
Abstract
A sense of filial responsibility, particularly where it is a strong cultural norm, may be beneficial for caregiver self-rated health and well-being. The purpose of this study was to examine associations between filial responsibility attitudes and both self-rated health and well-being within three cultural groups: Caucasian Canadian (n = 100), Chinese Canadian (n = 90), and Hong Kong Chinese (n = 125). Respondents were interviewed in person using a structured questionnaire. Multivariate analyses for the entire sample indicated associations between filial responsibility attitudes and both self-rated health status and overall well-being. Analyses performed within each cultural subgroup indicated that filial responsibility is associated with worse self-rated health in the Caucasian Canadian group. The results suggest caution in assuming that filial responsibility attitudes will be beneficial for caregiver outcomes; there may also be cultural variation.
Keywords
Adult children often feel responsible for and provide considerable support to their aging parents, yet providing care can have negative impacts on well-being. Although there has been some examination of the links between filial responsibility attitudes and care behaviors, the role of these attitudes in the subjective appraisal and experience of caregiving, and potential contribution to caregiver outcomes, receives less attention. Additionally, filial responsibility might be protective or harmful for caregiver well-being in differing cultural contexts. To examine these issues in further depth, the purpose of this study was to examine associations between attitudes of filial responsibility and both well-being and self-rated health among filial caregivers from three cultural groups: Caucasian Canadian, Chinese Canadian, and Hong Kong Chinese.
Description of the Problem
Filial caregivers often report both positive and negative aspects of their role, though in this regard, the meanings and appraisals of caregiving may be more important than the objective amount or level of care provided (Motenko, 1989). Indeed, some caregivers may actively engage with positive interpretations of meaning in order to cope (Hudson, 2004; Strang & Koop, 2003). The importance of meanings and subjective appraisals is perhaps most explicitly acknowledged in theoretical models of caregiver stress and coping (DeLongis, Coyne, Dakof, Folkman, & Lazarus, 1982; Lazarus & Folkman, 1984) often used in gerontological research.
Familialism and related expectations for family caregiving represent cultural values that can mitigate caregiver stressors, influence caregiving appraisals, and positively affect psychological well-being (Aranda & Knight, 1997; Martin, 2000; Tang, Li, & Liao, 2007; Youn, Knight, Jeong, & Benton, 1999). Familial expectations are believed to be more strongly and consistently internalized within specific cultural identities. For instance, members of ethnic minorities or non-Western cultural groups may have a high sense of filial responsibility, perceive family assistance as a more “normal” part of their life course (Cain, MacLean, & Sellick, 2004; Houldin, 2007; Skilbeck et al., 2005), and ascribe greater value and lower burden to care work (Marks, Lambert, Jun, & Song, 2007; Martin, 2000). Conversely, where care is unexpected (i.e., not normatively prescribed), caregivers may face barriers to satisfaction (Braudy Harris & Orpett Long, 1999; Kirsi, Hervonen, & Jylha, 2000). Such aspects may in part explain group differences in caregiver outcomes.
In contrast, however, where caregiving is expected or normatively prescribed, this might limit the ability to derive satisfaction (Calasanti & Slevin, 2001; McGrew, 1998; Rose & Bruce, 1995; Zhan, 2006), with high filial responsibility beliefs (i.e., those indicating obligation) facilitating guilt and feelings of inadequacy, exacerbating stress and burden (Cicirelli, 1993; Lyonette & Yardley, 2003; Selig, Tomlinson, & Hickey, 1991). This may be especially so when structural constraints make it difficult to meet ideals of filial responsibility. Individuals immersed within individualistic cultural contexts may interpret family relationships as ideally involving greater choice (Beck & Beck-Gernsheim, 2001; Fine, 2005) and responsibility as negative, even burdensome, even though these caregivers may be providing high levels of assistance. It is unclear, however, whether and how interpretations of the meaning of caregiving operate in ethnocultural groups of Western European or Caucasian American descent, and little research connects responsibility beliefs with well-being outcomes in these groups.
Because the symbolic meanings of care can differ between cultures, higher filial responsibility could buffer well-being in particular cultural groups of caregivers but not others. Moral obligations of filial responsibility (e.g., filial piety) are an important part of identity in many traditional Asian cultures (Holroyd & Mackenzie, 1995) and may provide a sense of role fulfillment, pride and self-worth (Wallhagen & Yamamoto-Mitani, 2006). For example, Korean and Vietnamese young adults in a study by Pyke (2000), when discussing plans for future care for their parents, applied favorable images of close family ties associated with Asian immigrants, in contrast to the unfilial behavior of the “normal American family.” Pyke suggested that filial responsibility promotes ethnic pride and affirmation through comparisons with other groups. In another study (Lee & Sung, 1998), high filial responsibility was associated with lower burden among Korean, but not American, caregivers.
However, there are contrasting results, with studies of Asian caregivers reporting, for example, no association between perceptions of caregiving meaning or reward and depression (Tang et al., 2007) or between familialism and caregiver burden (Youn et al., 1999). Others have reported a negative impact of normative fulfillment on quality of life (Yamamoto-Mitani et al., 2004) and of high filial responsibility attitudes on depression (Zhan, 2006). In two Asian American cross-cultural studies (Kim & Lee, 2003; Patterson et al., 1998), caregiving had similar negative impacts on caregiver health, despite cultural differences in filial piety.
Research specifically with diasporic, immigrant, and/or ethnic minority samples suggests that filial responsibility attitudes can generate satisfaction and reward (Jolicoeur & Madden, 2002; Lai, 2010), enhancing caregiver coping and role acceptance (Ho, Friedland, Rappolt, & Noh, 2003; Spitzer, Neufeld, Harrison, Hughes, & Stewart, 2003) and mitigating burden in these groups (Lai, 2007; Losada et al., 2006). More broadly, filial responsibility norms in these communities may bolster identity boundaries and ethnic pride (Pyke, 2000; Spitzer et al., 2003). Again, however, there are conflicting findings. The cultural value accorded to caregiving may ultimately harm well-being where caregivers struggle to fulfill high cultural expectations with diminished resources. In one study (Jolicoeur & Madden, 2002), Mexican American caregivers experienced greater stress, burden, and dissatisfaction, despite clearly fulfilling role obligations.
Finally, it is also possible that the assumed importance of filial responsibility attitudes, as distinguishing between cultural groups, may be more myth than reality; cultural interpretations of filial piety may be adapting over time in response to changing structural contexts (Ng, Phillips, & Lee, 2002; Sorensen & Kim, 2004; Wong & Chau, 2006). Furthermore, although filial responsibility may not be as strongly prescribed within North American culture, it may be ideologically prescribed (increasingly so, given cutbacks to formal services). The importance of the cultural expectedness of care provision (as reflected in filial responsibility) may also be overstated; for instance, structural constraints on caregiving experiences and hours of care may have more important impacts.
To address these issues, the purpose of the present study was to examine whether attitudinal support for filial responsibility might be protective or harmful for the well-being of caregivers in differing cultural contexts. Is filial responsibility associated with well-being and perceived health, controlling for other variables? Do differences exist in this regard between Caucasian Canadian, Chinese Canadian, and Hong Kong Chinese samples?
Methods
Face-to-face survey interviews were conducted from 2007 to 2008 in Hong Kong and Canada (Vancouver and Victoria). Eligible respondents provided care or support (defined broadly) for at least 3 hours a week to a parent older than 60 years of age who was accessible by car. The Hong Kong sample was selected from an existing random sample of noninstitutionalized older adults aged 60 and older (from the General Household Survey in Hong Kong). Respondents who reported being cared for by family members were included in the sampling frame for the present study, and caregivers who were adult children were approached for participation. The Caucasian and Chinese Canadian samples were recruited through advertising in local newspapers and newsletters, announcements at caregiver groups and Chinese Canadian association meetings, and word of mouth. A brief telephone screening interview confirmed eligibility. Caucasian was defined as White or light skinned and ancestrally from one of the following ethnic groups: Canadian, French Canadian, English/Welsh/Irish/Scottish, American, Norwegian, Danish, Swedish, Icelandic, French, German, Dutch/Belgian, or Eastern European. Chinese Canadians had to self-identify as Chinese and, to promote comparability with the Hong Kong sample, to have parents from Hong Kong or descended from Hong Kong people.
The research was approved by institutional review boards at the participating universities. Core measures were validated in English and Chinese; the interview schedule was translated into and back translated from Cantonese. Interviews lasted an average of 1.5 hours and were conducted in English with Caucasian Canadian respondents, in Cantonese with Hong Kong respondents, and in the preferred language with Chinese Canadian respondents.
As the dependent variable, the Personal Wellbeing Index (Lau, Cummins, & McPherson, 2005) is a seven-question measure of well-being developed for cross-cultural measurement. Respondents were asked how satisfied they felt in various life domains, such as health, relationships and standard of living, with 10 response categories ranging from 1 (extremely dissatisfied) to 10 (extremely satisfied). Responses are summed for all questions and coded continuously, with higher scores representing better well-being (α = .87). A single-item measure of self-rated perceived health asked, “For your age, would you say, in general, that you health is excellent, good, fair, poor, or bad for your age?” To address a skewed frequency distribution, the original 5 response options were dichotomized into better (coded 1) and worse (coded 0) perceived health.
Following Marks et al. (2008), we conceptualize filial responsibility attitudes as a potential index of “the meaning of caregiving activities” (p. 3620). The Filial Expectancy Scale (Kim & Lee, 2003; Lee & Sung, 1997) is extensively used and tested in both North American and Asian samples, with acceptable internal consistency (α = .76). Adapted for this study, it consists of five items: “Children should live close to their parents; want a house with enough room for their parents to feel free to move in; be willing to take care of their parents in whatever way necessary when they are sick; be willing to give their parents financial help, if they need it”; and “If children live nearby after they grow up, they should visit their parents at least once a week.” Response options ranged on a Likert-type scale from 1 (strongly disagree) to 5 (strongly agree), with an undecided (3) category. Higher scores indicate higher filial responsibility. A measure of filial piety (Liu, Ng, Weatherall & Loong, 2000) was also included to ensure comprehensive measurement. Six items included “When it comes to elderly parents, adult Canadians have the obligation to look after them; to assist them financially, if needed; to respect them; to take their direction; to please them and make them happy; and to retain contact with them.” Response options ranged from 1 (do not agree at all) to 5 (completely agree), with an undecided (3) option (α = .80). Higher scores indicated higher filial piety.
Cultural group (Caucasian Canadian, Chinese Canadian, or Hong Kong Chinese) was constructed as a dummy variable, with the Chinese Canadian group as the reference category.
Two domains of caregiver burden were also included as independent variables, components of the Multidimensional Caregiver Burden Inventory (Novak & Guest, 1989) and validated in Chinese (Chou, Lin, & Chu, 2002). This included the six-item time dependence dimension of caregiver burden (α = .85), representing burdens related to perceived time restrictions. The five-item social dimension of caregiver burden (α = .75) measured perceived role conflict (e.g., feeling resentful of other relatives). Likert-type response scales ranged from 1 (not at all) to 4 (very much so); higher scores were equated with greater perceived burden.
Control variables were selected on the basis of those commonly included in empirical research into caregiver burden and well-being, such as caregiver and care recipient characteristics and contextual features of care (e.g., relationship quality, amount of assistance provided). Caregiving behaviors were assessed with a summed index representing assistance with basic and instrumental activities of daily living (ADLs). Respondents were asked whether they helped with ADLs or instrumental ADLs (IADLs), from a list of 13 responses for each activity representing no (coded 0) and yes (coded 1). These responses were summed for all 13 items; higher scores indicated help with a greater range of tasks.
Data were collected on sociodemographic variables, including caregiver gender (1 = male, 0 = female), caregiver age (continuous), and annual household income (13 categories; missing values replaced with cultural group means). Single items measured self-reported care recipient health (five categories; higher scores indicated worse reported care recipient health) and memory (five categories; higher scores equated with worse reported memory). Finally, relationship quality was measured by summing three items (Lee & Sung, 1997), such as “How enjoyable is the time you and your parent spend together on a scale from ‘not at all’ (1) to ‘very greatly’ (5)?” Higher scores indicate better relationship (α = .78).
Multiple regression analyses were performed using SPSS Version 18.0 to examine associations between dependent (well-being and self-rated health) variables, filial responsibility attitudes, burden, and cultural group (a dummy variable) as independent variables; IADL or ADL assistance, sociodemographic characteristics, and relationship quality were included as control variables. Given the emergence of cultural group as a strong predictor in the multivariate analyses with the entire group, subsequent analyses were performed separately within each of the three cultural groups. Ordinary least squares regressions were used for well-being and binary logistic regressions for self-rated health. Standardized estimates for the latter were generated using calculated Z scores for the independent variables. Data were checked for multicollinearity, linearity, and homoscedasticity before commencing analyses. Multicollinearity between filial expectancy and filial piety was disconfirmed. The cutoff for determining statistical significance was p < .05.
Results
In total, 315 respondents were interviewed: 100 Caucasian Canadians (31.7%), 90 Chinese Canadians (28.6%), and 125 Hong Kong Chinese (39.7%). Respondent characteristics are summarized in Table 1 (with breakdown by cultural group). Data not included in Table 1 indicate that 67% of respondents had children of their own, 64.8% were married or partnered, 84.1% were high school graduates, and 71.4% worked in paid employment. A total of 59.6% of participants were daughters caring for mothers, 14.4% were daughters caring for fathers, 16.0% were sons caring for mothers, and 9.9% were sons caring for fathers. As such, 75.6% of the care recipients were female and 24.4% were male. Of the care recipients, 39.5% were married or living in common-law arrangements, 55.4% were widowed, and 5.1% were divorced.
Variable Frequencies, Means, and Standard Deviations
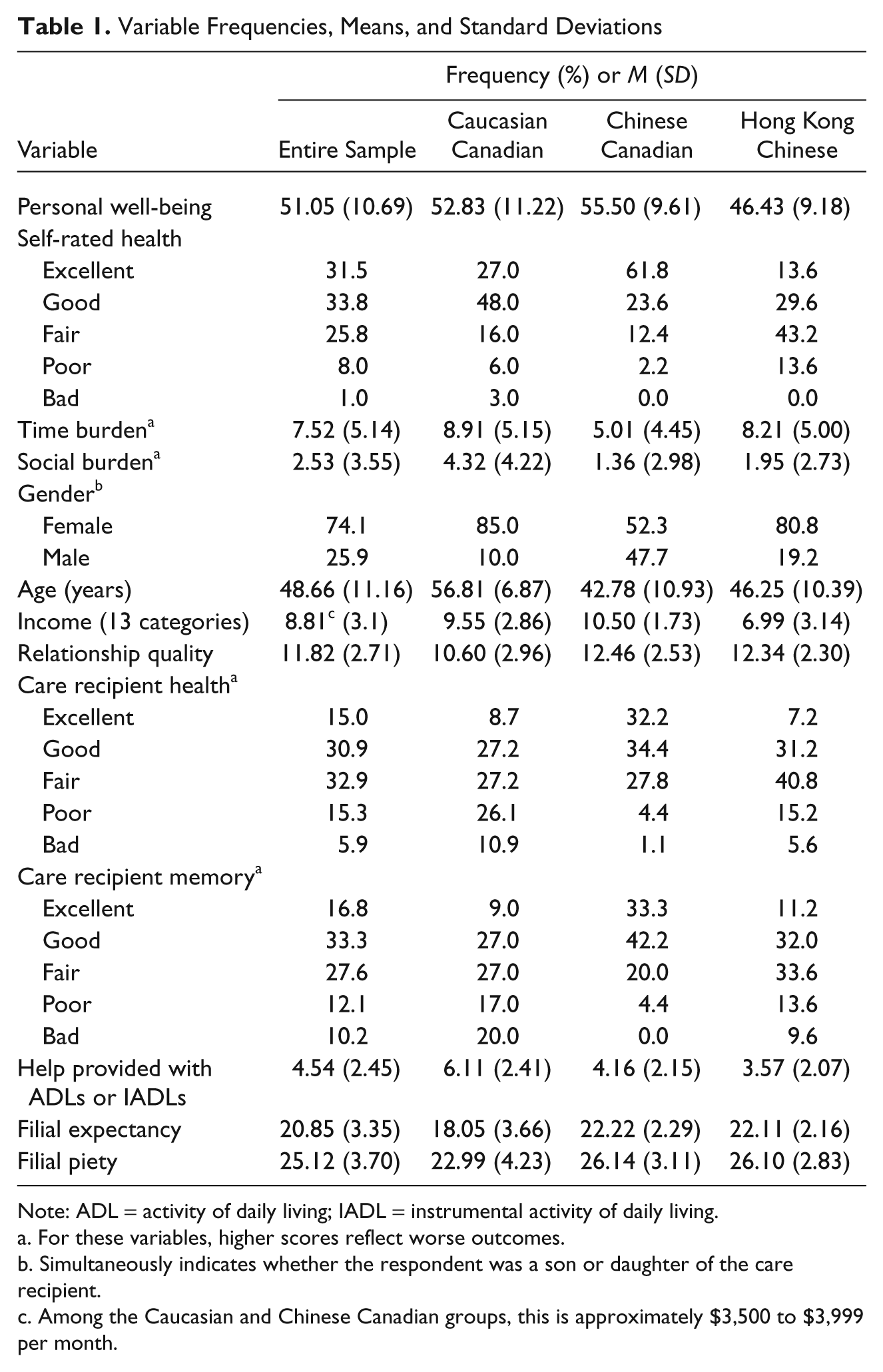
Note: ADL = activity of daily living; IADL = instrumental activity of daily living.
For these variables, higher scores reflect worse outcomes.
Simultaneously indicates whether the respondent was a son or daughter of the care recipient.
Among the Caucasian and Chinese Canadian groups, this is approximately $3,500 to $3,999 per month.
Just under half of participants (46.7%) reported being the primary caregiver. Approximately 34.6% coresided with their parent; those who did not coreside lived on average half an hour away from their parents. For each ADL and IADL, respondents were asked the average number of minutes it took them to help parents with that task each time. This equates to a group average of 225.55 minutes across all tasks. For each task, respondents were also asked how many times a week they performed that task on average. Considering all tasks together produces a group average of 8.60 times per week.
Dependent Variable: Self-Rated Health Status
Entire sample
A binary logistic regression was conducted on self-rated health for the entire sample (Table 2; statistically significant findings are highlighted in boldface type). The full model explains 31% of the variance in perceived health (Nagelkerke’s R2). Standardized β estimates are included in the text to compare the relative importance of independent variables. In logistic regression analysis, standardized estimates are produced using Z scores. Unstandardized estimates (B) are also presented in tables.
Results of Binary Logistic Regressions on Self-Rated Health
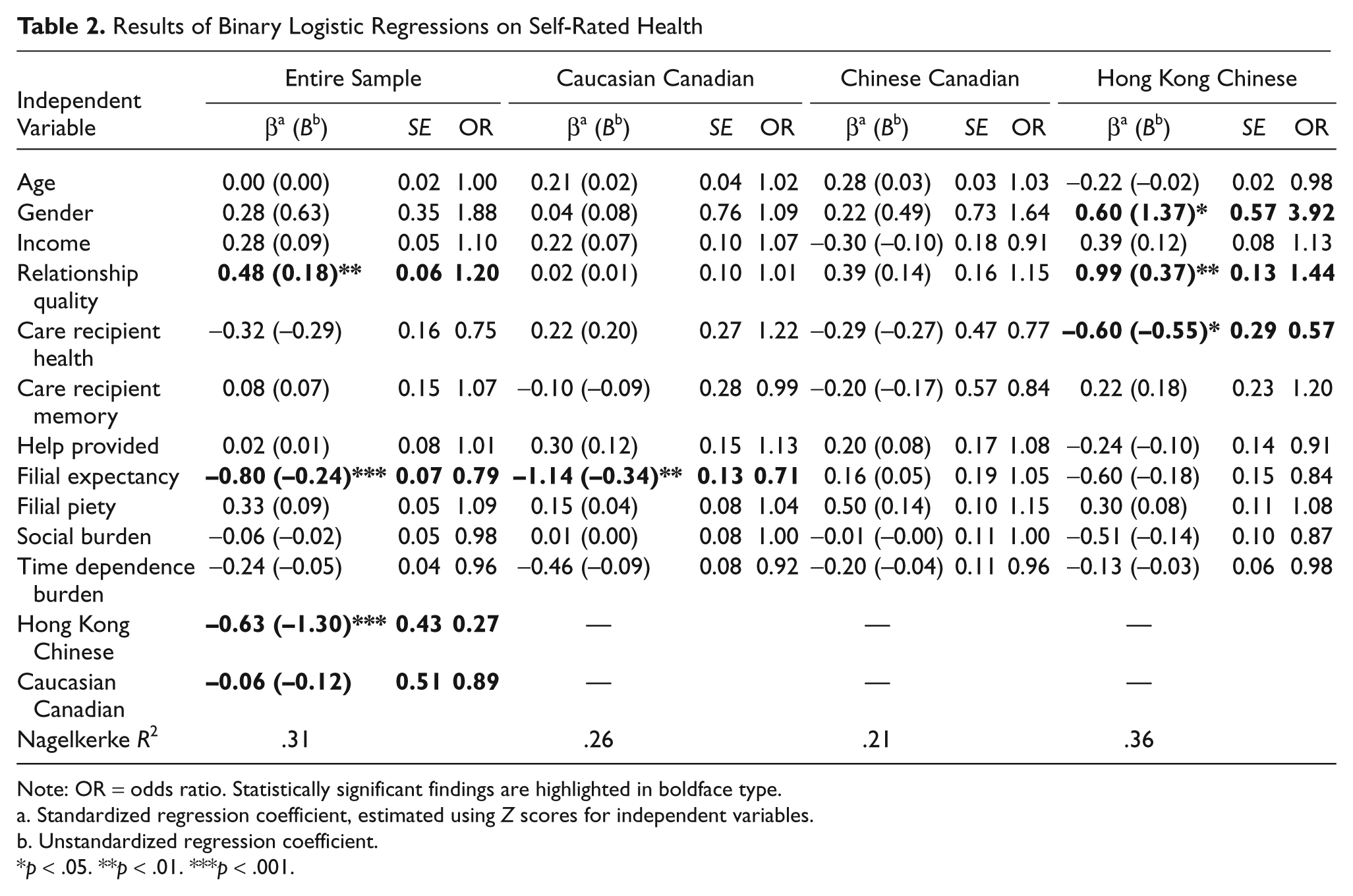
Note: OR = odds ratio. Statistically significant findings are highlighted in boldface type.
Standardized regression coefficient, estimated using Z scores for independent variables.
Unstandardized regression coefficient.
p < .05. **p < .01. ***p < .001.
The variable representing the Hong Kong Chinese cultural group was significant; specifically, the Hong Kong Chinese respondents tended to report poorer self-rated health compared with the Chinese Canadian respondents (odds ratio = 0.27, β = −0.63, p < .001). In addition, the measure of filial expectancy (but not piety) was associated with perceived health: stronger filial expectancy was associated with worse perceived health (odds ratio = 0.79, β = −0.80, p < .001). The only other statistically significant predictor of perceived health was relationship quality (odds ratio = 1.20, β = 0.48, p < .01): better relationship quality was associated with better self-rated health.
Cultural subgroups
Table 2 also presents the results for the regressions on self-rated health within each subsample. Overall, among Caucasian Canadian caregivers, only filial expectancy (β = −1.14, p < .01) is associated with self-rated health status. Greater support for filial responsibility in this group is associated with lower reported self-perceived health. Although not statistically significant, it is noteworthy that in the Chinese Canadian group, the direction of the association is reversed. In this group, however, none of the associations between independent or control variables and self-rated health reached statistical significance. Within the Hong Kong Chinese subgroup of caregivers, male gender (β = 0.60, p < .05), better perceived relationship quality (β = 0.99, p < .01), and worse perceived care recipient health (β = −0.60, p < .01) are associated with better self-rated health.
Dependent Variable: Well-Being
Entire sample
An ordinary least squares regression was conducted using well-being as the dependent variable (Table 3), for which the full model explains 38% of variance. The variable representing the Hong Kong Chinese cultural group is again significant, indicating that Hong Kong Chinese respondents tend to report poorer well-being compared with Chinese Canadian respondents (β = −0.29, p < .001). In addition, an association at p = .05 is noted for filial piety (β = 0.12). Stronger attitudinal support for filial piety is associated with higher well-being, and better perceived care recipient health is associated with higher well-being. Additionally, lower perceived social burden predicts better well-being (β = −0.17, p < .01), as does better perceived relationship quality (β = 0.28, p < .001), better perceived care recipient health (β = −0.11, p < .05), higher income (β = 0.22, p < .001), and older age (β = 0.20, p < .001).
Results of Ordinary Least Squares Regression on Well-Being
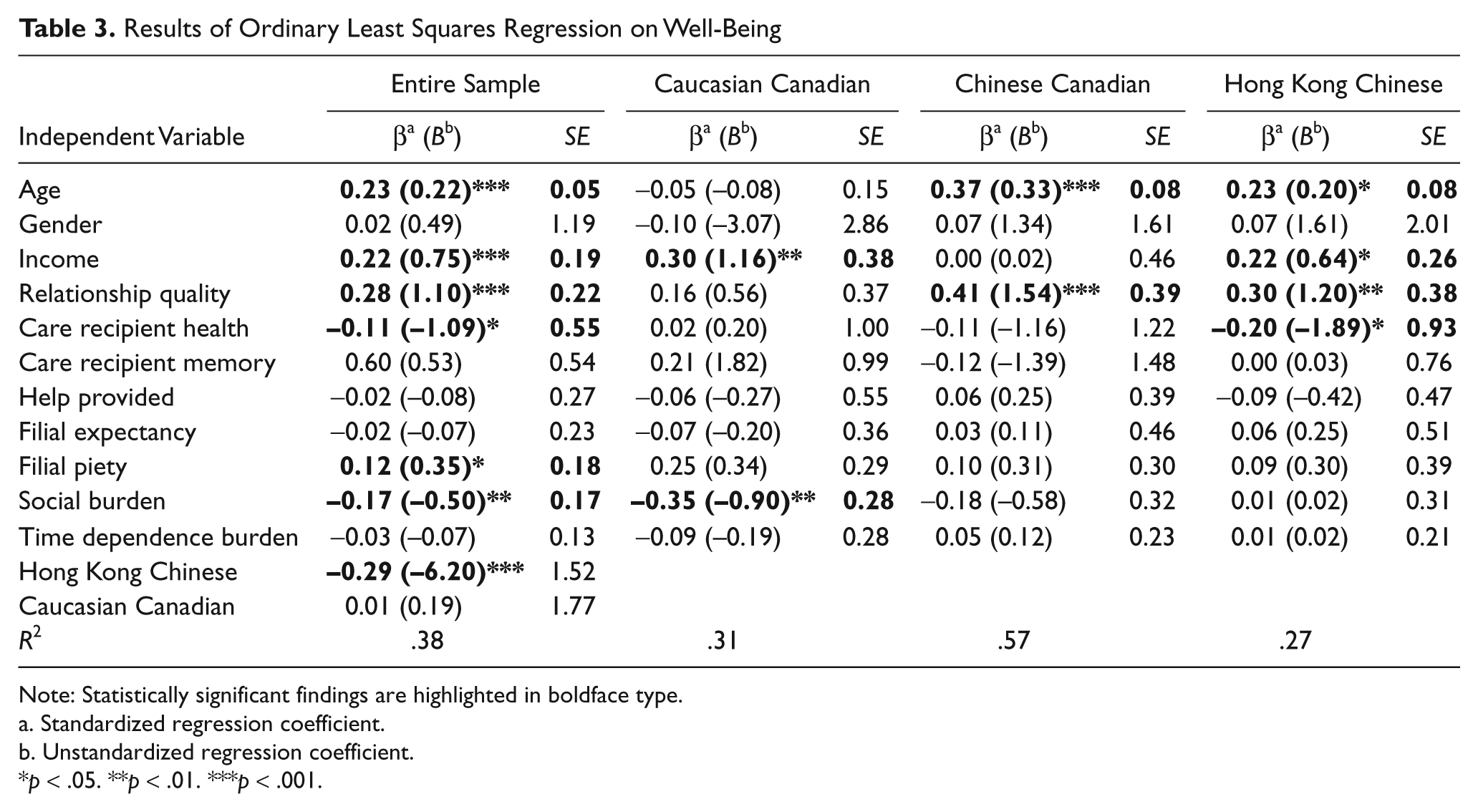
Note: Statistically significant findings are highlighted in boldface type.
Standardized regression coefficient.
Unstandardized regression coefficient.
p < .05. **p < .01. ***p < .001.
Cultural subgroups
Table 3 also summarizes the results for the regressions on well-being, within each subsample model. Overall, higher income (β = 0.30, p < .01) and lower reported social caregiver burden (β = −0.35, p < .01) are associated with better well-being in the Caucasian Canadian group. Although not statistically significant, the direction of the association between filial expectancy and well-being differs from the directions for both the Chinese Canadian and Hong Kong Chinese groups. Older age (β = 0.37, p < .001) and better perceived relationship quality (β = 0.41, p < .001) are associated with well-being in the Chinese Canadian group. Finally, older age (β = 0.23, p < .05), higher income (β = 0.22, p < .05), better perceived relationship quality (β = 0.30, p < .01), and care recipient health (β = −0.20, p < .05) predicted well-being in the Hong Kong subsample of caregivers.
Discussion
Is attitudinal support for filial responsibility protective or harmful for the well-being of caregivers in differing cultural contexts? Associations between filial responsibility attitudes and the outcome measures of well-being and perceived health were examined in the overall sample and in separate subsample analyses. As with most research with family caregivers, this study had a relatively small sample size, particularly for the subsample analyses; statistically insignificant estimates may be due to weak power, and as such, the results should be interpreted as tentative. Additional limitations that call for caution in interpreting the findings include the absence of detailed information about care recipient characteristics such as income and subsample variations in caregiver gender (i.e., a relatively higher proportion of men in the Chinese Canadian subsample) and perceived health of the care recipient (i.e., a relatively higher proportion of Caucasian Canadian caregivers perceived their parents’ health to be poor or bad).
Results for the sample as a whole indicate the importance of cultural group for both caregiver self-rated health and well-being, suggesting the need for separate subgroup analyses to further explore cultural patterns. In addition, findings for the sample as a whole highlight the potential role of filial responsibility attitudes but raise additional questions. For instance, stronger filial expectancy was associated with worse self-rated health, but stronger filial piety was associated with higher perceived well-being.
Subsequent analyses run for each cultural group separately did not demonstrate strong associations between filial responsibility attitudes and self-rated health and well-being outcomes, though may have been limited by sample sizes. In particular, neither filial responsibility measure was associated with caregiver well-being or self-rated health at a statistically significant level in the Hong Kong or Chinese Canadian subsamples. The most notable finding from these analyses is that in the Caucasian Canadian group, lower filial expectancy was associated with better self-rated health. That filial responsibility attitudes in this group were associated with poorer self-rated health lends support to other research suggesting that high attitudes of filial obligation may be associated with negative subjective outcomes among caregivers (Cicirelli, 1993; Lyonette & Yardley, 2003; Selig et al., 1991); the exact mechanism is unknown, though feelings of guilt and inadequacy, as well as, in a Western sociohistorical and cultural context, the (negative) symbolic meanings and identity implications of perceived obligation in family relationships, may be important (Beck & Beck-Gernsheim, 2001; Fine, 2005; Funk, 2008). Although not statistically significant, the direction of the association was reversed in the Chinese Canadian group, suggesting the need for future research to explore whether attitudes of filial responsibility are protective for this group.
The well-being measure is a far broader one than self-rated health, encompassing multiple life domains, and attitudes of filial responsibility may have a negative impact on self-perceived health (a domain-specific measure) but more positive associations with other life domains (e.g., satisfaction with achievement in life, personal relationships, feeling part of a community), which may in part explain the positive associations between piety and well-being in the overall sample. Again, cultural differences may still exist, as piety is arguably a measure more specific to Asian cultures; however, we were unable to detect such cultural differences in our data set.
To a limited extent, the data highlight the importance of caregiver self-perceived social burden for well-being, though only in the Caucasian subgroup. However, associations with time dependence burden and both well-being and self-perceived health were not evident, lending support to Chappell and Reid (2002), who concluded that whereas burden and well-being are highly correlated, “burden is not a strong predictor of well-being” (p. 779). Caregivers’ individual coping responses, as well as social support from informal and formal sources, may potentially buffer harmful effects of burden on self-perceived health and well-being.
As with any cross-sectional study, the causal direction of the findings cannot be confirmed. Although it is plausible that high self-rated health might lead to higher filial piety because these caregivers perceive they are able to provide care, it is difficult to imagine that Caucasian Canadian caregivers who view their own health as poor would increase their personal support for filial responsibility, instead of lowering it.
Further research with larger samples of randomly selected caregivers that uses separate cultural subsample analyses is needed. Furthermore, more specific measures of caregiver outcomes, such as caregiving satisfaction, positive appraisal of caregiving, depression, and objective measures of health status, should be used.
Other as yet unknown differences between these cultural groups may help explain the findings. In addition, there may be some sample variations. For instance, the proportion of respondents indicating that they were the ones who provided the most care to their parents ranged from 64.6% in the Caucasian Canadian group, to 48.8% in the Hong Kong Chinese group, to 24.7% in the Chinese Canadian group. Further research should explore how primary or secondary caregivers might differentially experience both filial responsibility and caregiver outcomes.
Future research could also examine the congruence or dissonance between attitudes and behaviors and whether and how might this be associated with caregiver outcomes. A caregiver with a high sense of responsibility but an inability to provide extensive task assistance may suffer from feelings of guilt that are harmful for well-being. Conversely, lower filial obligation among those providing high levels of care may result in stress and health declines (Marks et al., 2008) because of discrepancies between the role and beliefs.
Conclusions
The findings of this study suggest there are some associations between filial responsibility and both well-being and perceived health, when controlling for other variables. Although the findings must be viewed tentatively because of the small subsample sizes, we suggest that there may be important cultural differences and complexities. In particular, a high sense of filial responsibility may have more negative impacts for caregivers of Caucasian Canadian backgrounds. We propose that in a Western cultural context, feelings of responsibility for family members can be associated with feelings of guilt or inadequacy for some caregivers, as well as restrictions on personal and parental autonomy and independence that run counter to dominant Western ideals. As such, practitioners who work with family caregivers must be cautious not to universally promote filial responsibility as a moral imperative. However, there is also possibility for positive effects of high filial responsibility on caregiver outcomes, possibly for those from different cultural contexts or in terms of impacts on satisfaction with a variety of life domains that contribute to overall well-being. These effects remain to be further explored.
Footnotes
Acknowledgements
The assistance of Dr. Kee Lee Chou, Dr. David Lai, and Kileasa Wong with project design and data collection is gratefully acknowledged, as is the support of Linda Outcalt, Carren Dujela, and Nancy Davis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was funded by the Social Sciences and Humanities Research Council of Canada (Grant 410-2007-1791).