
Abstract
Guided by the life-course perspective, this study contributes to the family caregiving, aging, and disability literature by examining the daily experiences of three types of family caregivers in midlife and late adulthood. A sample of 162 caregivers from the National Survey of Midlife in the United States study completed interviews, questionnaires, and a Daily Diary Study. Multilevel models showed the patterns of daily time use did not differ by caregiver types. Caregivers of sons/daughters with developmental disabilities (DD) experienced more daily stressors than caregivers of parents with health conditions (HC) and caregivers of spouses with HC. Unmarried caregivers of sons/daughters with DD reported spending more time on daily leisure activities and exhibited greater daily stressor exposure than other family caregivers. Age did not moderate the associations between caregiver types and daily experiences. Findings highlight the important consideration of the caregivers’ characteristics to better determine the quality of their daily experiences in midlife and late adulthood.
According to the National Alliance for Caregiving and American Association of Retired Persons (2015), providing care to a family member who is ill or disabled is becoming more common and often lasts into midlife and late adulthood. The reliance on family care is evident by the number of aging and caregiving studies documenting the challenges of family caregiving (e.g., Coyle, Kramer, & Mutchler, 2014; Seltzer et al., 2009; Smith & Grzywacz, 2014; Strawbridge, Wallhagen, Shema, & Kaplan, 1997; Zarit et al., 2014), which predominately have focused on the well-being and experiences of spouses, adult children, and daughter-/son-in-laws as caregivers (e.g., Pinquart & Sorensen, 2011). With the rise in life expectancy of individuals with developmental disabilities (DD; Janicki, Dalton, Henderson, & Davidson, 1999), the nature of family caregiving needs and responsibilities in midlife and late adulthood is changing, and more families will find themselves providing long-term care to their adult child with DD. According to Braddock, Hemp, and Rizzolo (2008), approximately 1.7 million adults with DD are being cared by middle-aged and older family caregivers, and yet, the caregiving and aging literature has paid less attention to the well-being and experiences of this group of family caregivers in the context of other types of caregivers. Although the pathways to becoming a caregiver of a son/daughter with a DD differ from caregiving for a parent or spouse with a health condition (HC), the increasing prevalence of this group of family caregivers providing care through midlife and late adulthood highlights an imperative need to examine their daily experiences in relation to other types of family caregiving. The current study furthers the fields of family caregiving, aging, and disability by examining the influences of caregiving types on aspects of daily time use and stressor exposure.
Caregiving for a Son/Daughter With a DD
Parents caring for sons/daughters with DD often face unique caregiving challenges (e.g., Seltzer, Greenberg, Floyd, Pettee, & Hong, 2001). Unlike other types of family caregiving (e.g., caregiving for a parent or spouse with an HC), caring for a son/daughter with a DD often is a lifelong process that persists into middle-aged and late adulthood. The psychological, physical, and physiological toll of caring for a son/daughter with a DD has been documented in a number of studies (Gerstein, Crnic, Blacher, & Baker, 2009; Seltzer et al., 2010; Wong, Mailick, Greenberg, Hong, & Coe, 2014). In particular, these caregiving challenges have been documented at the daily level. Using a daily diary study design, Seltzer et al. (2009) found parents of adolescents and adults with disabilities reported higher levels of daily negative affect and levels of stress than parents of sons/daughters without disabilities. The researchers also found no differences in patterns of time use between the two groups. In another diary study, Smith et al. (2010) found mothers of adolescents and adults with autism spectrum disorders (ASDs) reported more daily stressors than mothers of children without disabilities. In contrast to the Seltzer et al. (2009)’s findings, Smith et al. (2010) reported mothers of adolescents and adults with ASD spent less time on daily leisure activities, more time providing daily childcare, and more time on daily household chores than mothers of children without disabilities. These findings demonstrated the greater psychological and physical toll of caring for a son/daughter with a DD when compared to parents of children without disabilities. Yet, less is known about the daily experiences of caregiving for a son/daughter with a DD in the context of caregiving for a parent or spouse with an HC.
Caregiving for a Parent With an HC
In contrast to caregivers of sons/daughters with DD, the average length of time an adult spent caring for a parent with an HC is much shorter, and the impacts of caring for a parent with an HC on the caregivers’ psychological and physical health have been studied extensively. Studies generally have found individuals providing care for a parent with an HC experience greater burden, psychological distress, and poorer physical health (e.g., Hoyert & Seltzer, 1992; Marks, Lambert, & Choi, 2002) than individuals who did not provide care. In studies documenting the transition into the caregiving role for a parent, researchers found that caregivers typically exhibit poorer mental health (Strawbridge et al., 1997) and decline in personal mastery (Seltzer & Li, 2000) when compared to noncaregivers. Utilizing a daily diary paradigm, Savla, Almeida, Davey, and Zarit (2008) examined the daily well-being of adult children on days they provided care to their parents when compared to days when they did not provide care. The researchers found greater levels of daily psychological distress on days when adult children provided care to their parents as compared to noncare days. Furthermore, the adult children reported greater number of daily stressors on care days when compared to noncare days.
Caregiving for a Spouse With an HC
According to Brody (1992), many families in the United States often rely on spouses for caregiving needs. The reliance on spouse for caregiving support is not without disadvantages. Past research has shown that caregivers of spouses with HC reported poorer psychological well-being and physical health when compared to nonspousal caregivers (e.g., Braun et al., 2009; Ory, Hoffmann, Lee, Tennstedt, & Schulz, 1999). Moreover, spousal caregivers were more likely to provide greater hours of support and less likely to obtain respite from their caregiving responsibilities when compared to those providing care to a parent or in-law (e.g., Tennstedt, Crawford, & McKinlay, 1993). Because a spouse represents an important attachment figure (Hazan & Shaver, 1987), the caregiving responsibilities may persist even after marital dissolution. For example, Cooney, Proulx, Snyder-Rivas, and Benson (2014) documented the role ambiguity of women providing care for their former spouses and the psychological challenges associated with the caregiving responsibilities. Together, these studies demonstrate the need to examine how different types of caregiving may shape daily experiences.
Daily Experiences
In the recent years, more research has focused on the impacts of caregiving on experiences at the daily level (e.g., Seltzer et al., 2009; Zarit et al., 2014). In this study, we focus on aspects of daily time use and stressor exposure. According to Pearlin, Schieman, Fazio, and Meersman (2005), disruptions or changes in social roles may result in disruptions in other aspects of one’s life. In specifics, providing care to a family member may lead to a recalibration of one’s time use in everyday activities (e.g., Smith et al., 2010) as well as increase one’s exposure to daily stressors, which are defined as the challenges of day-to-day living (e.g., Almeida, Wethington, & Kessler, 2002; Seltzer et al., 2009). By assessing experiences at the daily level, researchers may better capture the periodic peaks and valleys of the individual’s experiences that are reflective of the daily responsibilities, opportunities, and challenges salient to a person’s role as a caregiver. A daily assessment of experiences could function as a more sensitive barometer of life as a family caregiver. From a methodological standpoint, daily diary approach also helps to minimize the amount of time that elapsed between an experience and the account of the experience (Bolger, Davis, & Rafaeli, 2003). This proximal assessment can provide a less biased account of one’s well-being and experiences (Nisbett & Wilson, 1977).
Life-Course Influences
This study is guided by the life-course perspective (Elder, Johnson, & Crosnoe, 2003). With its emphasis on linked lives, the life-course perspective is a well-suited framework to examine the impacts of caregiving on daily well-being and experiences. Informed by the life-course principle that lives are lived interdependently (Elder et al., 2003), we investigate the moderating influence of marital status on the associations between caregiving types and aspects of daily experiences. Prior research documenting the buffering effects of marital status on caregiving has been mixed. Some studies (e.g., Brody, 1992; Marks, Lambert, Jun, & Song, 2008) have found that caregivers’ well-being was enhanced by combining a marital role with a caregiver role. In contrast, Spitze, Logan, Joseph, and Lee (1994) did not observe any buffering effects of marital status on caregivers’ distress. The mixed findings could be due to methodological differences as well as the sample of caregivers examined in the studies. Nonetheless, it is valuable to examine the extent to which the caregivers’ marital status shape the daily experiences of family caregiving in midlife and late adulthood.
In contrast to older individuals, younger individuals are more likely to occupy more social roles and responsibilities (Lachman & James, 1997). More social roles and responsibilities combined with providing care to a family member may be associated with greater time restriction on aspects of daily time use. Additionally, past studies examining age differences in exposure to daily stressors typically have found younger adults reported more number of daily stressors than older adults (Almeida & Horn, 2004; Stawski, Sliwinski, Almeida, & Smyth, 2008; Zautra, Finch, Reich, & Guarnaccia, 1991). This study also examines how age may influence the associations between caregiving types and daily experiences.
Study Aims
This study builds on and furthers the family caregiving, aging, and disability literature by examining the influences of different types of family caregiving, marital status, and age on aspects of daily experiences. In line with past research (e.g., Seltzer et al., 2009; Smith et al., 2010) that showed caregivers of sons/daughters with DD reported more restriction in time use and greater stressor exposure, we predicted that caregivers of sons/daughters with DD will report more time spent on daily household chores and less time on sleep, television watching, physical activities, and leisure activities than caregivers of parents with HC and caregivers of spouses with HC. We also hypothesized a main effect of caregiver types on daily stressors, whereby parents of sons/daughters with DD will report more daily stressors than caregivers of parents with HC as well as caregivers of spouses with HC.
The characteristics of the caregiver also may increase or decrease the quality of their daily experiences. We predict an interaction effect of caregiver types and marital status as well as caregiver types and age on aspects of daily experiences. Specifically, being unmarried will decrease the quality of the daily experiences (more time spent on daily household chores; less time on sleep, television watching, physical activities, and leisure activities; more number of daily stressors) of the caregivers, with the most impact on caregivers of sons/daughters with DD and the least impact on married caregivers providing care to parents with HC. Finally, we predict an interaction of caregiver types and age on daily experiences. Based on prior research documenting the greater demands and responsibilities of younger adults (Lachman & James, 1997), as well as the greater challenges of caregiving for a son/daughter with a DD (Gerstein et al., 2009; Smith et al., 2010), we predict that being younger and a caregiver of a son/daughter with a DD will have the most impact on areas of daily time use when compared to other types of family caregivers. Past literature has shown that younger adults report greater exposure to daily stressors (e.g., Almeida & Horn, 2004; Stawski et al., 2008); thus, we expect younger caregivers of sons/daughters with DD will report the most number of daily stressors.
Method
Sample
Participants derived from the second wave of the National Survey of Midlife in the United States (MIDUS-II). Collected between 2004 and 2006, MIDUS-II comprises a national probability sample of English-speaking, noninstitutionalized adults (n = 4,963) and an African American sample (n = 592) from Milwaukee, WI. Men and women ranged from 28 to 85 years of age. The analytic sample was selected based on a set of criteria. To be included, participants had to complete the Daily Diary Study portion of MIDUS-II (n = 2,022) and currently providing care to a family member.
Family caregivers were identified with a set of variables. To identify family caregivers, we retained respondents who reported yes to “During the last 12 months have you, yourself, given personal care for a period of one month or more to a family member or friend because of a physical or mental condition, illness, or disability?” To determine the type of family caregiving the respondent provided, the following item was utilized: “To whom did you give the most personal care?” Because we were interested in specific types of caregivers, we retained individuals who reported providing care to a son/daughter (biological, step, or adopted child), father/mother (biological, step, or adopted parent), and husband/wife (current or former spouse). Next, to determine whether the sons/daughters have DD, we utilized an additional item from the survey that asked whether the son/daughter living in the household has a developmental disability, such as autism, cerebral palsy, epilepsy, or mental retardation or has ever had long-term serious mental health problems. Individuals who reported yes to this question were retained. To identify whether the care recipients have DD or long-term serious mental HC, we used the question, “What type of developmental disability or long term serious mental health problem does the individual have?” Since we are interested in the caregivers of sons/daughters with DD (e.g., ASD, Down’s syndrome, and cerebral palsy), only those providing care to sons/daughters with DD were retained. Given the variability in caregiving that occurred in the past 12 months, we retained family caregivers who currently are providing care to the individual identified using the item, “Are you still helping (him or her)?”
Based on these selection criteria, 207 family caregivers were identified. From the 207 caregivers, this study focused on 23 midlife caregivers of a son/daughter with a DD, 93 caregivers of a parent with an HC, and 46 caregivers of a spouse with an HC. The analytic sample comprises 162 family caregivers and 1,296 days of daily diary data.
Procedures
Participants completed a set of telephone interview, mailed questionnaires, and the Daily Diary Study. The Daily Diary Study consisted of a telephone interview lasting 15–20 minutes across eight consecutive evenings. The telephone interview included questions on daily time use, stressors, and physical symptoms experienced in the previous 24 hours (Almeida et al., 2002).
Measures
Daily time use
During the Daily Diary Study period, participants reported the amount of time that they spent in each of the following activities in the past 24 hours: (a) sleep, (b) household chores (defined as doing yard work or other routine household chores), (c) work, (d) television watching, (e) physical activities, and (f) leisure activities (defined as activities actively choosing to do things for yourself). We excluded time spent on daily work because some of the respondents in the analytic sample were not working. On each study day, the total number of hours and minutes were calculated for each activity.
Daily stressors
The semistructured Daily Inventory of Stressful Events (Almeida et al., 2002) was used to assess daily stressors. On each study day, respondents reported whether they experienced certain types of daily stressors (arguments, avoided arguments, network stressors, home stressors, work stressors, discrimination, and other stressors) in the past 24 hours. The number of events reported on each day was summed.
Caregiver types
Family caregivers were coded as followed: caregivers of sons/daughters with DD (0), caregivers of parents with HC (1), and caregivers of spouses with HC (2).
Marital status and age
Marital status was a dichotomous variable between unmarried (0) and married (1). In the present analyses, age was a continuous variable.
Covariates
To account for potential influences among the associations of caregiving and aspects of daily experiences, several characteristics of the caregivers were included. Caregivers’ highest education level (coded from 0 = less than high school to 2 = associate degree/BA or higher) was included as controls. The number of chronic conditions (from a list of 31 conditions, including diabetes and migraine headaches) experienced in the past year was included (Cleary, Zaborski, & Ayanian, 2004). For the models predicting daily stressors, daily negative affect from the previous day was included as a control because past studies have shown that negative affect often is associated with stressor exposure and reactivity (Sliwinski, Almeida, Smyth, & Stawski, 2009). To assess daily negative affect, respondents were asked how frequently (0 = none to 4 = all of the time) they felt each of 14 negative emotions (e.g., restless or fidgety, nervous, and hopeless) in the past 24 hours (Ready, Akerstedt, & Mroczek, 2011). On each day, the average score across the 14 items was calculated. Because daily negative affect from the previous day was assessed repeatedly, the models predicting daily stressors included within- and between-person effects of daily negative affect using the person-mean center approach outlined by Hoffman and Stawski (2009).
Data Analyses
To assess the influences of caregiver types, marital status, and age on caregivers’ daily experiences, a set of two-level, multilevel model (SAS Proc Mixed), where days were nested within persons, was employed. For all outcomes, analyses were carried out in three models—main effect of caregiver types (Model A), interaction effect of caregiver types and marital status (Model B), and interaction effect of caregiver types and age (Model C). Continuous time-invariant covariates were centered at the sample mean. Preliminary analyses showed that a random intercept only model had acceptable fit. Because education had no significant effects on the outcomes, this covariate was dropped in the final models.
Results
Descriptive Findings
Table 1 presents the sociodemographic characteristics of the respondents by caregiver types. In this study, caregivers of sons/daughters with DD and caregivers of parents with HC were significantly younger than caregivers of spouses with HC. Caregivers of parents with HC were less likely to be married.
Demographic Characteristics by Caregiver Types.
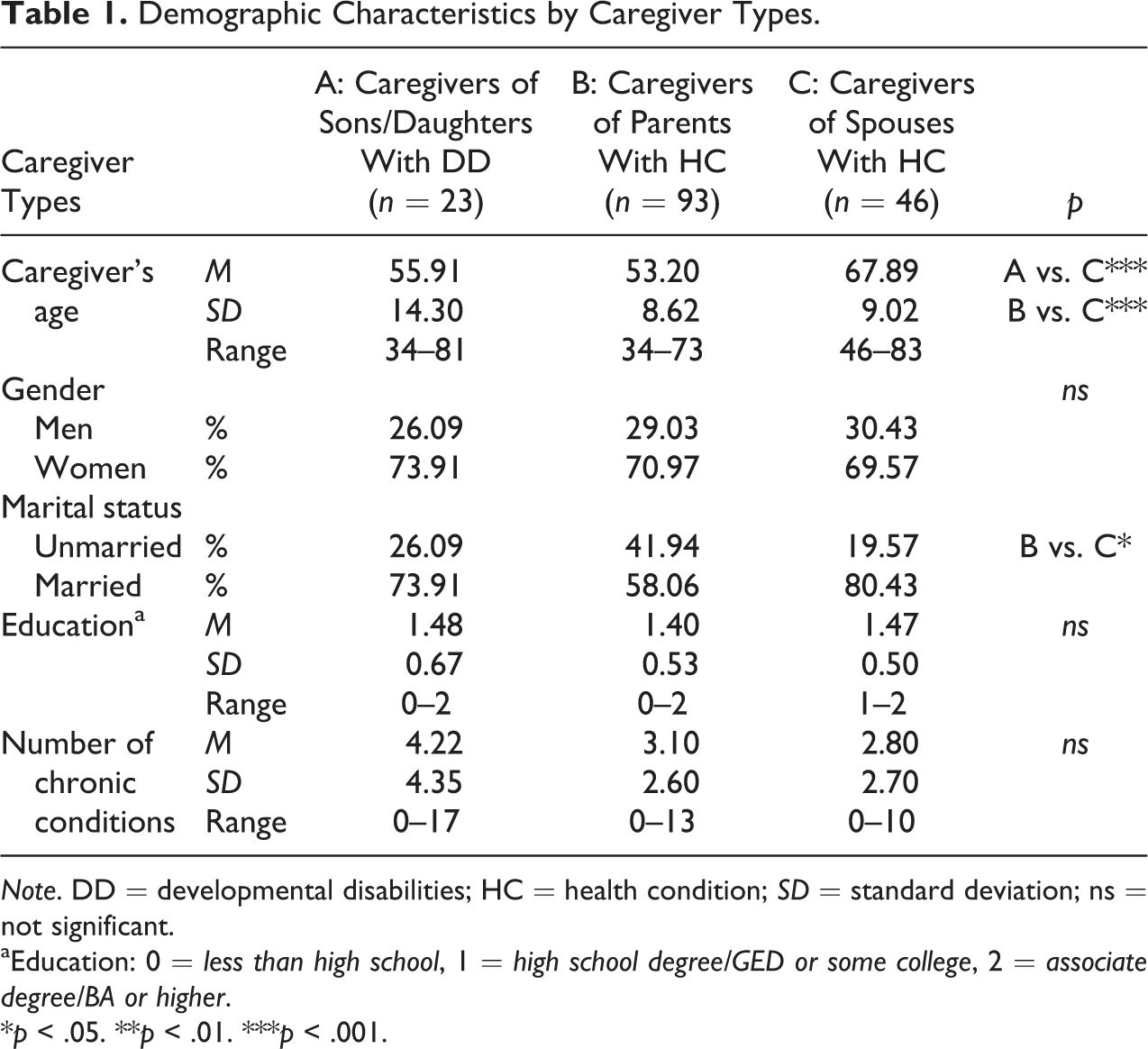
Note. DD = developmental disabilities; HC = health condition; SD = standard deviation; ns = not significant.
aEducation: 0 = less than high school, 1 = high school degree/GED or some college, 2 = associate degree/BA or higher.
*p < .05. **p < .01. ***p < .001.
Multivariate Findings
The first set of analyses examined the influences of caregiver types, marital status, and age on areas of daily time use. With the exception of time spent on daily leisure activities, no main or interaction effects were observed for other areas of time use. Contrary to our expectations, there was not a significant main effect of caregiver types on time spent on daily leisure (see Table 2, Model A). Age, however, significantly predicted time spent on daily leisure activities such that older adults providing care to family members reported spending more time on daily leisure activities than younger adults. There was a significant interaction effect of caregiver types and marital status (DD vs. parents: b = 2.052, standard error [SE] = 0.802, p < .01 and DD vs. spouses: b = 2.508, SE = 0.934, p < .01; see Table 2, Model B). When the simple slopes were probed, unmarried caregivers of sons/daughters with DD spent significantly more time on daily leisure activities than other groups of family caregivers (see Figure 1). Additionally, there was a trend toward significance between married caregivers of sons/daughters with DD and married caregivers of parents with HC. No significant interaction effect of caregiver types and age was observed (see Table 2, Model C).
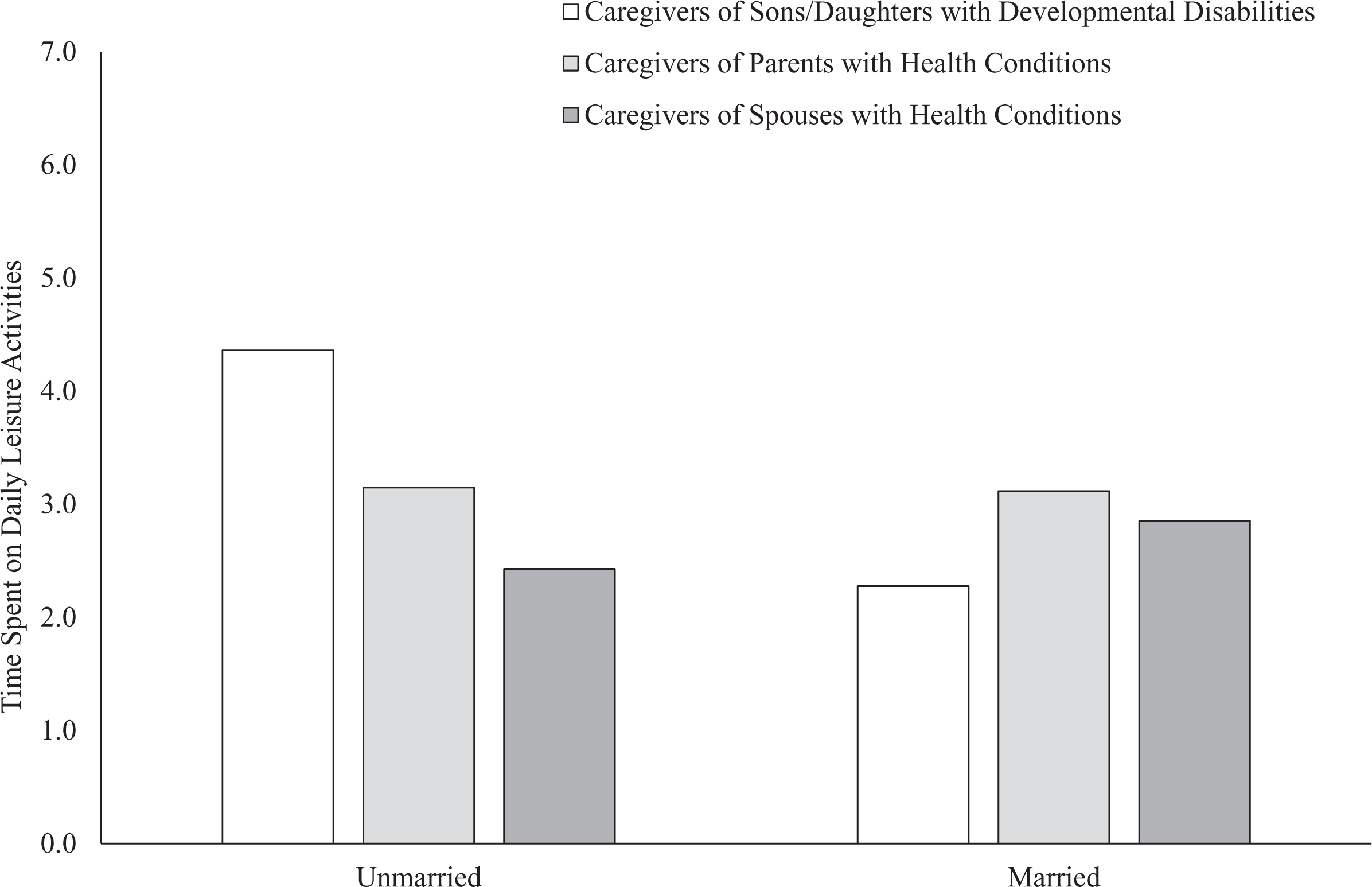
Time spent on daily leisure activities by caregiver types and marital status.
Multilevel Models Predicting Time Spent on Daily Leisure Activities.
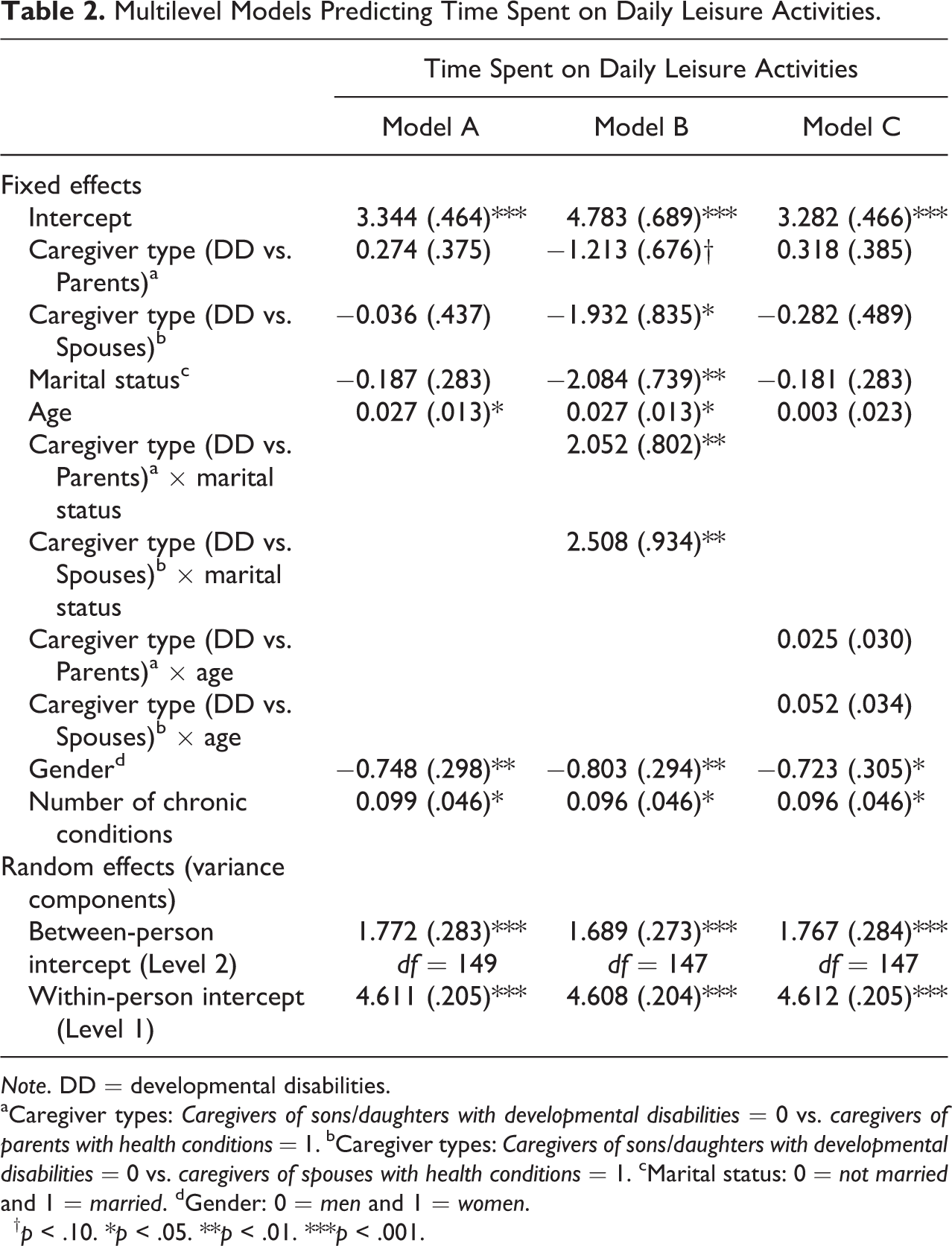
Note. DD = developmental disabilities.
aCaregiver types: Caregivers of sons/daughters with developmental disabilities = 0 vs. caregivers of parents with health conditions = 1. bCaregiver types: Caregivers of sons/daughters with developmental disabilities = 0 vs. caregivers of spouses with health conditions = 1. cMarital status: 0 = not married and 1 = married. dGender: 0 = men and 1 = women.
† p < .10. *p < .05. **p < .01. ***p < .001.
The second set of analyses assessed the effects of caregiver types, marital status, and age on number of daily stressors. As presented in Table 3, Model A, a significant main effect of caregiver types was observed (DD vs. parents: b = −0.391, SE = 0.110, p < .001 and DD vs. spouses: b = −0.289, SE = 0.125, p < .001). Caregivers of sons/daughters with DD exhibited greater number of daily stressors than caregivers of parents with HC and caregivers of spouses with HC. In line with the study hypothesis, there was a significant interaction effect of caregiver types, specifically between caregivers of sons/daughters with DD and caregivers of parents with HC and marital status on number of daily stressors (DD vs. parents: b = 0.576, SE = 0.232, p < .01). An examination of the simple slopes showed that unmarried caregivers of sons/daughters with DD reported significantly greater number of daily stressors than other family caregivers. As illustrated in Figure 2, unmarried caregivers of parents with HC reported the least amount of daily stressor exposure. Next, the interaction effect of caregiver types and age on number of daily stressors was examined, and the findings were nonsignificant (see Table 3, Model C).
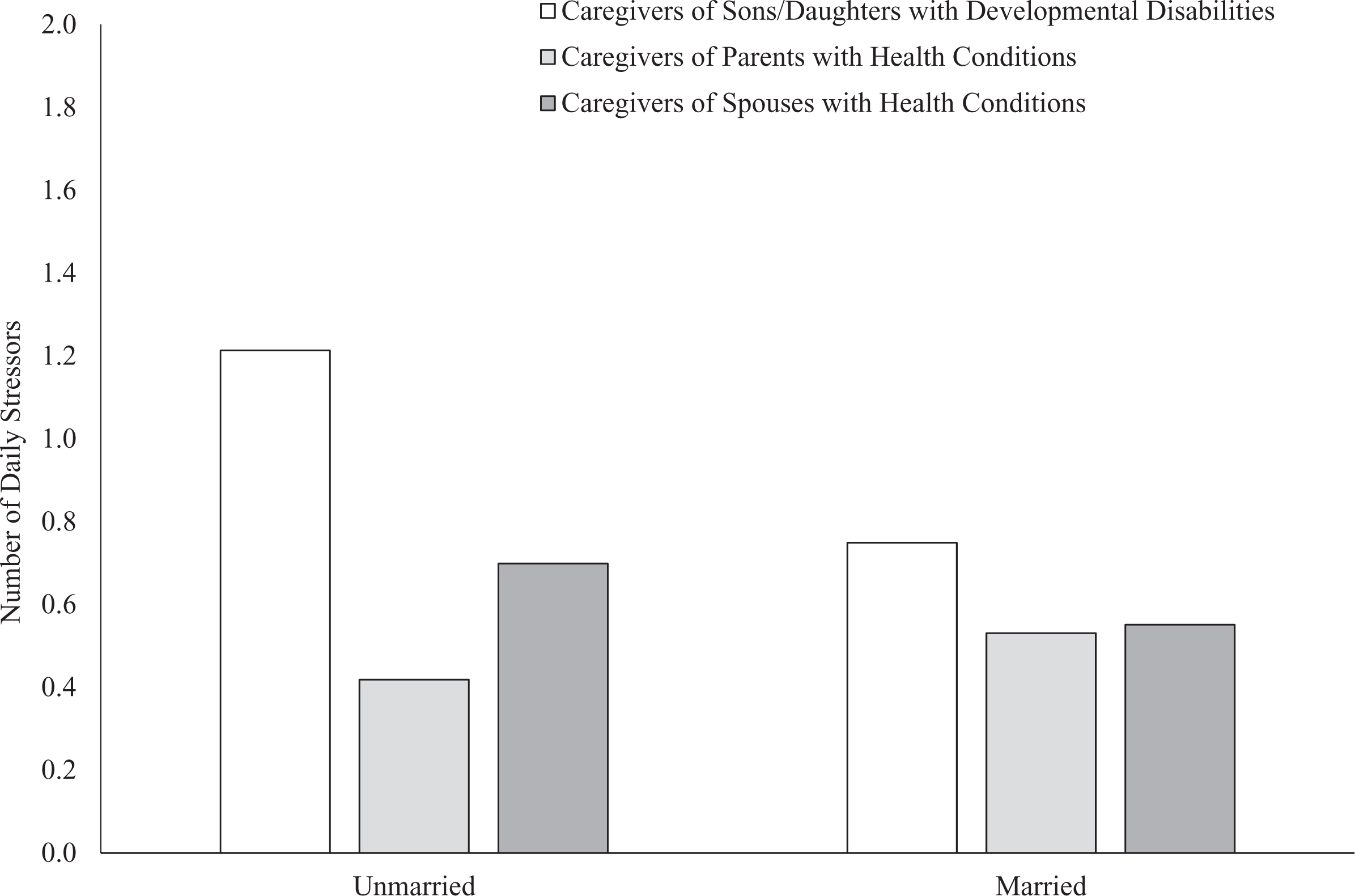
Number of daily stressors by caregiver types and marital status.
Multilevel Models Predicting Number of Daily Stressors.
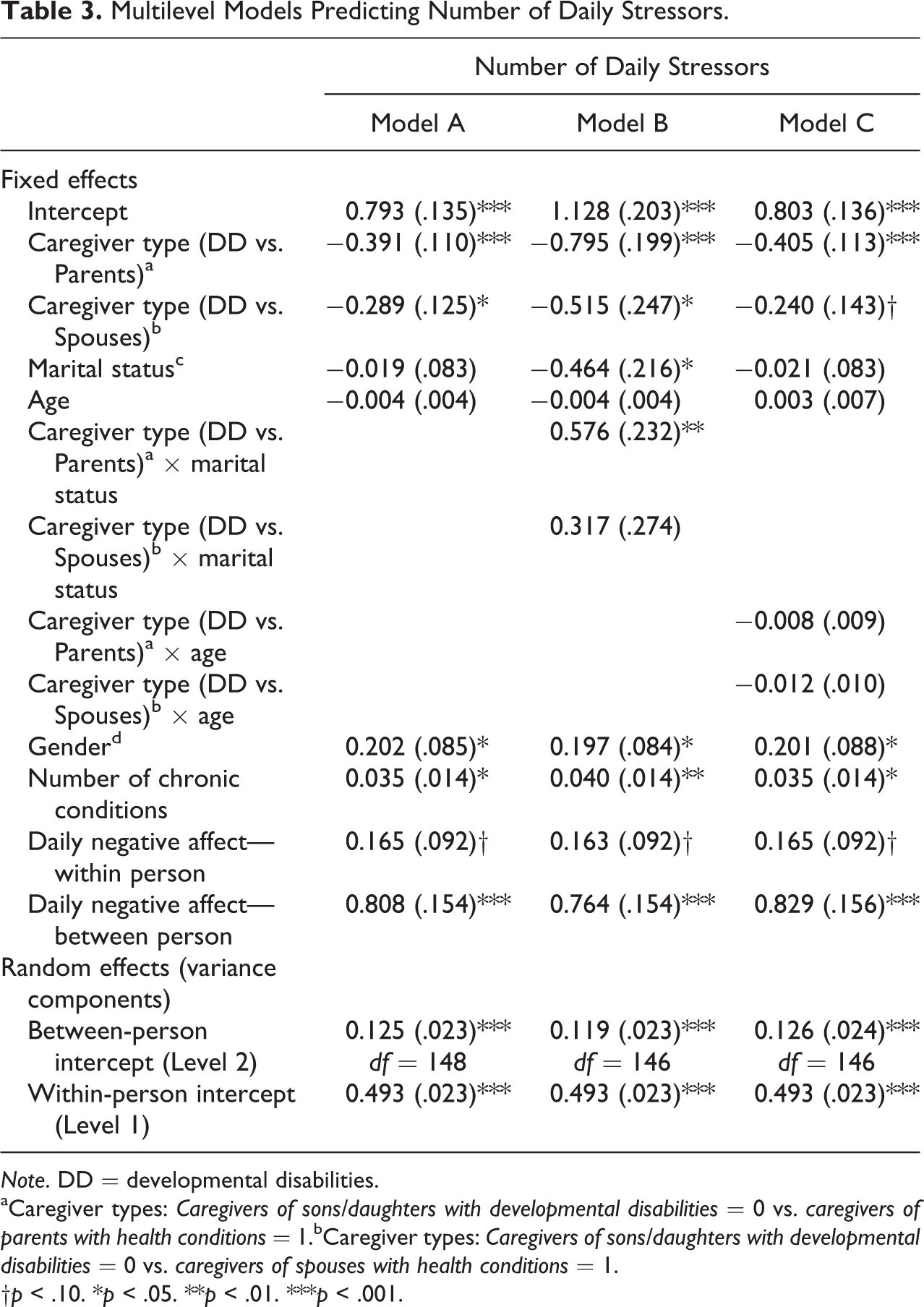
Note. DD = developmental disabilities.
aCaregiver types: Caregivers of sons/daughters with developmental disabilities = 0 vs. caregivers of parents with health conditions = 1.bCaregiver types: Caregivers of sons/daughters with developmental disabilities = 0 vs. caregivers of spouses with health conditions = 1.
†p < .10. *p < .05. **p < .01. ***p < .001.
Discussion
In the study of family caregiving and aging, less attention has been directed toward the examination of daily experiences of caregivers of sons/daughters with DD when compared to other types of family caregivers in midlife and late adulthood. Considering that the life expectancy of individuals with DD has increased (e.g., Janicki et al., 1999), and many rely on family members and services throughout their adulthood (Braddock, Hemp, & Rizzolo, 2008; Heller et al., 2008; Seltzer, Krauss, Orsmond, & Vestal, 2000), it is more important than ever to focus on this group of caregivers in the context of other types of family caregiving (e.g., caring for a parent or spouse). This study examined the influences of caregiving types on aspects of daily experiences and the moderating influences of marital status and age.
Contrary to expectation, the three groups of family caregivers did not differ in their patterns of daily time use with respect to areas of sleep, household chores, television watching, and physical activities. We predicted that caregivers of sons/daughters with DD would exhibit evidence of dysregulation in these areas of time use when compared to caregivers of parents with HC and caregivers of spouses with HC. However, the absence of a significant finding is in accordance with past work (e.g., Hoyert & Seltzer, 1992; Seltzer et al., 2009) that showed patterns of time use in caregivers of sons/daughters with DD closely resemble the time use of caregivers of children without DD and other types of family caregivers (e.g., caregiving for a parent, caregiving for a husband).
Based on the works of Smith et al. (2010), we predicted that caregivers of sons/daughters with DD would report less time spent on daily leisure activities than other groups of family caregivers. While there was not a main effect of caregiver types on time spent on daily leisure activities, a significant interaction effect of caregiver types and marital status on daily leisure activities was observed. Contrary to prediction that unmarried caregivers of sons/daughters with DD would report the least amount of time spent on daily leisure activities, findings from this study showed that unmarried caregivers of sons/daughters with DD spent the greatest amount of time on daily leisure activities when compared to other married and unmarried family caregivers. Perhaps not having a marital partner to turn to for social support, unmarried caregivers of sons/daughters with DD are turning to leisure activities as a resource to help cope with the daily caregiving responsibilities. This possible explanation would be in line with research documenting leisure as an important coping resource (e.g., Nimrod, Kleiber, & Berdychevsky, 2012). It is also possible that the amount of leisure activities embarked by unmarried caregivers of sons/daughters with DD could be a reflection of the caregiving responsibilities involving their sons/daughters with DD. However, the leisure activities item in MIDUS asked participants to provide information on time spent on activities that they actively chose to do for themselves, which may rule out the possible overlap with caregiving responsibilities. Unfortunately, due to the design of the MIDUS Daily Diary Study, we cannot separate out with whom the leisure activity involved or the self-reported benefits or burden of the leisure activities. The lack of information about the nature of the leisure activities points to the need for future studies to investigate the characteristics of leisure activities and the extent to which leisure activities impact other areas of daily well-being and health. After all, recent work has shown that leisure activities function as important moderators and mediators of daily psychological well-being and health in midlife (e.g., Zawadzki, Smyth, & Costigan, 2015).
In line with prior studies (e.g., Brody, 1992; Marks et al., 2008), the buffering effect of marital status on the association between caregiving types and daily experiences was observed. Specifically, in the context of caregiving for a son/daughter with a DD, the absence of a formal marital partner increased one’s exposure to daily stressors. Consistent with our hypothesis that unmarried caregivers of sons/daughters with DD would report more daily stressors than other family caregivers, this finding resonates with prior research documenting the unique challenges of parenting a son/daughter with a DD often translates into greater levels of stress (e.g., Smith et al., 2010; Gerstein et al., 2009). Thus, the combination of having to navigate caregiving responsibilities and not having a marital partner to help with day-to-day activities seemed to increase the caregivers’ vulnerabilities in other areas of their lives.
To better understand the context surrounding the nature of caregiving, we focused on the moderating influence of age on the associations between caregiving types and daily experiences. A main effect of age on daily leisure activities was observed such that older caregivers spent more time on daily leisure activities than younger caregivers. This finding is consistent with our prediction that younger caregivers may have more restrictions on their daily time use when compared to older caregivers due to their placement in the life course. Contrary to expectations, age did not moderate the associations between caregiving types and daily experiences. In this study, caregivers of spouses were older than the other types of caregivers, and it is possible the age difference could have contributed to absence of significant findings. Another possible explanation could be that individuals, regardless of age, who found themselves in the role of being a family caregiver may have developed strategies to help adapt to and cope with everyday stressors. It could also be that age does not best capture the quality of the daily experiences with respect to daily time use and stressor exposure. Past research (Birditt, Fingerman, & Almeida, 2005; Neupert, Almeida, & Charles, 2007) has showed that younger adults typically rate stressors to be more severe than middle-aged and older adults. Thus, age may have a greater influence on the perceptions of the daily experiences (e.g., severity of stressors experienced, benefits/limitations of time use) than the actual daily experiences.
The study has several limitations that warrant discussion. The small sample size of the caregivers of sons/daughters with DD is a concern to the study’s generalizability. It is important to note that our sample of caregivers of sons/daughters with DD derived from a population study that did not specifically recruit individuals raising a son/daughter with a DD or family caregivers. At the same time, the caregivers examined in this study may be a more random sample of the population, which is a strength of this study. The small sample size also did not permit us to separate the different diagnoses of developmental disabilities or health conditions of the care recipient. Past literature has shown certain conditions are more challenging for caregivers (e.g., Smith, Seltzer, & Greenberg, 2012), and thus this limitation should be considered when generalizing the findings. Due to the study design, we were unable to separate out whether the caregiver is providing double or triple care, which has been shown to be associated with overall psychological functioning (DePasquale et al., 2016; Perkins & Haley, 2010) or how caregiving burden may influence the quality of daily experiences. To capture a more complete understanding of the caregiving process in midlife and late adulthood, it would be valuable for subsequent studies to include responses from multiple sources (e.g., caregiver’s spouse/partner, care recipient, and additional caregivers) associated with the caregiving relationship.
Our study focused on the contrast between married and unmarried caregivers, which may have oversimplified the contextual influences of the marital role. The possible oversimplification of the marital context in this study was further illustrated by the subgroup of caregivers (n = 9) who reported being unmarried but were providing care to their former spouses. This unexpected finding raised questions about the nature of the caregiving relationship when marital role ambiguity (e.g., the role of a former spouse) exists. The work of Cooney et al. (2014), who found the need to protect their children (e.g., help to reduce son/daughter’s caregiving burden), altruism, and guilt were the predominate factors that motivated women to care for their former spouses, suggests that the caregiving role must be considered in the context of social ties and commitment when marital role ambiguity is present. Given the limited research on this subgroup of caregivers, future studies should investigate the nature of the marital context in shaping family caregivers’ daily experiences.
This study is strengthened by the use of a naturalistic sampling of daily time use and stressors, thereby enabling researchers to more accurately capture the experiences, challenges, and opportunities that family caregivers face on a day-to-day basis. Another advantage of this study is that daily leisure activities were defined as activities that participants actively choose to do for themselves rather than a set of specific leisure activities (e.g., reading). This methodological approach allowed the respondents, rather than the researchers, to identify the activities that they consider leisure activities, resulting in a more comprehensive assessment of time spent on daily leisure activities.
Altogether, our findings suggest that the nature of the caregiving activities, rather than the amount of daily time spent providing care, may matter more in impacting the daily experiences of caregivers of sons/daughters with DD when compared to other types of family caregivers. It is possible that the characteristics of the DD conditions (e.g., behavior problems, communication limitations) may be more demanding when compared to caring for a spouse or aging parent. Prior studies have shown that the characteristics of the DD conditions (e.g., behavior problems) can take a greater toll on the health of parents of adolescents and adults with DD but have less influence on the health of parents of individual without disabilities (e.g., Seltzer et al., 2009), thereby emphasizing the unique nature of caregiving for individuals with DD. While this study does not permit the examination of the different types of caregiving activities performed, findings from this study point to the need to better determine how caregiving needs and responsibilities for adults with DD are similar to and different from other types of family caregiving in the aging literature (e.g., caring for a spouse or a parent). Considering the current challenges faced by aging and disability resource centers in meeting the needs of individuals aging with intellectual and developmental disabilities and their family members (see Coyle, Putman, Kramer, & Mutchler, 2016), the knowledge gained from further identifying the similarities and differences in caregiving responsibilities of different types of family caregivers will help to better prepare aging and disability service providers in recognizing the nuances in service needs across aging family caregivers and individuals who are aging with DD.
Furthermore, the study findings highlight the need for services and programs to direct greater attention and resources to vulnerable family caregivers in middle-aged and late adulthood. Services and programs aimed to help reduce daily caregiving demands would be especially beneficial for unmarried caregivers of sons/daughters with DD who may not have a support system to ease the daily caregiving responsibilities. While there are educational programs assisting families of young children with DD to learn parenting skills to reduce stress (e.g., Singer, Ethridge, & Aldana, 2007 for a review), existing DD programs and service providers often lack the resources or training to meet aging needs (see Coyle et al., 2016). Existing caregiving, aging, and disability programs could be modified to include topics or support groups addressing the diversity of family caregiving responsibilities and demands in midlife and late adulthood. Therefore, these services and programs may help to reduce the daily challenges of family caregiving and increase the caregivers’ overall well-being and health in midlife and late adulthood.
Together, this study contributes to the fields of caregiving, aging, and disability literature by investigating the daily experiences of different types of caregivers in midlife and late adulthood. Findings from this study reinforce prior work documenting the daily wear and tear of caregiving for a son/daughter with a DD (Gerstein et al., 2009; Seltzer et al., 2009). Furthermore, to fully understand the impacts of caregiving on daily experiences, the characteristics of the family caregivers also must be considered.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The MIDUS II research was supported by a grant from the National Institute on Aging (P01-AG020166) to conduct a longitudinal follow-up of the MIDUS I investigation.