urgency of nuclear risks. Near-miss scenarios at ZNPP highlight acute geopolitical vulnerabilities. Since February 2022, 12 complete power outages at ZNPP have escalated the persistent regional risk. Atmospheric models warn that a major radionuclide could affect large parts of Europe, the Middle East, and North Africa (Sharifi et al., 2022). These events can become regional public health emergencies.
Psychological Trauma: The Invisible Toll of Nuclear Disasters
Nuclear disasters affect long-term mental health. A review of 79 Fukushima-related studies reported persistently elevated rates of post-traumatic stress (10.5%–62.6%) and depressive symptoms (12%–52%) among survivors (Shigemura et al., 2021). The Chernobyl Forum concluded mental health effects were the most significant public health consequence of the 1986 accident-a burden compounded by prolonged uncertainty and public mistrust (Cardis & Hatch, 2011). Critically, impaired mental health among frontline healthcare workers creates a systemic feedback loop in which psychological deterioration reduces clinical capacity precisely when it is most needed. Yet mental health integration is neglected worldwide, particularly in LMICs, where the WHO estimates that at least one in five emergency-affected individuals will develop a diagnosable mental health condition (Organization, 2020).
Addressing this gap requires targeted interventions. Psychological First Aid (PFA)-an evidence-informed early intervention designed to reduce acute distress and strengthen coping mechanisms-must be mandated for integration into standard nuclear emergency drills, supported by simulation-based protocols that replicate the cognitive and emotional demands of real radiological events (Chandler et al., 2022). Given the geographic dispersal of survivors and the collapse of local infrastructure that typify nuclear evacuations, telepsychiatry platforms provide an essential and scalable mechanism for post-disaster psychological triage, with demonstrated reductions in PTSD severity in recent mass-disaster settings (Gareayaghi et al., 2025). Mental health should be treated as a core component of nuclear and radiological emergency preparedness.
Recommendations for Global Actions
Readiness for nuclear and radiological emergencies relies on synchronized alert and response systems. Monitoring and early warning networks such as the International Radiation Monitoring Information System (IRMIS), Comprehensive Nuclear-Test-Ban Treaty Organization (CTBTO-IMS), and the European Union Radiological Data Exchange Platform (EURDEP), facilitate rapid identification of radiological events. Furthermore, standardized risk communication and legal frameworks, such as the IAEA Assistance Convention and GSR Part 7, enable effective international coordination.
Building on the foundational strategies above, WHO member states should incorporate nuclear scenarios into the International Health Regulations (IHR) to improve readiness, including fully equipped emergency medical systems and intensive training for healthcare personnel in disaster response, mental health, and decontamination. Integration of artificial intelligence (AI)-based modeling using live meteorological data, building aerodynamics, and patient mobility to develop real predictive models at the microscale will facilitate the prompt identification of contamination zones (FEMA, 2023). Additionally, developing a dynamic route-planning approach for the safest evacuation of HCPs could enhance radiation plume modeling. Post-disaster psychological triage can also incorporate modern AI-based tools, bolstering the provision of emergency psychological aid via telehealth in reducing morbidity (Jendoubi, 2025). The COVID-19 pandemic has exposed gaps in MCM supplies. Furthermore, insufficient potassium iodide (KI) stockpiles or of diethylenetriaminepentaacetic acid (DTPA) treatment facilities, due to severe environmental and infrastructural limitations in resource-constrained settings, may increase the risk to exposed populations (Maglas et al., 2024). This highlights the requirement of strategic stockpiling, especially in LMICs.
Conclusion
The persistent shortages of funding, training, communication, and storage infrastructure reveal the global system’s unpreparedness. Lessons from past events highlight the need for mental health integration, early warning systems and stronger preparedness. Enhancing the capacity of healthcare workers is crucial through organized training, robust early warning systems, and legislative frameworks. An urgent multidisciplinary strategy integrating community, technological, and medical approaches is required.
Footnotes
ORCID iDs
Author Contributions
The manuscript was conceptualized by NNHL, JMAA, MRH and NTH. NNHL extrapolated data for the literature review and synthesis; JMAA, MRH, PMK, MQL, LBDH, THV, NPHHT, ZZ and NTH lead read of work. NNHL, JMAA, MRH, PMK, MQL, ZZ and NTH formulated the outline for the manuscript. The first author is either NNHL or JMAA. Provide critical scientific input and assist with content refinement: MRH, PMK, MQL, LBDH, THV & NPHHT. NNHL, JMAA, MRH, ZZ and NTH reviewed existing policy frameworks and regional health priorities relevant to the topic. Review and editing of the final manuscript: all authors. NTH had the ultimate responsibility for deciding whether to submit for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article is partially funded by the Shenzhen Basic Research Program (JCYJ20241202124859016) for Zhilin Zhang.