
Abstract
Objective:
Successful aging (SA) is a concept that remains without a consensus definition. The purpose of the current study was to explore the components of SA by systematically reviewing factors correlated with SA. We also compared the relative strength of the components by using the meta-analytic method.
Methods:
A meta-analysis was conducted to quantitatively synthesize the correlates of SA from three online databases: PubMed, CINAHL, and SCOPUS.
Main Findings:
The correlates were categorized into four domains: (1) avoiding disease and disability, (2) having high cognitive/mental/physical function, (3) actively engaging in life, and (4) psychologically well adapted in later life. The domain “psychologically well adapted in later life” showed the strongest association with SA, ES(r) = .482.
Conclusion:
The findings of this study were meaningful in terms of examining the strength of the correlations between the domains and overall SA and, further, providing evidence for building interventions for aging population.
All humans experience aging, which is a continuous but irreversible process accompanying gradual deterioration with regard to body structure and function (van Leeuwen, Vera, & Wolkenhauer, 2010). However, life expectancy is improving, and as a result, the population of older individuals is increasing along with the amount of time spent as an older adult (Cha, Seo, & Sok, 2012). Therefore, we must shift our focus from “how long” to “how well” or “how healthy” to live as an older adult; in other words, the quality of life must be considered as an essential subject regarding aging.
Successful aging (SA) is an emerging concept representing this shift, stressing the quality of aging. The concept of SA has been used interchangeably with various terms such as healthy aging, productive aging, and aging well (Butler, 1988; Depp & Jeste, 2006; Peel, McClure, & Bartlett, 2005; Vaillant & Mukamal, 2001). All these terms imply that later life is no longer considered as a time characterized by illness and dependence but rather as a time of maintaining health and vitality (Martin et al., 2015).
The concept of SA has been interpreted from diverse perspectives, and its definition has evolved through the work of various researchers over the last 50 years (Martin et al., 2015). For instance, Baltes and Baltes (1990) proposed a model of SA based on a theory of adaptive development and effective life management. It explained behavioral, motivational, and cognitive processes in aging, and especially, along with decreasing cognitive function, they suggested the importance of adaptation strategies through the selective optimization with compensation model in achieving SA (Baltes & Baltes, 1990; Vance et al., 2008). Rowe and Kahn (1987) described the concept of SA by trying to differentiate it from “usual aging.” Despite this milestone for outlining the model of SA, there remains no consensus definition (Cosco, Prina, Perales, Stephan, & Brayne, 2014). Generally, SA is characterized by high ability and function in the physical, mental, and social domains. Specifically, according to Rowe and Kahn (1987, 1998), there are three components that comprise SA: (1) avoid disease or any disability, (2) maintain high cognitive and physical function, and (3) prolong active engagement in life.
Thus far, in addition to exploring the components of SA, there have been many studies on SA, including studies on perception of SA among diverse populations (Cheung & Lau, 2015; Javadi Pashaki, Mohammadi, Jafaraghaee, & Mehrdad, 2015; Javadi-Pashaki, Mohammadi, Jafaraghaee, & Mehrdad, 2015; Kelly & Lazarus, 2015; Reichstadt, Sengupta, Depp, Palinkas, & Jeste, 2010; Romo et al., 2013), exploring SA strategies (Harmell, Jeste, & Depp, 2014; Woo, 2011), and developing and testing SA instruments (Troutman, Nies, Small, & Bates, 2011). In particular, many prior studies have investigated the factors positively or negatively related to achieving SA in older individuals; thus, many correlates of SA have been documented. Nonetheless, although multiple components and correlates of SA have been explored, no studies have synthesized those factors or measured the strength of components and factors in order to identify those that contribute substantially to overall SA. These developments would be critical theoretically in that they would contribute to broadening our knowledge of the concept of SA. Practically, we hope to provide strong evidence for developing intervention programs toward helping older individuals improve their quality of later life as well as support them as they undergo aging processes successfully.
Therefore, the purpose of the study was to identify the component of SA by reviewing and categorizing the correlates reported in previous studies. In particular, we categorized the correlates into domains based on the model of Rowe and Kahn (1987, 1998) and compared the strength of each domain contributing to overall SA. The specific aims of this study were to (1) review correlates of SA in older adults, (2) categorize the correlates into domains based on Rowe and Kahn’s model (1987, 1998), (3) identify the strength of each domain contributing to SA, and (4) identify the factors of each domain showing the strongest contribution to SA. In this study, we defined SA based on an earlier model of SA (Pruchno, Wilson-genderson, & Cartwright, 2010; Rowe & Kahn, 1987, 1998). Thus, we assumed that SA is composed of multiple conditions, such as physical and cognitive health conditions and social engagement. Further, we assumed that the level of SA is determined by integrating subjective and objective considerations. In addition, correlates were defined as factors either positively or negatively correlated with the level of SA.
Methods
Design and Procedure
A meta-analysis was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis 2009 Checklist (Moher, Liberati, Tetzlaff, & Altman, 2009). The relevant studies were retrieved from three online databases—PubMed, CINAHL, and SCOPUS—filtering studies published in last 10 years (since 2005) and written in English. The search terms were the combination of “successful aging” and “factors” (or “influencing factors”). The final day of searching was January 8, 2016. Articles were included if they discussed factors associated with SA in older adults by examining correlations (Pearson’s r). However, articles were excluded if the studies (1) did not have the full text, (2) were written in a language other than English, (3) did not provide Pearson’s r, (4) examined issues other than the association between the factors and SA, (5) were experimental studies (e.g., randomized controlled trials), or (6) used qualitative analytic methodology. In total, 640 articles were found through online databases. Studies were carefully screened and selected by the first author. Among the 640 articles, 306 were excluded after removing duplicates, and 54 were additionally found in reference lists, and thus they were included. Then, another 373 articles were excluded in accordance with the inclusion/exclusion criteria for this study. Therefore, only 15 articles were included for the analysis. Specific searching procedures are illustrated in Figure 1.
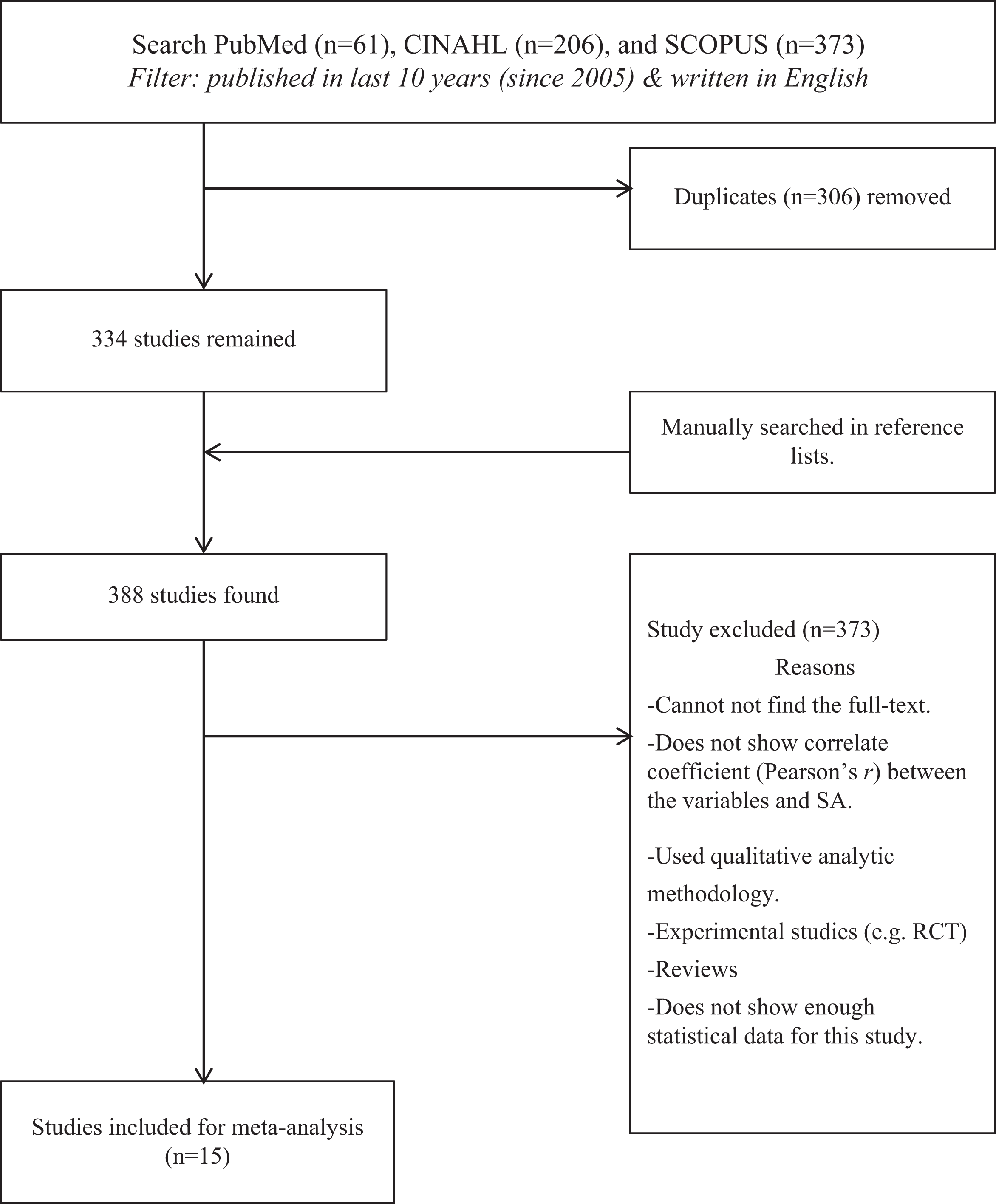
Flow diagram of study selection.
Quality Appraisal
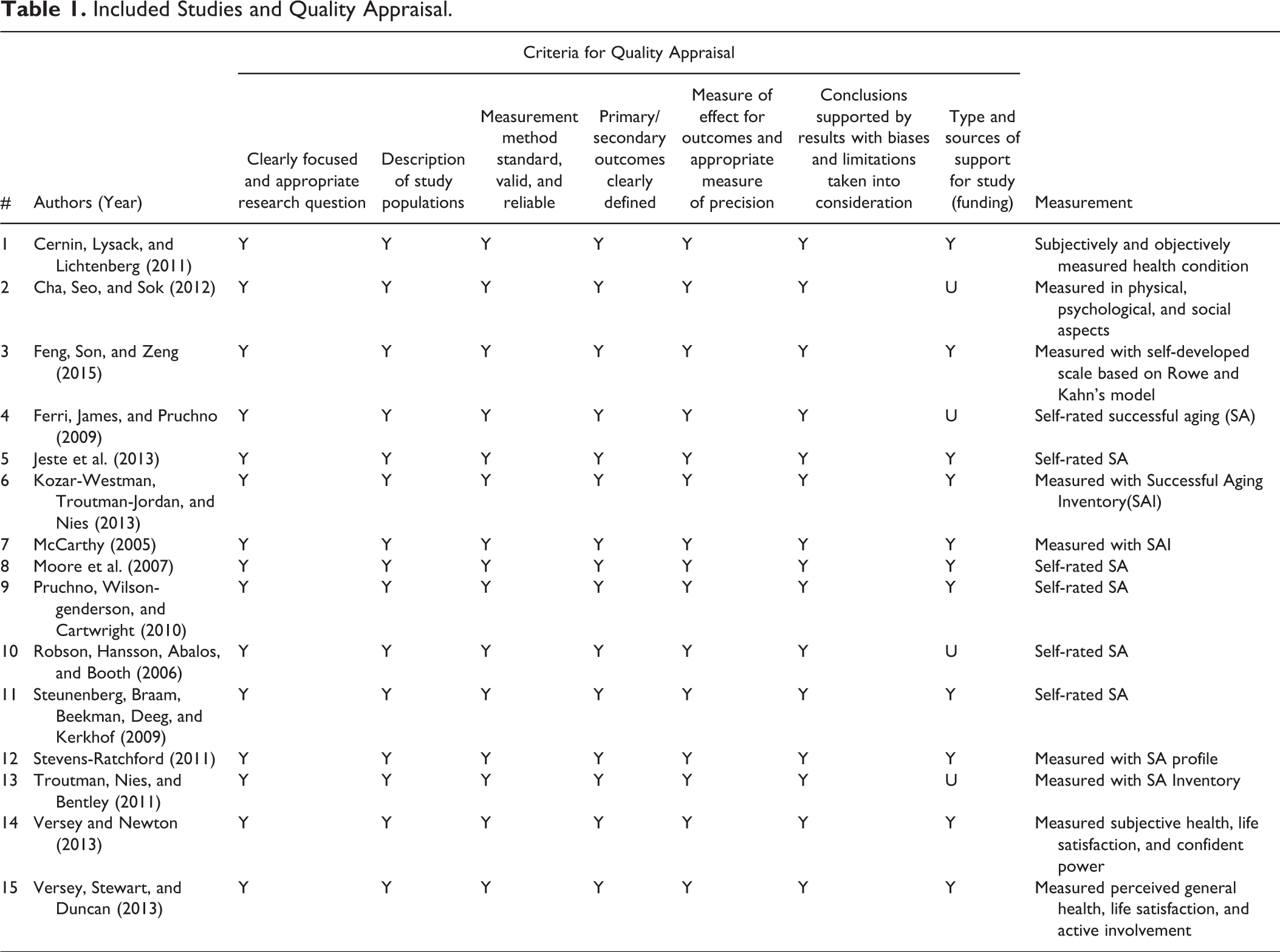
The quality of the included studies was evaluated by the 7 items extracted from the criteria for “domains and elements of observational studies” suggested by the U.S. Agency for Healthcare Research and Quality (West et al., 2002). In other words, the quality of every included study was rated by those 7 items—study questions, study population, measurement, the concepts of outcome, outcome measurement, conclusion, and funding. Each item was coded as “Y” (yes), “N” (no), or “U” (unclear). Two authors evaluated separately and matched the results. Several discussions were conducted for disagreements between two authors on ratings until 100% agreement was achieved. In the end, one nursing doctoral student reviewed and confirmed the results and showed 100% agreement. The results of the quality appraisal are listed in Table 1.
Included Studies and Quality Appraisal.
Data Analysis
Two authors participated in the data extraction and coding process. The coded variables extracted from the included studies were study information (authors, year, title of study, study design, and sample size), participant characteristics (gender and age), correlates of SA, correlation coefficients, and any important information. Each author coded the data separately and matched the results in order to achieve reliability. Any disagreement between the authors was discussed until a consensus was reached. Finally, 137 factors correlated with SA were extracted from 15 studies, and those factors were then categorized into four domains. The two authors reached 100% agreement on coding and categorizing the factors. Finally, one nursing doctoral student reviewed and confirmed the result of coding and categorizing and showed 100% agreement.
In addition, all correlation coefficients between the factors and SA reported in the included studies were coded and transformed into Fisher’s z-scores for interpreting the results. The effect sizes (ESs) were weighted by the study’s inverse variance and sample size. In this study, Comprehensive Meta-Analysis version 2.0 was used for the data analysis.
Results
Description of Studies
Fifteen studies were selected for this study. The number of study participants ranged from 53 to 15,191, and the mean age of participants ranged from 52 to 81.1. Six studies (40%) were published between 2005 and 2010, and the other nine (60%) were published in last 5 years, from 2011 to 2015. SA in our reviewed studies was measured by using either subjective health and well-being as the outcome of SA or self-rated SA. The specific explanation of how SA was measured across the studies is listed in Table 1.
Publication bias is considered a threat to the validity of the study results. To assess potential publication bias, we constructed a funnel plot (Figure 2) and conducted Egger’s regression test (Egger, Smith, Schneider, & Minder, 1997). Visually, the funnel plot seemed to display a symmetrical pattern, which meant there was neither possible omission of studies nor publication bias. However, as this is a subjective judgment, Egger’s test was additionally conducted. As a result, Egger’s test statistically confirmed the result of the funnel plot (intercept −.501, SD = .551, p = .365). Therefore, we concluded that there was no evidence of publication bias at the 5% significance level, and publication bias was not a threat to our study.
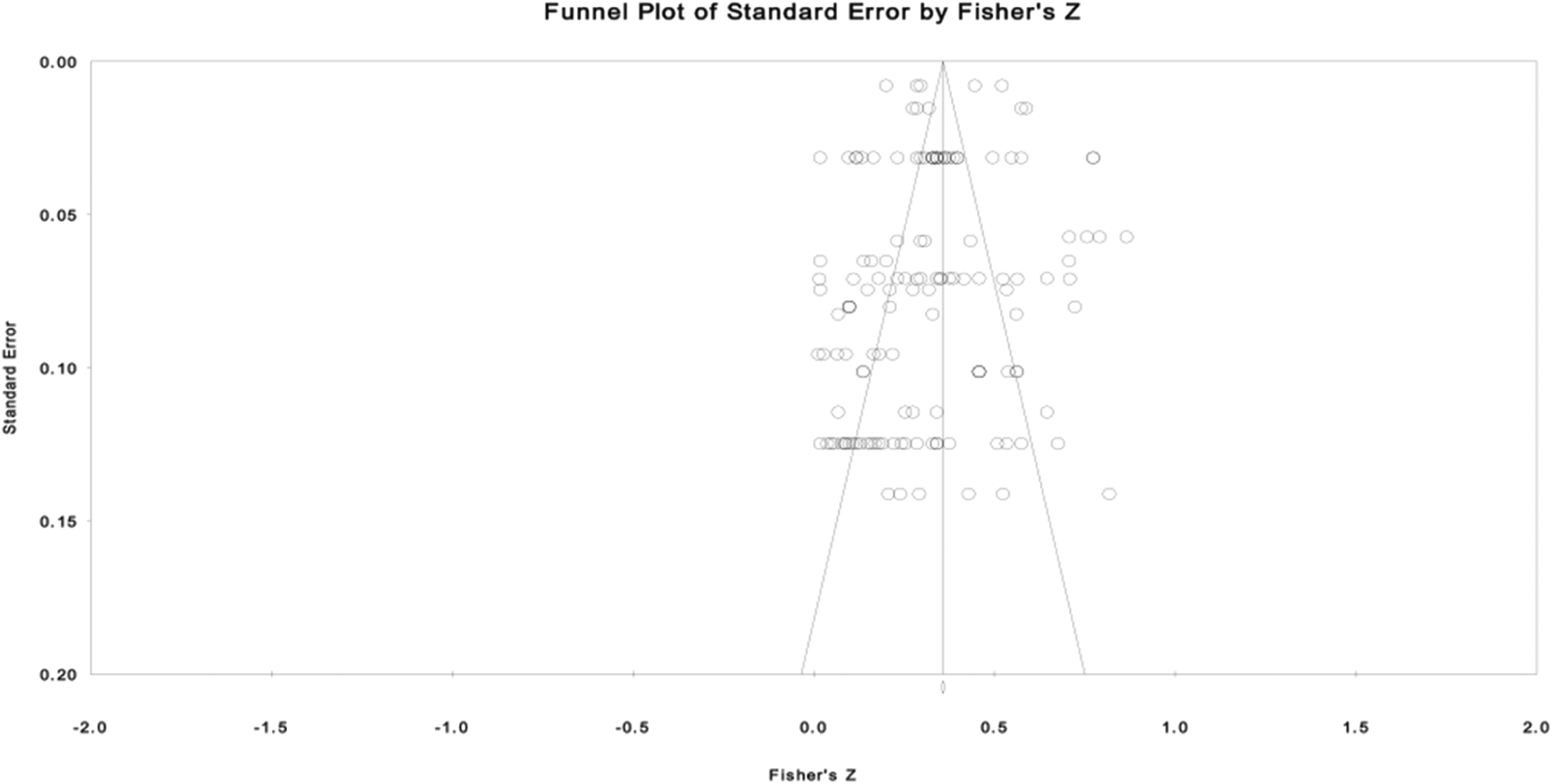
Funnel plot to test publication bias.
Heterogeneity of the effect was tested by using meta-analysis of variance in order to judge whether the publication years and sample sizes of the included studies affected the ESs. As a result, the ESs were not influenced by either the publication year or sample size of the included studies (p = .333 and p = .246, respectively). Thus, we concluded that there was consistency among the ESs in our included studies by publication year and sample size.
Overall ES of influencing factors
An overall ES of all correlates of SA was calculated. As judged by the Q test (Q = 3,084.746, p < .001) and I2 test (95%) for heterogeneity, there was a statistically significant amount of variation in ESs among the included studies. We also assumed that the included studies were not homogeneous in population parameters. For this reason, we calculated the results by applying a random effects model. The overall ES of the correlates was ES(r) = .358, which was a statistically significant medium ES (Cohen, 1992). Thus, the correlates examined in this study were overall positively correlated with SA in older adults.
ES of the domains
In total, we found 137 correlates of SA in older adults and categorized the factors into three domains based on Rowe and Kahn’s model: (1) avoiding disease and disability, (2) having high cognitive/mental/physical function, and (3) actively engaging in life. However, during the categorization process, we decided to build an additional domain, which was not included in Rowe and Kahn’s model, as several correlates were not incorporated into Rowe and Kahn’s domains. This domain was (4) psychologically well adapted in later life. Demographic influences were also examined.
All five domains were strongly associated with SA (Figure 3). The domain with the largest ES was the fourth domain, psychologically well adapted in later life, ES(r) = .482, which is considered a large ES by Cohen (1992). The next largest ESs were actively engaging in life, ES(r) = .373, high cognitive/mental/physical function, ES(r) = .314, and avoiding disease and disability, ES(r) = .307, all of which showed a significantly positive association with SA. The ESs of these three domains were all medium. As the first domain, avoiding disease and disability, involved both risk and protective factors, the ESs were all converted with the absolute values, allowing us to show the strength of the association. Demographic influences showed a small ES(r) = .113. Figures 3 and 4 show the ESs between the domains and SA, those between individual correlates and SA, and the forest plots, respectively.
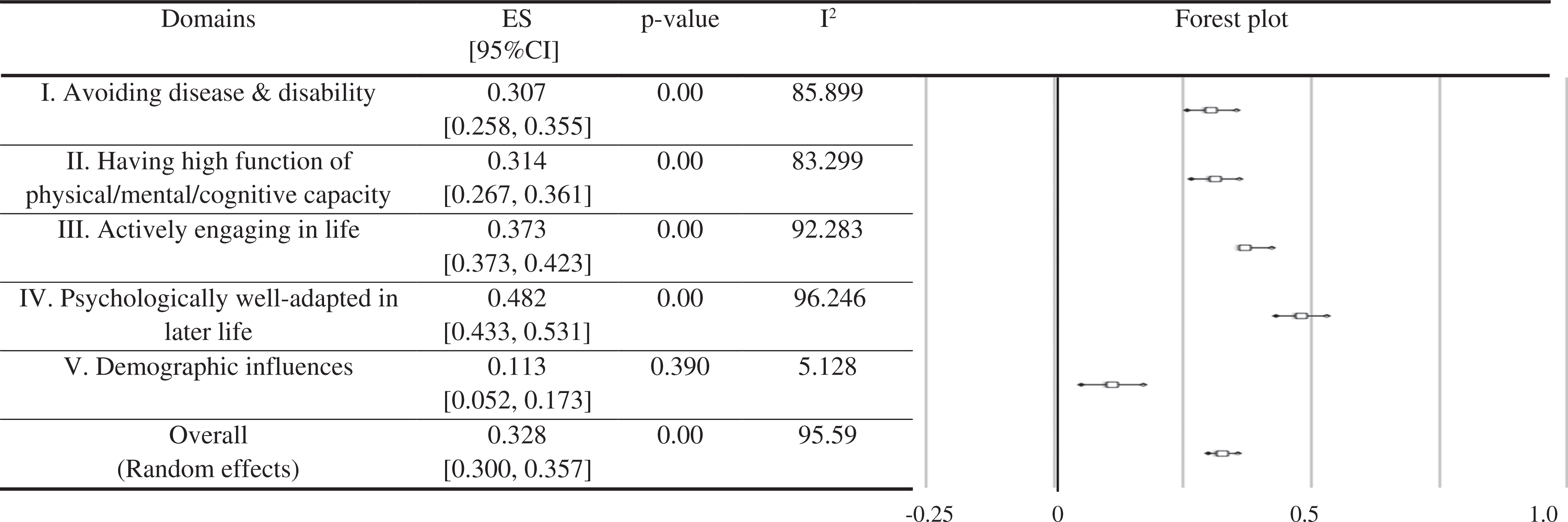
Effect sizes between domains and successful aging and forest plot.
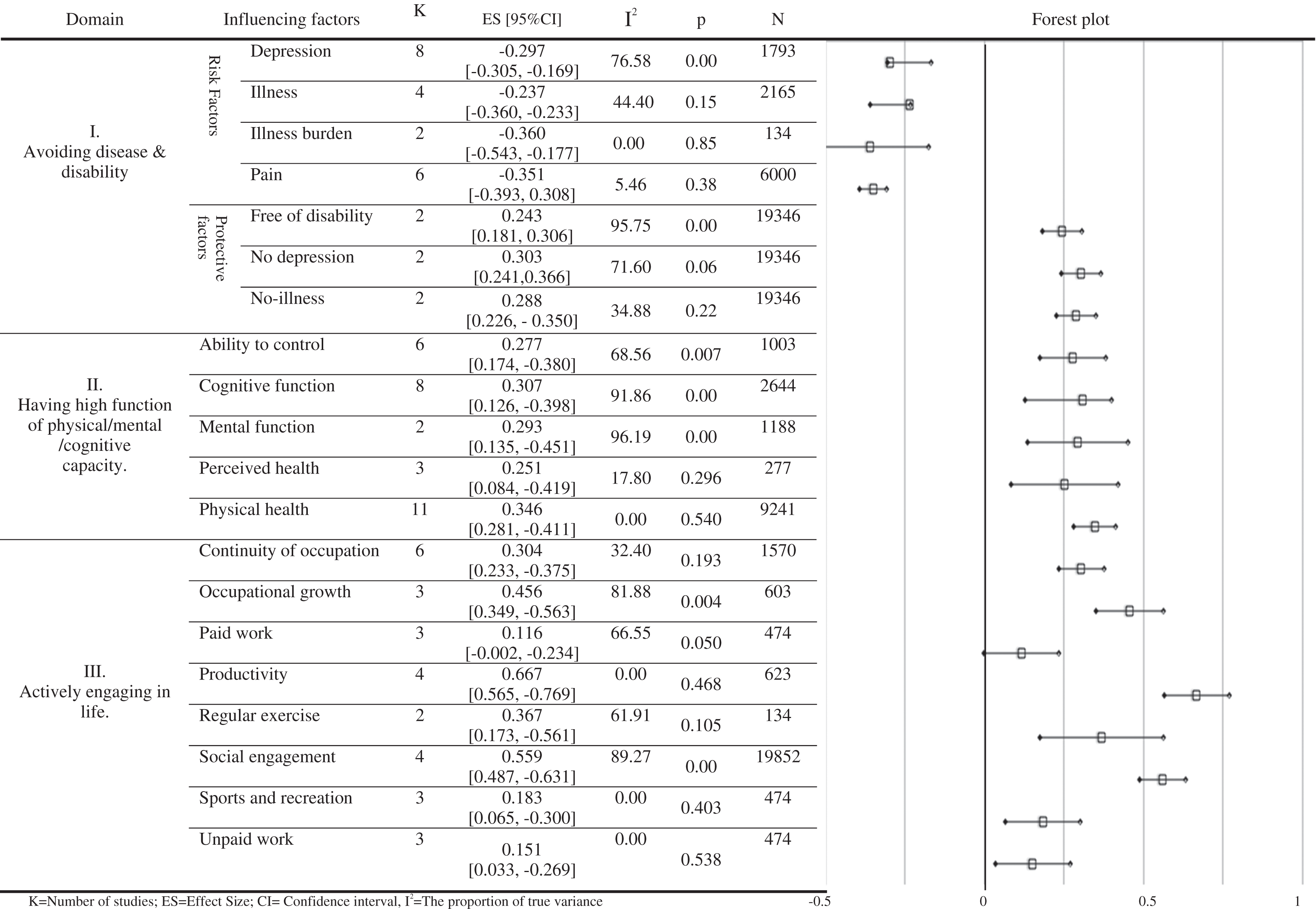
Effect sizes between correlates and successful aging and forest plot.
Avoiding disease and disability
There were seven correlates under this first domain, and those factors were divided into either risk factors or protective factors. Risk factors including illness burden, pain, depression, and illness were all associated with SA. Illness burden—a burden caused by comorbid diseases—showed the largest ES(r) = −.360, among the other risk factors, ES(r)pain = −.351, ES(r)depression = −.297, and ES(r)illness = −.237. Protective factors, including no depression, no illness, and free of disability, also showed an association with SA. In particular, no depression had the largest ES(r) = .303, compared with other protective factors, ES(r)no-illness = .288 and ES(r)free of disability = .243. All seven correlates had a medium ES.
High cognitive/mental/physical function
Under this domain, there were five correlated factors: physical function, cognitive function, mental function, ability to control, and perceived health. All five factors were significantly associated with SA. Specifically, the ES of physical function was the largest, ES(r) = .346, followed by cognitive function, ES(r) = .307, mental function, ES(r) = .293, ability to control, ES(r) = .277, and perceived health, ES(r) = .251. All five factors had a medium ES.
Actively engaging in life
Eight correlated factors were categorized into this domain: continuity of occupation, occupational growth, paid work, unpaid work, productivity, regular exercise, social engagement, and sports and recreation. All the factors, except paid work, showed significant association with SA. Productivity showed the largest ES(r) = .667; and productivity, social engagement, ES(r) = .559, and occupational growth, ES(r) = .456, showed large ESs, while regular exercise, ES(r) = .367, and continuity of occupation, ES(r) = .304, showed medium ESs; and sports and recreation, ES(r) = .183, and unpaid work (e.g., housework, home maintenance, volunteerism, gardening; ES(r) = .151) showed small ESs. Paid work showed the smallest ES; however, it was not statistically significant, ES(r) = .116.
Psychologically well adapted in later life
Six correlated factors were included: life satisfaction, perception of the aging process, personal characteristics, purpose in life, perceived social support, and spiritual commitment. All the factors, except spiritual commitment, were significantly associated with SA. Perception of the aging process showed the largest ES among the six influencing factors, ES(r) = .645. Perception of the aging process, purpose in life, ES(r) = .551, personal characteristics, ES(r) = .518, and life satisfaction, ES(r) = .503, showed large ESs, and perceived social support, ES(r) = .279, showed a medium ES. Spiritual commitment showed the smallest ES; however, it was not statistically significant, ES(r) = .153.
Demographic influences
Demographic factors correlated with SA were found in our reviewed studies. Thus, we tested nine factors including age, alcohol drinking, cigarette smoking, body mass index, education, gender, nutrition, race, and sleep quality. However, none of the factors, except education, showed a significant association with SA. Education showed a small ES(r) = .172.
Discussion
This study identified the factors that correlated with SA in older adults through an extensive literature search and examined the strength of each domain and correlate contributing to SA using meta-analysis. There were four domains identified in this study describing SA: (1) avoiding disease and disability, (2) having high cognitive/mental/physical function, (3) actively engaging in life, and (4) psychologically well adapted in later life. The first three domains were adopted from the elements of SA presented by Rowe and Kahn (1987, 1998). According to Rowe and Kahn (1987, 1998), people should avoid diseases or disease-related disability, maintain high physical and cognitive function, and prolong their engagement in life in order to achieve SA. However, we also found an additional domain, which we called “psychologically well adapted in later life.”
Psychological aspects in SA were actually documented occasionally. For example, in the SA model of Phelan and Larson (2002), positive adaptation was one component of SA. The rest were life satisfaction, freedom from disability, high/independent functioning, active engagement with life, longevity, and mastery/growth. Further, Kahana and Kahana (2003) suggested that SA is composed of social psychological resources, preventive and corrective adaptations, and psychological/existential/social well-being. Nonetheless, no studies to date have examined the strength of its contribution to overall SA.
Indeed, the last domain psychological adaptation showed the strongest association with SA, ES(r) = .482. The interpretation of the result is that in addition to maintaining physical, cognitive, and social function, psychological functioning plays a vital role in SA. In terms of the domain of psychological adaptation, perception of the aging process and life satisfaction showed large ESs. That is, how people perceive and value their process of aging, and consequently, how they feel about their lives was important in achieving SA. This is consistent with Havighurst (1961, 1963), whose definition of SA involved focusing on one’s inner feelings of happiness and satisfaction in his or her present and past life (Havighurst, 1961, 1963; Ouwehand, de Ridder, & Bensing, 2007). Furthermore, according to the findings of this study, not only present and past life but perceived direction in future lives was important, as evidenced by the factor “purpose in life,” which also showed a large ES. This finding stresses the notion that SA is not starting to disengage from life and prepare for death like what Cumming and Henry (1961) insisted, but rather, continually moving on with a direction and goals for the rest of one’s life.
The next domain that showed a strong association with SA was “actively engaging in life,” ES(r) = .373. In particular, productivity and social engagement were strongly associated with SA, showing large ESs. This seems to be a meaningful result, as previous studies have focused more on being free of disability and good physical function in terms of SA. Indeed, according to Depp and Jeste (2006), who conducted a systematic review to examine the definitions as well as predictors of SA, most previous SA literature tended to focus on disability and physical functioning as a main component (definition) of SA (26 out of 29 definitions), and the next most frequent component was cognitive functioning (13 definitions). Compared with those two components, life satisfaction/well-being (9 definitions) and social/productive functioning (8 definitions) were less frequently considered (Depp & Jeste, 2006). However, according to the findings of this study, psychological and social functions, including life satisfaction, productivity, and social engagement, were more important factors with regard to SA.
Interestingly, most of the demographic variables did not show an association with SA, except education. According to a previous study examining the predictors of SA through a systematic review, female gender, ethnicity, and education were not related to SA. Instead, they reported that age (young–old) was a predictor of SA (Depp & Jeste, 2006). These are conflicting results with the findings of current study; thus, further investigations are necessary to clarify and confirm the association between demographic variables and SA.
Recently, Cosco, Prina, Perales, Stephan, and Brayne (2014) conducted a systematic review study to explore the operational definitions of SA. The authors searched and gathered about 105 operational definitions and categorized them into five constructs: physiological, well-being, engagement, personal resources, and extrinsic factors. Interestingly, there was a construct named extrinsic factors, which involved finances. In our study, there was a variable “paid work,” which seems consistent with “finances.” However, based on the statistical analysis, we found that it was not significant in association with SA. This should also be clarified by future studies.
This study has a strong implication that psychological and social aspects in older adults, which have been less frequently considered, are as important as, or perhaps more important than, physical and cognitive functional aspects of SA. Aging will eventually lead to physical and cognitive deterioration—no one can avoid this gradual process. However, it does not mean that SA is not possible toward the end of life. According to the findings of current study, if older individuals are socially active and psychologically well adapted, they can achieve SA in later life, nonetheless they eventually encounter physical and cognitive deterioration. Hence, health professionals could play an important role in helping and supporting older adults through interventions and programs to enhance psychological adaptation and prolong social engagement. In particular, we suggest that health professionals should have a future goal–oriented, optimistic viewpoint when meeting and caring for older people, as the study results revealed that perception of the aging process, life satisfaction, and purpose in life highly contributed to achieving SA.
The present study is meaningful in its contribution to the definition of SA, for which there is no consensus, through finding multiple influencing factors. However, there were some limitations, like any other study. Because this study only included the studies that reported Pearson’s r between the factors and SA, other influencing factors presented with odds ratios or those explored with qualitative methodologies were excluded. Thus, several correlated factors might be missing. Moreover, as there is neither an agreed-upon definition of SA nor a widely used measurement tool, included studies used inconsistent methods to measure SA (e.g., self-rated measures, SA profile, SA Inventory). Accordingly, caution must be exercised in interpreting the results; however, based on the test for heterogeneity, the ESs were not influenced by the measurement tools of the included studies (p = .425). We listed each measurement tool used in the included studies in order to show the variations across studies (Table 1). Finally, this study considered the correlates of SA from an individual perspective and did not consider environmental or social inequality perspectives.
Conclusion
Although many operational definitions have been proposed for SA, no studies have examined the strength of each domain’s contribution to SA. We therefore explored the components of SA by reviewing the correlates of SA identified in previous studies and categorized the correlates into domains based on the model of Rowe and Kahn (1987, 1998). Then, using the meta-analytic method, the domains were compared with regard to strength of association with SA. In total, four domains of SA were identified: (1) avoiding disease and disability, (2) high cognitive/mental/physical function, (3) actively engaging in life, and (4) psychologically well adapted in later life. Specifically, the last domain, psychologically well adapted in later life, showed the strongest association with SA, although the existent model suggested by Rowe and Kahn (1987, 1998) only captured the first three domains. We hope that the findings of this study will contribute to filling the theoretical needs for defining SA as well as identifying evidence for building interventions and programs to achieve SA in older adults.
Footnotes
Authors’ Note
Dr. Sin-Hyang Kim and Dr. Sihyun Park were solely responsible for all the content and writing of the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by INHA Research Grant.