
Abstract
The Ankle-Brachial Index (ABI) is universally mandated for diabetic foot ulcer (DFU) risk stratification, yet its prognostic validity for tissue repair remains structurally inconsistent. To evaluate this diagnostic paradox, we implemented a target trial emulation framework in a dual-campus prospective cohort of 528 patients, utilizing doubly robust estimation and restricted cubic splines to characterize the non-linear relationship between continuous ABI and 20-week healing outcomes. The analysis revealed a profound hemodynamic divergence. The ABI maintained log-linear validity as a predictor against major amputation (OR 0.77 per 0.1-unit increase). In contrast, wound healing followed an inverted U-shaped trajectory. Healing efficacy reached a structural peak at an ABI of approximately 0.90, yielding a 27.9% predicted area reduction. Beyond this threshold, the incremental prognostic benefit of the metric plateaued and eventually collapsed. Sensitivity analyses confirmed that this loss of fidelity is a diagnostic artifact driven by extreme medial arterial calcification (≥1.30) rather than physiological perfusion loss. These findings demonstrate that reliance on categorical ABI thresholds induces a systemic misclassification of microvascular risk. Consequently, clinical guidelines should transition toward continuous hemodynamic profiling and multi-modal assessments to identify occult ischemia in pseudonormalized populations, effectively decoupling diagnostic strategies for limb salvage from tissue repair.
Keywords
Introduction
The global burden of diabetes mellitus continues to escalate at an unprecedented rate, with recent estimates from the International Diabetes Federation reporting a prevalence of 589 million adults (Duncan et al., 2025). Within this expanding epidemiological landscape, the diabetic foot ulcer (DFU) represents a devastating sequela, affecting up to one-third of diabetic patients during their lifetime (Armstrong et al., 2020). The clinical consequences are frequently catastrophic, as these ulcerations act as the sentinel event for approximately 84% of non-traumatic lower-limb amputations (McDermott et al., 2023). While neuropathy often precipitates the initial injury, the adequacy of lower-limb perfusion fundamentally dictates wound fate, making accurate hemodynamic assessment via the Ankle-Brachial Index (ABI) universally mandated for risk stratification (Fitridge et al., 2024).
However, the evaluative utility of the ABI is increasingly complicated by a hemodynamic paradox that undermines the validity of current diagnostic standards (Chuter et al., 2024). While low ABI values robustly predict macro-vascular failure such as amputation, the relationship between ABI and tissue repair remains erratic. Numerous evaluations have failed to establish a consistent correlation between ABI readings and healing trajectories, creating a fragmented clinical picture (Argyriou et al., 2024). This inconsistency likely stems from a mechanistic decoupling between macro-circulatory pressure and micro-circulatory metabolic demand, further exacerbated by hyperglycemia-driven medial arterial calcification (MAC). By stiffening vessel walls and artificially inflating systolic readings, MAC induces a state of “pseudo-normality” where a normal ABI (0.90–1.30) masks occult microvascular failure (Aboyans et al., 2012).
From a methodological perspective, the traditional reduction of the ABI to a binary categorical metric discards granular continuous data and obscures complex non-linear patterns. Systematic evidence is currently lacking regarding whether the ABI influences wound healing through a linear trajectory or if arterial non-compliance creates specific structural inflection points where the prognostic fidelity of the metric collapses (Brouwers et al., 2022). Relying on universal, age-agnostic thresholds risks a systemic misclassification of vascular risk, necessitating a more rigorous audit of the ABI’s structural validity within a causal inference framework (Hernán & Robins, 2016).
To address these evaluative gaps, we implemented a prospective study utilizing a target trial emulation framework. Our primary objective was to deconstruct the non-linear dose-response relationship between the continuous ABI and 20-week wound healing outcomes. By deploying doubly robust estimation to minimize confounding bias, we aimed to isolate the independent prognostic value of the ABI and identify the specific thresholds where arterial calcification distorts diagnostic signals (Bang & Robins, 2005). This approach seeks to provide a more stable methodological foundation for clinical decision-making, ensuring that hemodynamic assessments accurately reflect the physiological requirements of diabetic tissue repair.
Methods
Target Trial Emulation and Structural Framework
Implementation of a target trial emulation framework allowed for the rigorous assessment of the structural validity of the ABI (Robins & Finkelstein, 2000). The prospective, dual-campus observational design addressed two methodological imperatives: (a) mitigating baseline confounding and (b) neutralizing measurement errors inherent to diabetic hemodynamic assessments. Temporal synchronization was enforced through a strict Time Zero (T0) protocol. T0 was operationalized as the exact date of formal study enrollment and initial referral. This architecture anchored covariate ascertainment and outcome tracking to a unified baseline, effectively preventing immortal time bias.
Institutional Context and Ethical Governance
The evaluation cohort was assembled between October 2024 and August 2025 across two high-volume clinical sites: the University of Malaya Medical Centre (UMMC) and the University Malaya Specialist Centre (UMSC). Recruitment bypassed isolated specialist silos by integrating multidisciplinary pathways, including orthopedic surgery, trauma, and dedicated diabetes care units. Independent institutional review boards validated the ethical protocols for UMMC (MREC Ref: 20241023-14342) and UMSC (MREC Ref: 2025113-14583). Following written informed consent, clinical variables were archived within the ipesakit institutional registry. The surveillance framework adhered strictly to the Declaration of Helsinki and STROBE guidelines to maintain longitudinal fidelity (Von Elm et al., 2007).
Participant Selection and Measurement Fidelity
Inclusion Benchmarks and Baseline Standardization
Eligibility thresholds were established a priori to secure the construct validity of the target population. Participants were required to meet specific inclusion criteria: (a) age of 18 years or older; (b) documented Type 2 Diabetes Mellitus fulfilling American Diabetes Association (ADA) standards (American Diabetes Association Professional Practice Committee et al., 2025); (c) active diabetic foot ulceration categorized as Wagner Grade 1 to 3; and (d) commitment to a standardized 20-week clinical monitoring protocol.
Exclusionary Filters and Structural Integrity
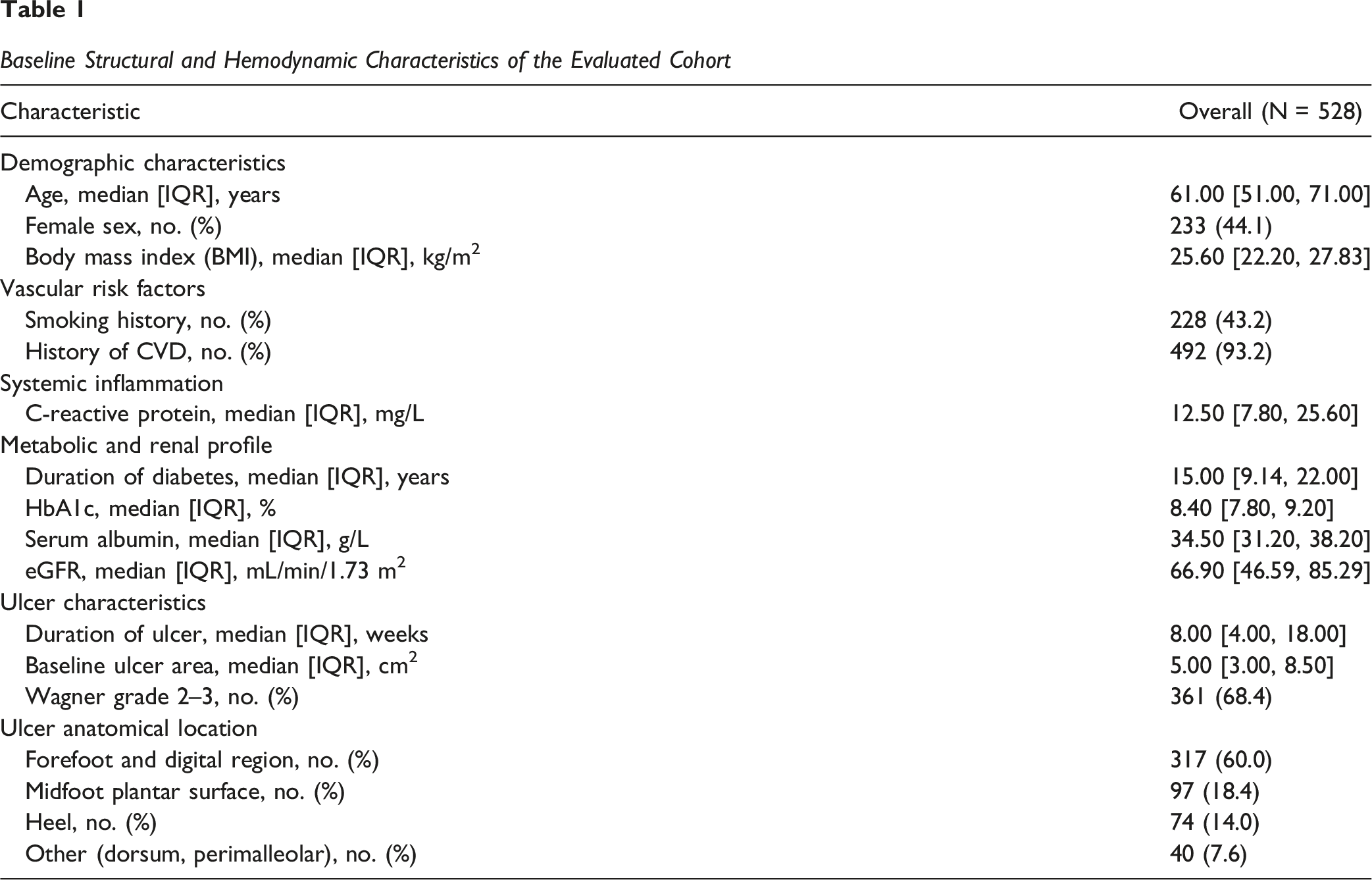
To protect the evaluation from external measurement artifacts, strict exclusionary filters were applied. Patients were ineligible if they presented with: (a) ulcers of non-diabetic etiology such as venous stasis or trauma; (b) conditions limiting life expectancy to under six months; (c) chronic systemic immunosuppression; (d) critical limb ischemia necessitating immediate surgical amputation; (e) ipsilateral revascularization performed within the previous three months or scheduled at baseline; and (f) incomplete baseline covariate data. This multi-layered screening matrix ensured the structural integrity of the subsequent causal inference modeling. At enrollment, the anatomical location of each target ulcer was systematically documented according to a standardized regional classification: forefoot and digital region, midfoot plantar surface, heel, and other sites encompassing the dorsum and perimalleolar area. The predominance of forefoot and digital lesions (60.0%; n = 317) is consistent with the neuropathic pressure distribution characteristic of this patient population, while heel and midfoot involvement reflected the neuroischemic burden present across the higher Wagner grade strata.
Clinical Protocol and Metabolic Standardization
Control of extraneous variance in healing trajectories was achieved by enforcing a uniform multidisciplinary care protocol based on International Working Group on the Diabetic Foot (IWGDF) guidelines (Schaper et al., 2024). Standardized interventions encompassed regular sharp debridement, rigorous infection control, and structured mechanical offloading. Antibiotic therapy was governed by an infection-tiered protocol consistent with IWGDF recommendations (Schaper et al., 2024). For all participants presenting with clinical evidence of active wound infection at enrollment, specifically the presence of at least two local inflammatory indicators including erythema, localized warmth, induration, or purulent discharge, empirical broad-spectrum antibiotic therapy was initiated within 24 hours of confirmed eligibility. Transition to culture-directed narrow-spectrum regimens was implemented following microbiological sensitivity reporting, typically within 48 to 72 hours of wound swab processing. Participants requiring intravenous therapy were co-managed by the infectious disease and orthopaedic surgery teams, with oral step-down guided by documented clinical improvement at subsequent surveillance visits. Mechanical offloading was applied universally and stratified by ulcer anatomical location. Total contact casting served as the primary modality for plantar forefoot and midfoot lesions, whereas irremovably modified removable cast walkers were deployed for heel and dorsal wounds where direct casting was contraindicated. Adherence was documented at each scheduled visit, and any deviation from the assigned offloading protocol was recorded as a protocol exception within the institutional registry. Within the evaluation framework, metabolic stabilization functioned as a core parameter. Systemic instability was neutralized through continuous monitoring of glycemic and nutritional indices, specifically HbA1c and serum albumin. Systemic glucocorticoid exposure was tightly restricted and documented to prevent unmeasured pharmacological interference with the outcome metrics.
Hemodynamic Measurement and Metric Operationalization
Certified vascular personnel ascertained the primary evaluative metric, the ABI, at T0 via a strict handheld Doppler protocol (Aboyans et al., 2012). Hemodynamic reproducibility was secured through a mandatory 10-min supine rest period prior to measurement. The analytical framework deliberately bypassed traditional binary categorization by modeling the ABI as a continuous variable. This decision preserved granular dose-response data, enabling the detection of non-linear diagnostic signals routinely obscured by the conventional 0.90 threshold. To explicitly deconstruct measurement distortion, supra-physiologic readings exceeding 1.30 were retained in their raw form rather than artificially truncated. Such operationalization permitted the direct statistical modeling of medial arterial calcification and pseudo-normal hemodynamics. A pre-planned sensitivity analysis subsequently isolated the predictive validity of pure occlusive disease by excluding these non-compressible vessels.
Outcome Operationalization and Censoring Management
Primary and Secondary Endpoints
Baseline target ulcers were identified by the largest surface area or most advanced Wagner grade, quantified via digital planimetry. For participants presenting with concurrent satellite lesions, clinical surveillance and outcome adjudication were strictly restricted to the primary index ulcer. Tracking multiple distinct healing trajectories within a single systemic host violates the independence assumption required for doubly robust estimation. We operationalized the singular index lesion to represent the primary metabolic demand, deliberately excluding satellite wounds from the quantitative data collection architecture to prevent competing healing rates from destabilizing the primary outcome metric. The primary evaluative endpoint was defined as the Percentage Area Reduction (PAR) at 20 weeks. This extended observation window deliberately bypassed the conventional 12-week benchmark to capture the protracted kinetic spectrum of neuroischemic repair. By operationalizing PAR as a continuous outcome rather than utilizing binary closure events, the analytical framework preserves granular physiological data across advanced lesions. This design effectively accommodates the severe chronicity of the cohort and avoids the misclassification of substantial yet incomplete regenerative progress. The PAR was calculated according to the following equation:

To fortify the analysis against extreme outliers, PAR values were Winsorized to a strict bounded range of −100% to 100%. The incidence of major ipsilateral limb amputation served as the secondary outcome.
Adjudication and Attrition Correction
Critical clinical events, specifically amputation, revascularization, or death, triggered a composite failure adjudication and were automatically assigned a PAR value of −100%. Within the 20-week observation window, 23 participants (4.4%) underwent ipsilateral revascularization procedures following enrollment. These events were not anticipated at baseline and arose in response to progressive ischemic deterioration identified during scheduled surveillance visits. Each case was reviewed by the adjudication panel, confirmed as a protocol-defined composite failure event, and assigned a PAR of −100% prior to IPCW integration. This handling ensures that the hemodynamic benefit of revascularization does not artificially inflate wound healing estimates within the primary analytical models, preserving the interpretive integrity of the ABI as the sole exposure of interest. No participants were revascularized electively or as a pre-planned procedure during the observation period; all 23 cases represented unscheduled clinical interventions driven by documented deterioration in limb perfusion status. To neutralize selection bias introduced by participant attrition, the evaluation framework incorporated Inverse Probability of Censoring Weighting (IPCW) (Cole & Hernan, 2008; Robins & Finkelstein, 2000). This causal inference technique corrected for non-medical loss to follow-up, ensuring the evaluated cohort continuously reflected the baseline population and preserving the longitudinal integrity of the data.
Analytical Framework for Validity Assessment
Statistical Software and Distributional Testing
Computational procedures were executed using R software (Version 4.3.2) (Austin, 2018). Assessment of data distribution involved the Shapiro-Wilk test. Continuous variables are reported as the mean with standard deviation for parametric data or the median with interquartile range for non-normal distributions. Categorical metrics are presented as frequencies and percentages. Inter-group comparisons were performed using two-tailed Student’s t-tests, Wilcoxon rank-sum tests, Chi-squared tests, or Fisher’s exact tests as appropriate. Statistical significance was maintained at a two-tailed alpha of 0.05.
Structural Covariate Selection Protocols
Structural adjustment sets were established a priori based on clinical pathways and structural modeling principles to secure internal validity (Harrell, 2015). To prevent overadjustment and preserve the integrity of the causal path, no post-baseline variables were permitted within the regression models. Highly skewed covariates underwent log-transformation to ensure distributional stability. The final adjustment matrix encompassed five critical domains: (a) demographics including age, sex, and body mass index; (b) vascular burden encompassing smoking status and cardiovascular history; (c) systemic inflammation measured via C-reactive protein; (d) metabolic and renal function comprising diabetes duration, HbA1c, serum albumin, and eGFR; and (e) wound characteristics including ulcer duration, Wagner grade, and baseline area. The adjustment matrix deliberately prioritized proximal physiological and metabolic drivers of arterial non-compliance, such as renal function and glycemic chronicity. Sociodemographic proxy variables, including race and ethnicity, were omitted from the primary causal models. This structural decision prevents the conflation of pure biomechanical hemodynamic signals with complex, unmeasured socio-cultural determinants of healthcare access.
Composite Weighting for Causal Inference
The evaluation framework implemented a composite weighting strategy to neutralize baseline confounding and potential selection bias resulting from participant attrition. Baseline covariate balance was achieved via stabilized weights derived from the Generalized Propensity Score (GPS) (Austin, 2018). Informative censoring was simultaneously addressed through IPCW. The participant-specific weight (

Stability of the estimation was ensured by Winsorizing extreme weights at the 1st and 99th percentiles. Post-weighting balance was evaluated using absolute correlation coefficients between the ABI and baseline covariates. Achieving a threshold of less than 0.1, visualized through Love plots, served as the formal benchmark for validating the pseudo-population suitable for causal inference.
Doubly Robust Estimation and Non-linear Modeling
The analytical core utilized a Doubly Robust (DR) estimation framework to minimize residual confounding (Bang & Robins, 2005). This methodology integrated baseline covariates into outcome models that were simultaneously weighted by the composite framework. For the primary outcome of 20-week PAR, weighted linear regression was employed. The analysis evaluated potential non-linear dose-response relationships between the ABI and wound repair via Restricted Cubic Splines (RCS) with four knots positioned at standard percentiles (Harrell, 2015). Non-linearity was formally assessed using Wald-type tests. Where significant curvature was detected, spline analysis identified data-driven inflection points using the median ABI as the reference value. Secondary outcomes involving major amputation were modeled through weighted logistic regression. Effect sizes are reported per 0.1-unit increase in the ABI as regression coefficients (β) or odds ratios (OR) with corresponding 95% confidence intervals (CI). Standard errors were estimated using Robust Sandwich Estimators to accommodate potential model misspecification.
Robustness Validations and Heterogeneity Assessments
The robustness of the primary findings was verified through a multi-layered sensitivity matrix: (a) per-protocol analysis to evaluate adherence impact; (b) exclusion of non-compressible vessels (ABI >1.30) to isolate the predictive effects of pure occlusive disease; (c) threshold validation using the ABI as a categorical variable based on RCS-derived inflection points; and (d) assessment of potential unmeasured confounding via E-values (VanderWeele & Ding, 2017). Prespecified subgroup analyses were stratified by age, sex, smoking status, and Wagner grade. Heterogeneity of effect was evaluated through interaction terms within the weighted regression models. Findings are summarized via forest plots to visualize stratum-specific effect sizes and their associated uncertainties.
Data Governance and Ascertainment Fidelity
Standardization and Blinded Outcome Assessment
Strict adherence to ICH-GCP guidelines governed all evaluative procedures (Abraham, 2010). Clinical personnel completed mandatory standardization protocols prior to cohort enrollment to minimize observer variance. To neutralize detection bias, wound morphometrics and Wagner grading were independently quantified by two outcome assessors strictly blinded to baseline hemodynamic profiles. Quantitative outputs were averaged to establish the final metric.
Data Integrity and Adjudication Protocols
Inter-rater morphometric discrepancies exceeding 10% or categorical grading conflicts triggered mandatory adjudication by a third independent physician. Longitudinal data integrity was fortified through a double-entry verification architecture. This system systematically cross-referenced digital registry inputs against primary clinical source documents to ensure zero-loss fidelity.
Reporting Standards and Power Considerations
Compliance and Reproducibility
The evaluation architecture adhered strictly to the STROBE guidelines to ensure methodological transparency (Von Elm et al., 2007). To facilitate reproducibility, all causal inference procedures and weighting algorithms utilized established R packages, specifically WeightIt for Generalized Propensity Score estimation and rms for Restricted Cubic Spline modeling. All analytical codes were archived within the institutional registry to maintain a verifiable audit trail of the evaluation process.
Sample Size Sufficiency and Validity
The final cohort size of 528 participants was evaluated a priori to ensure sufficient statistical power for the doubly robust framework (Austin & Steyerberg, 2015). Given the implementation of the 13-variable adjustment matrix, the sample provided approximately 40 observations per variable for the primary healing model. This ratio significantly exceeds the conventional threshold for stable coefficient estimation in multivariable modeling. Post-hoc power calculations confirmed that the study was adequately powered to detect a minimum 5% difference in PAR with a two-tailed alpha of 0.05 and a power exceeding 0.80, thereby securing the reliability of the clinical inferences derived from the non-linear models.
Results
Cohort Assembly and Baseline Structural Dynamics
Baseline Structural and Hemodynamic Characteristics of the Evaluated Cohort
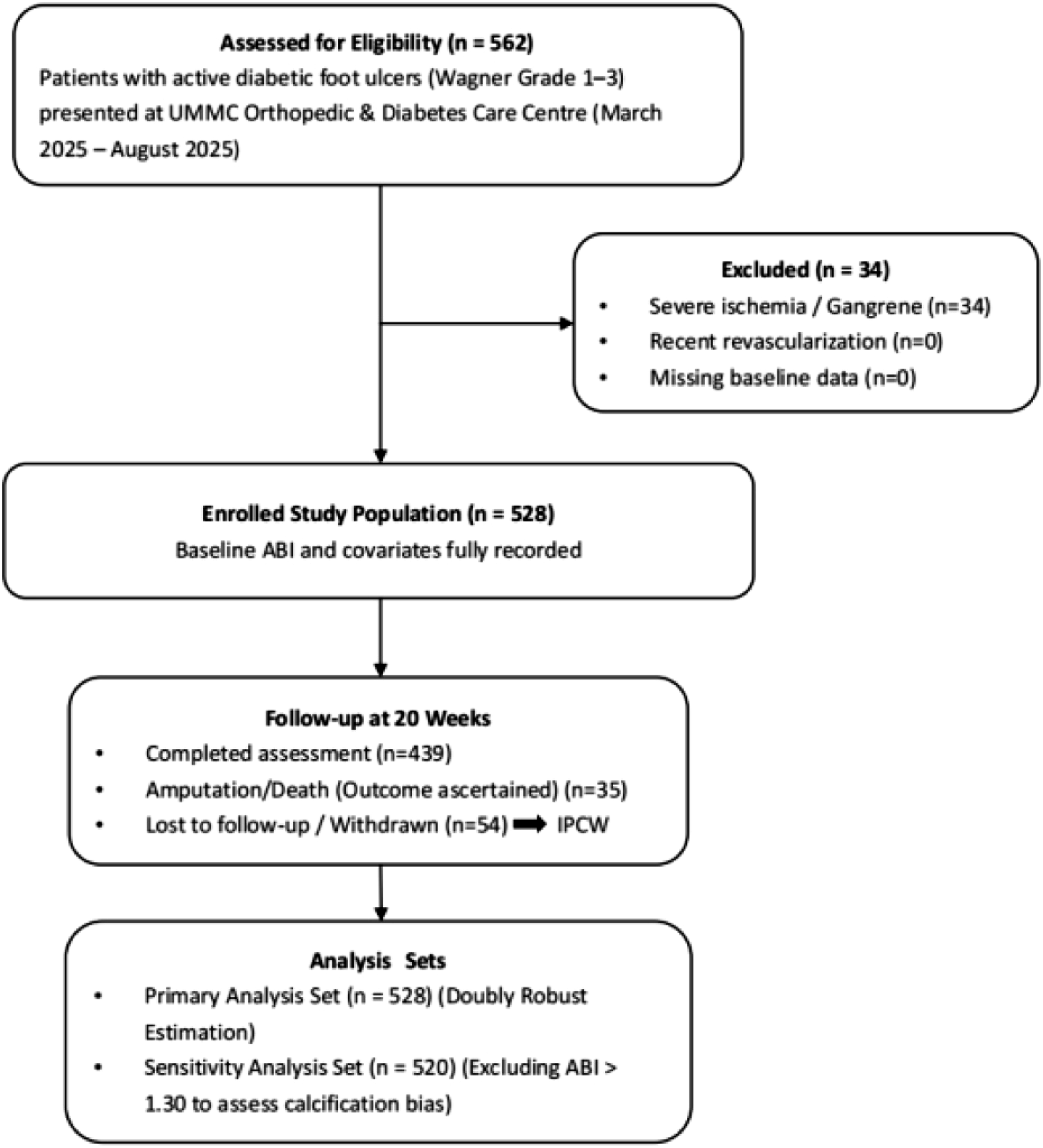
Participant Screening and Attrition Trajectory Within the Target Trial Emulation Framework.
Target Trial Emulation Fidelity and Covariate Balance
The composite weighting algorithm successfully neutralized baseline structural confounding. Generalized Propensity Score (GPS) implementation generated stable weight distributions without extreme truncation penalties. The effective sample size (ESS) was maintained at 217.1 after stabilizing weights. Crucially, the weighting architecture achieved strict covariate balance; absolute correlation coefficients for all specified confounding domains were systematically compressed below the rigorous 0.10 threshold across the entire continuous ABI spectrum. This diagnostic confirmation validates the simulated pseudo-population, ensuring that subsequent outcome models are robust against measured baseline imbalances (Supplemental Table S1; Supplemental Figure S1).
Evaluation of Linear Hemodynamic-Healing Trajectories
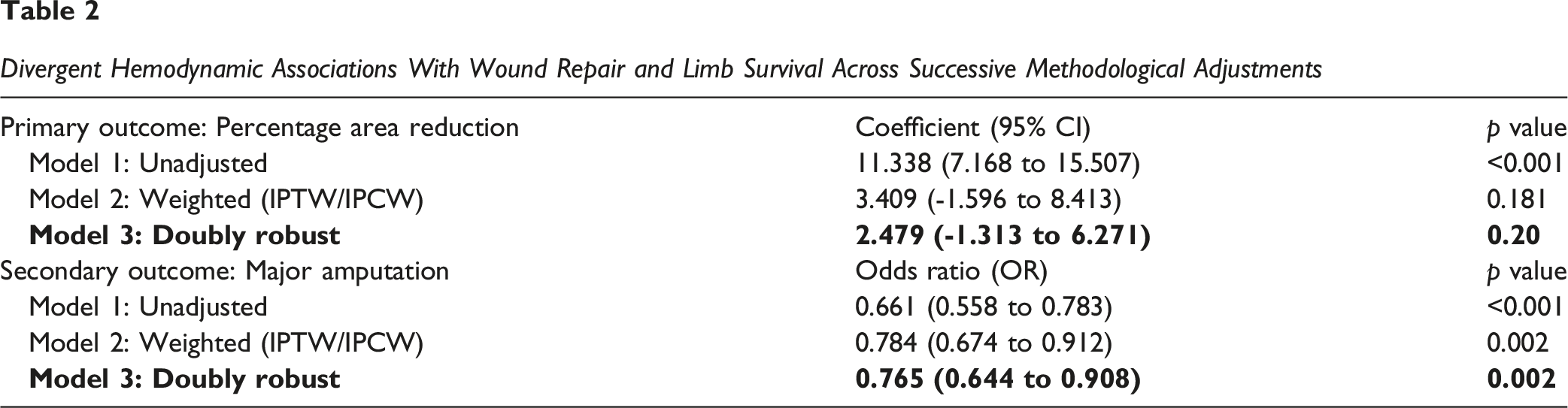
Divergent Hemodynamic Associations With Wound Repair and Limb Survival Across Successive Methodological Adjustments
Hemodynamic Impact Divergence and Major Amputation Risk
In stark contrast to the healing outcomes, the ABI maintained robust structural validity as a linear predictor of limb survival. Across all model specifications, higher ABI values consistently conferred protection against critical ischemic events. Within the fully adjusted doubly robust framework, each 0.1-unit incremental increase in baseline ABI translated to a highly significant 23.5% reduction in the odds of major ipsilateral amputation (OR 0.77; 95% CI 0.64–0.91; p = 0.002). This divergence confirms that while ABI fails to linearly predict the metabolic demands of wound closure, it remains a mathematically stable proxy for the macro-circulatory flow required to prevent tissue necrosis (Table 2).
Non-Linear Hemodynamic Threshold Modeling
Restricted cubic spline (RCS) modeling delineated a significant inverted U-shaped relationship between the continuous ABI and 20-week PAR (p for non-linearity <0.001; Figure 2). The structural dose-response relationship bifurcated into three discrete hemodynamic phases. In the primary ischemic phase (ABI <0.62), predicted PAR values were negative, indicating a state where perfusion is insufficient to meet basal metabolic requirements, resulting in progressive wound expansion or clinical deterioration (Figure 2). Non-linear Dose-Response Dynamics Between the Continuous Ankle-Brachial Index and Healing Efficacy.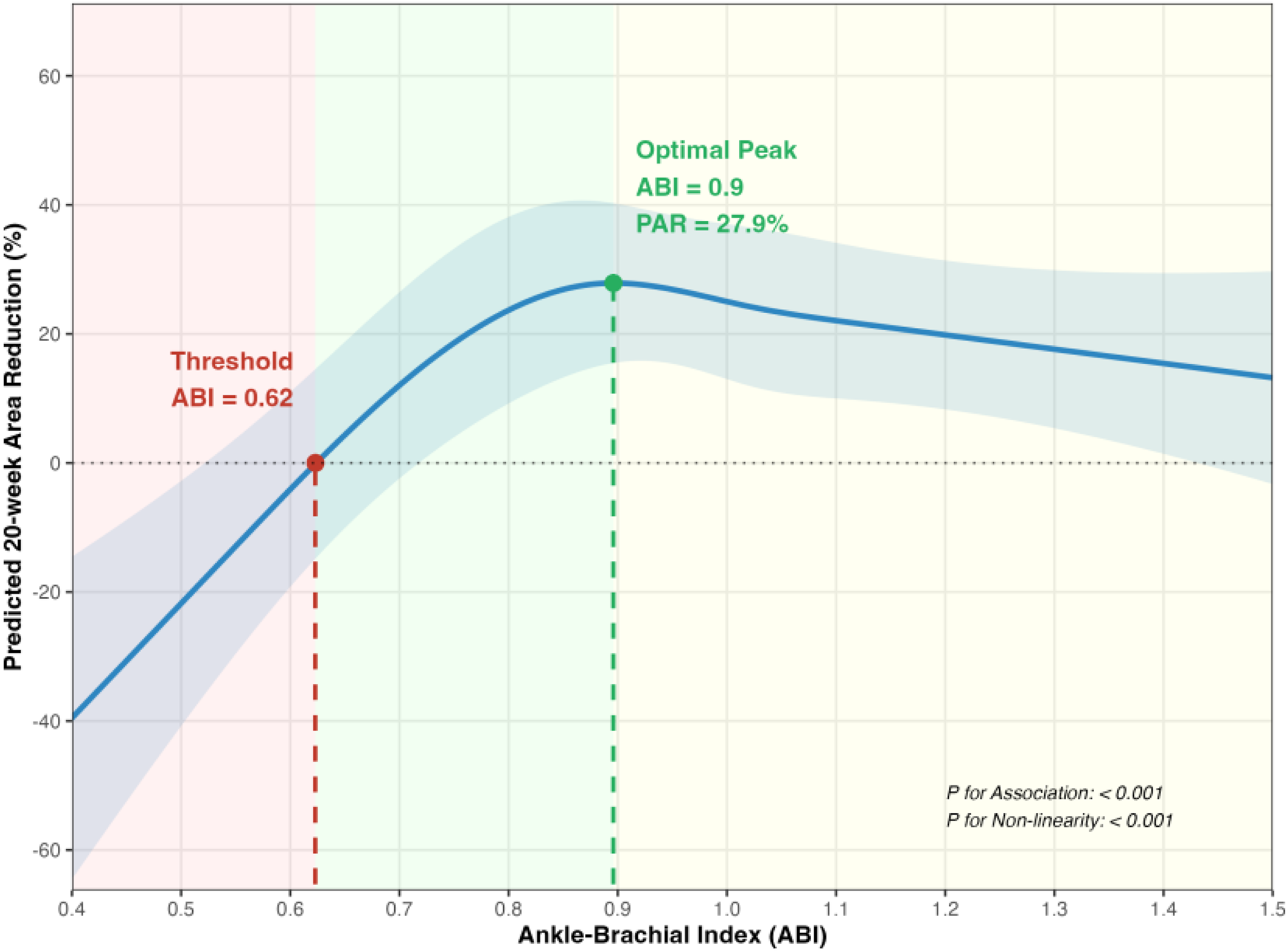
The therapeutic acceleration phase (0.62 ≤ ABI ≤0.90) demonstrated that healing efficacy increased with higher perfusion pressure, reaching a maximum predicted PAR of 27.9% at the 0.90 inflection point. Conversely, in the pseudo-normal phase (ABI >0.90), the healing benefit deviated from linear expectations and entered a sustained declining trajectory. This divergence suggests that beyond the 0.90 threshold, the prognostic fidelity of the ABI is systematically compromised by competing vascular pathologies, primarily medial arterial calcification.
Sensitivity Matrices for Robustness Validation
Multiple sensitivity analyses confirmed the stability of the primary findings across varying analytical scenarios (Supplemental Table S2). Notably, following the planned exclusion of non-compressible vessels (ABI ≥1.30), a positive linear association between the ABI and PAR was successfully restored (β = 6.67; 95% CI 0.40–12.94; p = 0.038). This restoration provides empirical evidence that the downward trajectory observed in the full cohort is a diagnostic artifact driven heavily by extreme arterial stiffening (≥1.30). Without the negative leverage of these non-compressible vessels, the 0.62 to 1.29 range functions as a net positive continuous spectrum.
Furthermore, threshold validation using traditional categorical assignments revealed no significant difference in healing efficacy between the sub-optimal (0.62–0.90) and assumed optimal (≥0.90) groups (p = 0.742). Rather than contradicting the non-linear model, this statistical parity confirms the “ceiling effect” of the ABI. It demonstrates that once the 0.62 ischemic threshold is surpassed, further elevations into the pseudo-normal range (≥0.90) do not confer superior tissue repair, thereby invalidating the traditional reliance on 0.90 as a definitive therapeutic benchmark. Severe healing impairment was specifically isolated to the high-risk ischemic group (ABI <0.62; β = −40.66; 95% CI -82.25 to 0.93; p = 0.056).
To assess the potential impact of unmeasured confounding, E-value analysis yielded point estimates of 1.87 for major amputation and 1.66 for the primary healing outcome. These values indicate that substantial unmeasured confounding would be required to negate the observed associations, thereby reinforcing the structural robustness of the doubly robust estimates.
Subgroup Heterogeneity Assessment
Effect modification analysis revealed that age and sex significantly modified the association between the ABI and tissue repair (p for interaction <0.001; Figure 3). Hemodynamic benefits were predominantly localized to participants aged ≥65 years (n = 215) and female cohorts (n = 233). This localization suggests that tissue repair in these specific demographics may possess a higher degree of macro-perfusion dependence, potentially due to age-related microvascular rarefaction. Effect Modification and Stratum-Specific Heterogeneity Across Clinical Subgroups.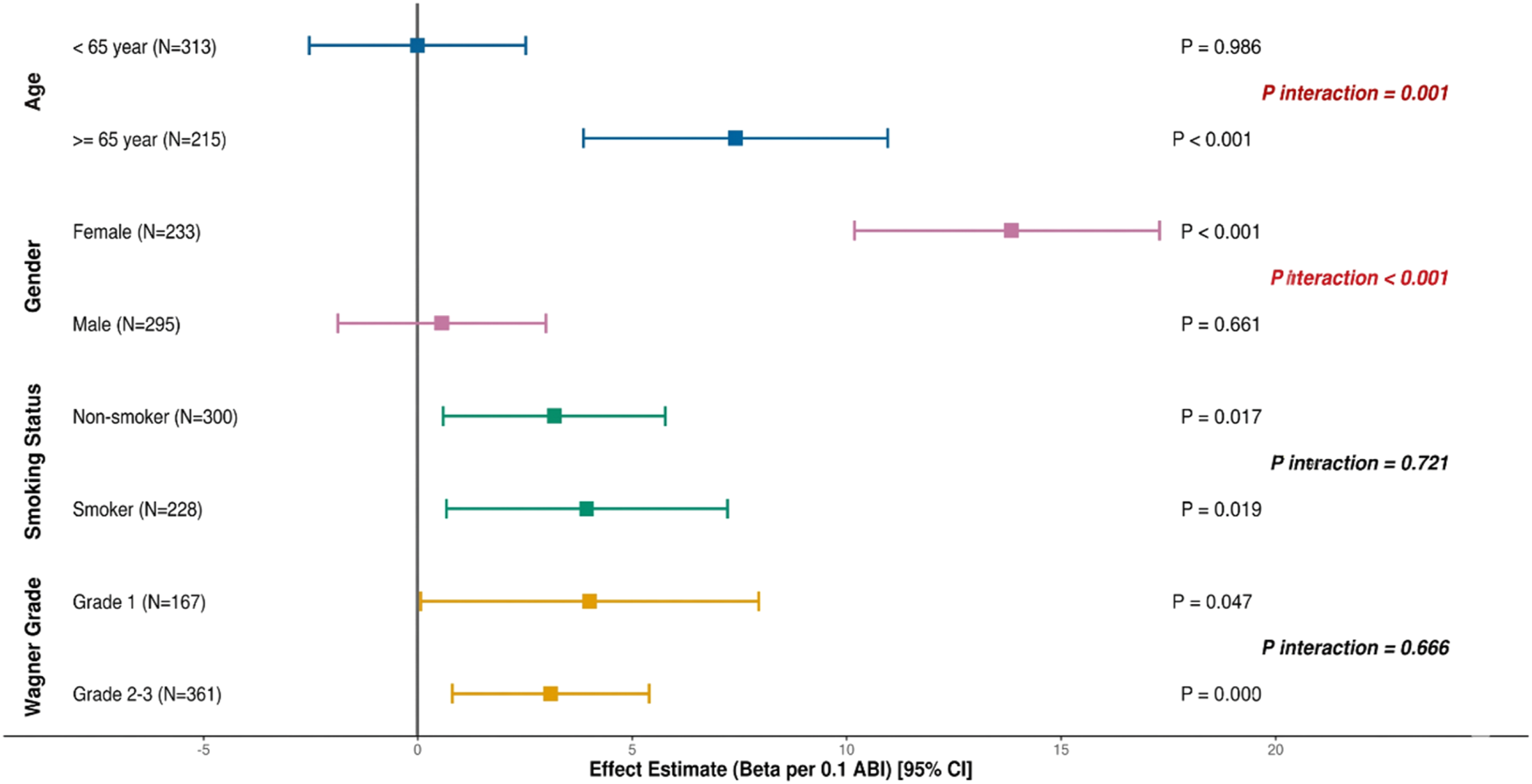
No significant interaction effects were detected for smoking status (p = 0.72) or Wagner grade (p = 0.67). The observed non-linear patterns and hemodynamic thresholds remained stable across varying levels of wound severity and tobacco exposure. This consistency demonstrates that the identified inflection points (0.62 and 0.90) function as robust structural benchmarks within the broader diabetic foot population, regardless of baseline clinical heterogeneity.
Robustness of Estimates Against Informative Censoring
The evaluation framework rigorously quantified the potential impact of participant attrition on the longitudinal outcome estimates. Of the 528 participants initially enrolled at Time Zero (T0), 54 individuals (10.2%) were lost to follow-up or withdrawn prior to the 20-week primary endpoint (Figure 1). To neutralize potential selection bias arising from non-random loss to follow-up, IPCW was integrated into the doubly robust analytical framework.
A comparative analysis demonstrated that the primary hemodynamic associations remained invariant to participant attrition. Specifically, the effect estimate for ABI in the IPCW-adjusted model (β = 2.48; 95% CI -1.31 to 6.27) was virtually identical to the estimates derived from a restricted complete-case analysis (β = 2.48; 95% CI -1.30 to 6.26; p = 0.20; Supplemental Table S2). This numerical stability across weighting specifications confirms that the observed relationships were not driven by informative censoring or selective attrition, further securing the internal consistency of the target trial emulation.
Discussion
This evaluation deconstructs the systemic misinterpretation of hemodynamic signals that often complicates risk stratification in diabetic foot management (Chuter et al., 2024). By implementing a target trial emulation framework, the analysis identified a significant inverted U-shaped relationship between the ABI and wound healing trajectories, effectively addressing the structural failure of traditional linear models to account for arterial non-compliance (Argyriou et al., 2024). These findings suggest that while the ABI remains a stable predictor for macro-vascular outcomes such as limb survival (Zhan et al., 2015), its prognostic fidelity for tissue repair diminishes as values exceed the physiological normal range. This divergence indicates that a categorical 0.90 threshold introduces a systematic misclassification of vascular risk in diabetic populations, as it lacks the discriminatory power to differentiate between intraluminal perfusion pressure and the confounding effects of medial arterial calcification (Brouwers et al., 2022).
A central observation from this structural modeling is the mechanistic decoupling of macro-circulatory maintenance from micro-circulatory metabolic demand (Jeffcoate et al., 2005). The results confirm that the ABI maintains linear validity as a predictor of major amputation (OR 0.77; p = 0.002), likely because preventing tissue necrosis requires only a minimal baseline of axial flow to sustain basal viability (Armstrong et al., 2020). In contrast, the 20-week PAR followed a non-linear trajectory that peaked at 27.9% before losing incremental fidelity and plateauing due to pseudo-normalization (Fitridge et al., 2024). This identifies a fundamental evaluative gap between macro-perfusion metrics and micro-metabolic outcomes, as wound closure is an energy-intensive process requiring functional capillary recruitment and endothelial responsiveness—physiological parameters that the ABI systematically fails to represent when readings are artificially inflated by medial arterial calcification (Chen et al., 2024). These protracted kinetics directly challenge the utility of traditional temporal evaluative benchmarks. Given that the maximum predicted PAR reached only 27.9% over an extended 20-week observation window, evaluating advanced neuroischemic lesions at a standard 12-week interval risks the premature classification of treatment failure. Clinical protocols require extended surveillance architectures to accurately capture the delayed metabolic responsiveness characteristic of this population.
The identified hemodynamic thresholds (0.62 and 0.90) provide objective benchmarks that define the structural boundaries of the therapeutic window in diabetic repair (Schaper et al., 2024). The primary ischemic phase (ABI <0.62) represents a critical perfusion deficit where healing is statistically improbable, as local oxygen delivery falls below the energetic threshold required for regenerative kinetics (Aboyans et al., 2012). Conversely, the blunted efficacy and subsequent decline observed at ABI >0.90 suggest a failure of the metric’s prognostic fidelity rather than a physiological reversal of benefit (Roshan et al., 2024). Our sensitivity analysis, which restored a positive linear association (β = 6.67; p = 0.038) after the targeted exclusion of non-compressible vessels (ABI ≥1.30), provides empirical support for the hypothesis that the loss of predictive value is primarily an artifact of extreme calcification (Salle et al., 2023). The categorical analysis further corroborates this ceiling effect; the statistical equivalence (p = 0.742) between the 0.62–0.90 and ≥0.90 strata proves that merely pushing the ABI into the “normal” range does not guarantee superior metabolic repair (Pan et al., 2025). Within the context of chronic hyperglycemia, a high-normal ABI may mask underlying microvascular dysfunction, inducing a systematic detection bias that may preclude timely revascularization for patients with occult ischemia (Pan et al., 2025).
The interaction between ABI and tissue repair was further modified by age and sex (p for interaction <0.001), with an amplified macro-perfusion dependence observed in participants aged ≥65 years and female cohorts (Wolf et al., 2024). In these demographics, tissue repair appears to exhibit a higher degree of intraluminal pressure dependence as a compensatory mechanism for age-related microvascular rarefaction and impaired capillary recruitment. These findings indicate that hemodynamic permissiveness is contingent upon the individual microvascular reserve (Bordage, 2009). From an evaluative perspective, reliance on a single, age-agnostic binary threshold constitutes a systematic misclassification of vascular risk, which risks overlooking critical ischemic signals in high-vulnerability patient groups (Cook & Artino, 2016).
Ultimately, these findings suggest a need to re-evaluate the diagnostic interpretation of the ABI, particularly in clinical scenarios where seemingly normal readings (0.90–1.30) coexist with stagnant wound healing trajectories. Given the observed loss of prognostic fidelity beyond the 0.90 threshold, a normal reading should not necessarily be interpreted as a definitive endpoint for vascular assessment in non-healing wounds. The potential for pseudonormalized pressures in this range indicates that clinical reliance on binary classifications may systematically delay further vascular investigation for patients with occult ischemia. To improve risk stratification, diagnostic protocols could benefit from a multi-modal approach that prioritizes non-pressure-dependent metrics, such as the Toe-Brachial Index or transcutaneous oxygen tension (Schuwirth & Van Der Vleuten, 2011), whenever wounds fail to progress despite an apparently adequate ABI. The clinical rationale for prioritizing the TBI in this context is grounded in its relative immunity to the calcification artifact that undermines ABI fidelity. Digital vessels are anatomically distinct from tibial and peroneal vessels in their susceptibility to medial arterial stiffening, meaning that toe pressures can reflect functional perfusion capacity even when ankle pressures are spuriously elevated. A TBI below 0.70, or an absolute toe pressure below 30 mmHg, has been proposed as a more reliable threshold for identifying critical ischemia in diabetic patients with suspected pseudonormalization. The inability to provide this correlation within the current dataset is acknowledged as a boundary condition, and it underscores the need for prospective studies that collect both ABI and TBI simultaneously to formally quantify the diagnostic gap that this evaluation has identified structurally.
A clinically operational question that arises directly from these structural findings concerns the hemodynamic threshold at which revascularization should be considered to optimize wound healing outcomes. The present data suggest that the ischemic inflection point of ABI 0.62 constitutes a physiologically meaningful decision boundary. Below this threshold, predicted PAR values entered negative territory, reflecting a perfusion state insufficient to sustain basal regenerative kinetics regardless of local wound management quality. This pattern is mechanistically consistent with a perfusion floor below which capillary recruitment and transcutaneous oxygen delivery to the wound bed are structurally inadequate. On the basis of these observations, patients presenting with an ABI below 0.62 alongside a non-healing wound trajectory should prompt expedited vascular surgery referral for revascularization consideration, rather than continued conservative management in isolation. Equally important, however, is the diagnostic challenge posed by the pseudo-normal range. Among participants with ABI values between 0.90 and 1.30, the metric’s prognostic fidelity was demonstrably compromised by medial arterial calcification, meaning that a seemingly adequate hemodynamic reading does not preclude underlying microvascular insufficiency. In practical terms, the absence of measurable wound healing progression over three to four consecutive surveillance weeks despite an ABI within the conventional normal range should function as an independent clinical trigger for secondary vascular investigation, incorporating non-pressure-dependent modalities such as the Toe-Brachial Index or transcutaneous oxygen tension. Taken together, these findings support a dual-trigger framework for revascularization decision-making: one threshold anchored to absolute ABI magnitude, and a second anchored to functional wound healing trajectory over time, rather than reliance on any single static hemodynamic cutoff.
The identification of this evaluative gap necessitates a fundamental recalibration of multidisciplinary team workflows. Historically, clinical triage protocols have utilized a normal ABI as a definitive gatekeeper, inadvertently creating a diagnostic ceiling that stalls cross-specialty referrals (VanderWeele & Ding, 2017). Based on the structural findings of this target trial emulation, endocrinologists, vascular surgeons, and podiatrists may benefit from adopting a decoupled diagnostic pathway. For patients exhibiting stagnant tissue repair despite an ABI in the 0.90 to 1.30 range, clinical protocols should strongly consider an immediate secondary diagnostic reflex. This approach supports the direct integration of non-pressure-dependent audits, including the Toe-Brachial Index or transcutaneous oxygen tension. Such a systemic adjustment shifts the evaluative focus from isolated axial flow metrics to the broader metabolic-vascular continuum, ensuring that hemodynamic pseudo-normality does not administratively delay critical revascularization interventions (Gigerenzer & Gaissmaier, 2011).
This evaluative shift carries profound implications for health professional education and the structural design of clinical pathways. Standardized vascular curricula predominantly emphasize the interpretation of binary hemodynamic thresholds while frequently neglecting the confounding effects of arterial non-compliance. Future medical education frameworks must integrate the concept of metric fidelity auditing. This pedagogical update will train clinicians to explicitly recognize the discordance between macro-circulatory signals and actual micro-metabolic demands. By embedding these non-linear hemodynamic principles directly into practice guidelines, healthcare organizations can structurally mitigate the diagnostic artifacts induced by medial arterial calcification. Ultimately, this evolution enhances the decision-making validity of the health professions by replacing a rigid metric-centric model with a framework governed by longitudinal tissue viability.
Limitation
This evaluation is subject to specific methodological boundary conditions. The emphasis on a dual-campus setting ensures high internal validity through standardized multidisciplinary care, yet it necessitates a cautious extrapolation of these thresholds to global cohorts with divergent metabolic archetypes. Hence, replicating this target trial emulation framework across diverse international healthcare infrastructures remains an essential future step to validate the broad applicability of these specific hemodynamic inflection points. Regarding the hemodynamic assessment, the absence of concurrent toe pressure measurements represents a recognized constraint of this evaluation. Toe-Brachial Index (TBI) data were not collected during the study period for two operational reasons. Handheld photoplethysmography equipment required for standardized digital pressure acquisition was not uniformly available across both clinical sites throughout the recruitment window, and the volume and acuity of the patient population made the addition of a second vascular measurement protocol at each enrollment visit operationally unfeasible within the existing MDT workflow. We acknowledge that this limitation is consequential. The TBI is substantially less susceptible to medial arterial calcification than the ABI, as digital vessels are typically spared from the calcification process that artificially elevates ankle pressure readings. In the pseudo-normal ABI range of 0.90 to 1.30, where the prognostic fidelity of the ABI collapses most severely in this cohort, concurrent TBI values would have provided a pressure-independent reference point to distinguish true perfusion adequacy from calcification-driven artifact. The absence of this reference constrains the granularity of the micro-perfusion characterization within that specific hemodynamic stratum. The sensitivity analysis excluding ABI ≥1.30 provides a partial structural substitute for this gap, but it cannot replicate the individual-level discriminatory capacity of a directly measured toe pressure. Integrating TBI alongside ABI at baseline is a clear priority for future iterations of this work.
Simultaneously, the observational design presents an inherent potential for residual confounding from unmeasured factors. Chief among these is offloading adherence during unsupervised daily activity, which, despite being documented at each scheduled surveillance visit, was not formally quantified at the patient level between visits, introducing a degree of unmeasured variability in the primary healing estimates. Furthermore, the methodological rigors of causal inference introduced specific statistical trade-offs. We acknowledge that the implementation of Generalized Propensity Score weighting resulted in a reduction of the effective sample size (ESS) to 217.1. This attrition of statistical information is an expected consequence of achieving strict structural covariate balance across a continuous exposure spectrum in a highly heterogeneous clinical population. To mitigate potential instability, weights were strictly truncated at the 1st and 99th percentiles. These constraints are ultimately contextualized by the E-value point estimates (1.87 for amputation; 1.66 for PAR), which suggest that substantial unmeasured confounding would be required to negate the observed effects. An additional boundary condition involves the explicit focus on proximal physiological confounders, which precluded the formal assessment of effect measure modification across different racial or ethnic strata. Understanding how socio-cultural determinants interact with medial arterial calcification burden remains a distinct evaluative target, necessitating future prospective registries designed to capture comprehensive demographic gradients alongside metabolic metrics. Finally, our protocol restricted hemodynamic evaluation strictly to the ipsilateral limb of the index ulcer. While this maintained focus on the primary target lesion, exploring the contralateral hemodynamic profile in patients with bilateral presentations represents a compelling avenue for future investigation to better characterize systemic microvascular reserve. Consequently, the identified hemodynamic inflection points and structural conclusions remain highly reliable within the target trial emulation framework. The occurrence of unscheduled revascularization events in 23 participants during follow-up, while managed through composite failure adjudication and IPCW correction, represents an additional boundary condition. Although these cases were systematically handled to prevent outcome contamination, the absence of a dedicated post-revascularization subgroup analysis limits the granularity with which perfusion recovery trajectories can be characterized in this cohort.
Conclusions
This structural evaluation demonstrates that the ABI functions as a divergent prognostic metric in diabetic foot management, maintaining linear validity for limb survival while exhibiting a significant inverted U-shaped relationship with tissue repair. Healing efficacy reaches a structural peak at an ABI of approximately 0.90 (Predicted PAR: 27.9%), beyond which the prognostic fidelity of the metric is systematically compromised by medial arterial calcification rather than a true physiological loss of perfusion benefit. These findings suggest that the clinical interpretation of the ABI should transition from binary thresholds toward a continuous hemodynamic profiling approach, recognizing that a seemingly normal reading in a stagnant wound often represents a state of “pseudo-normality” masking occult ischemia. Ultimately, decoupling the diagnostic strategies for limb salvage from those for wound healing is essential to ensure that microcirculatory failure is not overlooked due to calcification-driven artifacts, thereby aligning clinical practice with the evolving global standards for precision diabetic care (Armstrong et al., 2023).
Supplemental Material
Supplemental material - Evaluating the Diagnostic Validity of the Ankle-Brachial Index in Diabetic Populations: A Methodological Deconstruction of Pseudo-normality and Its Impact on Health Professional Decision-Making Using a Target Trial Emulation Framework
Supplemental material for Evaluating the Diagnostic Validity of the Ankle-Brachial Index in Diabetic Populations: A Methodological Deconstruction of Pseudo-normality and Its Impact on Health Professional Decision-Making Using a Target Trial Emulation Framework by Aiden Yi-Fei Wang, Xiu-Wen Ling, Amber Haseeb, Atiqah Aziz, Han Ling Tan and Terry Hao-Yu Qin in Evaluation & the Health Professions
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to the clinicians, nursing staff, and administrative personnel of the Department of Orthopaedic Surgery, Faculty of Medicine, Universiti Malaya, for their invaluable support throughout this study. We extend our special thanks to the teams at the University of Malaya Medical Centre (UMMC) and the University Malaya Specialist Centre (UMSC) for providing the clinical infrastructure and professional assistance essential for the successful completion of this dual-campus research.
Ethical Considerations
This study was conducted in strict adherence to the ethical principles outlined in the Declaration of Helsinki. Ethical oversight was managed independently for each of the two participating clinical sites. Formal approval for the UMMC was granted by its Medical Research Ethics Committee (MREC Ref: 20241023-14342). Concurrently, ethical approval for the UMSC was overseen and granted by its respective institutional board (MREC Ref: 2025113-14583). Written informed consent was obtained from all participants prior to their enrollment in the study.
Author Contributions
Conceptualization: T.H.Y.Q. and A.Y.F.W.; Methodology: A.Y.F.W., T.H.Y.Q., and A.A.; Software: A.Y.F.W.; Validation: X.W.L., A.H., and A.A.; Formal Analysis: A.Y.F.W.; Investigation: T.H.Y.Q., X.W.L., A.H., and A.A.; Resources: T.H.L. and A.A.; Data Curation: T.H.Y.Q. and X.W.L.; Writing – Original Draft Preparation: A.Y.F.W. and T.H.Y.Q.; Writing – Review & Editing: All authors; Visualization: A.Y.F.W.; Supervision: T.H.L. and T.H.Y.Q.; Project Administration: T.H.Y.Q. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Universiti Malaya Bantuan Khas Penyelidikan - Early Career Research Grant (BKP-ECRG, Project No. BKP031-2025-ECRG) and the Universiti Malaya Specialist Centre C.A.R.E. Fund Research Grant (UMSC-RG, Project No. UMG004C-2025).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to patient privacy and ethical restrictions but are available from the corresponding author on reasonable request.
AI-assisted Technology Statement
During the preparation of this manuscript, the authors used ChatGPT (OpenAI) in order to refine the academic language, improve the readability of the discussion, and ensure the logical consistency of the structural modeling framework. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.