
Abstract
We concatenate 28 years of historical depressive symptoms data from a longitudinal cohort study of U.S. gay men who are now midlife and older (n = 312), with newly collected survey data to analyze trajectories of depressive symptomatology over time and their impact on associations between current stress and depressive symptoms. Symptoms are high over time, on average, and follow multiple trajectories. Aging-related stress, persistent life-course sexual minority stress, and increasing sexual minority stress are positively associated with depressive symptoms, net of symptom trajectories. Men who had experienced elevated and increasing trajectories of depressive symptoms are less susceptible to the damaging effects of aging-related stress than those who experienced a decrease in symptoms over time. Intervention efforts aimed at assisting gay men as they age should take into account life-course depressive symptom histories to appropriately contextualize the health effects of current social stressors.
Introduction
Current cohorts of U.S. midlife and older gay-identified men (hereafter, gay men) have traversed a historical period of tremendous personal bearing, which stems from two interrelated social phenomena. First, the AIDS epidemic had a profound impact on their lives that is difficult to overstate (Fredriksen-Goldsen & Muraco, 2010; LeBlanc, 2011; Rosenfeld, Bartlam, & Smith, 2012). In the early years, AIDS was seen as “the gay plague” (Shilts, 1987) and evoked negative societal responses because (a) it appeared to affect only gay men who already were highly stigmatized, (b) gay men were considered inherently dangerous because transmission routes were not well understood, (c) AIDS was physically disfiguring, and (d) those afflicted were held responsible for their condition. Gay men not infected with HIV were subject to “courtesy stigma” (Goffman, 1963). Many of these men are part of the “AIDS Generation” and came of age during the early stages of AIDS, whereas others were well into adulthood when AIDS began to decimate entire gay communities, especially in AIDS epicenters such as Los Angeles, New York City, and San Francisco where deaths numbered in the tens of thousands (Halkitis, 2014). These men survived the trauma of losing friends and partners to a ruthless disease, some survived being infected with HIV themselves, and all witnessed the transformation of AIDS from a near certain death sentence to a largely manageable chronic disease beginning in the mid-1990s. In various ways, AIDS is a defining aspect of their development across the adult life course.
Second, these gay men have traversed the life course within a social context that has undergone dramatic changes over the last 40 years, with laws and public policies emerging in many parts of the country to protect their civil rights. Until fairly recently, the view of homosexuality as a deviant and pathological perversion was entrenched in U.S. society. This pathologized view of homosexuality remained until 1973 when homosexuality per se was removed from the Diagnostic and Statistical Manual of Mental Disorders (Krajeski, 1996). This change came about as a result of emerging research on homosexuality and the increasing visibility of the gay rights movement in the 1960s (Institute of Medicine [IOM], 2011). The gay rights movement continued to gather momentum throughout the 1970s, only to be sidelined by the AIDS epidemic in the 1980s (Halkitis, 2014), and a resurgence as the AIDS case fatality rate declined. Thus, in a relatively short period of historical time, views on homosexuality have changed, although societal acceptance of sexual minorities is far from universal.
However, little is known about how the general mental health status of these gay men has evolved over this unprecedented period or how life-course stress associated with their sexual minority status affects their mental health. Such information is needed to tailor mental health-care programs designed to assist these men in their later years because their numbers are growing exponentially as part of the general aging of the American population. Existing intervention efforts would benefit by drawing upon life-course data, as recommended in a recent report by the IOM (2011). This exploratory study builds an understanding of how the past may influence the present among a cohort of gay men who are now midlife and older (i.e., born before 1965, the “baby boomer” generation and older) to begin to fill this research gap.
Aging often engenders stressful experiences that negatively affect mental health among all persons, such as financial strain, health-related hardships, caregiving burdens, social isolation, relocations, and bereavements (e.g., Alexopoulos, et al., 2002; Moos, Schutte, Brennan, & Moos, 2005; Pearlin & Skaff, 1996). However, such difficulties may be exacerbated for gay men in comparison with heterosexuals. For example, existing research has shown that, on average, midlife and older gay men are more likely than their heterosexual counterparts to live alone (Wallace, Cochran, Durazo, & Ford, 2011). Living alone subsequently makes them vulnerable to social isolation, which is associated with poor health (e.g., Fredriksen-Goldsen, 2011). Multiple HIV-related bereavements earlier in life may be additionally harmful to their mental health (Wight, LeBlanc, de Vries, & Detels, 2012). Indeed, emerging research suggests that midlife and older gay men may be disproportionately in poorer health than heterosexuals as measured by multiple indices (e.g., self-rated health, depression, disability, and tobacco use; de Vries, 2014). As with heterosexual populations, aging for gay men is not always a source of stress (Lyons, Pitts, & Grierson, 2013), but a growing body of empirical evidence suggests that they may be disproportionately vulnerable to the strains of getting older (IOM, 2011).
Notably, many midlife and older gay men continue to be challenged by stress associated with their sexual minority status or experience lagged effects of earlier life-course gay-related victimization (Emlet, Fredriksen-Goldsen, & Kim, 2013). “Sexual minority stress theory” (Meyer, 2003a, 2003b) builds on more general stress process theory (e.g., Pearlin, Schieman, Fazio, & Meersman, 2005) and posits that sexual minority populations have been exposed to unique stressors throughout their lives, including stigma, experiences of discrimination, internalized homophobia, and sexual identity concealment (Meyer, 1995). These types of stress contribute to physical and mental health disparities between sexual minority and nonsexual minority populations (IOM, 2011), disparities that are particularly prominent in the later years when multiple comorbidities begin to appear (Fredriksen-Goldsen, Kim, Barkan, Muraco, & Hoy-Ellis, 2013).
Conceptual Model
Our work is driven by a Life course, aging and sexual minority stress conceptual model (see Figure 1), in which background factors (e.g., educational attainment and employment) influence other aspects of the stress process including the occurrence of aging-related stress and sexual minority-related stress, which then impact depressive symptoms. Of particular importance to the model, as discussed below, is the moderating effect of depressive symptom trajectories on the relationship between stress and health. Our approach uses the life-course framework to integrate concepts from the general stress process model (Pearlin et al., 2005) and the minority stress model (Meyer, 2003a, 2003b). Key paradigmatic principles of the life course (e.g., stability and change in trajectories) are used to locate these stress processes within a specific historical time and to examine the intersection of that history with individual biography (Elder, Johnson, & Crosnoe, 2003; Pearlin et al., 2005). Although aging-related and sexual minority–related stress experiences envelop the entire gay population, we conceptualize that their significance to the emotional well-being of particular gay men is conditional upon their own depressive symptom trajectories.
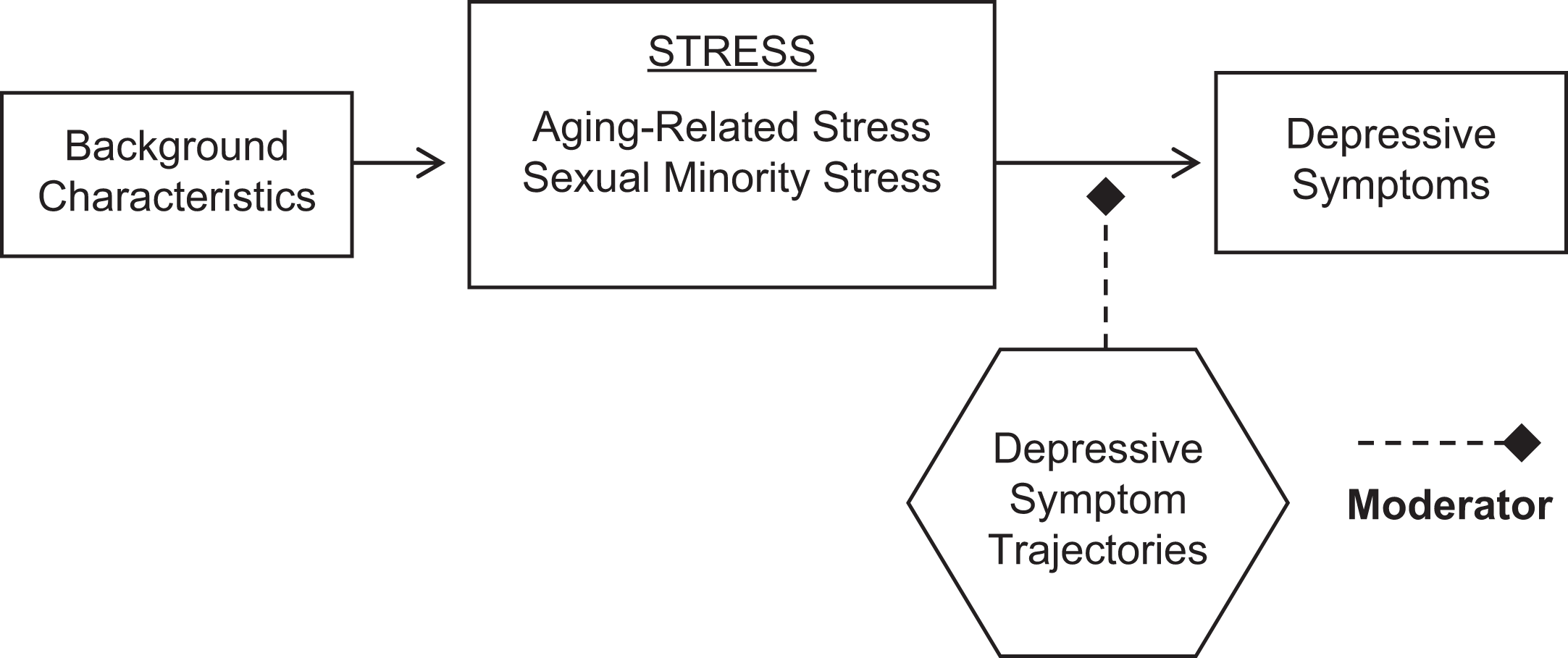
Life course, aging, and sexual minority stress model.
We contend that the past can be chronicled by examining how depressive symptom trajectories affect current associations between stress and psychological well-being. This approach is consistent with previous work documenting the modifying effect of clinical depression histories on contemporary stress and depression associations (Kessler, 1997). Depression histories may be related to current stress reactivity and condition the individual’s response to stress, independent of other traditionally delineated psychosocial factors, that is, stress bufferers (e.g., social support and coping strategies; Kessler, 1997). Consequently, if depression histories are not taken into consideration, the full effect of stress on current emotional well-being may be mischaracterized (Kessler, 1997).
This approach also is in line with the “kindling hypothesis” (Post, 1992) or the premise that persons may become in some ways sensitized to stress (i.e., “kindled”). This hypothesis was originally situated within a neurobiological perspective, but it has been extended to psychosocial forms of stress and stress responses (George, 2006). Two prominent conflicting explanations are embedded within the kindling hypothesis (Monroe & Harkness, 2005; Morris, Ciesla, & Garber, 2010): (1) individuals may become more sensitized to stress over time and experience recurrences of mood disorder triggered by even minor adversities and (2) recurrent episodes of mood disorder may become autonomous of stress to the extent that stress no longer evokes a mental health response (Monroe & Harkness, 2005). We investigate whether associations pertaining to historical depressive symptom histories operate similarly.
Hypotheses
We hypothesize that (1) multiple depressive symptom trajectories will be detected among these gay men, reflecting heterogeneity across the 28-year study period; (2) aging-related stress, sexual minority stress, and increasing sexual minority stress will be positively associated with current depressive symptomatology; (3) depressive symptom trajectories will affect current depressive symptomatology among some gay men more than others; and (4) the association between current stress and depressive symptoms will be conditional on historical mental health trajectories, with stress having more of an impact on depressive symptoms among some men compared to others depending on their depressive symptom trajectories. We make no a priori assumptions regarding the direction of the hypothesized conditional relationships since previous work has produced mixed findings (i.e., some individuals may become more reactive to stress over time whereas others may become less reactive; Monroe & Harkness, 2005).
Method
The Sample
Data are from two sources. The first is historical data collected over three decades (beginning in 1984/1985) from participants of the Multicenter AIDS Cohort Study (MACS; Detels et al., 1992), one of the largest and longest running studies of the natural history of HIV/AIDS in the United States. The original sample comprised homosexual men who were aged 18 years and older when the study began (additional cohorts recruited for separate studies subsequent to 1984/1985 are not included in this study). A variety of recruitment techniques were used to enroll homosexual men in four U.S. metropolitan areas (Los Angeles, Baltimore, Chicago, and Pittsburgh; baseline N = 4,954), and the data for this study are from the University of California, Los Angeles (UCLA) study site (baseline N = 1,637; 49.5% were HIV positive). Methodological details of the original MACS have been published previously (Kaslow, et al., 1987). Most surviving MACS participants have been assessed (e.g., physical exam, biomarker collection, and interview administration) biannually since the study’s inception, except as described below, for a maximum of 58 completed visits at the time of this analysis. Over the lengthy course of the study, some participants have opted to limit their participation to providing blood samples only, many have died from HIV/AIDS-related disease (Los Angeles N = 680) or other causes (Los Angeles N = 109), and some have been lost to other forms of attrition. Beginning at Visit 23 (in 1995), temporary censoring of some low-risk HIV-negative participants was implemented for budgetary reasons (Los Angeles N = 536). Nearly half of these censored participants were reentered to the study beginning at Visit 36 in 2001 (Los Angeles N = 239). If a participant relocates to an area near one of the other MACS study sites, the participant was asked to continue participation at that site. Thus, the sample size for the Los Angeles MACS is variable, subject to ongoing attrition, reentry, and participant relocation.
The second data source is The Aging Stress and Health Among Gay Men Study (ASH-GM), a contemporary survey of these same Los Angeles-based MACS participants conducted over a 9-month period in 2012/2013, the time span comprising MACS Visit 58. The total number of Los Angeles-based MACS participants eligible for this visit, including those who were originally from one of the other three MACS sites but subsequently relocated to the Los Angeles area, was 498. Participants were invited to complete a paper-and-pencil survey, which required approximately 30–40 minutes. Most were handed the survey at their usual visit and asked to complete and return it within 30 days. The survey was mailed to Los Angeles-based participants who moved out of the area entirely or who only agreed to be contacted about MACS sub-studies and to those who missed having it offered to them at their regular study visit. Participants were provided with incentive gift cards.
In all, 433 surveys were distributed and 342 were returned (a 78.98% return rate). Of these, 30 were excluded from the current study because of ineligibility (e.g., did not self-identify as gay). The final analytic sample size is 312. This research was approved by the UCLA Office of the Human Research Protection Program.
Measures
Depressive symptoms were assessed with the 20-item Center for Epidemiologic Studies–Depression Scale (CES-D; Radloff, 1977) and included items such as “I felt depressed,” “I felt lonely,” and “I could not ‘get going’.” Participants were asked how often (0 = rarely or none of the time to 3 = all of the time) in the past week they experienced the symptom (Visit 58 α = .89). CES-D data were collected at every MACS visit: For Visits 1 through 57 (i.e., biannual data collected between 1984/1985 and 2012/2013), we created long-term trajectories of depressive symptoms (see below). The participant’s modal response for the other items at that visit was imputed for up to 5 missing items (average number of imputed cases per visit = 5.61). Participants missing more than 5 items at a visit were missing for that visit. The number of CES-D visits ranged from 4 to 57 (mean = 40.93). The number of totaled CES-D scores at each visit ranged from 311 at Visit 1 to 150 at Visits 32 and 35 (during censoring), and the mean number of participants across all visits was 224.04. For Visit 58 (N = 312), the CES-D data are from the ASH-GM survey. Consistent with previous studies (e.g., Aneshensel, Frerichs, & Clark, 1981), all CES-D scores (+1.00) were log transformed to improve their nonnormal distribution.
Aging-related stress was assessed in the ASH-GM survey with a measure adapted from the Out and Aging Study (Metlife, 2006). Participants were asked to think about their lives as they get older and to rate concern (1 = not at all to 4 = very) about 8 items (α = .88) such as being alone, outliving income, and having a place to live. Responses were added and divided by 8 to retain the original response metric.
We developed a 4-item sexual minority stress scale based on its four theoretical components (concealment, discrimination, stigma, and internalized homophobia), as suggested by Meyer (2003b). Participants were asked how much (1 = not at all to 4 = very much) they needed to hide their sexual orientation, felt discriminated against, felt people were uncomfortable around them, and had negative feelings about themselves, all due to their sexual orientation. Responses were averaged across items. These items were assessed currently (at the time of the ASH-GM survey, α = .67) and retrospectively (1984/1985 baseline, α = .77). The measures were moderately correlated (R = .32, p < .001), providing evidence that participants were able to differentiate the past from the present.
For retrospective sexual minority stress, participants were asked to think back to 1984/1985 when the MACS study began and record their responses to the 4 items based on how they remember feeling at that time. Retrospective recall is necessary because no concurrent data on sexual minority stress were collected in 1984/1985. Our approach to measuring earlier life-course stress is based on the technique of Pearlin, Nguyen, Schieman, and Milkie (2007) who assessed financial strain earlier in the life course by anchoring questions to specific time points to assess both the timing and the persistence of financial difficulty over time. To facilitate recall, a detailed timeline of historical and pop culture events and circumstances of the period was provided, along with space to fill in personally relevant events. Change in sexual minority stress was calculated by subtracting the baseline value from the current value. When used together, the coefficient for the baseline score represents the effect of sexual minority stress that is stable between 1984/1985 and 2012/2013, and the coefficient for the change score represents the effect of change between the two times.
Background characteristics that may influence parameter estimates were controlled statistically. Relationship status was scored as same-sex registered domestic partnership, same-sex legal marriage, same-sex partnership with no legal status, something else, and single (the reference group). Current area of residence and area of origin were controlled (Southern California, yes/no). Self-rated health was scored fair or poor versus good to excellent. Other control variables were laboratory-assessed HIV status (HIV positive at baseline, seroconverted from HIV negative to HIV positive during the study, HIV negative throughout the study [the reference group]), had an AIDS diagnosis (yes/no), current age (in years, to identify simple linear effects), cohort (to identify deviations from the linear age trend: pre-baby boomer, born before 1946; early baby boomer, born between 1946 and 1953; and late baby boomer, born after 1953 [the omitted reference group]), non-Hispanic White versus other, 4 or more years of college versus not, and employed full time versus not. Methodological controls included being part of the original UCLA Los Angeles cohort (yes/no) and being temporarily censored between 1995 and 2001 (yes/no). Minimal missing data (≤3.2%) were imputed with the mode.
Analysis
Development of longitudinal depressive symptoms trajectories
We use a latent class mixture model for the longitudinal data, which is a semi-parametric method that identifies distinctive clusters of relatively homogeneous individual trajectories of depressive symptoms over time (e.g., Jones, Nagin, & Roeder, 2001; Nagin & Odgers, 2010). This method differs from growth curve models, which assume that one trajectory characterizes the population and that heterogeneity among people can be fully captured by differences in the intercept and slope. Instead this method posits multiple trajectories, that is, different intercepts and shapes.
Depressive symptoms since MACS baseline (Visits 1–57) are operationalized as clusters of trajectories. A polynomial relationship is used to link depressive symptoms with visit number, specifically a quadratic-censored normal model of the type:
Testing stress and depressive symptoms models
We use sequential ordinary least squares regression models to assess theorized associations. Relationships between current depressive symptoms, aging-related stress, sexual minority stress, and change in sexual minority stress are first estimated. Next, background and methodological variables are controlled to eliminate spuriousness. The CES-D trajectories are then operationalized as a series of dummy variables (i.e., belongs to trajectory Group 1 yes/no, belongs to trajectory Group 2 yes/no, etc.). The main effects of these trajectories on current depressive symptoms are first examined, controlling for other variables in the model. Next, multiplicative interaction terms are added to assess effect modification between the trajectory group dummy variables and aging-related stress, current sexual minority stress, and change in sexual minority stress (all mean centered). The Wald test assesses whether the effects for added variables collectively differ from 0.
Results
The Sample
Table 1 presents descriptive characteristics of the ASH-GM sample. On average, participants were 60 years old (range = 48–78 years), with most born during the early to late baby boom period. The majority were non-Hispanic White and college graduates, and 4 in 10 were employed full time (a reasonable number given the age of the sample—30% reported being retired). Most were HIV negative, although one quarter were HIV positive at baseline in 1984/1985 and 14% seroconverted between 1984/1985 and 2012/2013. Ten percent had an AIDS diagnosis, and 15% rated their health as fair/poor. Nearly half were single. One quarter grew up in Southern California and nearly 80% currently resided in Southern California. Nine in 10 were originally members of the UCLA MACS cohort, and 39% were temporarily censored between 1995 and 2001. The average participant reported midrange aging stress, lower than midpoint sexual minority stress at baseline, and even lower concurrent sexual minority stress. Finally, the mean CES-D score at the time of the ASH-GM survey of 11.84 was somewhat high (Blazer, 2003). The overall mean CES-D score across all of the 57 prior visits was 9.26 (SD = 6.21), with the lowest being 8.07 (SD = 8.11) at Visit 28 in 1998 and the highest being 10.84 (SD = 10.20) at Visit 50 in 2008.
Characteristics of Sample of Gay Men Aged 48–78 Years in 2012/2013.
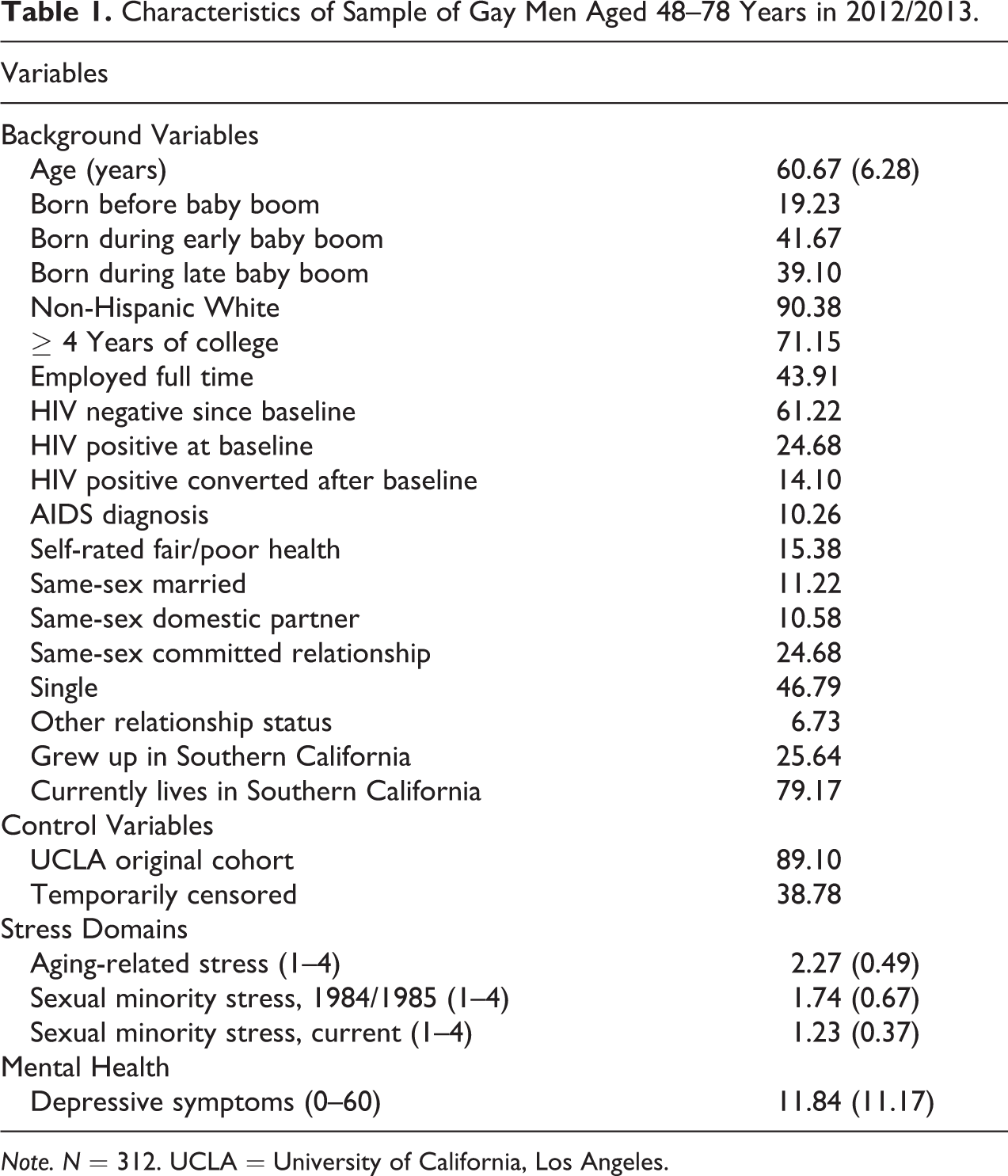
Note. N = 312. UCLA = University of California, Los Angeles.
Longitudinal Depressive Symptoms Trajectories
Figure 2 shows the trajectories calculated for depressive symptoms. After examining BIC, PPs, and group sample sizes, a five-group model was identified as best describing the data (BIC = −15,578.82). As shown in the figure, most groups differ in their average level of depressive symptoms over this lengthy time frame, although one group is stable.
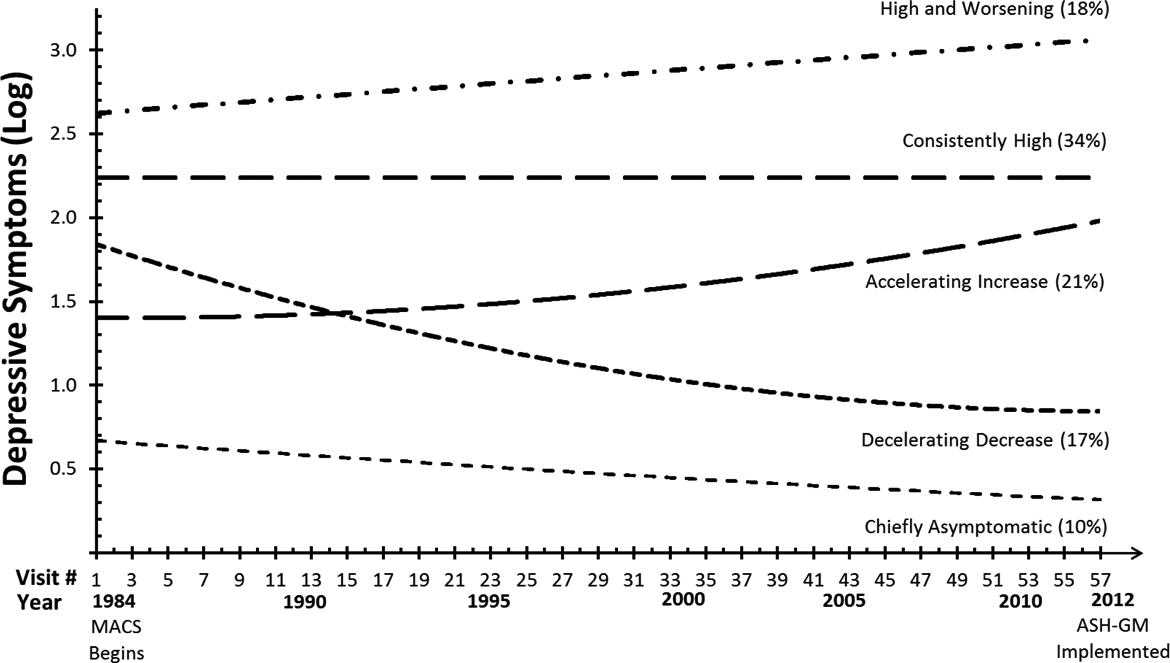
28-Year depressive symptom trajectories among gay men aged 48–78 years in 2012/2013 (N = 312).
The first group, chiefly asymptomatic (9.62%, n = 30), was best described by a linear equation (b 0 = 0.56, SE = 0.05, p < .001; b 1 = −0.01, SE = 0.002, p < .001; mean PP = .99, range = .88–1.0). This group was initially lowest on symptoms and thereafter showed a very slight decline.
The second group, decelerating decrease (16.99%, n = 53), was characterized by a quadratic equation: The intercept (b 0 = 1.88, SE = 0.06, p < .001), linear term (b 1 = −0.04, SE = 0.005, p < .001), and quadratic term (b 2 = 0.0003, SE = 0.00008, p < .001) were all statistically significant (mean PP = .95, range = .51–1.0). This group started with moderately high symptoms at baseline and showed a curvilinear decline (improvement) over the three decades.
The third group, accelerating increase (21.15%, n = 66), was also characterized by a quadratic equation: The intercept (b 0 = 1.39, SE = 0.06, p < .001) and quadratic term (b 2 = 0.0002, SE = 0.00007, p < .01) were statistically significant, whereas the linear term (b 1 = −0.0007, SE = 0.004, p > .05) was not (mean PP = .94, range = .52–1.0). These men started with similar levels of symptoms as the decelerating decrease group but, contrastingly, showed a curvilinear increase in symptoms over time.
The fourth group, consistently high (34.29%, n = 107), was best represented by an intercept only equation (b 0 = 2.24, SE = 0.02, p < .001; mean PP = .92, range = .50–1.0). These men were at the same high level of depressive symptomatology across the span of the study.
The fifth group, high and worsening (17.95%, n = 56), was best described by a linear equation (b 0 = 2.63, SE = 0.04, p < .001; b 1 = 0.008, SE = 0.001, p < .001; mean PP = .96, range = .59–1.0) and showed the highest depressive symptoms at baseline with an increase over time.
Sample Characteristics by Group Membership
Table 2 shows current sample characteristics by trajectory group membership. Whereas there was considerable variability in some of these characteristics across the five groups, few characteristics were significantly different from one another across groups. Men in the high and worsening depressive symptoms group were more likely than men in any of the other four groups to report their current health as fair or poor (p < .001). Men in the high and worsening depressive symptoms group were also less likely currently to be legally married compared to those in the chiefly asymptomatic group (p < .05). These men were also more likely currently to be single compared to men in the chiefly asymptomatic group (p < .01) and compared to men in the accelerating increase group (p < .05). Men in the high and worsening depressive symptoms group were higher on current sexual minority stress compared to those in the chiefly asymptomatic group (p < .05) and the consistently high group (p < .05).
Characteristics Gay Men Aged 48–78 Years in 2012/2013 (N = 312) by Depressive Symptom Trajectory Group.
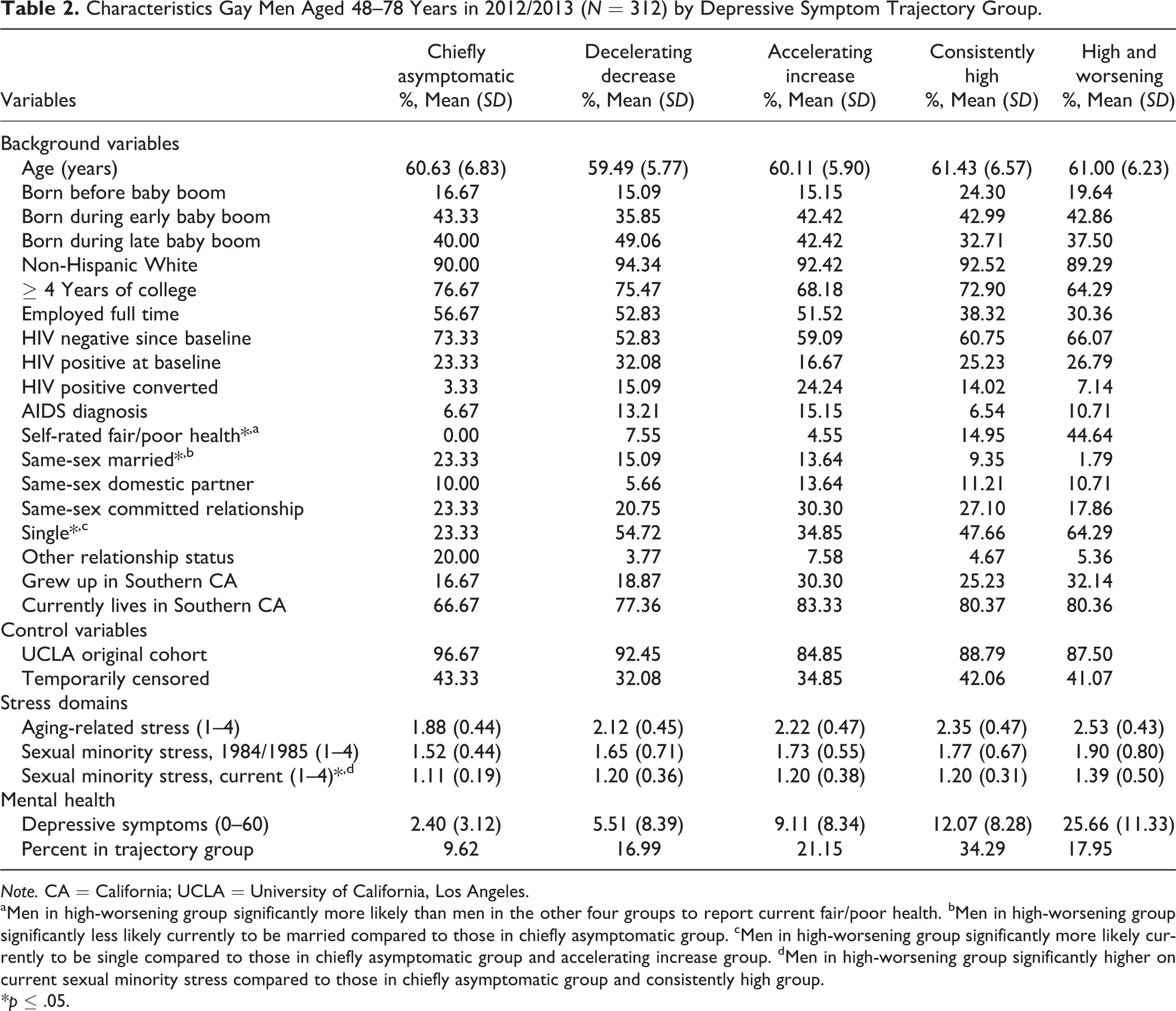
Note. CA = California; UCLA = University of California, Los Angeles.
aMen in high-worsening group significantly more likely than men in the other four groups to report current fair/poor health. bMen in high-worsening group significantly less likely currently to be married compared to those in chiefly asymptomatic group. cMen in high-worsening group significantly more likely currently to be single compared to those in chiefly asymptomatic group and accelerating increase group. dMen in high-worsening group significantly higher on current sexual minority stress compared to those in chiefly asymptomatic group and consistently high group.
*p ≤ .05.
Testing Stress and Depressive Symptom Models
The relationships of depressive symptoms with current aging-related stress, baseline sexual minority stress, and change in sexual minority stress (between 1984/1985 and 2012/2013) were positive and highly significant when considered simultaneously (aging-related stress, b = 0.67, SE = 0.07, p < .001; baseline sexual minority stress, b = 0.54, SE = 0.14, p < .001; change in sexual minority stress, b = 0.49, SE = 0.14, p < .01; intercept = 1.41, SE = 0.20, p < .001; R 2 = .29). As shown in Model 1 in Table 3, adjustment for sample characteristics reduced these regression coefficients, but they remained statistically significant: Depressive symptoms were high among those with high aging-related stress, stably high levels of sexual minority stress, and increasing levels of sexual minority stress. Sample characteristics that also were significantly associated with depressive symptoms (results not shown) were full-time employment (b = −0.49, SE = 0.10, p < .001) and self-rated fair/poor health (b = 0.80, SE = 0.14, p < .001).
Regressions of Current Depressive Symptoms on Aging-Related Stress, Sexual Minority Stress, and Depressive Symptom Trajectories Among Gay-Identified Men Aged 48–78 Years in 2012/2013 (Adjusteda).
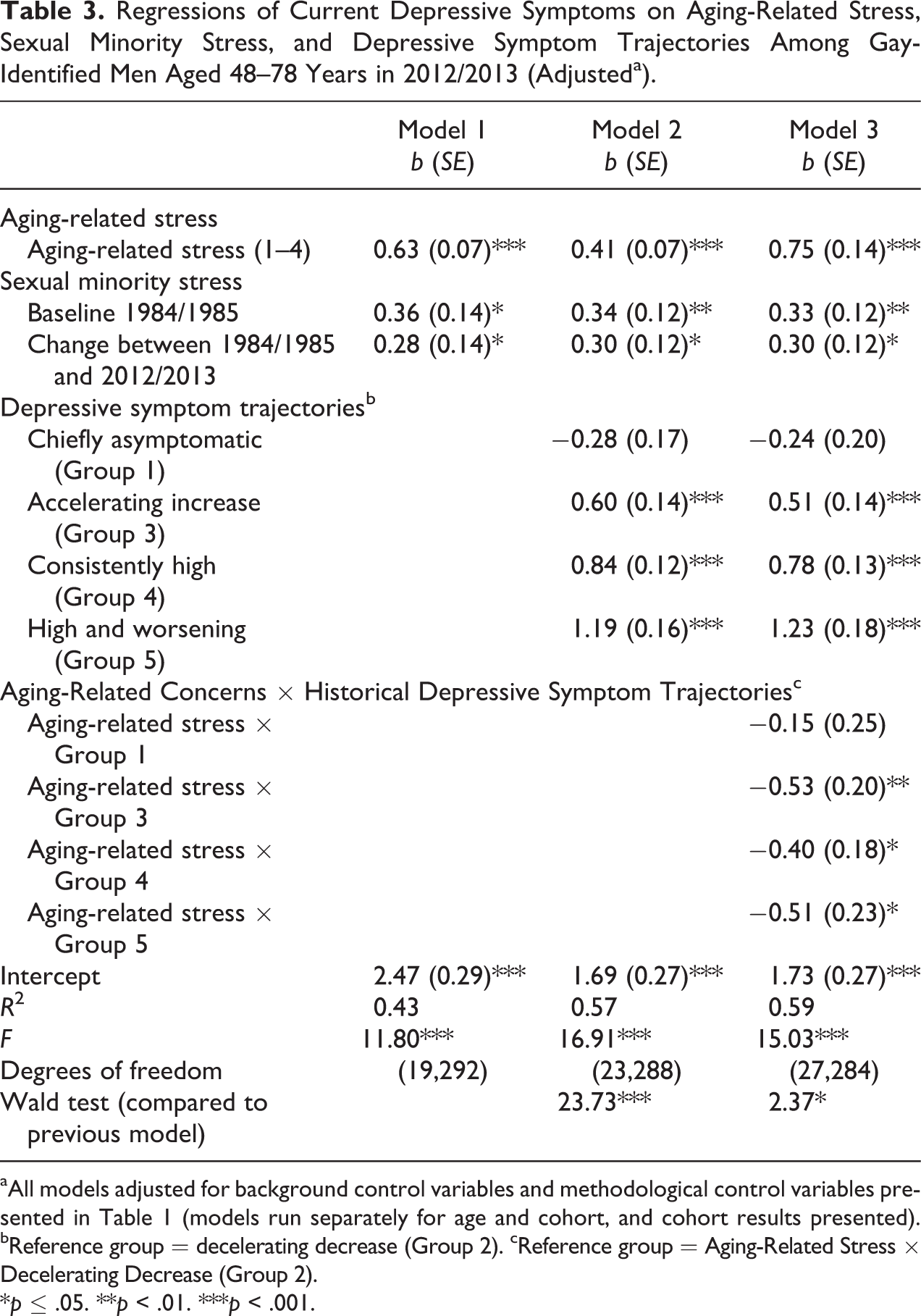
aAll models adjusted for background control variables and methodological control variables presented in Table 1 (models run separately for age and cohort, and cohort results presented). bReference group = decelerating decrease (Group 2). cReference group = Aging-Related Stress × Decelerating Decrease (Group 2).
*p ≤ .05. **p < .01. ***p < .001.
The addition of depressive symptom trajectory groups in Model 2 significantly improved model fit. Group 2 (decelerating decrease) is chosen as the reference category for these analyses for ease of interpretation since this group’s association with depressive symptoms is significantly different from almost all of the other groups except Group 1 (chiefly asymptomatic). Men in Group 2 had significantly less frequent depressive symptoms than those in Groups 3 (accelerating increase), 4 (consistently high), and 5 (high and worsening). Supplemental comparisons indicated that coefficients for all other trajectory groups significantly differed from one another, with the exception of Group 3 (accelerating increase) in comparison with Group 4 (consistently high; p > .05). Compared to Model 1, the R 2 for Model 2 increased from .43 to .57, indicating that the depressive symptoms trajectories accounted for 14% of additional variance in current depressive symptoms, net of stressors and controls.
Three sets of interactions with trajectory groups were then separately tested: (a) aging-related stress, (b) baseline sexual minority stress, and (c) change in sexual minority stress. The addition of the interaction terms to the model was statistically significant only for aging-related stress. As shown in Model 3 in Table 3, the specific interaction terms were statistically significant for all groups except Group 1 (chiefly asymptomatic). Compared to Group 2 (decelerating decrease), aging-related stress had a significantly smaller association with current depressive symptoms among those in Groups 3 (accelerating increase), 4 (consistently high), and 5 (high and worsening). Supplemental tests (not shown) indicated that this slope was statistically significant for Groups 1, 2, and 4, and nonsignificant for Groups 3 and 5.
As shown in Figure 3, when aging-related stress is low, Groups 1 (chiefly asymptomatic) and 2 (decelerating decrease) have similar low levels of symptoms, but Group 2 more closely resembles Group 3 (accelerating increase) when aging-related stress is high. Thus, the impact of aging-related stress on current depressive symptoms appeared to be most depressogenic among men who exhibited improvement in depressive symptoms across the three decades (the decelerating decrease group). The depressive impact of aging-related stress was least pronounced among men who showed an accelerated increase in symptoms.
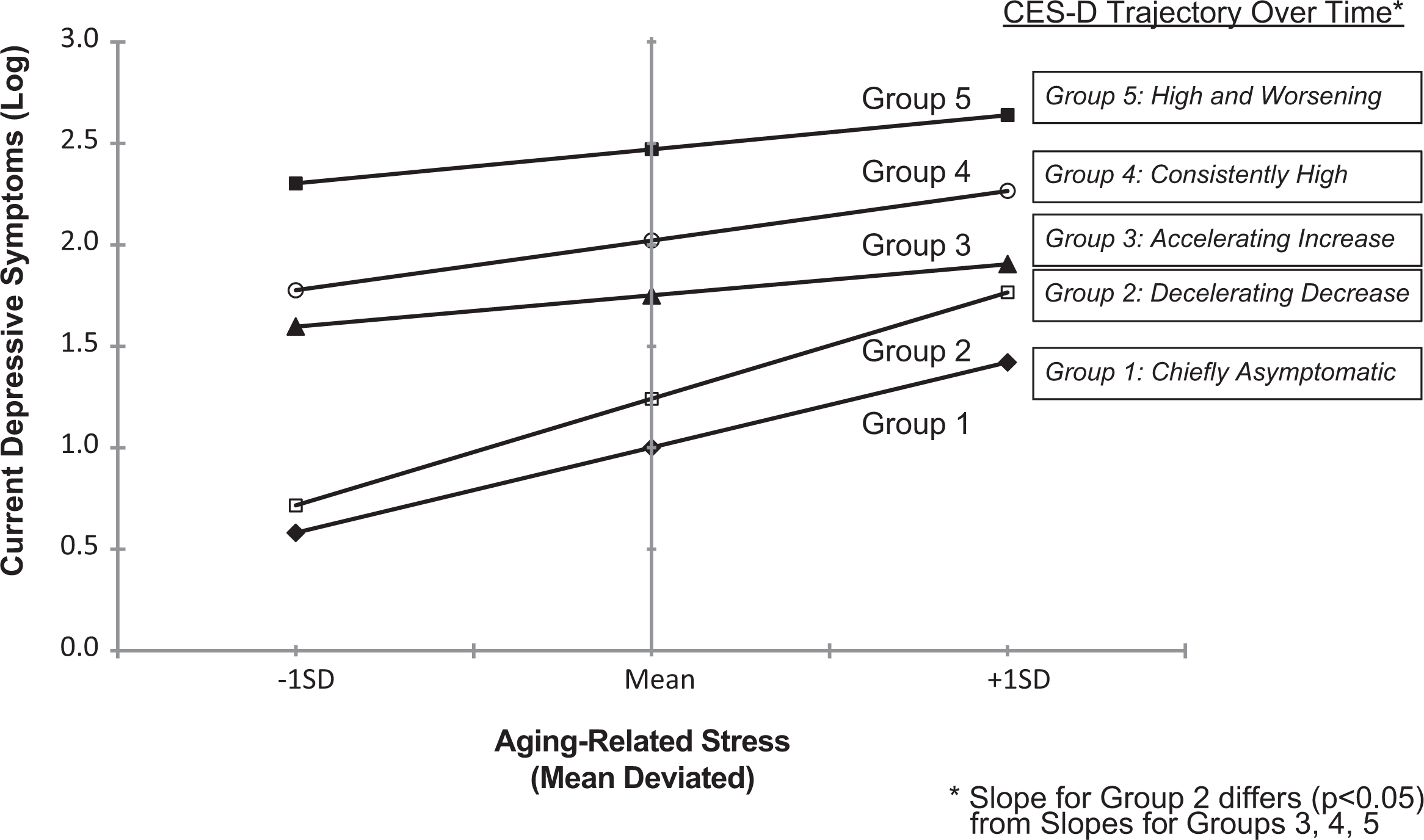
Effect of historical CES-D trajectory group membership on the association between aging-related stress and depressive symptoms. CES-D = Center for Epidemiologic Studies–Depression.
Discussion
This exploratory study found that depressive symptoms over time in this select cohort followed several distinct trajectories that took on various shapes. This finding is consistent with our first hypothesis and with a key principal of the life-course perspective, namely, that transitions or changes in state make up long-term trajectories (e.g., Elder et al., 2003). The sample generally is high in depressive symptomatology: Over half of the men were assigned to “consistently high” or “high and worsening symptom” trajectory groups. These findings were in sharp contrast to other studies of the general population using the same latent class mixture approach. For example, in a representative population-based cohort of older adults in France, Montagnier et al. (2014) found that approximately two thirds of men were assigned to a “never depressed” group and most did not reach high depressive symptom scores. Liang, Xu, Quinones, Bennett, and Ye (2011), using six waves of data from the U.S. Health and Retirement Study and a shortened version of the CES-D, found that only 3.6% of the sample followed a consistently high depressive symptom trajectory. Comparisons between these population-based studies and our study are complicated by different sampling design and methods. Still, these differences may reflect the overall mental health disparity between sexual minorities and heterosexuals (attributed to sexual minority stress; Meyer, Schwartz, & Frost, 2008; or institutionalized discrimination; Hatzenbuehler, McLaughlin, Keyes, & Hasin, 2010) as well as the historical impact of HIV/AIDS on the lives of these men. Alternatively, these findings may be specific to the distinctive nature of this sample.
This study integrates an aging and sexual minority stress model and finds that stressors experienced in both areas are consequential to depressive symptoms among midlife and older gay men. Consistent with previous studies (and our second hypothesis), we found that aging-related stress was positively associated with depressive symptoms in the sample as a whole. We also found that depressive symptoms were high among those with stably high levels of sexual minority stress and those with increasing levels of sexual minority stress between 1984/1985 and 2012/2013. Thus, sexual minority stress has been emotionally harmful for some of these gay men over the long haul of adulthood, even in a social climate of growing acceptance of sexual minorities. However, our findings should be interpreted with some caution, given the retrospective nature of the sexual minority change measure.
This is the first study to examine how depressive symptom trajectories shape the impact of life stressors on current depressive symptomatology among midlife and older gay men. It is well established that previous depressive symptomatology is a significant risk factor for subsequent depressive symptoms (e.g., Kessler, McGonagle, Swartz, Blazer, & Nelson, 1993; Montagnier et al., 2014) Findings presented here support this conclusion (and our third hypothesis) in that being in the increasing, high, and worsening depressive symptom trajectory groups, in comparison to being in the decelerating decrease group, was associated with experiencing more frequent current depressive symptoms. Our findings of positive associations between depressive symptoms and both aging-related stress and sexual minority stress are all the more strengthened because we can rule out confounding due to previous depressive symptom trajectories as an alternative explanation.
This also is the first study to show that depressive symptom trajectories can condition the association between aging-related stress and current depressive symptomatology among midlife and older gay men (consistent with our fourth hypothesis). Our results suggest that men who had experienced elevated levels of depressive symptoms in the past, especially those who showed an accelerated increase in symptoms, are somewhat less reactive or desensitized to the damaging effects of aging-related stress. Although Kessler (1997) found that stress was more impactful to clinical depression among those without prior depression histories, the fundamental tenet remains the same: Previous mental health histories may affect current stress and mental health experiences. Our findings provide some support for the “kindling” premise in that, among some men, recurrent depressive symptomatology or elevated depressive symptoms may become autonomous of certain forms of stress to the extent that this stress no longer evokes a negative response.
However, depressive effects of sexual minority stress were not conditional on depressive symptom trajectories (inconsistent with our fourth hypothesis). This finding may be due to the fact that aging-related stress is a newer experience than sexual minority stress for most of these gay men, and it may be more salient to their current life-course experiences than sexual minority stress, making aging-related stress more susceptible to the impact of previous depressive symptom patterns. (We note that supplemental analysis showed that the interaction terms for Aging-Related Stress × Age/Cohort and Sexual Minority Stress × Age/Cohort were not statistically significant, meaning the effects of these forms of stress are not contingent upon age or cohort.) Such an interpretation is consistent with the proposition that certain stressors may be “eclipsed” over time by those that are more prevalent or dominant in the individual’s life, weakening the association between depressive history and other forms of stress (Monroe & Harkness, 2005; Morris et al., 2010). Aging-related stress and sexual minority stress (earlier and current) are significantly correlated (R = .25, p < .001 for both), but their combined effects on depressive symptoms are not conditional. Thus, the effect of one form of stress does not depend on the other, and our findings suggest that the moderating effect of depressive symptom trajectories is stress domain specific, that is, specific in this instance only to aging-related stress.
There are important limitations to this study to acknowledge. First, the sample of gay men was self-selected and volunteered to participate in the MACS in 1984/1985 and to complete the ASH-GM survey in 2012/2013. Characteristics of these men are similar to those most affected by HIV/AIDS at the onset of the epidemic in the early 1980s (gay, non-Hispanic White men living in urban areas such as Los Angeles). Still, study results should not be generalized to the population of gay men, especially those not residing in such urban areas. Second, there is the possibility that unobserved confounding variables are responsible for significant effects (e.g., aging-related stress may be related to unmeasured personality traits, which could account for its significant association with depressive symptoms). Third, our examination of longitudinal depressive symptom trajectories is not equivalent to controlling for prior depressive symptoms at the individual level because trajectory groups collapse variation within the group, an unavoidable limitation of this method of analysis. Fourth, using retrospective recall for baseline sexual minority stress introduces recall bias, which may be influenced by factors such as stress, health, and/or HIV status. Fifth, sample size may account for some of the nonsignificant findings and a larger sample would have allowed for a more extensive examination, particularly of racial/ethnic subgroup differences, for whom stress experiences may be compounded by other forms of minority stress (Thoits, 2010). Finally, aside from HIV seroconversion, we do not investigate events and circumstances that actually occurred during these men’s lives across the time span of the MACS, essentially leaving a “black box” that needs to be filled by future studies to help explain why these depressive symptom trajectories may have evolved.
In practical terms, our results suggest that intervention efforts must continue to target sexual minority stress as a precursor to emotional distress among midlife and older gay men. Our finding of a significant positive association between current depressive symptoms and persistent and increasing sexual minority stress over the previous three decades is indicative of its pernicious nature and suggests that prolonged exposure to this form of stress does not dissipate its negative mental health effect. Supplemental analysis showed no differential mental health effects of sexual minority stress by age or cohort, meaning that its emotional damage is no less harmful for the oldest men compared to younger men.
Conclusion
It is important for practitioners and researchers to gauge depressive symptom histories among midlife and older gay men because there is wide heterogeneity in symptom trajectories over time, and these histories may play a role in reactions to aging-related stress. We found that aging-related stress is depressive for the men in our sample, on average, but this association is not present for those who have shown accelerated increase and decelerated decrease in depressive symptoms over the previous 28 years. This finding means there is not a one-to-one correlation between experiencing increasing or decreasing symptoms over time and subsequent high or low aging-related depressive symptoms, respectively. Practitioners need to determine whether depressive symptom histories may have sensitized or desensitized their patients to the current health effects of stress in order to develop appropriate treatment plans. Future studies should aim to uncover major events and circumstances that are associated with depressive symptom trajectories among midlife and older gay men.
Footnotes
Acknowledgments
The contents of the article are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health. We thank Allen J. LeBlanc, Dennis S. Miles, May Htike, Daniel Cheng, John Oishi, Kevin Barrett, Charles Doran, and Jessica Reit for assistance with the study’s implementation.
Authors’ Note
This research was approved by the UCLA Office of the Human Research Protection Program.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the National Institute on Aging (R21-AG-042036, Richard G. Wight, Principal Investigator) and the National Institute of Allergy and Infectious Diseases, with supplemental funding from the National Cancer Institute (UO1-AI-35042, UL1-RR025005 [GCRC], UO1-AI-35043, UO1-AI-35039, UO1-AI-35040, UO1-AI-35041, Roger Detels, UCLA Principal Investigator).