
Abstract
This study examined the longitudinal reciprocal effects between health and social support in older adults’ relationships with their children and friends. Data are from the 2006 and 2010 waves of the Health and Retirement Study (N = 3,760). We focused on three specific aspects of social support: frequency of contact, positive interactions, and negative interactions. We used autoregressive cross-lagged models to examine the bidirectional effects between social support and health. When the bidirectional effects between health and social support were simultaneously examined, the longitudinal effect of social support on health was not significant. In contrast, older adults’ poor health was associated with decreased contact and decreased positive interactions with friends as well as with increased negative interactions with their adult children and friends. The findings suggest that older adults’ poor health has a negative impact on their social relationships and that such effect surpasses the impact of social relationships on health.
Introduction
Positive social relationships and good health are two of the most important determinants of successful aging that are closely related to each other. Numerous studies have shown that social support has a positive effect on health, both through a direct effect on it and through buffering the negative effects of stressful life events on health or illness burden (Berkman & Syme, 1979; Hatfield, Hirsch, & Lyness, 2013; House, Umberson, & Landis, 1988). Poor health, in turn, often exerts a negative influence on social relationships through increased caregiving burden and restricted mobility (Eide & Røysamb, 2002).
Although strong evidence demonstrates the positive link between social support and health, little research has simultaneously examined the reciprocal causal pathways between health and social support using longitudinal data (Li & Zhang, 2015 is a notable exception). Furthermore, although previous research has found that various social networks serve different functions (e.g., family vs. friends; Dean, Kolody, & Wood, 1990) and that social relationships can exert both positive and negative influences depending on the types or the nature of support it provides, few studies have incorporated these findings into research on the relationship between health and social support.
Thus, the current study examines (1) the longitudinal reciprocal effects between health and social relationships in later life and (2) whether these effects differ by various sources (i.e., children vs. friends) and types of support (i.e., frequency of contact, positive social interactions, and negative social interactions). We focus on older adults’ relationships with their children and friends given the scarce attention on these relationships compared to marital relationships. For older adults who are not married, their children and friends play a significant role in providing support (Cantor, 1979; de Vries, Utz, Caserta, & Lund, 2014; Hatch & Bulcroft, 1992). Further, previous research suggests that older adults who received support only from kinship networks show poorer health than their peers who received support from both their kinship and their nonkinship networks (White, Philogene, Fine, & Sinha, 2009), suggesting that we need to look beyond family relationships in studying social relationships. Regarding different types of support, in order to capture both quantitative and qualitative aspects of one’s social relationships, we examine three different aspects of older adults’ relationships with their children and friends: frequency of contact, positive interactions, and negative interactions. Conceptually, the frequency of contact is a measure of social integration, which can be defined as the “existence or quantity of social relationships,” whereas the latter two aspects are measures of social support, or emotional support, which represents the quality of the relationships or the process through which social relationships affect health (House, Umberson & Landis, 1988, p. 293). However, because we examine the frequency of contact with children and friends, who often serve as important sources of social support for older adults, we use social support as an umbrella term to refer to all three measures of social relationships used in this study. In the following, we review previous research that explored the effects of health on social support and vice versa. We then present our research which simultaneously examines such effects and explain how the relationship between social support and health would vary depending on different types and sources of support.
Reciprocal Relationship Between Health and Social Support
As noted previously, there is strong evidence supporting the positive association between social support and health (House, Landis, & Umberson, 1988). In particular, numerous studies have shown that a higher level of social integration, measured by the frequency of contact, the presence of social ties, and the number of social activities or organizational affiliations, is associated with better health and lower mortality even after various biological and psychosocial factors that influence both social relationships and health are controlled for (Berkman & Syme, 1979; Hatfield et al., 2013; Holt-Lunstad, Smith, & Layton, 2010; House, Landis, et al., 1988). The mechanisms through which social relationships affect health are diverse. Social support from others, including emotional, instrumental, and financial support, exerts a positive influence on one’s health through increased immune functioning, ability to cope with stress, and healthy behaviors (Oxman & Hull, 1997). However, because most of these studies have examined the effect of social support on health in a unidirectional way, the possibility that those who have poorer health may have less supportive relationships to begin with (i.e., selection effect) was often overlooked.
Compared to a plethora of literature on the effects of social integration or support on health, research on the effects of health on social support is relatively scarce. Further, previous studies present conflicting findings regarding the effects of poor health on social relationships. On the one hand, some studies (e.g., Deimling, Bass, Townsend, & Noelker, 1989) report that poor health and disability constrain older adults’ ability to interact with others and that they are associated with social and emotional loneliness. For example, based on longitudinal data of community-dwelling adults aged 55 and older, Dykstra, Van Tilburg, and De Jong Gierveld (2005) found that poorer self-rated health and greater functional limitations were significantly associated with higher levels of loneliness among older adults. Using the same data, Korporaal, van Groenou, and van Tilburg (2008) found that disability was related to higher levels of emotional loneliness among women but did not find any significant association among men. On the other hand, other studies have found health problems to be associated with increased support. In a comparison of the levels of perceived social support between cancer patients and nonpatients, Tempelaar et al. (1989) found that, on average, cancer patients reported higher levels of perceived support than did nonpatients.
The inconsistencies in previous research findings regarding the effect of health on social support may be in part attributable to methodological issues such as different sample characteristics across studies. Among the studies we reviewed above, those reporting significant associations between poorer health and lower levels of social support used community-based representative samples, whereas those reporting higher levels of social support used voluntary clinical samples comprising patients with specific diseases (e.g., cancer). By using voluntary samples, researchers face the risk of recruiting participants who are different from the general population, and it is plausible that those patients with greater support are more willing to share their thoughts and experiences with the researchers.
In sum, despite much research on the relationship between health and social support, two important gaps remain in previous research. First, because most studies have examined this relationship in one direction, we have limited understanding about the reciprocal effects between the two. Second, because studies have used different samples to examine the relationship between health and social support, there are inconsistencies in findings. Recently, Li and Zhang (2015) have tried to address these problems by examining the reciprocal relationship between older adults’ network types and health. Using longitudinal data gathered in China, they examined the extent to which four different network types (i.e., diverse, friend, family, and restricted) affected various health outcomes and vice versa. They found that there are strong reciprocal relationships between social network types and the health of older adults. However, their study does not inform us about how the quantity or the quality of support from children and friends affect older adults’ health as well as the effect of health on these different aspects of social relationships. In the current research, we try to address these gaps by examining the bidirectional effects between health and social support in a probability sample of older adults in the United States. Specifically, we examine the extent to which health and social support at Time 1 (T1) simultaneously influence social support and health at Time 2 (T2), controlling for T1 measures. By doing so, we aim to explore the causal pathways through which health and social support influence each other over time.
Variations by Sources and Types of Support
The second objective of this study is to examine whether the reciprocal effects between health and social support differ depending on the sources (i.e., children vs. friends) and types of support (i.e., frequency of contact, positive social interactions, and negative social interactions). In order to explicate these potential variations, we first draw on Litwak’s task specific model (Litwak, 1985; Messeri, Silverstein, & Litwak, 1993). This model suggests that different social network members perform different tasks in providing support depending on their proximity, length of commitment, size, and the commonality of life styles. For example, older adults may rely on their spouse or family members living nearby to perform the tasks that require long-term commitment and geographic proximity, such as help with instrumental support; however, for tasks that require commonality of life styles such as leisure activity, older adults may prefer friends to children.
In light of this model, sources of support (i.e., children vs. friends) may be important in the impact of health on older adults’ frequency of contact. Compared to their healthy peers, older adults with poorer health are more likely to depend on their children for instrumental support, as children are an important source of support when aging parents are in need (Hogan & Eggebeen, 1995). Thus, older adults with poorer health may show more frequent contact with their children. On the other hand, relationships with friends are more likely to be based on voluntary and reciprocal exchanges of support (Adams & Blieszner, 1995). Thus, when older adults with poorer health are no longer able to participate in shared activities and become limited in reciprocating the support that they receive from friends, their frequency of contact with friends, especially with distant ones, may naturally decrease. Thus, in the case of the quantity of support, older adults’ poor health is likely to be associated with more frequent contact with children but less frequent contact with friends.
However, for another type of support, namely positive interactions in social relationships, sources of support may not play a critical role. Socioemotional selectivity theory (Carstensen, 1992) suggests that as people perceive the finality of time they have in life, they tend to focus on close social ties that can fulfill their emotional needs. With such selection, although older adults’ overall social contact may decrease with age, their closest social ties and the emotional support that they receive from these relationships tends to remain stable over time. Poor health may naturally lead one to think about limited time left to live. Thus, older adults with poorer health may be more likely to focus on emotionally close social relationships compared to their peers with relatively good health. Further, even within close social ties, older adults with poorer health may naturally focus on the relationships that are accepting and supportive in order to maximize their emotional gains. Thus, poor health may be associated with increased level of positive interactions with both children and friends.
Regarding the impact of poor health on negative social interactions, because of the dearth of research in this area, it is difficult to generate a clear hypothesis. However, two alternative hypotheses may be posited. On the one hand, poor health may be associated with reduced negative interactions with both children and friends, given that those in the older adults’ close circle of social support may try not to be too demanding and critical when the older adults are going through stressful life events (Ha & Ingersoll-Dayton, 2008). Also, in light of socioemotional selectivity theory presented above, older adults with poorer health may be more likely to avoid negative social interactions and focus on positive ones. On the other hand, because increased contact inevitably brings more negative as well as positive interactions within a relationship, and older adults with poor health are likely to have increased contact with children but decreased contact with friends, older adults with poorer health may experience more negative interactions with children than do their healthy peers, but not with their friends.
To date, although much research has examined the impact of different sources and types of social support on health, few studies have systematically examined the impact of health on various aspects of social relationships. Further, only a few studies have examined this question in a bidirectional model, where health and social relationships exert reciprocal influence on each other. In our examination of longitudinal, bidirectional effects between health and social support, we examine not only the impact of health on frequency of contact, positive interactions, and negative interactions with adult children and friends, but also the reciprocal effects of various aspects of social support on health. We propose that social support will have a positive effect on health, yet the health effects on social support would differ by the sources and types of support as explained above.
Method
Data Source
The data for this study were drawn from the 2006 and 2010 waves of the Health and Retirement Study (HRS), a nationally representative panel survey of individuals aged 51 and older. The first wave of the HRS data collection was conducted in 1992. Subsequent data collections occurred every two years through 2014, with new cohorts added in 1998 and 2004. The HRS consists of five subsamples: original HRS sample (born in 1931–1941), Oldest-Old sample (born before 1923), Children of the Depression Age sample (born in 1924–1930), War Baby sample (born in 1942–1947), and Early Baby Boomer sample (born in 1948–1953). The response rates of these subsamples ranged from 70% to 80.4%.
Analytic sample
Since 2006, a random half of the HRS participants received an additional questionnaire on psychosocial aspects of their lives after their in-person interviews. This leave-behind questionnaire (LBQ) included measures of frequency of social contact and the level of positive and negative interactions with children and friends; this information enabled us to explore the reciprocal effects between health and older adults’ social relationships. The 2006 LBQ participants were reinterviewed in 2010. (In 2008, another half of the original sample was given the LBQ; thus, 2008 LBQ participants do not overlap with 2006/2010 LBQ participants.) To examine the way health (or social support) at T1 (2006) affects support from children and friends (or health) at T2 (2010), controlling for the outcomes at T1, we used an analytic sample of 3,760 older adults who were aged 60 or older and who had participated in the 2006 and 2010 core and LBQ interviews.
Attrition in longitudinal data
One potential limitation of using longitudinal data is that the data may suffer from selective attrition. In our study, among 18,469 individuals who participated in the 2006 core survey, 14,483 (approximately 78.4%) participated in the 2010 survey. Among the nonparticipants (n = 3,986), 2,593 had died, 1,373 were alive but did not respond, and 20 asked to be dropped from the sample before the 2006 wave. Using logistic regression models, we conducted attrition analysis, examining whether respondents with certain demographic characteristics were more likely to have died or dropped out of the study during the 4-year period. This analysis revealed that those who were older, had poorer health, and were male were less likely than younger, healthier, and female respondents to participate in the follow-up surveys. Given such selective attrition, caution should be taken in generalizing our findings. Education and race did not significantly affect the attrition.
Measures
Measures of social support
Three variables were used to assess the quantitative and qualitative aspects of social support: frequency of contact, positive social interactions and negative social interactions. Frequency of contact was assessed with the following questions: “On average, how often do you (a) meet, (b) speak on the phone, or (c) exchange letters or email with any of your [children, friends]?” Response categories ranged from 1 = less than once a year or never to 6 = three or more times a week. We calculated the mean of 3 items for children and friends, respectively. Positive interactions were assessed with the following three questions regarding children (α = .82) and friends (α = .84): (a) “How much do they really understand the way you feel about things?” (b) “How much can you rely on them if you have a serious problem?” and (c) “How much can you open up to them if you need to talk about your worries?” Negative interactions were assessed with the following four questions (α = .76 for children and α = .73 for friends): (a) “How often do they make too many demands on you?” (b) “How much do they criticize you?” (c) “How much do they let you down when you are counting on them?” and (d) “How much do they get on your nerves?” Response categories for both scales ranged from 1 = not at all to 4 = a lot. These measures were adopted from Schuster, Kessler, and Aseltine (1990).
Self-ratings of health
Previous research has shown that self-rated health (1 = excellent health to 5 = poor health) is strongly correlated with other objective measures of health and is a good predictor of mortality (Bernard et al., 1997). Given that older adults’ ability to engage in social activities may be affected by disability or major chronic health problems, we also considered the level of functional limitations, the number of chronic health problems, and the onset of new conditions as our independent variables in our preliminary analyses. However, of all these variables, self-rated health yielded the most robust findings. Thus, we focus on the impact of self-rated health in this article. Functional limitations are included in the model as a control variable.
Control variables
We controlled for sociodemographic variables, including age (in years), gender, race (1 = non-White, 0 = White), education (in years), marital status, functional limitations, and depressive symptoms, as these factors are closely related to variations in health and social support (Bozo & Guarnaccia, 2010; McLaughlin, Adams, Vagenas, & Dobson, 2011). Marital status was assessed with three dummy variables capturing widowed, divorced, and never married individuals (reference category = married individuals). In the preliminary analyses, we also tried a different categorization of marital status to capture changes in marital status. However, because of the small number of people who experienced a change between T1 and T2, we included T1 marital status only. Functional limitations assesses the number of problems in activities of daily living (ADL), including bathing, eating, dressing, walking across a room, and getting into or out of bed. For each activity, respondents were asked, “Because of a health problem, do you have any difficulty with [specific activity]?” Response categories included “Yes,” “No,” Can’t do,” and “Don’t do.” Responses of “Yes” and “Can’t do” were included in counting the number of ADL impairments. Depressive symptoms (α = .80) is the sum of 8 Center for Epidemiologic Studies Depression Scale items (Steffick, 2000) assessing whether the respondent had experienced the following sentiments much of the time during the preceding week: depressed, everything is an effort, felt alone, felt sad, could not get going, felt happy, sleep is restless, and enjoyed life. We reverse-coded two positive indicators before we summed up the responses.
Analysis Plan
We first summarized sample characteristics using descriptive statistics (means, standard deviations, and paired t-tests) and presented correlations between health and social support variables. To address the research questions, we employed autoregressive cross-lagged model, a simultaneous structural equation modeling (SEM). This model is widely used to detect the reciprocal relationships between two variables (Kenny, 1975; Li & Zhang, 2015). Specifically, as shown in Figure 1, we hypothesized that social support and health simultaneously influence each other over time and allowed social support and health to be correlated with each other at T1 and T2. Thus, health (social support) at T1 can influence social support (health) at T2 both directly and indirectly through social support (health) at T1.
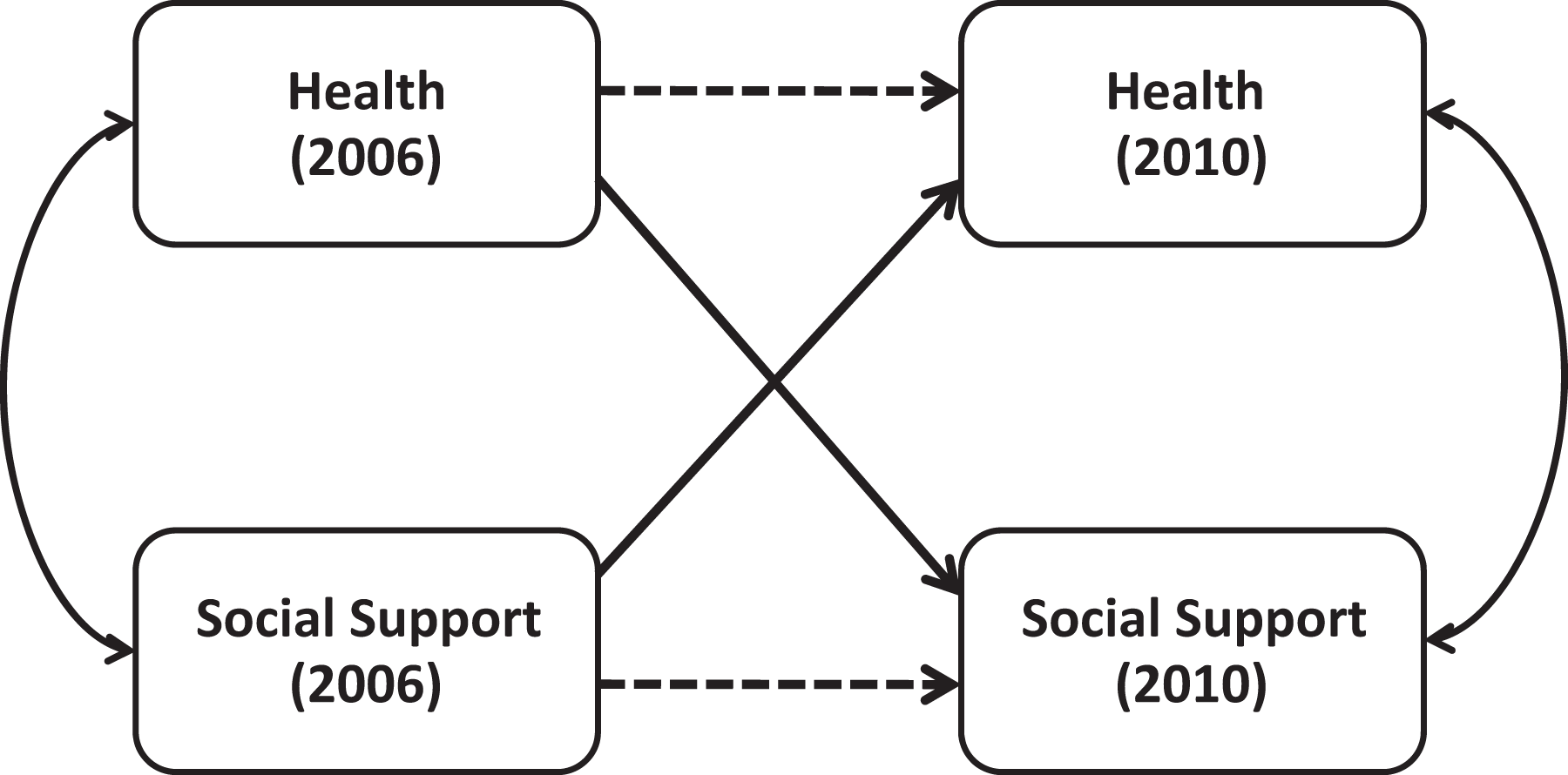
Conceptual model.
We tested the study hypotheses with six sets of simultaneous SEM, depending on types (i.e., frequencies of contact, positive social interactions, and negative social interactions) and sources (i.e., from children and friends) of social support. We examined the model fits using the indicators and thresholds recommended by Hu and Bentler (1998, 1999), including chi-square, root mean square error of approximation ≤ .08, incremental fit index ≥ .90, and comparative fit index ≥ .90. Analyses were conducted using SPSS AMOS 19.
Results
Sample Characteristics
Table 1 shows descriptive statistics. For social support and health measures, paired t-test results are presented to show significant changes over the 4-year period. The results show that, except for positive interactions with children, all indicators of support declined significantly. The participants also reported poorer health in 2010 than in 2006 (t = 8.32, p < .001). The mean age of the analytic sample was 70.79 ± 7.15, with 17% being non-White and 43% having received college education. About 67% of the participants were married, 11% divorced, and 20% widowed.
Descriptive Statistics.
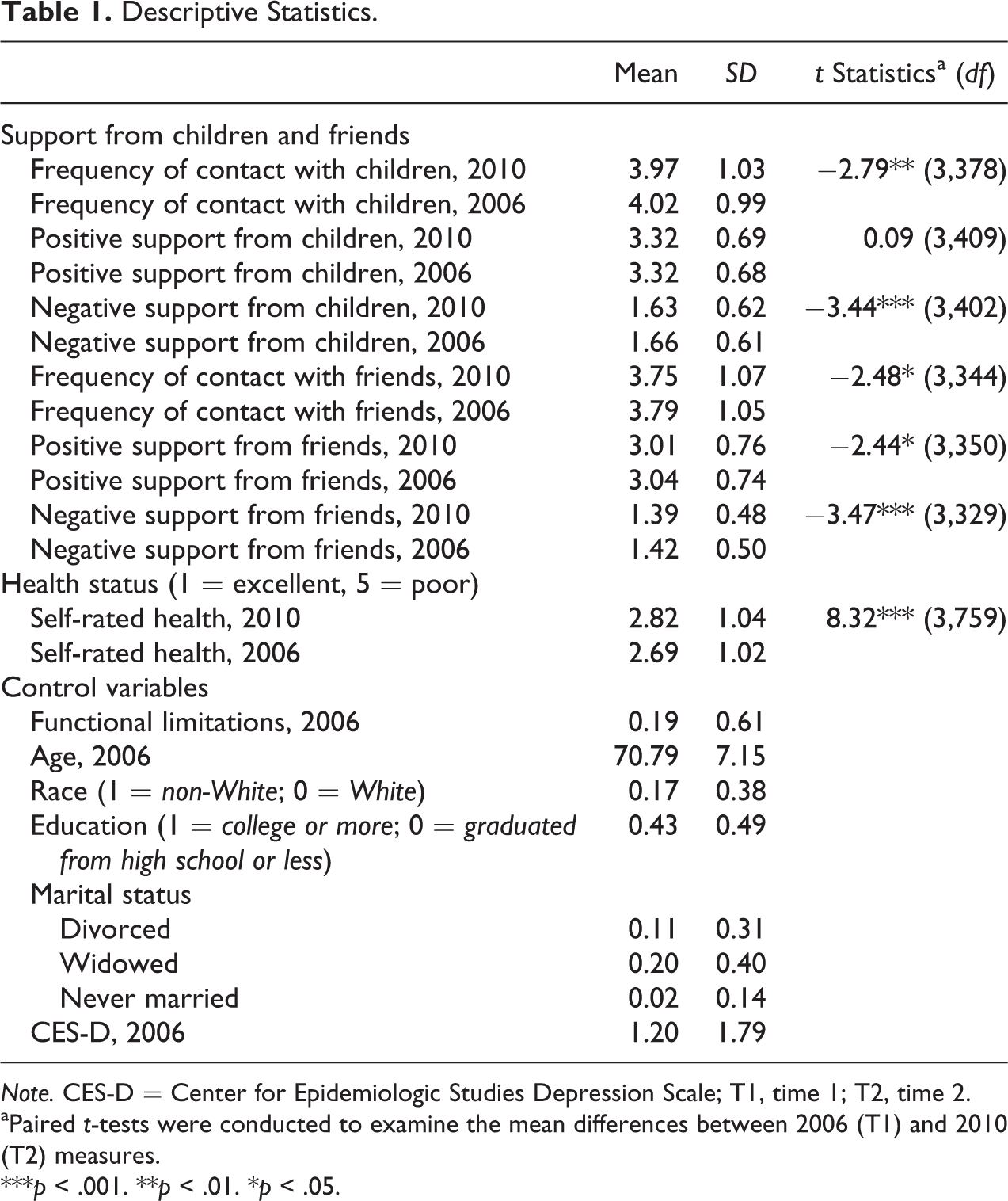
Note. CES-D = Center for Epidemiologic Studies Depression Scale; T1, time 1; T2, time 2.
aPaired t-tests were conducted to examine the mean differences between 2006 (T1) and 2010 (T2) measures.
***p < .001. **p < .01. *p < .05.
Table 2 shows correlations among health and social support variables. At the bivariate level, poorer health at both T1 and T2 was associated with fewer contact, fewer positive social interactions, and more negative interactions with children and friends at T1 and T2.
Correlations Among Health and Social Support Variables.
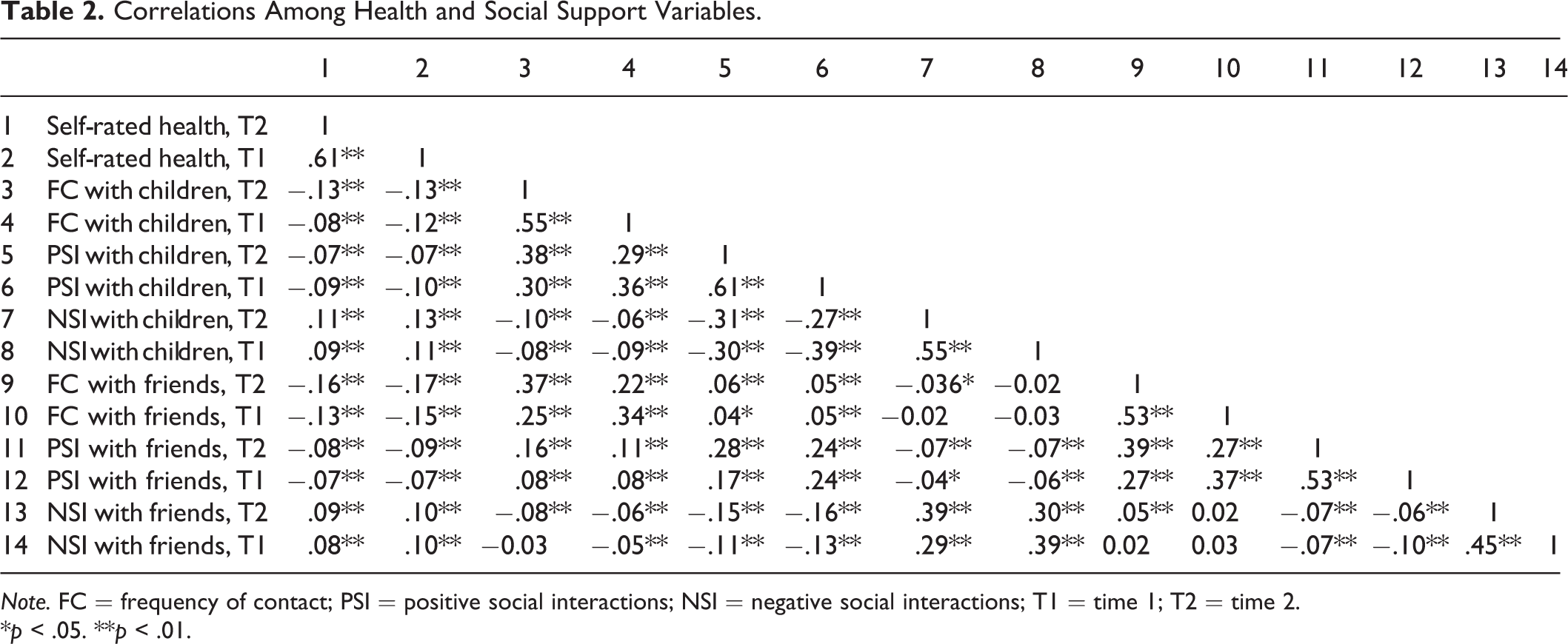
Note. FC = frequency of contact; PSI = positive social interactions; NSI = negative social interactions; T1 = time 1; T2 = time 2.
*p < .05. **p < .01.
Multivariate Analyses
Next, we used simultaneous equation models to predict both the effects of health on social support and the effects of social support on health (Tables 3–5). Interestingly, the hypothesis that social support at T1 will be associated with better health at T2 was not supported in any of the models. None of the three indicators of social support at T1 exerted a significant influence on health at T2. In contrast, the effects of health at T1 on social support at T2 were significant in four of six models, although the directions of these effects did not always support our hypotheses.
Reciprocal Effects Between Health and Frequency of Social Contact With Children and Friends.
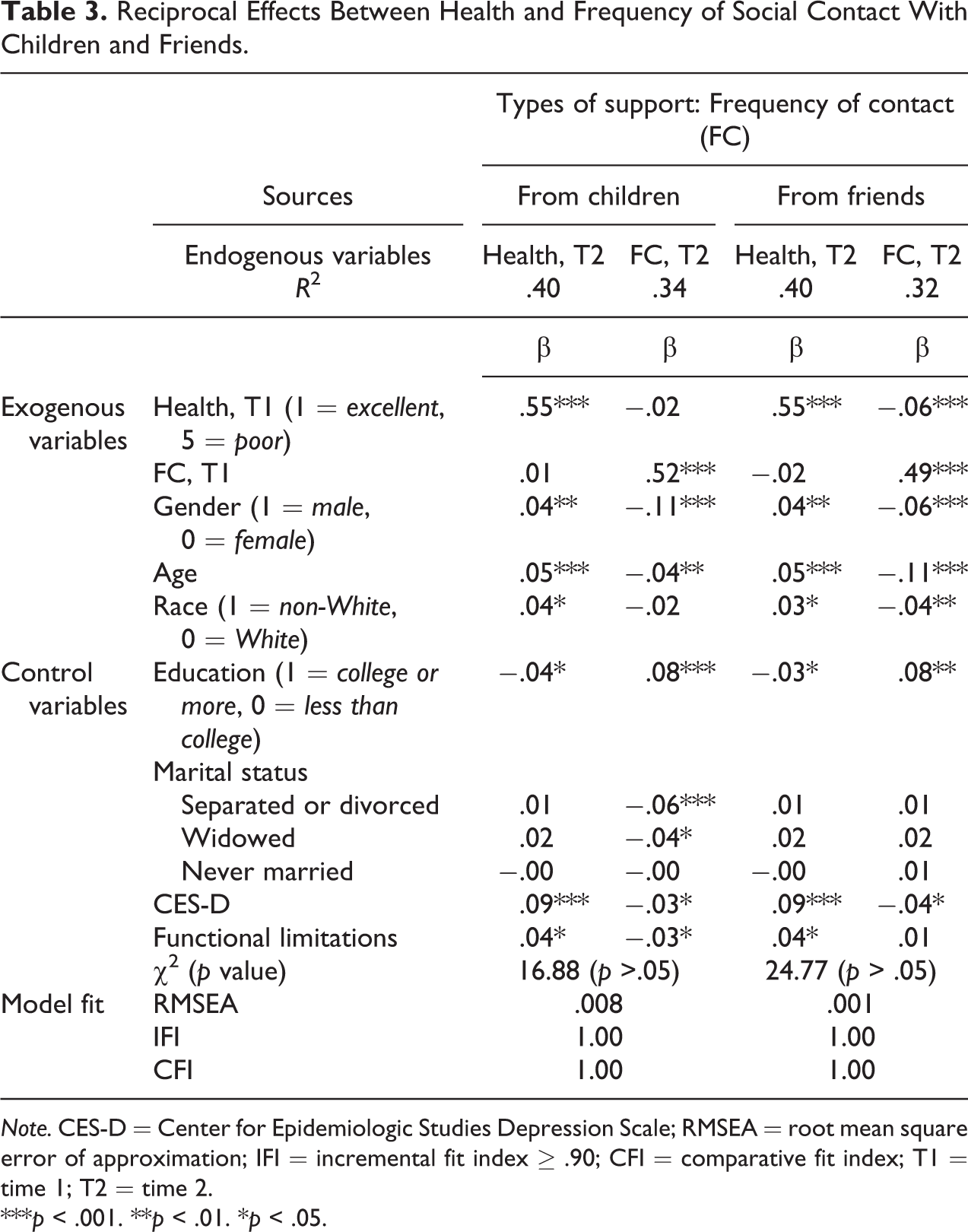
Note. CES-D = Center for Epidemiologic Studies Depression Scale; RMSEA = root mean square error of approximation; IFI = incremental fit index ≥ .90; CFI = comparative fit index; T1 = time 1; T2 = time 2.
***p < .001. **p < .01. *p < .05.
Reciprocal Effects Between Health and Positive Social Interactions With Children and Friends.
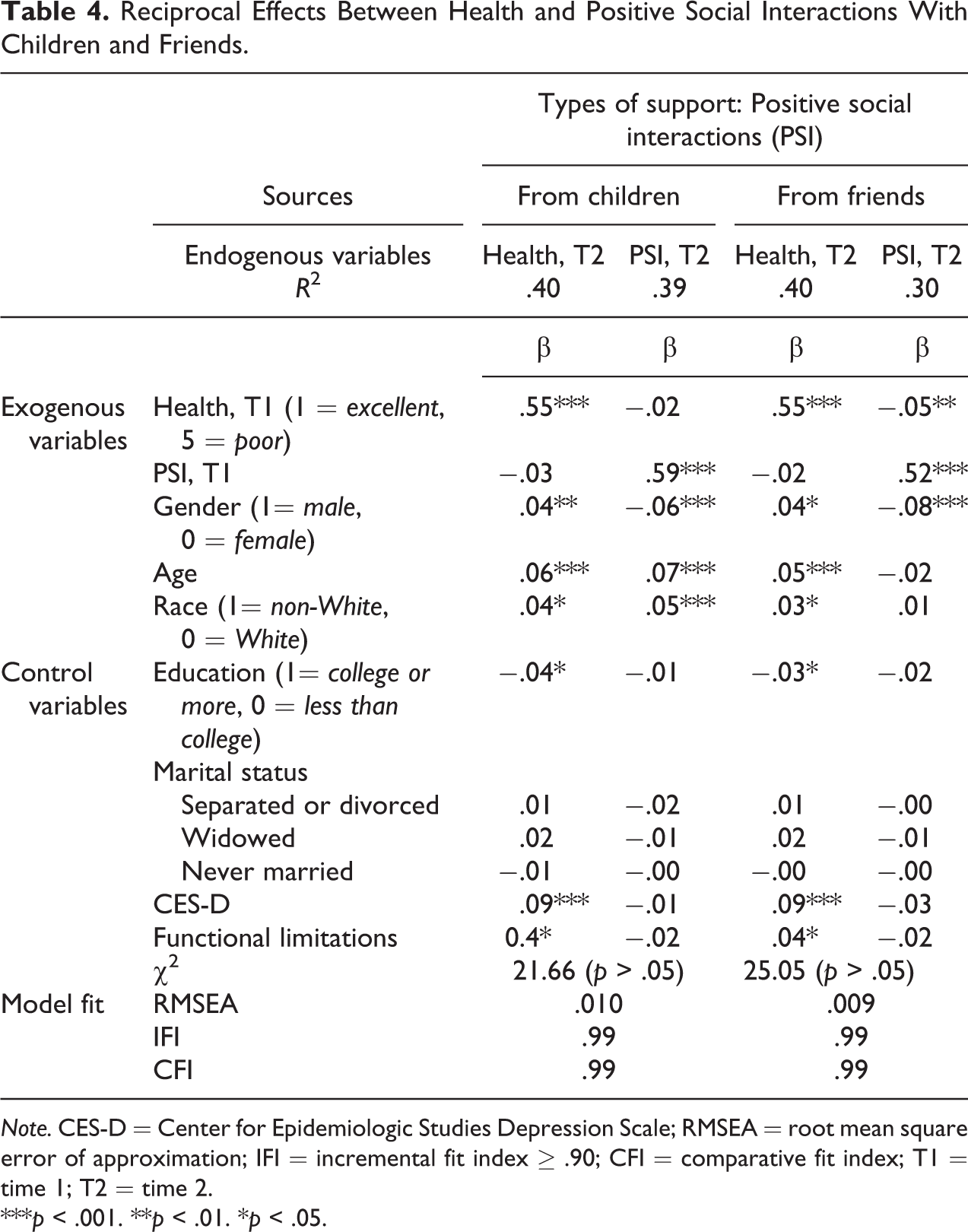
Note. CES-D = Center for Epidemiologic Studies Depression Scale; RMSEA = root mean square error of approximation; IFI = incremental fit index ≥ .90; CFI = comparative fit index; T1 = time 1; T2 = time 2.
***p < .001. **p < .01. *p < .05.
Reciprocal Effects Between Health and Negative Social Interactions With Children and Friends.
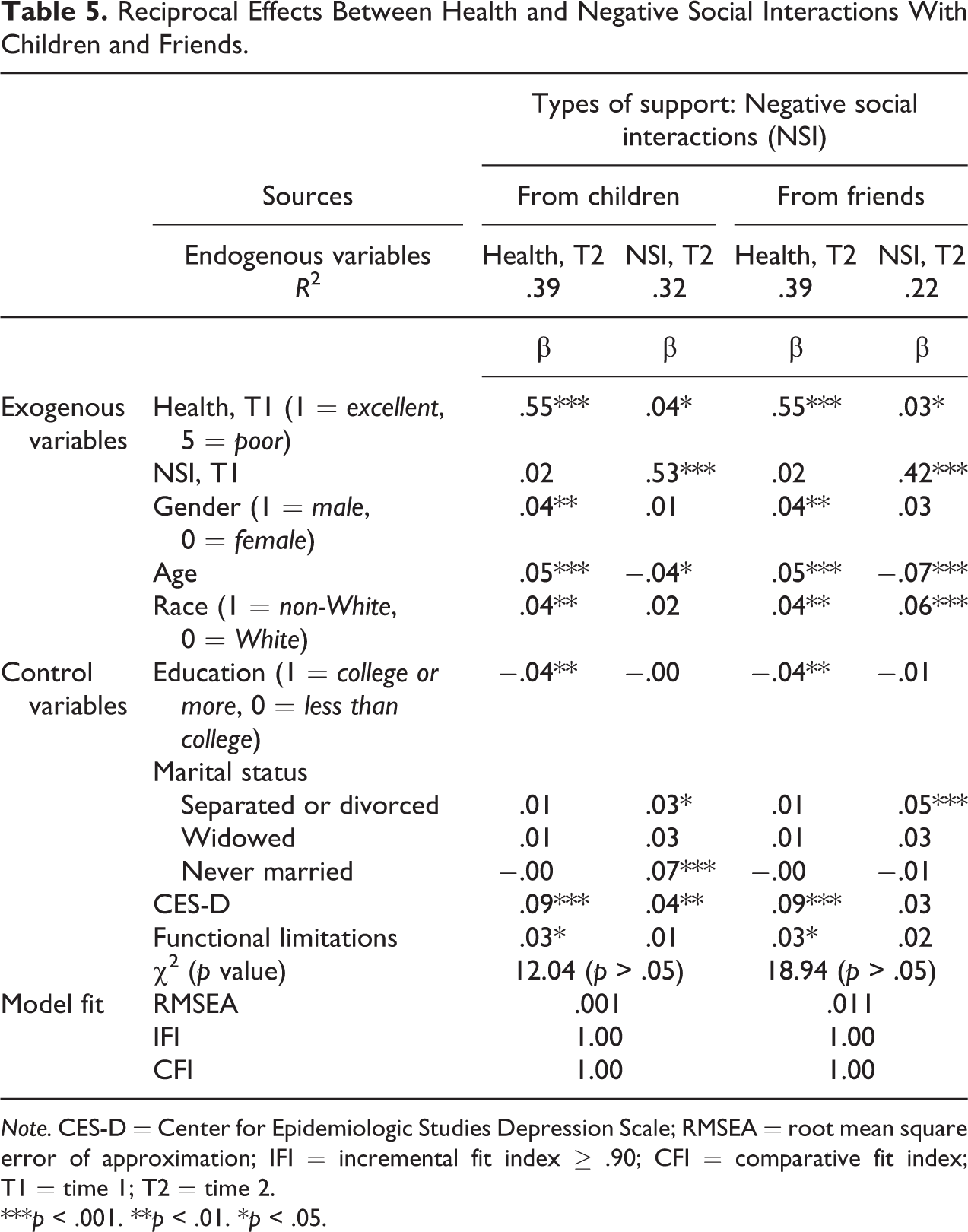
Note. CES-D = Center for Epidemiologic Studies Depression Scale; RMSEA = root mean square error of approximation; IFI = incremental fit index ≥ .90; CFI = comparative fit index; T1 = time 1; T2 = time 2.
***p < .001. **p < .01. *p < .05.
Specifically, the hypothesis that poor health at T1 will be associated with more frequent contact with children and less frequent contact with friends at T2 was supported only in predicting contact with friends. As shown in Table 3, poor health at T1 had a negative effect on contact with friends (β = −0.06, p < .001), yet the frequency of contact with children was not affected by earlier health condition. The next hypothesis that poor health at T1 will be associated with more positive interactions with children and friends at T2 was not supported. Instead, poor health exerted a negative effect on positive interactions with friends (β = −0.05, p < .01), and it did not have a significant effect on positive interactions with children (Table 4). As for negative interactions (Table 5), poorer health at T1 was associated with greater negative interactions with both children (β = .04, p < .05) and friends (β = .03, p < .01) at T2.
Among control variables, being male was associated with poorer health, fewer contacts, and fewer positive interactions with children and friends. However, there were no significant gender differences in the level of negative social interactions with children and friends. Older respondents reported poorer health and fewer contacts with children and friends. However, they also reported more positive interactions with children and less negative interactions with both children and friends. Non-White respondents reported poorer health, fewer contacts with friends, and more negative interactions with friends. Regarding support from children, however, non-White respondents reported higher levels of both positive and negative interactions compared to their White peers. Respondents with college education reported better health and more frequent contact with children and friends. Being separated or divorced was associated with fewer contacts with children and more negative interactions with children and friends. Widowed older adults also experienced less frequent contact with children and friends than did married respondents, and never married older adults reported greater negative interactions with children. Depressive symptoms were associated with poorer health, fewer contacts, and more negative interactions with children and friends. Functional limitations were associated with poorer health and fewer contacts with children.
Discussion
Summary of Findings
Using a national probability sample of older adults, our research examined the longitudinal reciprocal effects of health and social support and the extent to which these effects differed, depending on the types and the sources of support. We hypothesized that health would not only be influenced by but also influence social support. We also hypothesized that such reciprocal relationships would vary by the types and the sources of support, given older adults’ interest in fulfilling emotional needs and the different functions of children and friends in older adults’ support networks. In this section, we summarize our key findings and discuss their implications for future research.
First, contrary to our hypothesis and previous research findings, none of the T1 indicators of social support in our model showed a significant influence on self-rated health at T2. This finding was quite surprising, given the robust previous research findings showing the beneficial effects of social support on health. We further conducted ordinary least squares regression analysis to see if unidirectional effects of T1 social support on T2 health were significant, and we found that all three indicators of support from children and friends at T1 were significant predictors of health at T2 in these models, even after controlling for health at T1. Thus, we can infer that, although earlier social support predicts later health, when both directions of the effects between health and social support are considered simultaneously, the effect of health on social support is by far greater than the effect of social support on health. Although more research is necessary to understand the exact reason for the null effect of social support on health in the bidirectional models, our finding underscores the significance of health in determining the quality of one’s social relationships in later life. In particular, the finding that poor health is associated with greater negative interactions with both children and friends is alarming, given previous research findings that negative interactions have a potent, deleterious influence on one’s well-being (Newsom, Mahan, Rook, & Krause, 2008). Future research should further explore the factors that could help older adults preserve positive relationships with others when they are going through daily stresses associated with health problems.
An alternative explanation for our findings is that the 4-year gap that we examined is too short for us to observe any noticeable impact of social support on changes in health, whereas the impact of health is visible in the short term. Previous research has suggested that positive and negative interactions with significant others influence health through physiological mechanisms such as allostatic load or inflammation (Clark, Bond, & Hecker, 2007). It is likely that it takes time for these underlying mechanisms to accumulate stress and influence health. Hence, future research should explore whether the reciprocal effects between health and social support change over time, using longitudinal data with a longer time frame.
Our results partially supported our second hypothesis in that the effects of poor health on social support differed, depending on the types and the sources of support. However, some of the findings were not supportive of our specific hypothesis. First, with regard to the effect of poor health on the frequency of social contact, poor health was associated with fewer contacts with friends, yet it did not have a significant influence on contact with children. In terms of positive interactions, poor health was associated with lower levels of positive interactions with friends and did not influence positive interactions with children. As for negative interactions, poor health was associated with higher levels of negative interactions with both children and friends.
Although our findings did not show any evidence that poor health is associated with increased contact with children as we hypothesized, the finding that poor health had a negative impact on contact with friends but not so much on contact with children supports our hypothesis that children and friends carry out different functions in times of need. Friendship is often formed based on shared interests and activities (Connidis & Davies, 1992). Older adults whose health is poor may no longer be able to engage in these activities and may thus experience fewer contacts and less positive interactions with friends. Although older adults may have difficulty meeting with children as well, children’s provision of support in times of need may cancel out the effect of this trend.
With regard to positive interactions, we initially hypothesized that positive interactions with both children and friends will increase when older adults have poor health. Our hypothesis was based on socioemotional selectivity theory, which suggests that older adults selectively focus on close social relationships when they perceive their lifetime as limited. However, the results show that older adults’ friendships may be vulnerable to poor health in later life. Maintaining positive relationships with friends may be especially difficult, given that other friends may also be going through health problems in later life.
With regard to negative interactions, although the effect sizes were small, poor health was associated with greater negative interactions with both children and friends. Several factors may account for such an effect. Respondents with poor health may become more dependent on children and friends because of their disability, and such increased dependence may create room for more negative interactions (Johnson & Troll, 1994). Further, poorer health may limit one’s ability to reciprocate support and have a negative effect on older adults’ perception of self (Thomas, 2010), which may negatively influence one’s social relationships with others. Poor health may also make a sick person less tolerable about critiques and demands from his or her children and friends.
Limitations and Future Directions
The current study has a few limitations. First, in this study, we focused on self-rated health as an indicator of older adults’ health status. We decided to do this because (1) self-rated health is one of the most effective global measures for assessing one’s objective state of health (Bernard et al., 1997) and (2) using other summary measures, such as functional limitations and number of chronic conditions, did not produce clearer findings. Also, because our analyses were based on a mostly community dwelling probability sample, we did not have enough cases to investigate the effects of specific diseases (e.g., cancer, heart failure) on older adults’ social relationships. However, given that specific health problems or illness manifestation may have different implications for family relationships and support, as well as social stigma, future studies should explore how specific diagnostic groups and changes in various aspects of health (e.g., the presence of a chronic illness, physical vs. cognitive functioning, need for personal care) affect older adults’ social relationships.
Second, our social support measures are limited in that they capture only the older adults’ perceptions of support from children and friends, which can be influenced by the older adults’ mood and health-related distress. Our measures also do not specify whether changes in the frequency of contact are initiated by the older adults or by others. To better understand changes in social dynamics when older adults have health problems, it is important to examine the way their health affects the behaviors and perceptions of various actors (e.g., the older adults themselves, their children, and their friends) differently. Future studies should also explore the extent to which health affects objective measures of support, such as hours of care given or received.
Finally, future studies should investigate the effects of possible mediating and moderating factors. For example, an interesting variable to consider may be the caregiving status of children or other family members. Previous research has suggested that negative interactions between parents and children increase when parents feel that they are dependent on their children (Ha & Ingersoll-Dayton, 2008) or when their children are dependent on them (Pillemer & Suitor, 2002). Building on this literature, future research should investigate the question of whether the negative effect of poor health on older adults’ relationships with children and friends is explained or exacerbated by the caregiving burden associated with health problems.
Conclusions
In conclusion, our findings show that when reciprocal effects of health on social support are examined in an autoregressive cross-lagged model, poor health at T1 exerts a significant negative influence on social relationships at T2 among older adults, whereas social support at T1 does not exert much influence on older adults’ health at T2. These findings suggest that social relationships suffer when older adults experience health problems. The findings also indicate that the negative effects of poor health are greater on friendships than on parent–child relationships among older adults. These findings call for policies or social service programs that could help older adults maintain or strengthen their social relationships in times of need, such as when older adults experience health problems.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the John A. Hartford Faculty Scholars Program in Geriatric Social Work, administered by the Gerontological Society of America (PI: Jung-Hwa Ha) and the Research Settlement Fund for the new faculty of SNU.